Real-time analysis of 6,000 COVID-19 studies for 223 treatments. c19early.org
Joined June 2020
- Tweets 1,245
- Following 210
- Followers 10,462
- Likes 2,042
642 Photos and videos


Pinned Tweet

This is why it's possible to have a pandemic for an easily treatable virus.
Here are two “experts” definitely claiming that ivermectin has no benefit for hantavirus.
The problem? It's impossible to know this - there are no studies.
Once definitive claims are made, moral, legal, career, and reputational liabilities strongly disincentivize any admission of error. If future data shows benefit, the error will not be corrected.
Ivermectin is one of hundreds of compounds that could help and would be logical to test further immediately. There is extensive data suggesting potential benefit.
—
Preclinical data suggesting potential benefit of ivermectin for hantavirus:
• Endothelial barrier and capillary-leak modulation - relevant for both HFRS and HCPS/HPS, as increased vascular permeability and thrombocytopenia are central to the pathophysiology of both syndromes, with kidney-predominant injury in HFRS and lung-predominant injury in HCPS. Preclinical research shows reduction of alveolar-capillary permeability, BALF protein leakage, lung wet/dry ratio, and pulmonary edema in acute lung injury models, and indirect support from LPS inflammatory-shock, NF-κB/cytokine, NLRP3, and bleomycin lung-injury/fibrosis studies.
• Anti-inflammatory and lung-injury protection - especially relevant to HCPS, where pulmonary edema, hypoxia, hypotension/shock, and immune-mediated vascular leakage dominate severe disease. Preclinical research shows protective signals related to acute lung injury, cytokine suppression, NF-κB/p65 modulation, NLRP3, NET/GSDMD-related lung injury, LPS-induced inflammatory injury, myocarditis, and fibrosis models.
