OK that went well, I think 😎.
Here are my reading of the sessions:
SESSION 1: UK-REBOA
Most would say REBOA as currently delivered does not have a place in ED phase of care of major trauma patients thought to have non-compressible haemorrhage.
BUT:
? - Does it have a niche in the right patients - if only we could recognise them?
? - Would the results be the same for new techniques like partial REBOA
? - Has the right place always been prehospital / deployed situations? (given the caveats above)
We still don't have answers for non-compressible torso haemorrhage, and although there are other devices out there/on the horizon, they come with their own issues and are (far far) less rigorously evaluated.
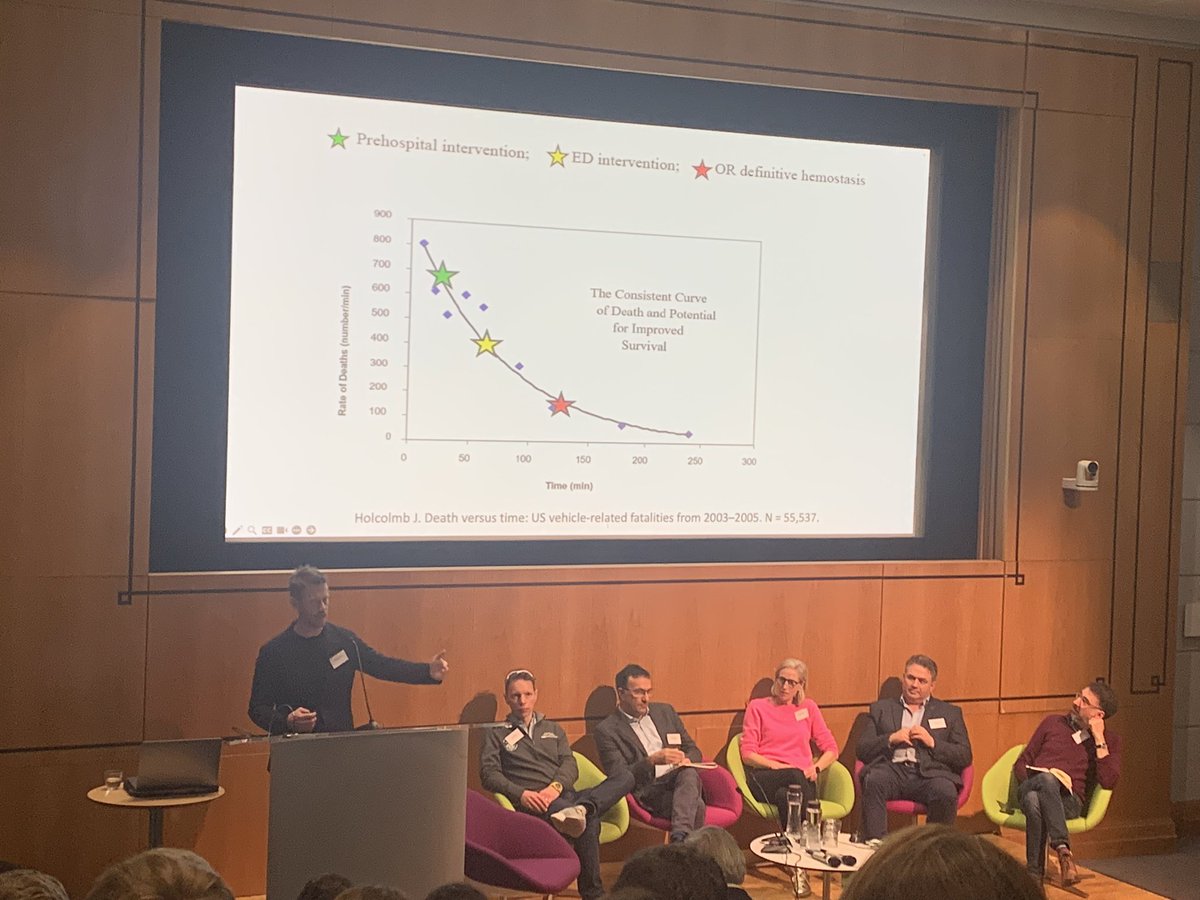
SESSION 2: THE BLEEDING PATIENT
TIME came up again and again.
Are we fast enough. Are we as fast as we think we are (no).