• Importin-α/β and NF-κB pathway interference - the hantavirus nucleocapsid (N) protein interacts with importin-α and modulates TNF-α/NF-κB signaling, providing a specific target aligned with known ivermectin mechanisms.
• Broad-spectrum antiviral activity against dengue, Zika, West Nile, yellow fever, Japanese encephalitis, chikungunya, Semliki Forest, Sindbis, HIV-1, SARS-CoV-2, and influenza is also supportive. Hantaviruses are also enveloped RNA viruses, although biologically distinct from flaviviruses, alphaviruses, coronaviruses, retroviruses, and influenza viruses.
• Inhaled formulations of ivermectin may be of particular interest for HCPS, allowing direct, localized treatment to the lower respiratory tract.


8
19
1,749
Covid Analysis: 200 COVID-19 treatments retweeted
The three trials cited all show efficacy despite terrible design and attempts not to.
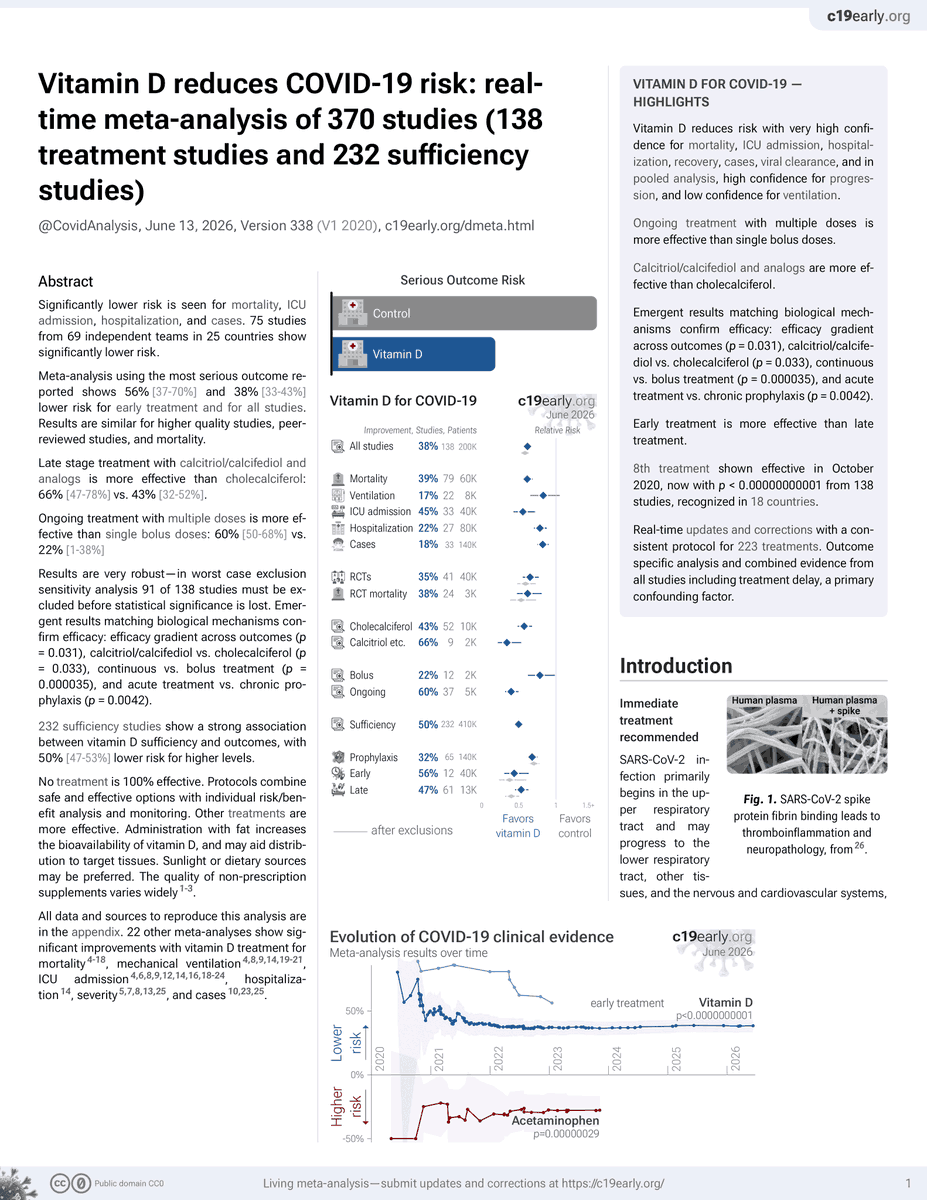
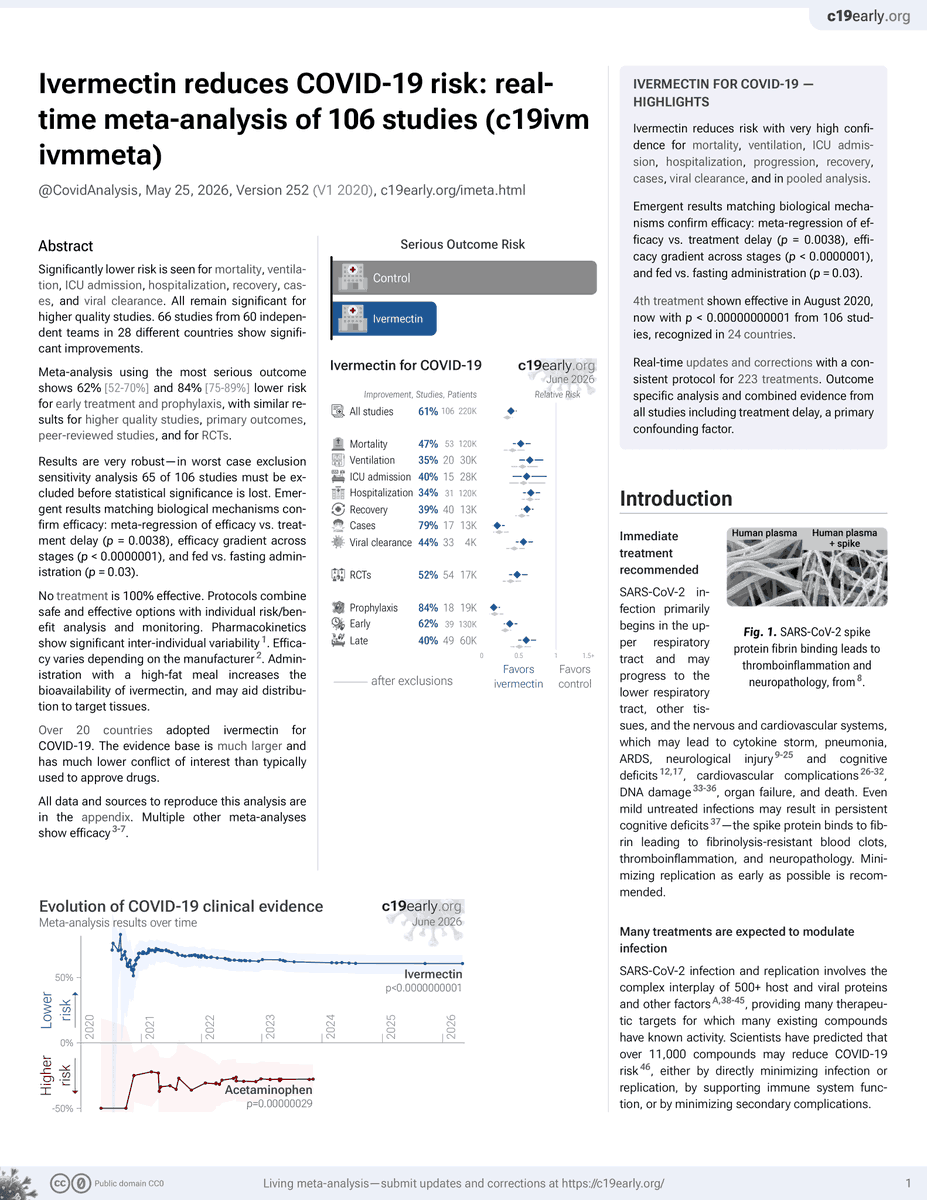
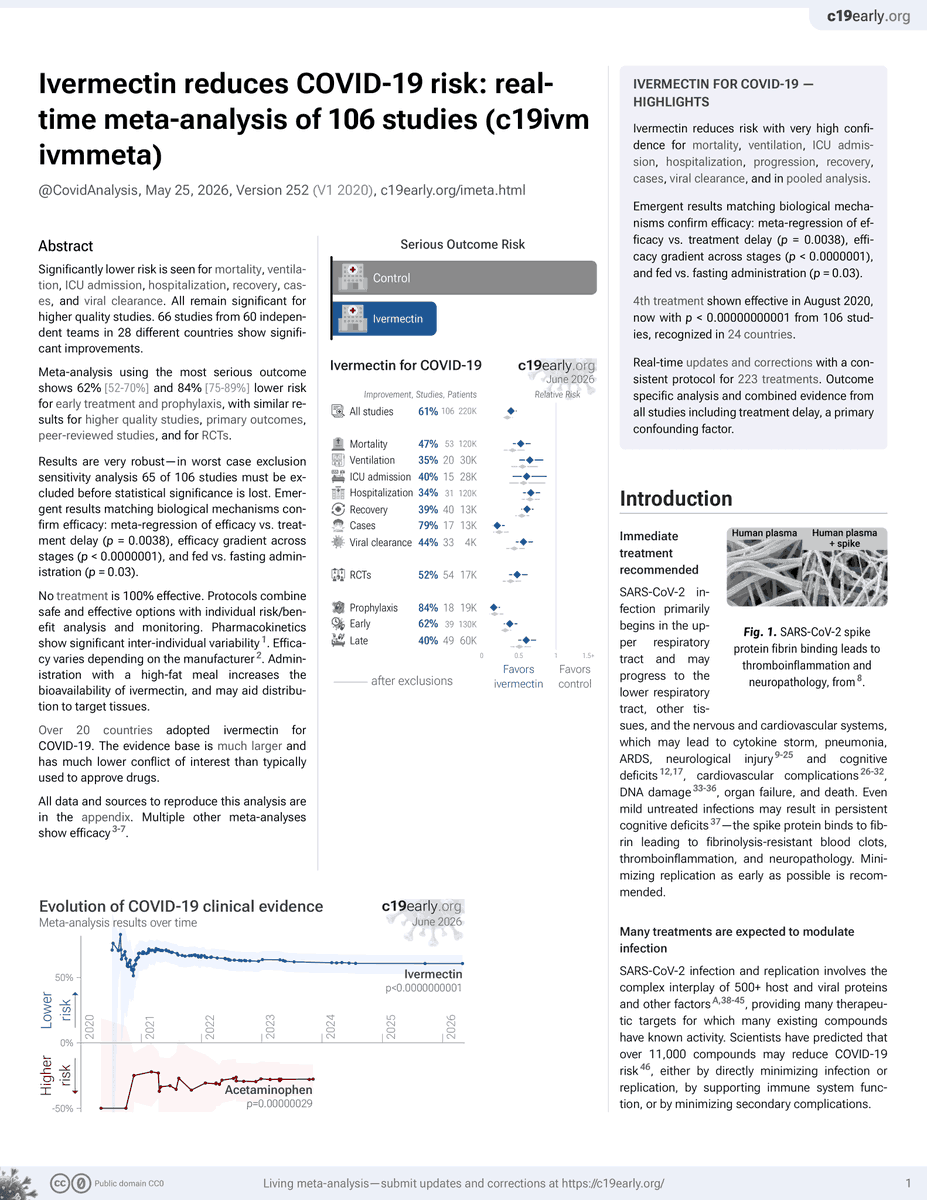
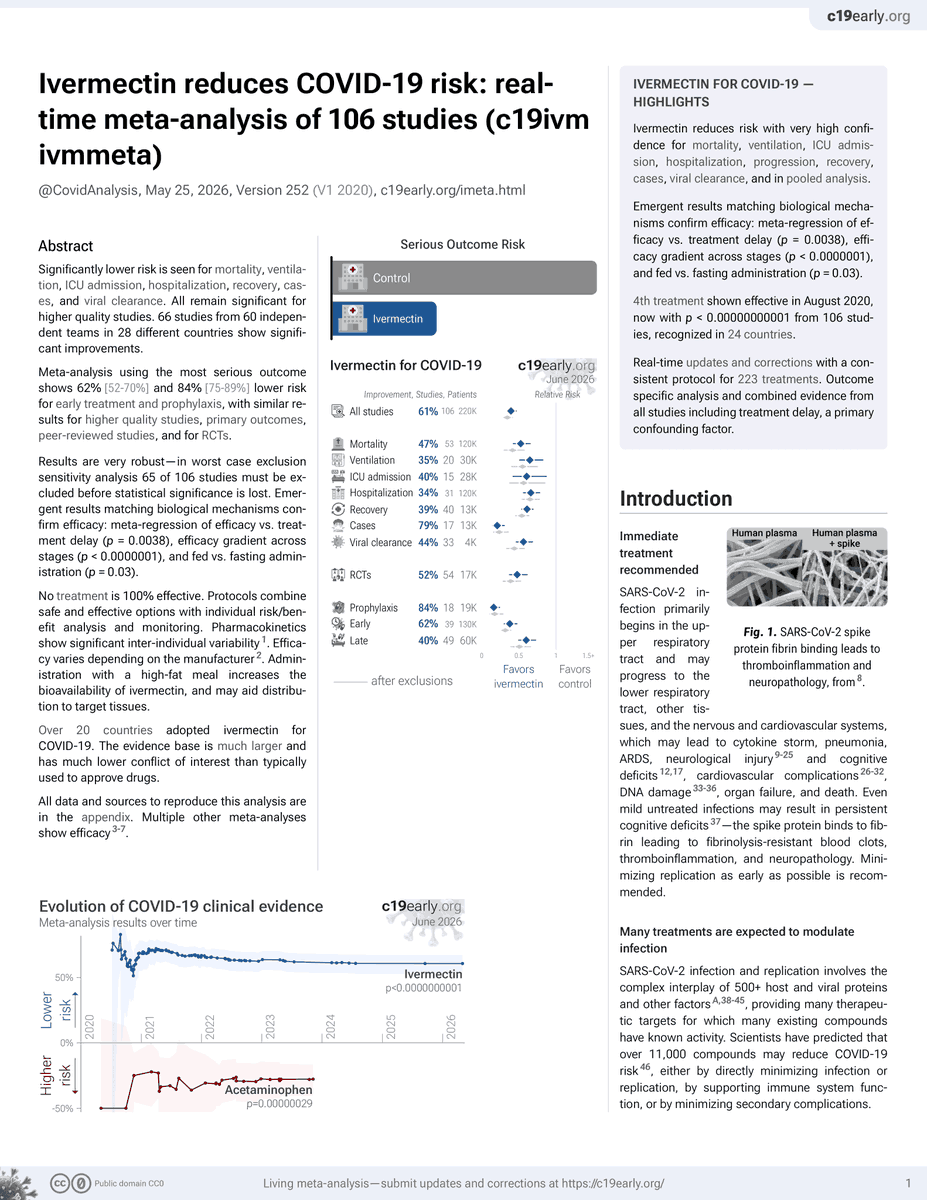
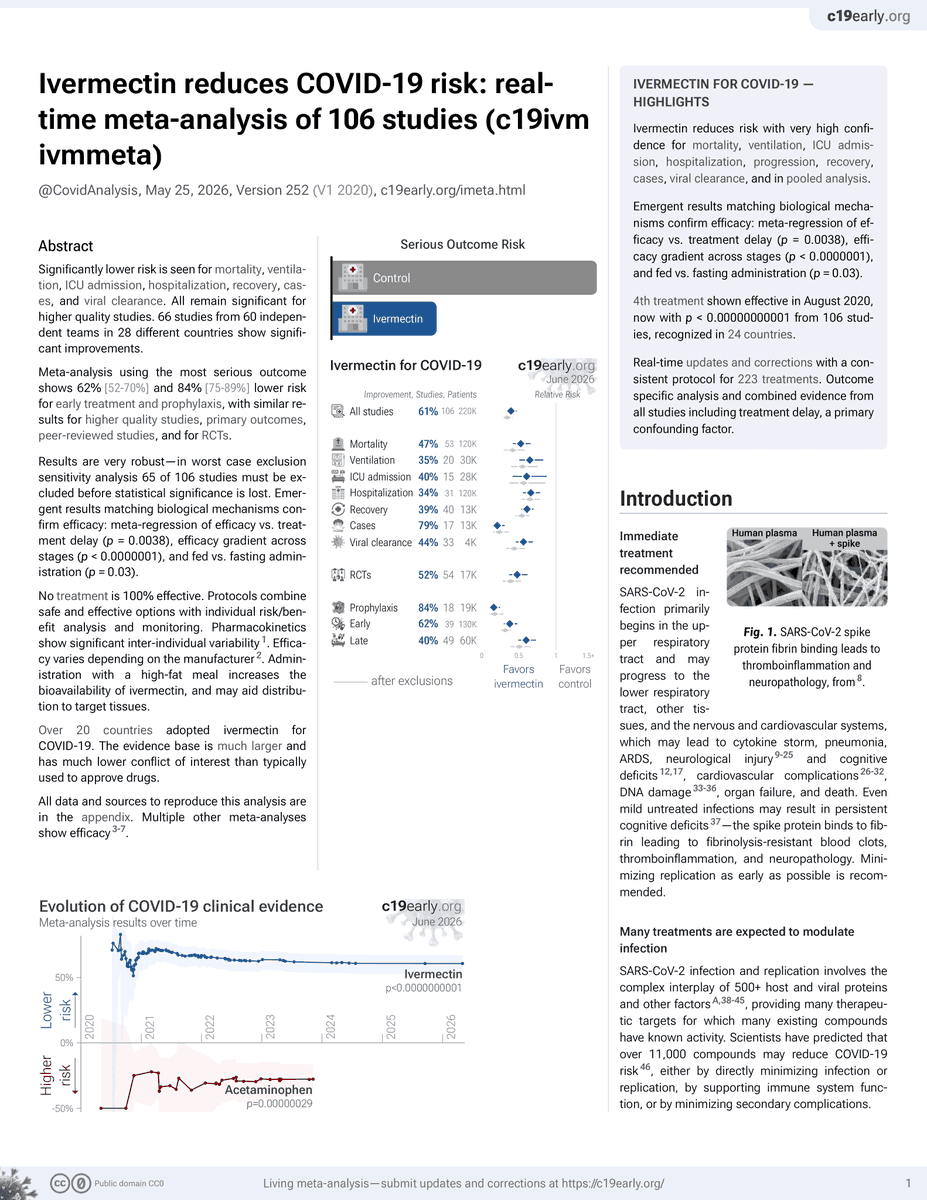
66 studies in 28 countries show significant efficacy (many more positive w/o significance).
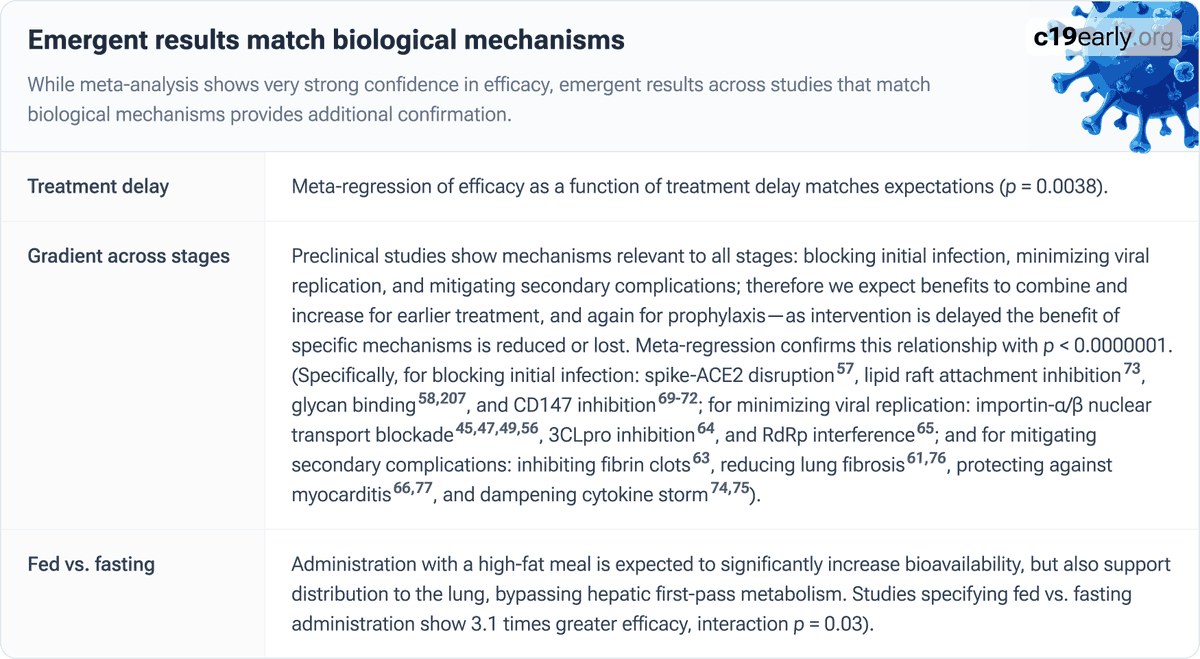
Results across studies match the biological mechanisms which confirms reliability: meta-regression of efficacy vs. treatment delay (p = 0.0038), efficacy gradient across stages (p < 0.0000001), and fed vs. fasting administration (p = 0.03).
This is not possible without a real treatment effect - it would require an unrealistic conspiracy where many well-respected teams in many countries conspire to harm humanity and coordinate fraudulent results.
The last refuge of those that made a mistake here is to simply claim all 66 studies showing significant efficacy are garbage, without even reading them. But this doesn't work - you need to explain how the variation in results across studies matches the biological mechanisms.
Social pressure was extreme, as Scott Alexander said: "if you say anything in favor of ivermectin you will be cast out of civilization and thrown into the circle of social hell ... All the health officials in the world will shout 'horse dewormer!' at you..." This led to remarkable actions, for example nobody would think that 36% lower risk of long-term morbidity from COVID-19 is not meaningful, but the authors of the Oxford study actually claimed this ("unlikely" to be "clinically meaningful").
If you believe there is no efficacy, answer these two questions:
- Do you consider 36% lower long-term morbidity clinically meaningful (100 million people according to common long COVID estimates)?
- Do you think the above conspiracy is real, or have another explanation for the emergent results across studies that match the biological mechanisms?
—
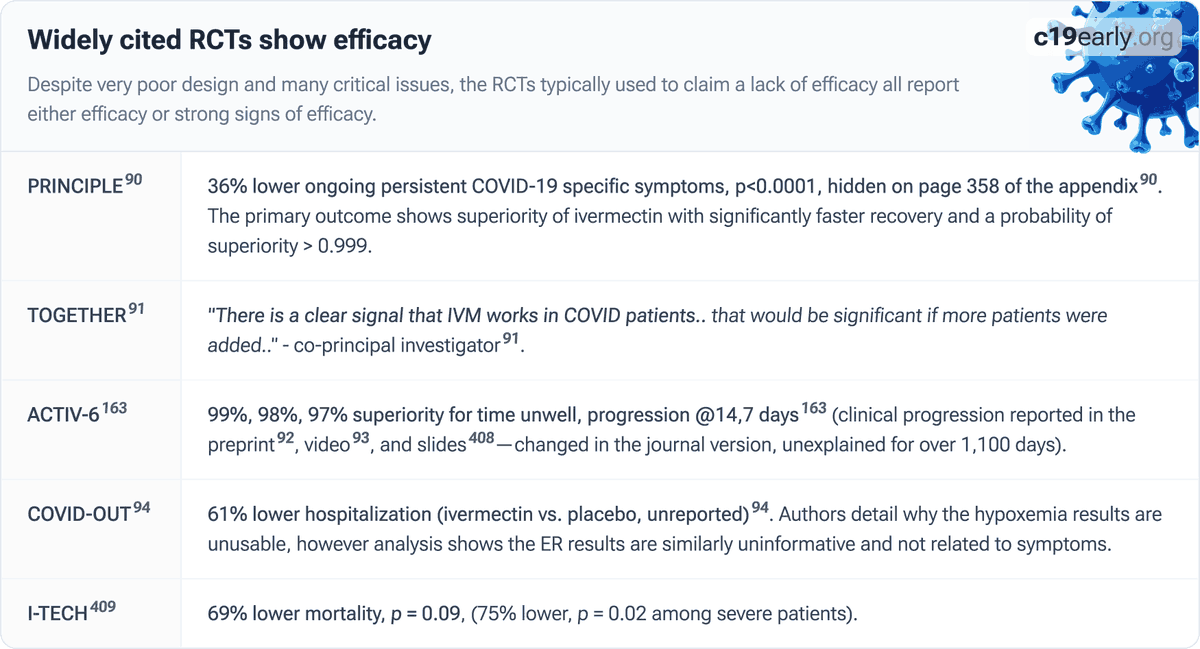
PRINCIPLE: significantly faster recovery and 36% lower long COVID, p < 0.0001 (pre-specified ongoing persistent COVID-19 symptoms combined with meta-analysis, data on page 358 in the appendix). This is remarkable given the design for failure: very late, low-dose, incorrectly administered, truncated treatment with low-risk patients. Results were withheld for 600 days until 2024.
ACTIV-6: 99%, 98%, 97% superiority for time unwell, progression at 14 and 7 days - reported in the preprint, video, and slides - changed in the journal version, unexplained for over 1,300 days.
COVID-OUT: 61% lower hospitalization (ivermectin vs. placebo, unreported). Authors detail why the hypoxemia results are unusable, however the data shows the ER results are similarly uninformative and not related to symptoms. They deleted the symptom recovery outcome. We can create it from the data - it shows the opposite of what they claim.
Two of these trials are from a Russia conspiracy theorist - perhaps not the most reliable source. He claims our analysis of 6,000 studies for 223 treatments is Russian propaganda despite it being clear that we are in the US (and X also now shows locations).
c19early.org/imeta.html#tldr
1
3
8
783
Two major confounding issues in many real-world paxlovid studies are confounding by contraindication and healthy-user bias:
🔴 Studies that do not (or only partly) exclude contraindicated patients in the control group overestimate efficacy due to the preferential inclusion of higher risk patients in the control group.
🔴 Studies that do not account for healthy-user bias also overestimate efficacy because patients seeking out and receiving paxlovid are also more likely to use other beneficial non-prescription treatments or interventions.
The FDA largely disregards both of these - their key selection criteria was handling index time selection. All five of the FDA selected studies are subject to significant healthy-user bias, 3 of 5 do not exclude contraindicated patients, and one does so only partially.
accessdata.fda.gov/drugsatfd…
accessdata.fda.gov/drugsatfd… ⬇️
1
2
284
Analyzing new studies in real time can provide key real-world and lower-conflict-of-interest evidence, and is also important for COVID because SARS-CoV-2 evolves - treatment efficacy can vary significantly across variants.
Should the FDA analyze evidence in real-time?
75%
Yes
25%
No
4 votes • Final results
1
4
219
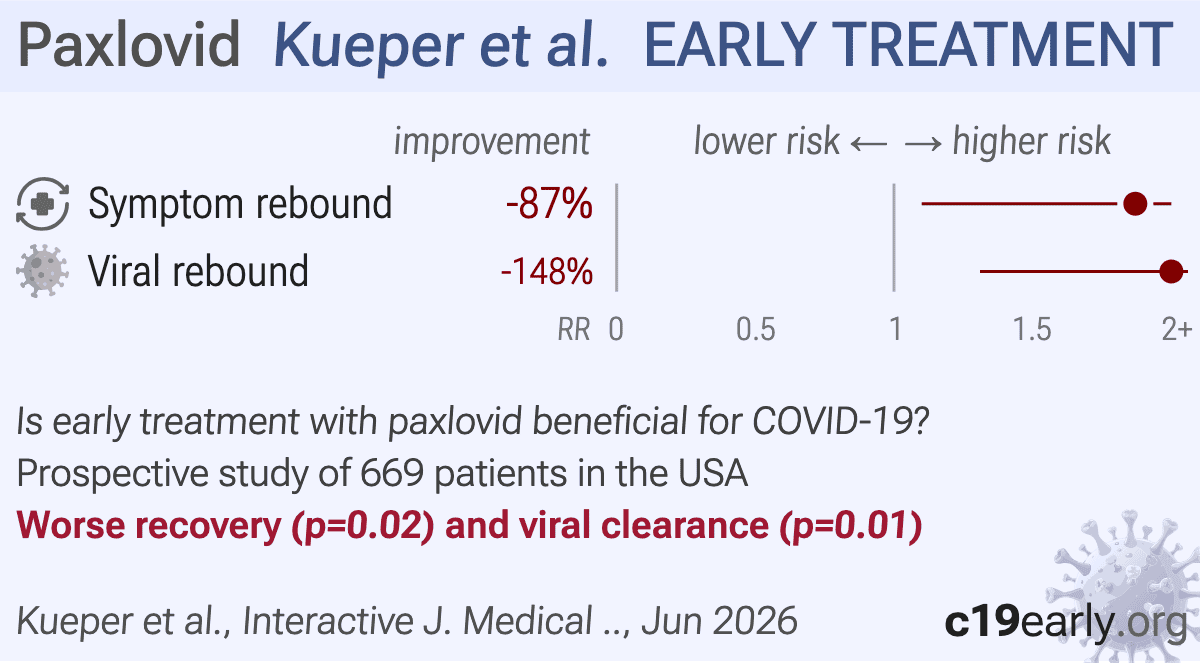
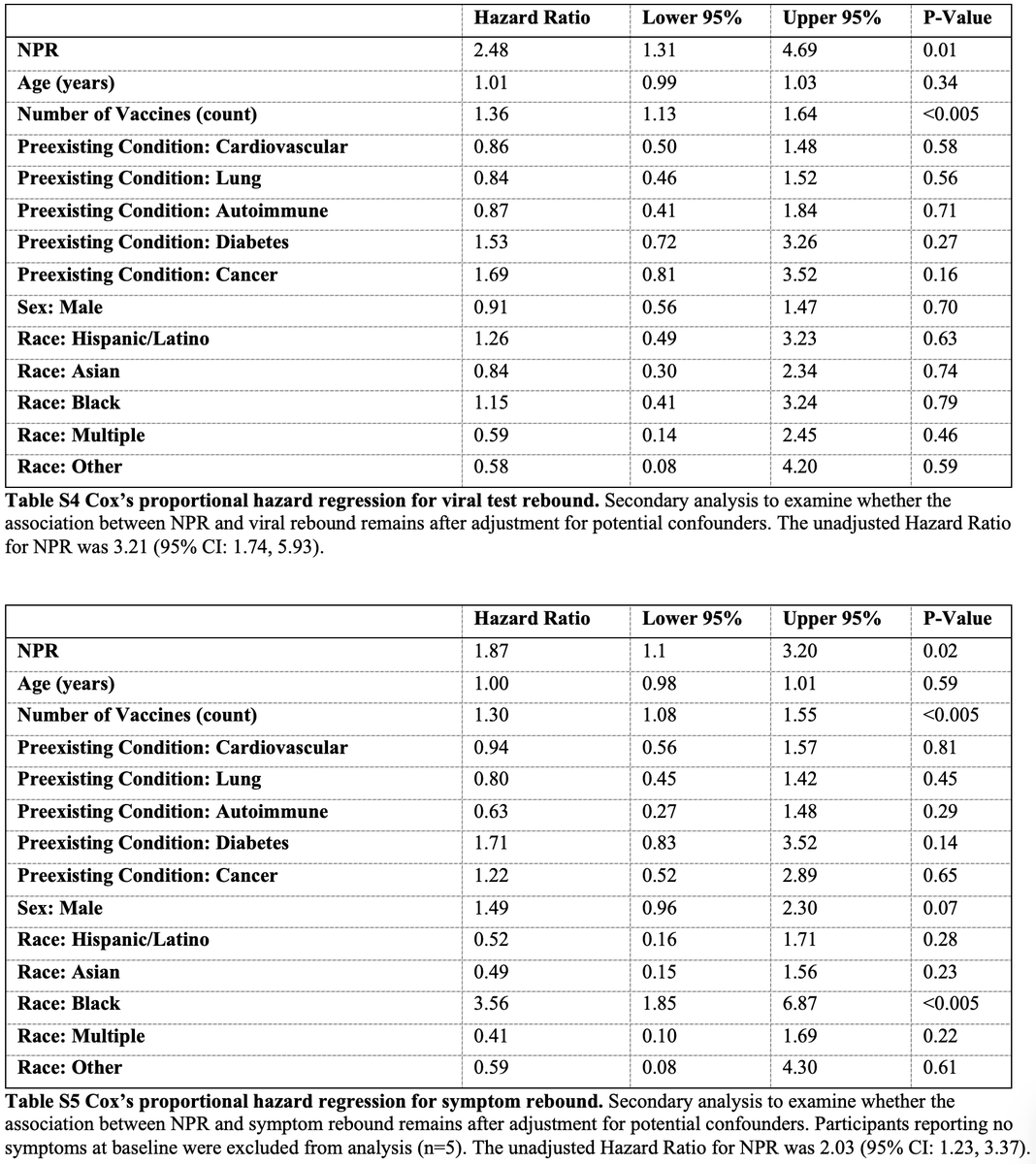
🔴 A recent study shows significantly higher risk of symptom and viral rebound with paxlovid.