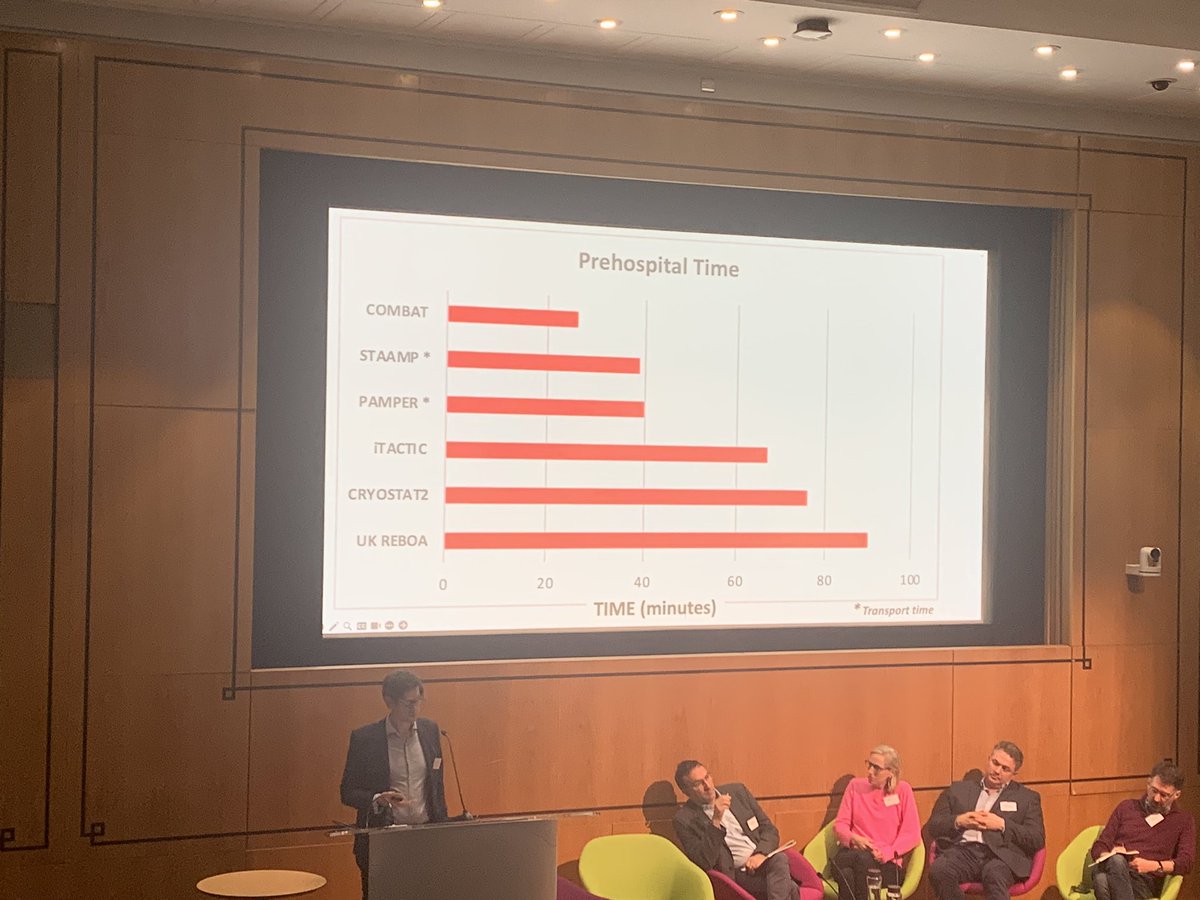
There are clear differences between different systems.
We need to consistently examine what we do and identify the opportunities to be faster.
If we had been faster - if we could be faster - would REBOA have worked?
Do we need a way to physically separate these patients from the wider ED/trauma population?
SESSION 3: CRYOSTAT2
There was general acceptance that high-dose cryoprecipitate (or fibrinogen concentrate) should not be given to all trauma patients on arrival.
Cryoprecipitate remains indicated when there is low fibrinogen, and is likely safe and effective when given empirically later in bleeding (eg after 8 units RBCs).
Again patient selection is key. Point of care fibrinogen or equivalent ROTEM/TEG could guide treatment.
Probably a case now for all UK MTCs to have immediate point of care access to ROTEM & TEG.
Processes and human factors are as important if not more important than what we are giving.
Again hospital design and planning important.
We should examine/research moving away from blood-bank based therapies.
How do we audit and quality improve coagulation therapies. What should we be measuring to drive improvements?
DAY 2: DECISION MAKING IN TRAUMA
(I am going to do this day a disservice by summarising it so succinctly, but...)
Again and again on Day 1, the issues of patient selection came up, and the recognition that we don't have the tools to consistently do this, even in expert hands.
Decision making in trauma care is complex and nuanced and not easily explainable by the people who made those decisions. Uncertainty is higher at the times when the most critical decisions must be made.
There's a real opportunity for AI decision support. AIs (or SOFTWARE as we are encouraged to refer to these tools) cannot MAKE decisions. But they can potentially integrate multiple data points to "expose" the current state of the patient.
There are many many aspects to consider in moving from an in-solico prediction model to a real world widely used and trusted decision support tool, and no one has done this as yet, really, for anything in medicine.
The team
@nigeltai and
@ZBPerkins have put together at
@QMULBartsTheLon are on their way to doing this.
PUBLIC ENGAGEMENT & INVOLVEMENT
There was a lot of enthusiasm for a programme of work to develop a "roadshow" of sorts that could be used locally in MTCs, TUs etc to showcase to the public how trauma care has improved over the last 15 years, especially through research-led changes an interventions. An opportunity as well to highlight local injury prevention activities, successes and innovations, and to highlight the important of things like bystander bleeding control training (first aid!). Check in with James
@thepiercy if you have ideas / want to get involved.
THAT'S IT from the meeting - but the conversations will continue and we will explore how we can develop these into recommendations and policy (so good to hear everyone else's take-homes too). Thank you to everyone who attended and contributed, in person and online.🙏