What did the FDA say about these results? ⬇️
1
8
20
1,530
Study: c19early.org/kueper.html
Nothing from the FDA - generally they do not analyze new independent studies after approval, with limited exceptions.
In 2023 they reviewed 5 studies. The review's analysis of confounding is biased toward results beneficial to Pfizer. ⬇️
1
4
423
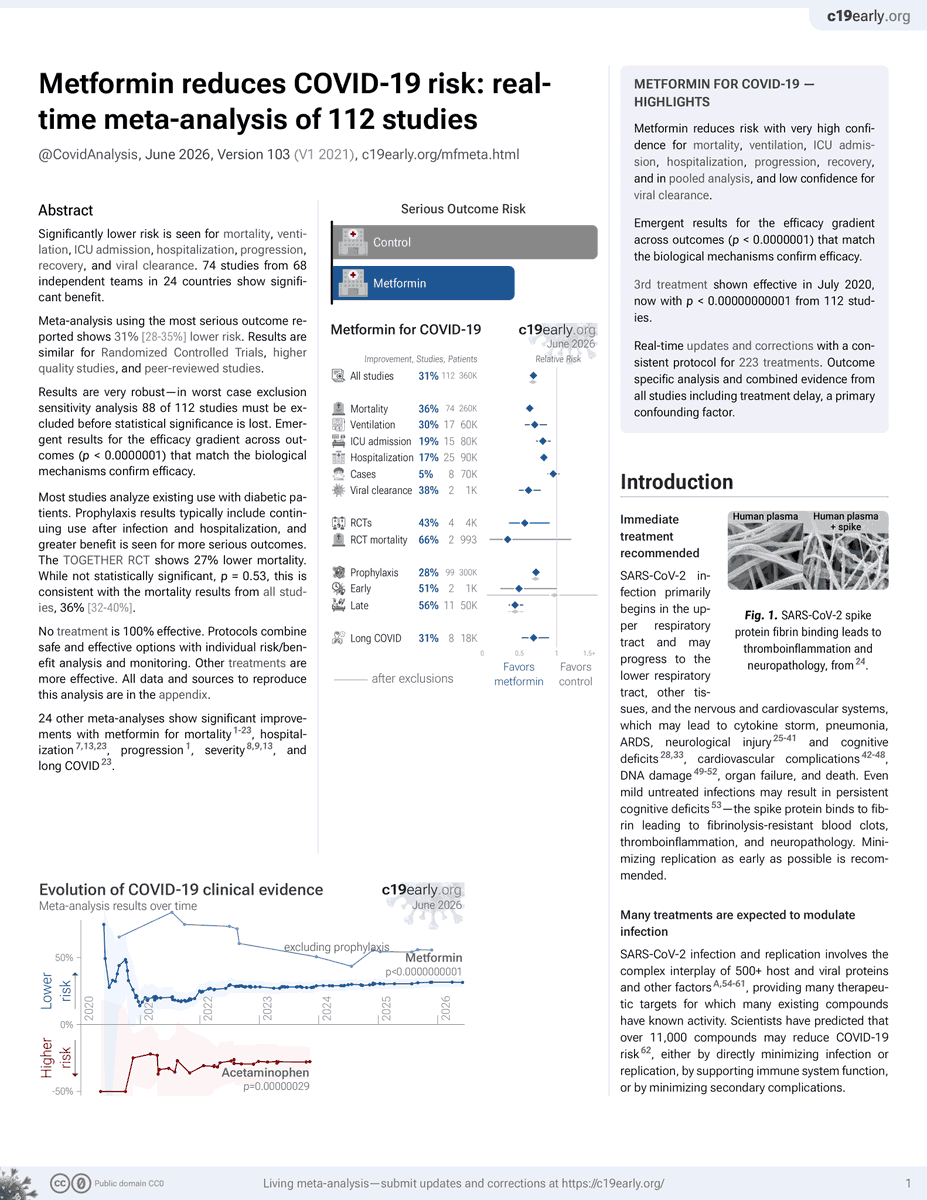
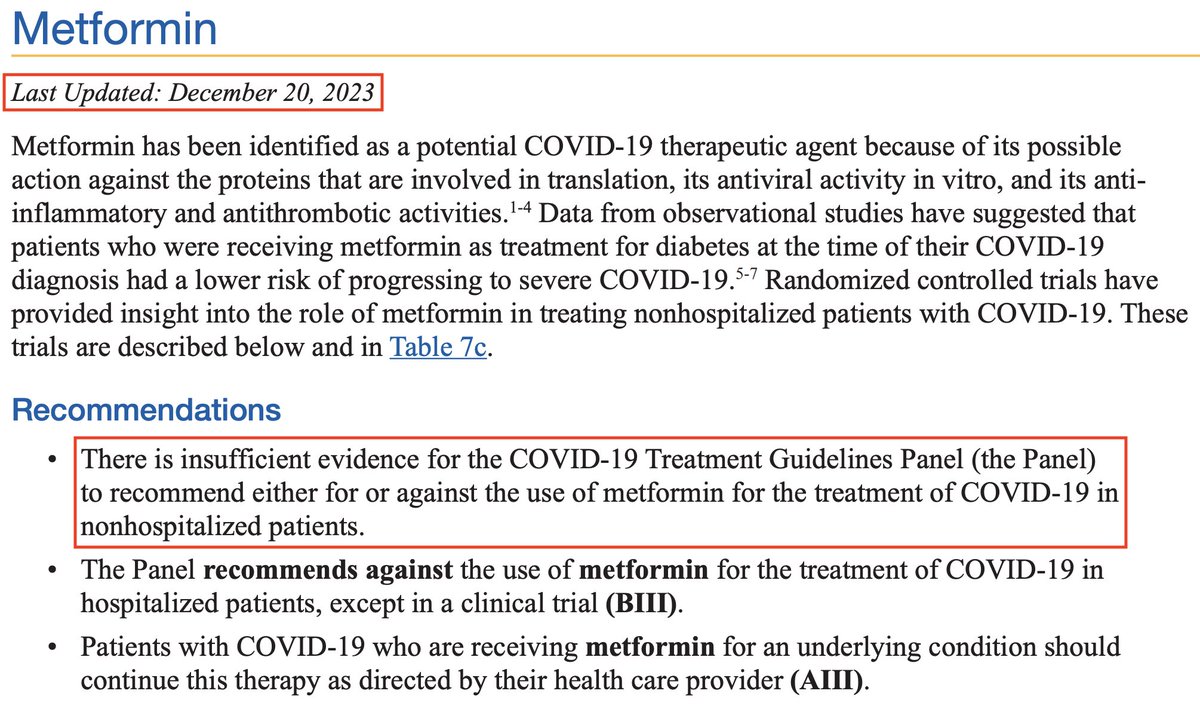
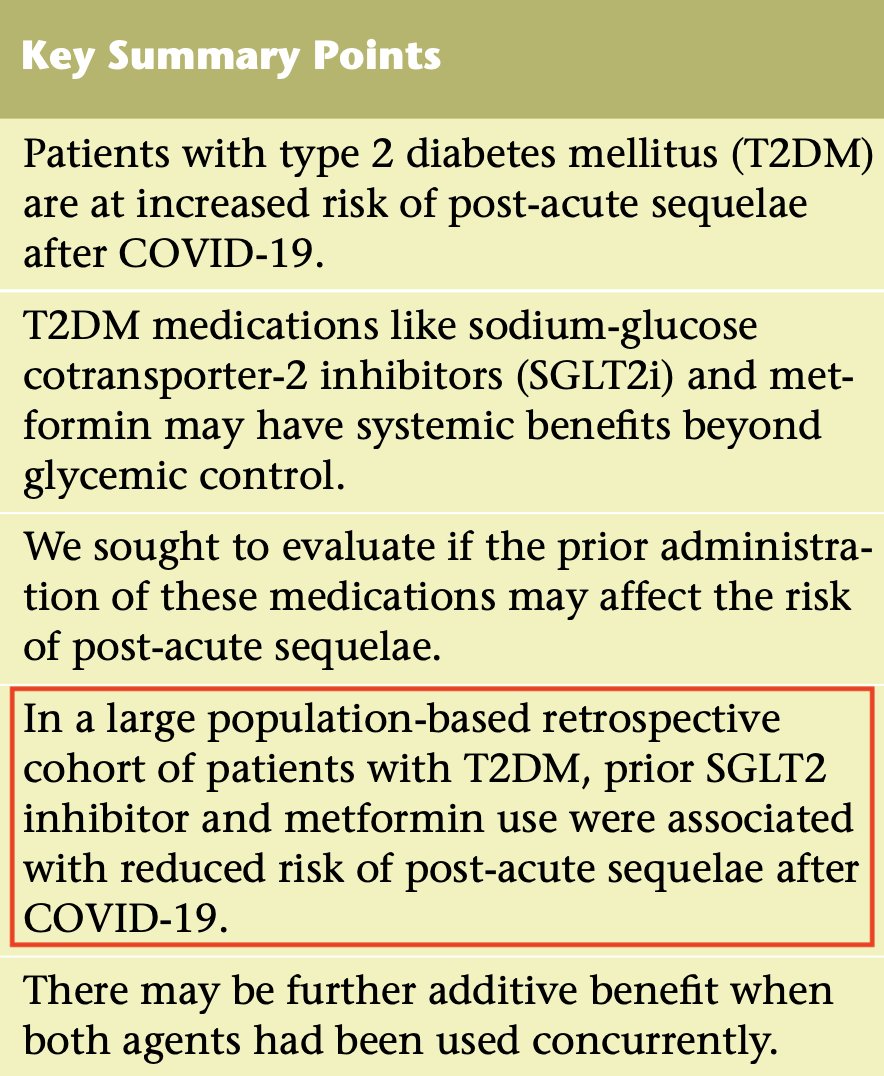
Lower risk of long COVID with metformin: c19early.org/ngiam2.html
This is the 112th study - meta-analysis shows significantly lower COVID-19 risk with metformin (p < 0.0000001).
NIH is behind - they claim "insufficient evidence", but have only looked at 4 studies, with no updates since 2023. ncbi.nlm.nih.gov/books/NBK57…
3
9
326
Covid Analysis: 200 COVID-19 treatments retweeted
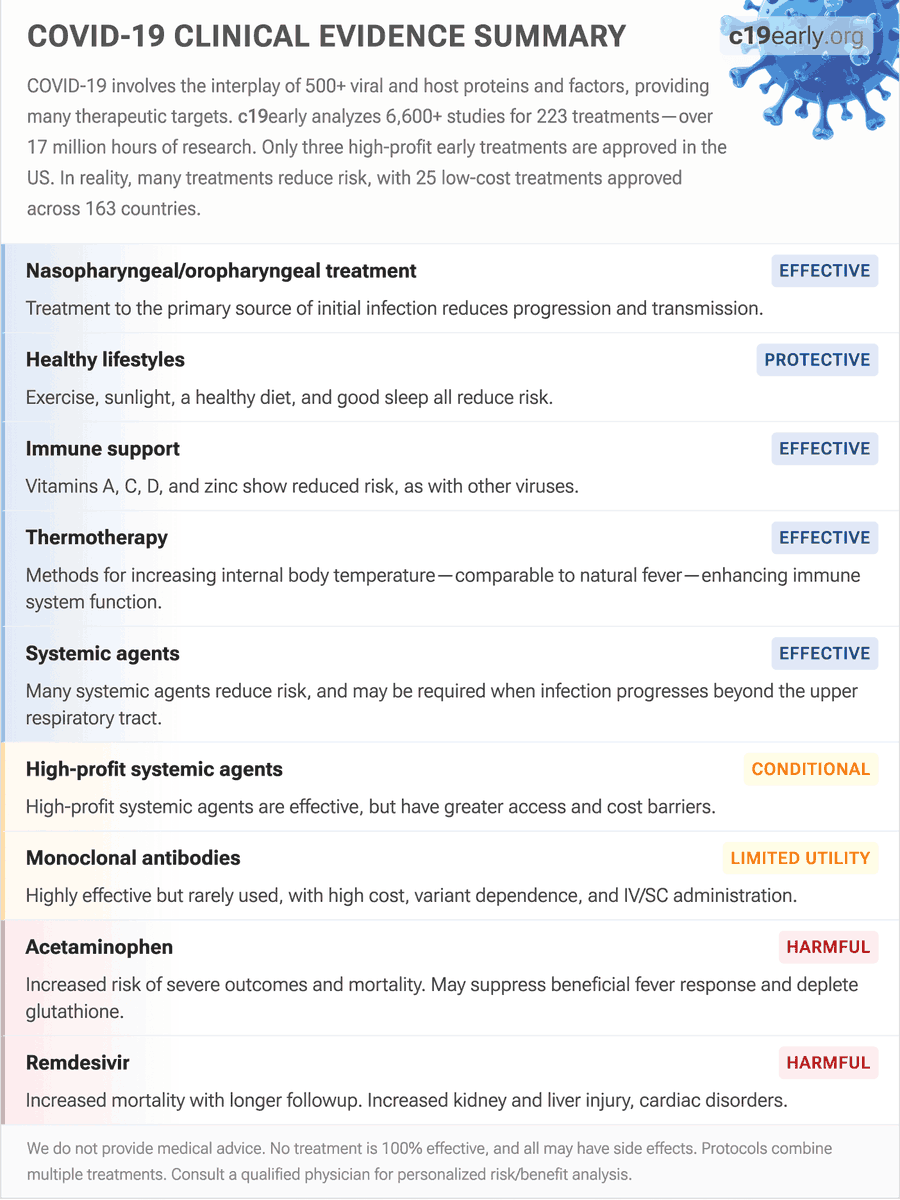
25 low-cost treatments were approved in other countries. None were approved in the US.
For most treatments, US authorities did not review the evidence. A few had belated minimal reviews that typically concluded "insufficient evidence" while ignoring most of the studies. The FDA rejected one while admitting that they did not review any of the studies.
Real-time proactive review of treatment evidence is required - not just for COVID-19, but for all diseases.
Failure to proactively analyze data in real time guarantees delayed recognition of efficacy or harm, by which time moral, legal, career, and reputational liabilities strongly disincentivize any admission of error.
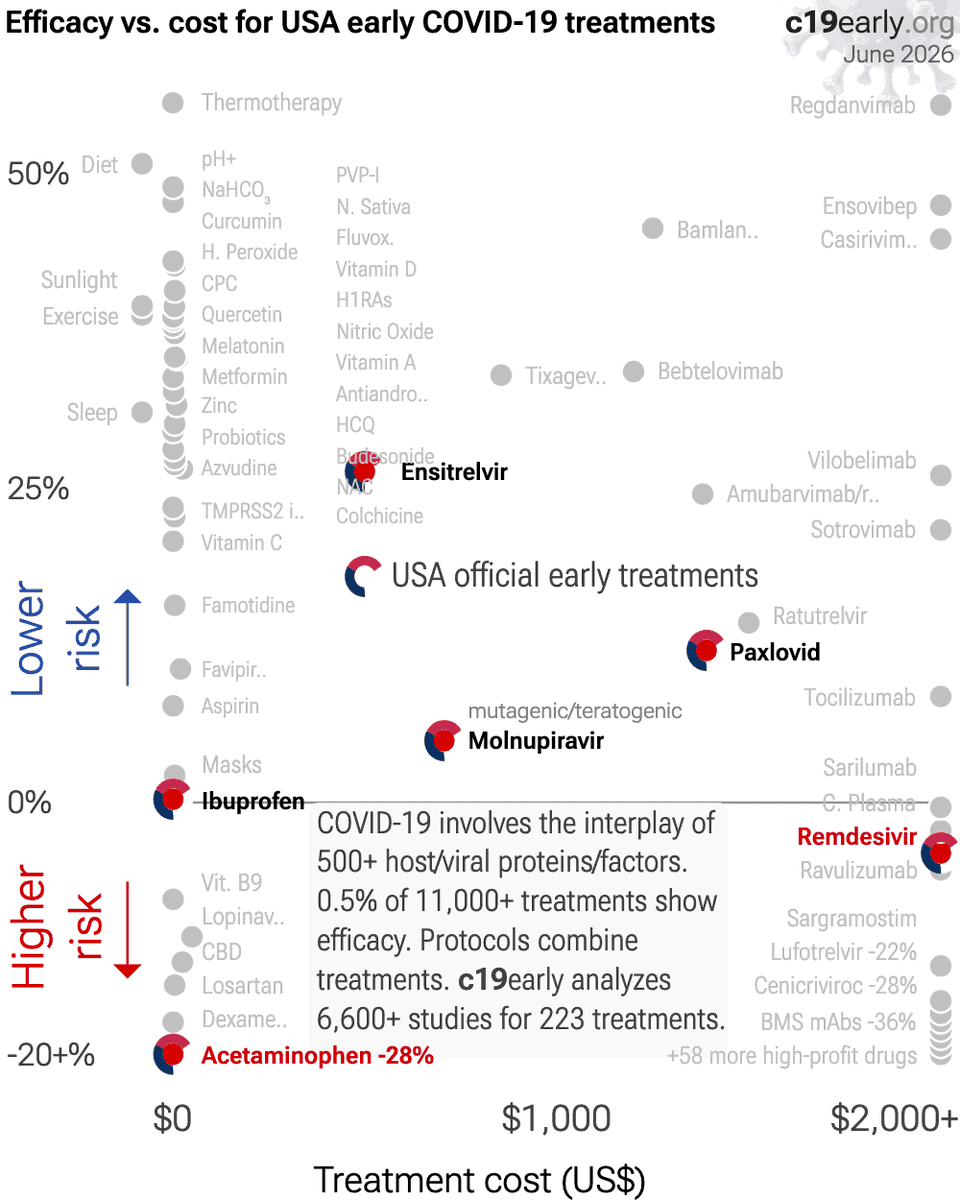
Analysis of 223 COVID-19 treatments: c19early.org/
3
13
549
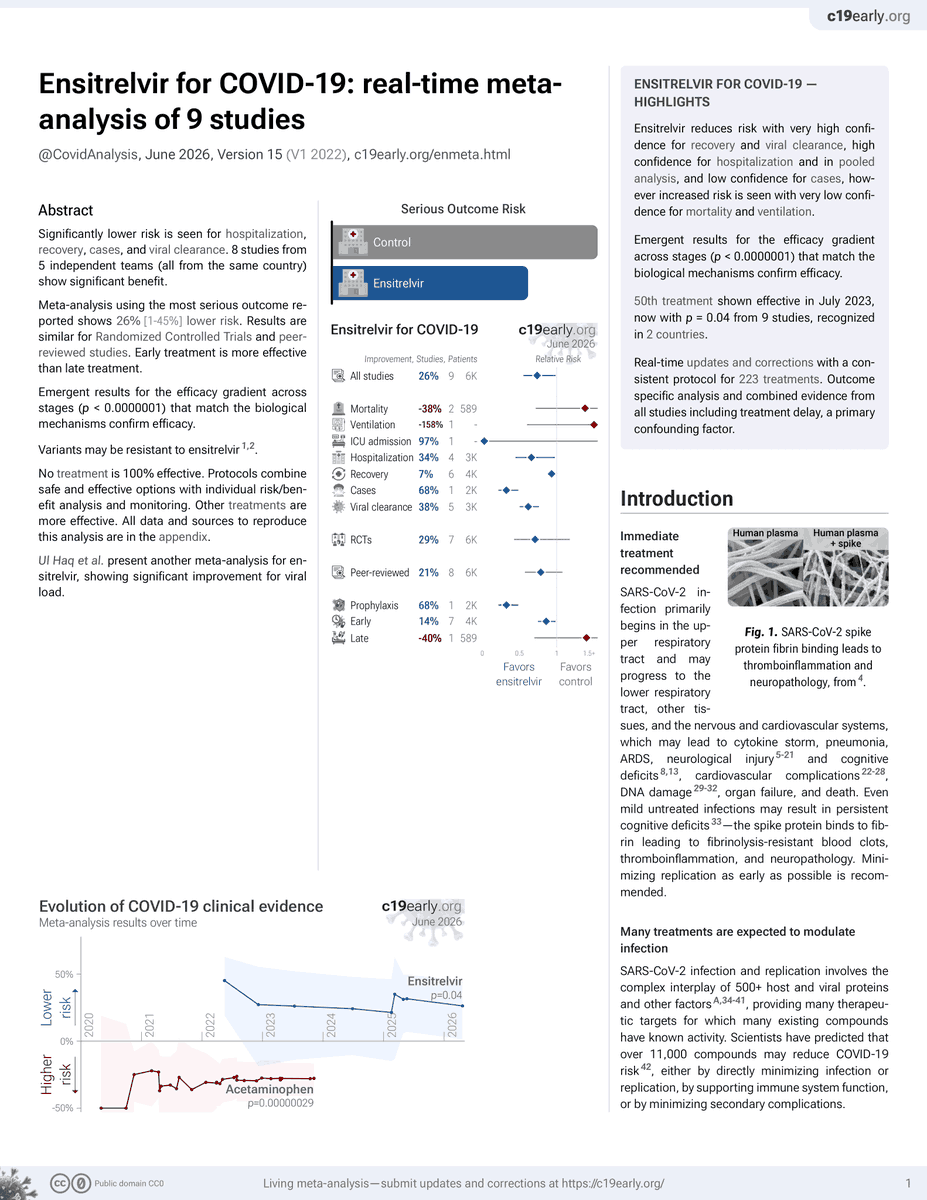
The FDA approved ensitrelvir for COVID-19.
4 years late. Ensitrelvir was known effective and approved in Japan in 2022.
Ensitrelvir is an older-generation 3CLpro inhibitor - avoiding ritonavir but with its own inherent CYP3A inhibition.
There are more effective, safer, and less-expensive COVID-19 antivirals, including newer-generation 3CLpro inhibitors, however this is the FDA’s best approval to date.
1
1
4
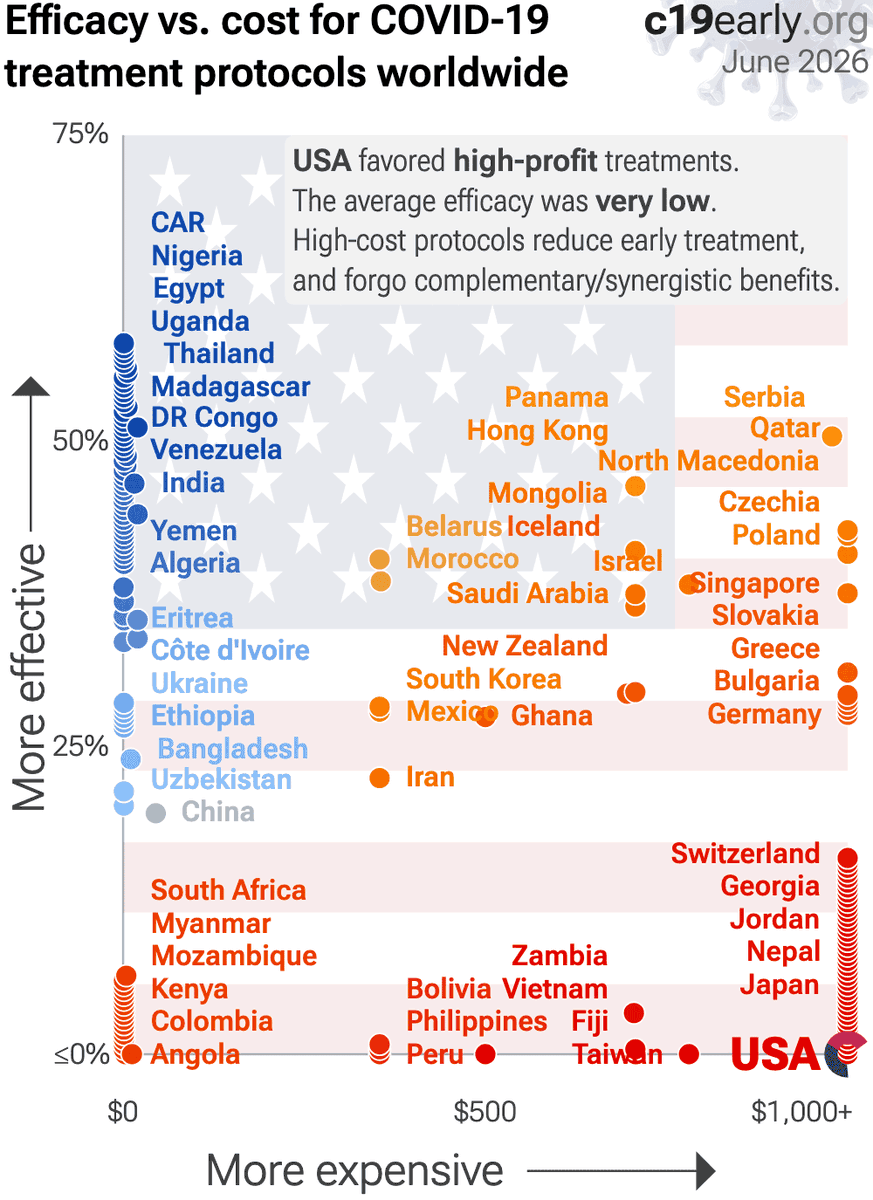
412
Official protocols varied widely around the world. USA has more room for improvement.
c19early.org/soc/usa.html
2
183
Covid Analysis: 200 COVID-19 treatments retweeted
Actually this study points towards efficacy: 32% lower mortality for noncritical patients, despite greater baseline severity in the treatment group, very low dose, poor administration, and very late treatment.
In the critical group the baseline imbalance was severe, also pointing towards efficacy.
Adjustment for severity is required because of the response-adaptive randomization, is specified in the protocol and first post-completion SAP, but was deleted and not reported.
Details:
🔴 Severe baseline imbalance and no adjustment, despite being in the protocol and indicated by CONSORT. Randomization resulted in 58% more critical patients at baseline in the treatment group (38 vs. 24). Baseline APACHE II scores were higher in both critical and noncritical groups (11 vs. 9 and 7 vs. 6). 25% of critical treatment patients had APACHE II ≥17 while the corresponding value for the control group is 12. This is a severe imbalance - the difference in expected mortality for APACHE II 17 vs. 12 is about 2x. The PaO2/FiO2 medians show severe ARDS for treatment versus moderate ARDS for control.
🔴 Concurrent cohort results better. Table S7 shows results for the concurrent ivermectin-specific cohort which are notably better - 72.6% and 72.3% probability of superiority for survival. Failure to adjust for severity results in an underestimate. These results should be more accurate because the controls were randomized at the same sites in the same time window under the same conditions as the ivermectin patients, eliminating cross-domain and cross-period confounding that the pooled analysis must correct for through model assumptions about exchangeability across the broader REMAP-CAP cohort.
🔴 Inconsistent blinding claims. The second post-hoc SAP states that "The authors of this document are blinded to all individual data other than publicly disclosed results", however the authors include three members of the Statistical Analysis Committee (SAC). The SAC is described in the first post-hoc SAP as "unblinded to all interventions and domains as part of their role for REMAP-CAP" in order to run the analyses that updated response-adaptive randomization weights and evaluated statistical triggers. The reference to the SAC and its unblinded role was removed from the second SAP.
🔴 Model penalizes noncritical efficacy. Authors specify using a hierarchical prior that shrinks the estimates for critically and noncritically ill patients toward an overall intervention effect. However, because antivirals are mechanistically expected to be more effective early in the disease course and may be ineffective when used during very late-stage critical illness, mathematically pooling these biologically distinct populations will attenuate a genuine early treatment benefit. This unfair penalization of the noncritical efficacy signal is compounded by the very small sample size and severe baseline imbalances in the critical cohort, which forces the model to rely heavily on a blended average, and is likely to obscure true phase-dependent treatment effects.
🔴 Claim of no analysis prior to second SAP impossible. The second post-hoc SAP claims "The SAP was subsequently revised (Version 2, 29 September 2023) before any analysis was conducted...", however REMAP-CAP is an adaptive platform trial that requires analysis to operate. For example, allocation ratios "were updated in May 2022 following an adaptive analysis to weight assignment to the intervention that appeared most favorable at that time" which requires outcome analysis, and the termination decision requires analysis. The platform-wide adaptive analyses run continuously throughout the trial by Berry Consultants update randomization weights based on ongoing outcome data. The first post-hoc SAP explicitly described this: "there will be analyses conducted by the Statistical Analysis Committee (SAC) using additional randomizations and unblinding of other randomizations. The SAC is unblinded to all interventions and domains."
🔴 Results withheld for years. Results were withheld for 553 days (end of followup to CCR24 presentation), with the more accurate concurrent ivermectin-specific analysis being withheld for 1,247 days (end of followup until journal publication).
🔴 Inappropriate termination. The trial was terminated early when the concurrent ivermectin-specific analysis showed 72.6% and 72.3% probability of superiority for the critical and noncritical groups respectively, percentages that underestimate superiority at the time due to failure to adjust for baseline severity.
🔴 Remdesivir use. Remdesivir use was higher in the treatment group which adds risk given the ICU population and 90 day outcomes. Meta regression with followup duration for remdesivir shows declining efficacy with harm past ~60 days followup, which may reflect antiviral efficacy being offset by side effects. Authors do not adjust for remdesivir use. The journal paper confirms this - Tables S8 and S9 show better results for patients not treated with remdesivir.
🔴 Allocation inconsistency. According to Table S2, the adaptive randomization proportion for ivermectin began at 1.0:1.0 and was subsequently updated to 1.0:2.0 in May 2022, however the results report >60% allocated to ivermectin which is inconsistent.
🔴 Expected failure based on design. In the protocol authors note that previous trials used 0.2mg/kg - 0.6mg/kg and they note that a dose-response effect has been seen, however they chose the lowest dose, and further do not specify administration with food, indicating a design favoring failure. The presentation acknowledges that the dose is too low and not expected to be effective. They also note poor absorption in severe disease and presence of ileus, exarcerbated in critical illness, and they note studies show improved absorption with ivermectin oral solution. However, administration was done with tablets dissolved in water, which is noted to be a poor choice.
🔴 Design for ICU patients - inappropriate outcome. The organ support-free days (OSFD) primary outcome was designed for ICU patients. The outcome assumes patients start at risk of needing organ support and the question is whether they receive it and how long. For a critically ill ICU patient already on organ support, this makes immediate sense - every day off support is a day of recovery. For a non-ICU ward patient on supplemental oxygen, the outcome is more degenerate: most of these patients will never need organ support regardless of treatment, so the OSFD scale collapses toward the maximum (22) for most patients. Looking at Table 2, the median OSFD for noncritically ill patients is 22 in both arms. Figure 3B confirms 68-70% of noncritically ill patients were at the ceiling. The posterior probability of superiority on this outcome is computed from a sample that is ceiling-dominated.
🔴 32% lower mortality for noncritical patients. While authors describe the result as negative, there was 32% lower mortality for noncritical patients, despite greater baseline severity in the treatment group, very low dose, poor administration, and very late treatment.
Preliminary analysis - send us updates/corrections. Additional issues: c19early.org/hashmi.html

1
1
5
279
The ANTICOV trial tested early treatment with HCQ, ivermectin/ASAQ, and fluoxetine/budesonide
(83, 182, and 143 patients).
All arms were terminated early. No paper to date.
How many primary outcome progression events were there across these arms? (n/408 vs. control 9/817) ⬇️
100%
0
0%
2
0%
4
0%
6
1 votes • Final results
1
2
319
Covid Analysis: 200 COVID-19 treatments retweeted
RCTs remove and add bias. Sometimes better. Sometimes worse.
Examples:
- RCTs for paxlovid are biased because they exclude patients at DDI risk better than real-world use.
- RCTs add enrollment delay. Consider a low-cost treatment for an acute respiratory infection - real-world use may be to have it on hand and take it immediately on symptoms. An RCT might treat patients days after symptoms, with results providing no information on immediate use.
In some domains, observational studies have low value, e.g., nutrition where adjusting for confounding factors is very difficult. In some domains, RCTs are not practical or ethical, or may add substantial bias.
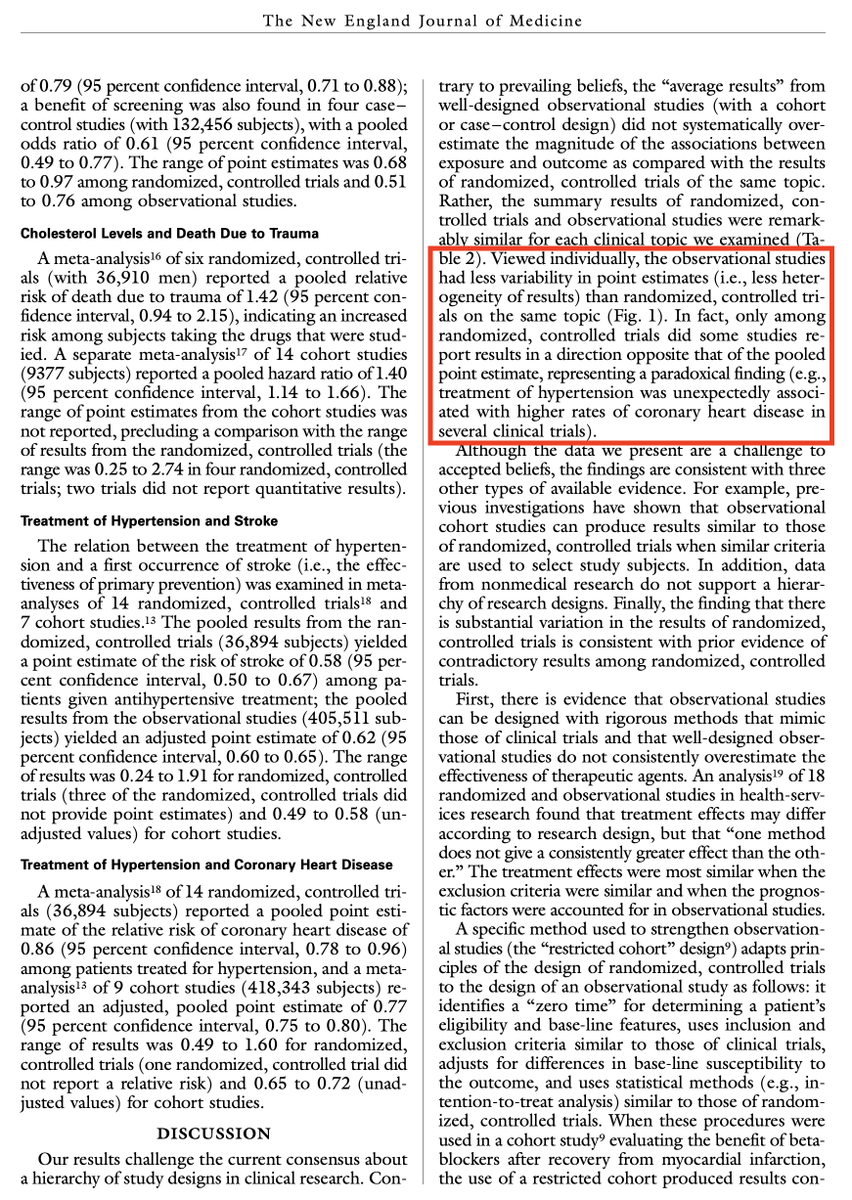
Three large comparisons show no systematic difference in results for RCTs and observational studies. Well-designed studies are possible in both cases for many domains, but in general both RCTs and observational studies can have bias ranging from minimal to extreme; and factors other than RCT/observational may be more important.
nejm.org/doi/full/10.1056/NE…
cochranelibrary.com/cdsr/doi…
c19early.org/rctobs.html
RCTs are easier to evaluate, but all studies must be carefully evaluated for many potential issues. While observational studies require greater expertise to analyze, the advantages in practicality, cost, time, and ethics are substantial.


1
1
3
295
Covid Analysis: 200 COVID-19 treatments retweeted
Ensitrelvir was approved in Japan in 2022. This trial released results in 2024.
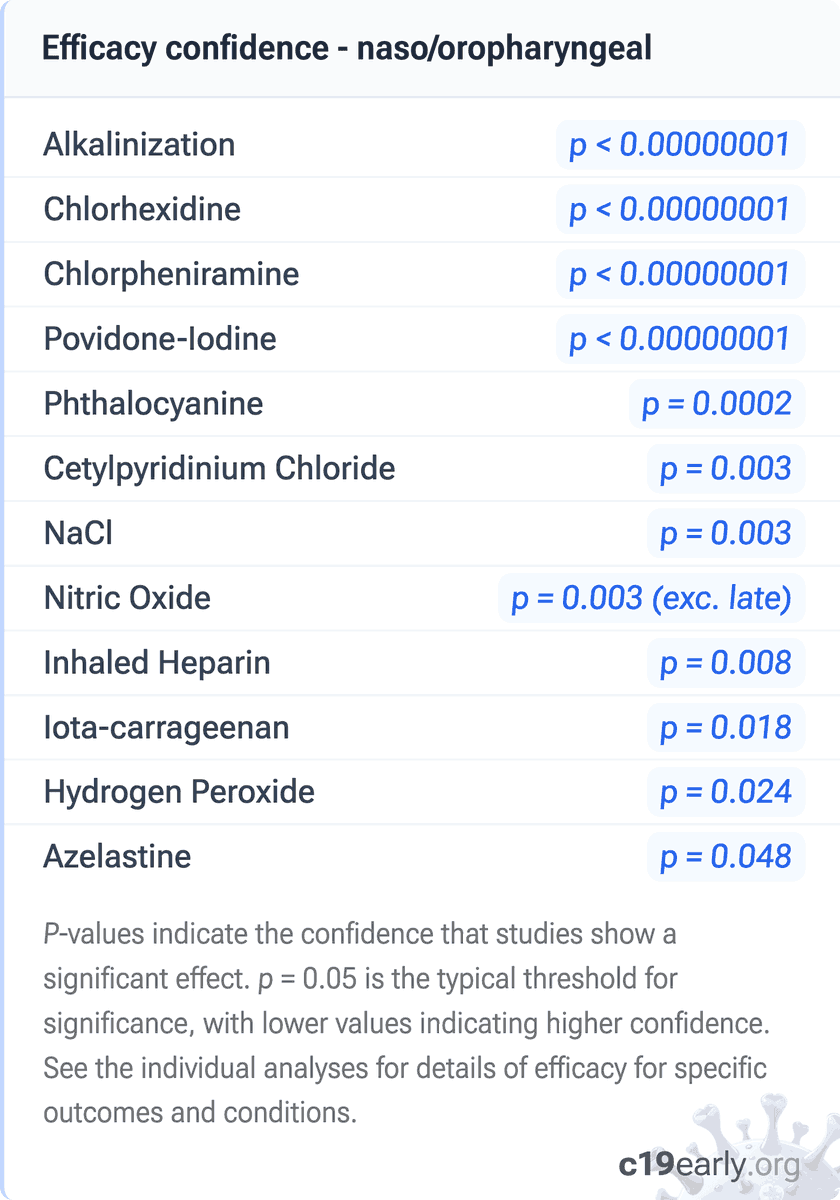
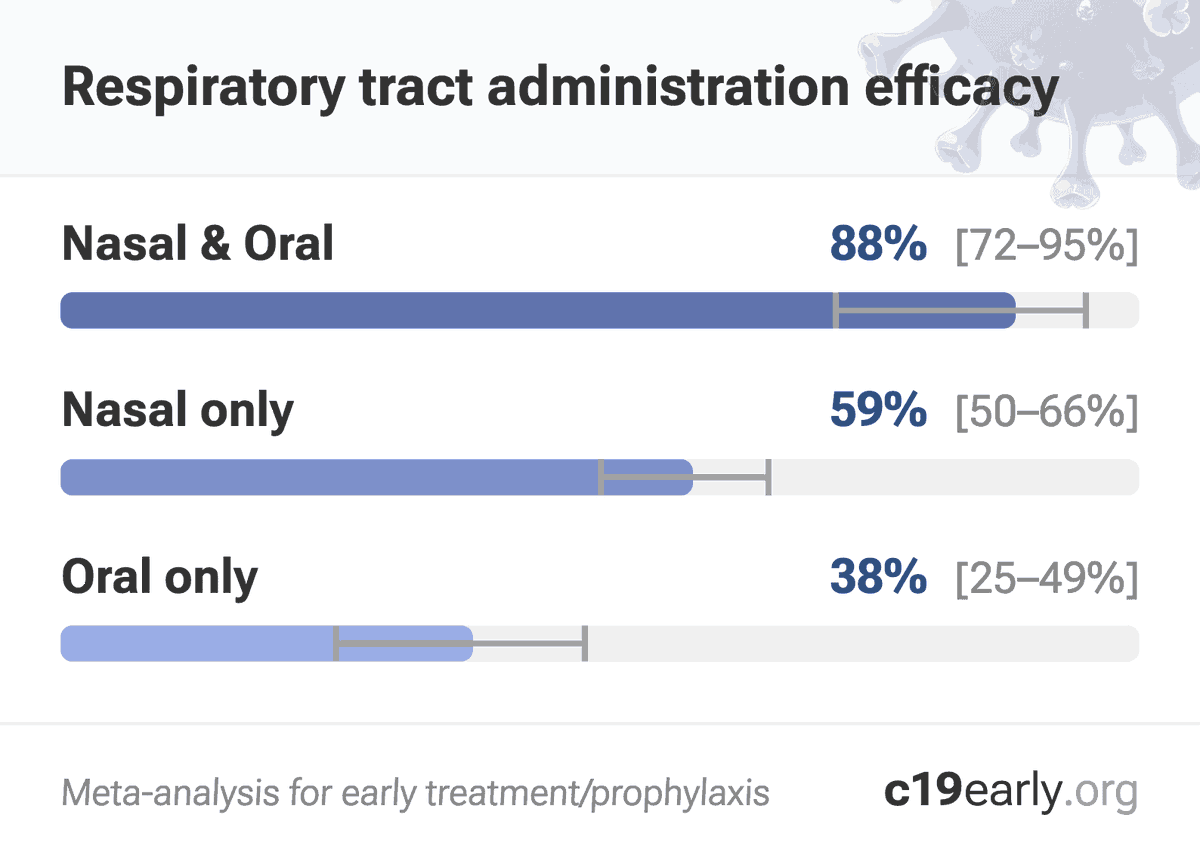
Many treatments show efficacy for prophylaxis.
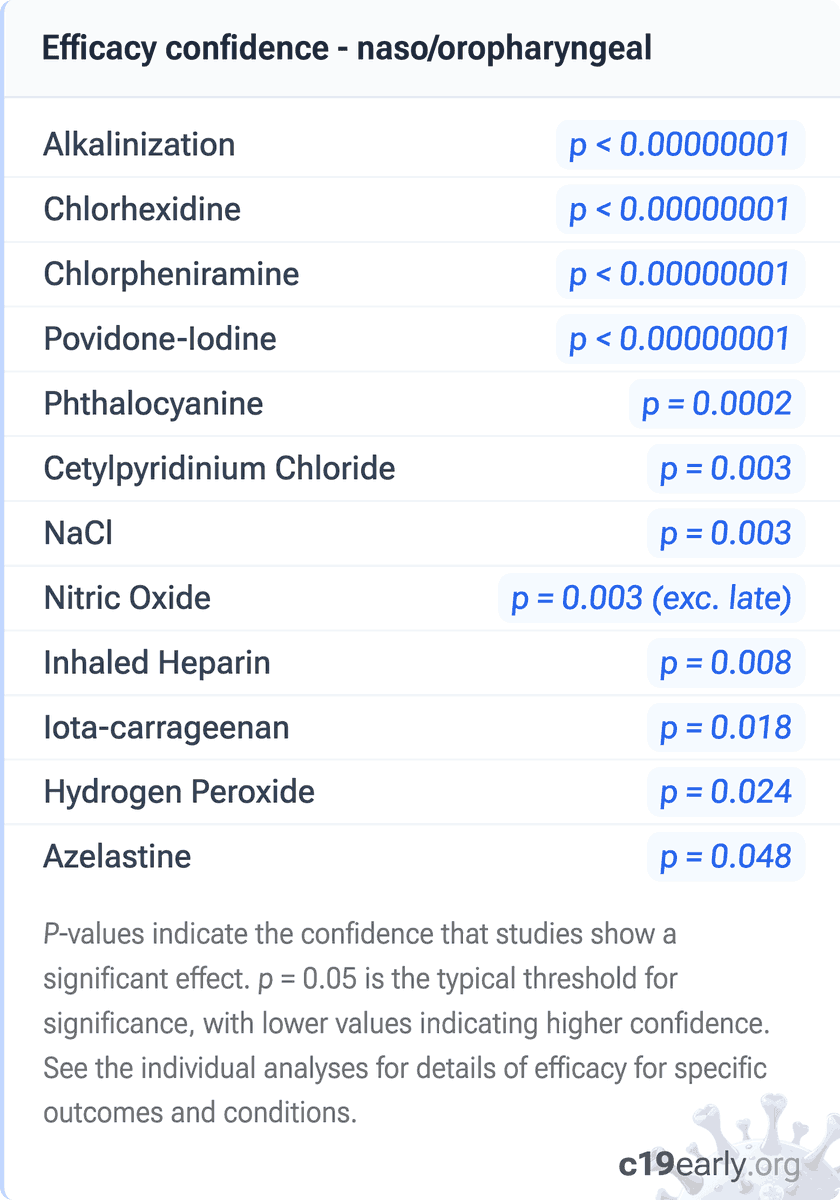
Extensive clinical data, including 65 randomized controlled trials, shows lower risk with several nasal and oral sprays/rinses, including several prophylaxis trials. Mechanisms of action include virucidal effects, blocking viral attachment, creating a physical barrier, physical removal, and enhancing mucociliary clearance. Combined nasal and oral application is most effective. c19early.org/rtadmin.html
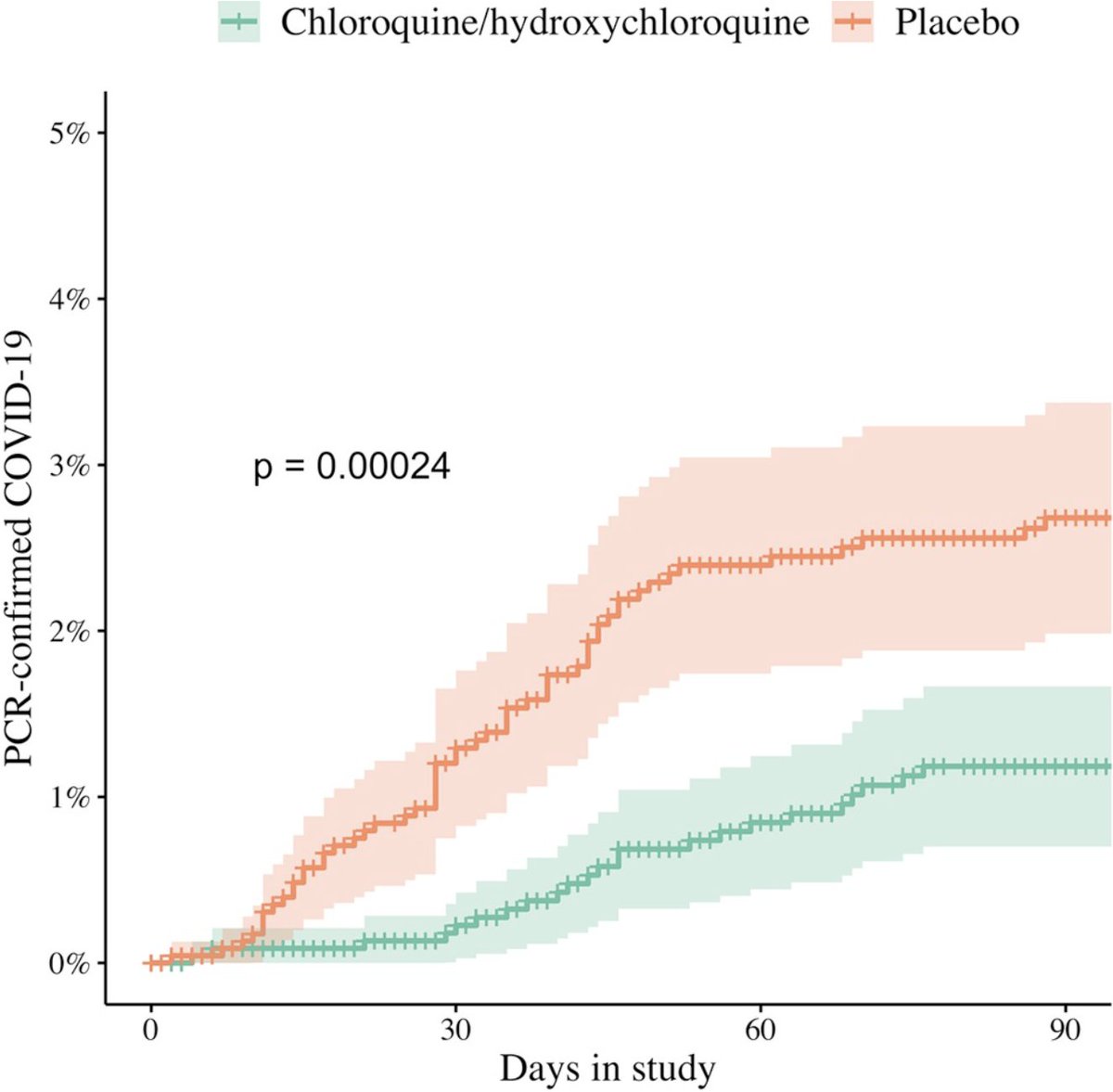
As another example, the largest HCQ/CQ RCT (Oxford COPCOV) shows 57% lower symptomatic PCR COVID-19 (p = 0.0002). Oxford authors also included a meta-analysis of 8 RCTs confirming significantly lower symptomatic PCR cases. c19early.org/schilling3.html
Analysis of 221 treatments: c19early.org/
2
19
66
5,034
Covid Analysis: 200 COVID-19 treatments retweeted
Several critical issues:
- Severe baseline imbalance and no adjustment, despite being in the protocol and indicated by CONSORT. Randomization resulted in 58% more critical patients at baseline in the treatment group (38 vs. 24). Baseline APACHE II scores were higher in both critical and noncritical groups (11 vs. 9 and 7 vs. 6). 25% of critical treatment patients had APACHE II ≥17 while the corresponding value for the control group is 12. This is a severe imbalance - the difference in expected mortality for APACHE II 17 vs. 12 is about 2x. The PaO2/FiO2 medians show severe ARDS for treatment versus moderate ARDS for control.
- Concurrent cohort results better. Table S7 shows results for the concurrent ivermectin-specific cohort which are notably better - 72.6% and 72.3% probability of superiority for survival. Failure to adjust for severity results in an underestimate. These results should be more accurate because the controls were randomized at the same sites in the same time window under the same conditions as the ivermectin patients, eliminating cross-domain and cross-period confounding that the pooled analysis must correct for through model assumptions about exchangeability across the broader REMAP-CAP cohort.
- Inconsistent blinding claims. The second post-hoc SAP states that "The authors of this document are blinded to all individual data other than publicly disclosed results", however the authors include three members of the Statistical Analysis Committee (SAC). The SAC is described in the first post-hoc SAP as "unblinded to all interventions and domains as part of their role for REMAP-CAP" in order to run the analyses that updated response-adaptive randomization weights and evaluated statistical triggers. The reference to the SAC and its unblinded role was removed from the second SAP.
- Model penalizes noncritical efficacy. Authors specify using a hierarchical prior that shrinks the estimates for critically and noncritically ill patients toward an overall intervention effect. However, because antivirals are mechanistically expected to be more effective early in the disease course and may be ineffective when used during very late-stage critical illness, mathematically pooling these biologically distinct populations will attenuate a genuine early treatment benefit. This unfair penalization of the noncritical efficacy signal is compounded by the very small sample size and severe baseline imbalances in the critical cohort, which forces the model to rely heavily on a blended average, and is likely to obscure true phase-dependent treatment effects.
- Claim of no analysis prior to second SAP impossible. The second post-hoc SAP claims "The SAP was subsequently revised (Version 2, 29 September 2023) before any analysis was conducted...", however REMAP-CAP is an adaptive platform trial that requires analysis to operate. For example, allocation ratios "were updated in May 2022 following an adaptive analysis to weight assignment to the intervention that appeared most favorable at that time" which requires outcome analysis, and the termination decision requires analysis. The platform-wide adaptive analyses run continuously throughout the trial by Berry Consultants update randomization weights based on ongoing outcome data. The first post-hoc SAP explicitly described this: "there will be analyses conducted by the Statistical Analysis Committee (SAC) using additional randomizations and unblinding of other randomizations. The SAC is unblinded to all interventions and domains."
- Results withheld for years. Results were withheld for 553 days (end of followup to CCR24 presentation), with the more accurate concurrent ivermectin-specific analysis being withheld for 1,247 days (end of followup until journal publication).
- Inappropriate termination. The trial was terminated early when the concurrent ivermectin-specific analysis showed 72.6% and 72.3% probability of superiority for the critical and noncritical groups respectively, percentages that underestimate superiority at the time due to failure to adjust for baseline severity.
- Remdesivir use. Remdesivir use was higher in the treatment group which adds risk given the ICU population and 90 day outcomes. Meta regression with followup duration for remdesivir shows declining efficacy with harm past ~60 days followup, which may reflect antiviral efficacy being offset by side effects. Authors do not adjust for remdesivir use. The journal paper confirms this - Tables S8 and S9 show better results for patients not treated with remdesivir.
- Allocation inconsistency. According to Table S2, the adaptive randomization proportion for ivermectin began at 1.0:1.0 and was subsequently updated to 1.0:2.0 in May 2022, however the results report >60% allocated to ivermectin which is inconsistent.
- Expected failure based on design. In the protocol authors note that previous trials used 0.2mg/kg - 0.6mg/kg and they note that a dose-response effect has been seen, however they chose the lowest dose, and further do not specify administration with food, indicating a design favoring failure. The presentation acknowledges that the dose is too low and not expected to be effective. They also note poor absorption in severe disease and presence of ileus, exarcerbated in critical illness, and they note studies show improved absorption with ivermectin oral solution. However, administration was done with tablets dissolved in water, which is noted to be a poor choice.
- Design for ICU patients - inappropriate outcome. The organ support-free days (OSFD) primary outcome was designed for ICU patients. The outcome assumes patients start at risk of needing organ support and the question is whether they receive it and how long. For a critically ill ICU patient already on organ support, this makes immediate sense - every day off support is a day of recovery. For a non-ICU ward patient on supplemental oxygen, the outcome is more degenerate: most of these patients will never need organ support regardless of treatment, so the OSFD scale collapses toward the maximum (22) for most patients. Looking at Table 2, the median OSFD for noncritically ill patients is 22 in both arms. Figure 3B confirms 68-70% of noncritically ill patients were at the ceiling. The posterior probability of superiority on this outcome is computed from a sample that is ceiling-dominated.
- 32% lower mortality for noncritical patients. While authors describe the result as negative, there was 32% lower mortality for noncritical patients, despite greater baseline severity in the treatment group, very low dose, poor administration, and very late treatment.
Preliminary analysis - please send updates/corrections. Additional issues and details: c19early.org/hashmi.html
2
1
5
303
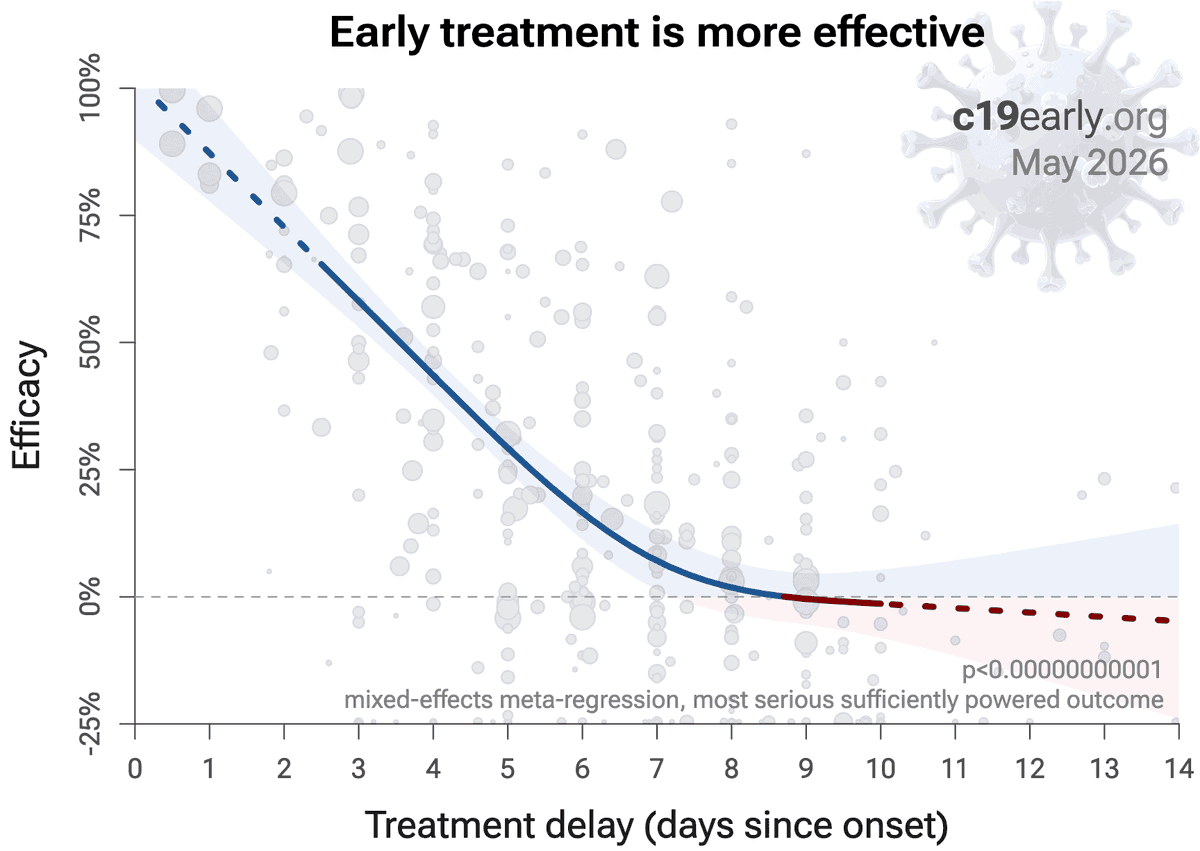
Ensitrelvir shows efficacy for treatment within 48 hrs, but no significant effect for delayed treatment (interaction p ≈ 0.02).
Consistent with analysis of 221 treatments - early treatment is more effective.
Prescription treatments have greater access barriers for early use.
May 13

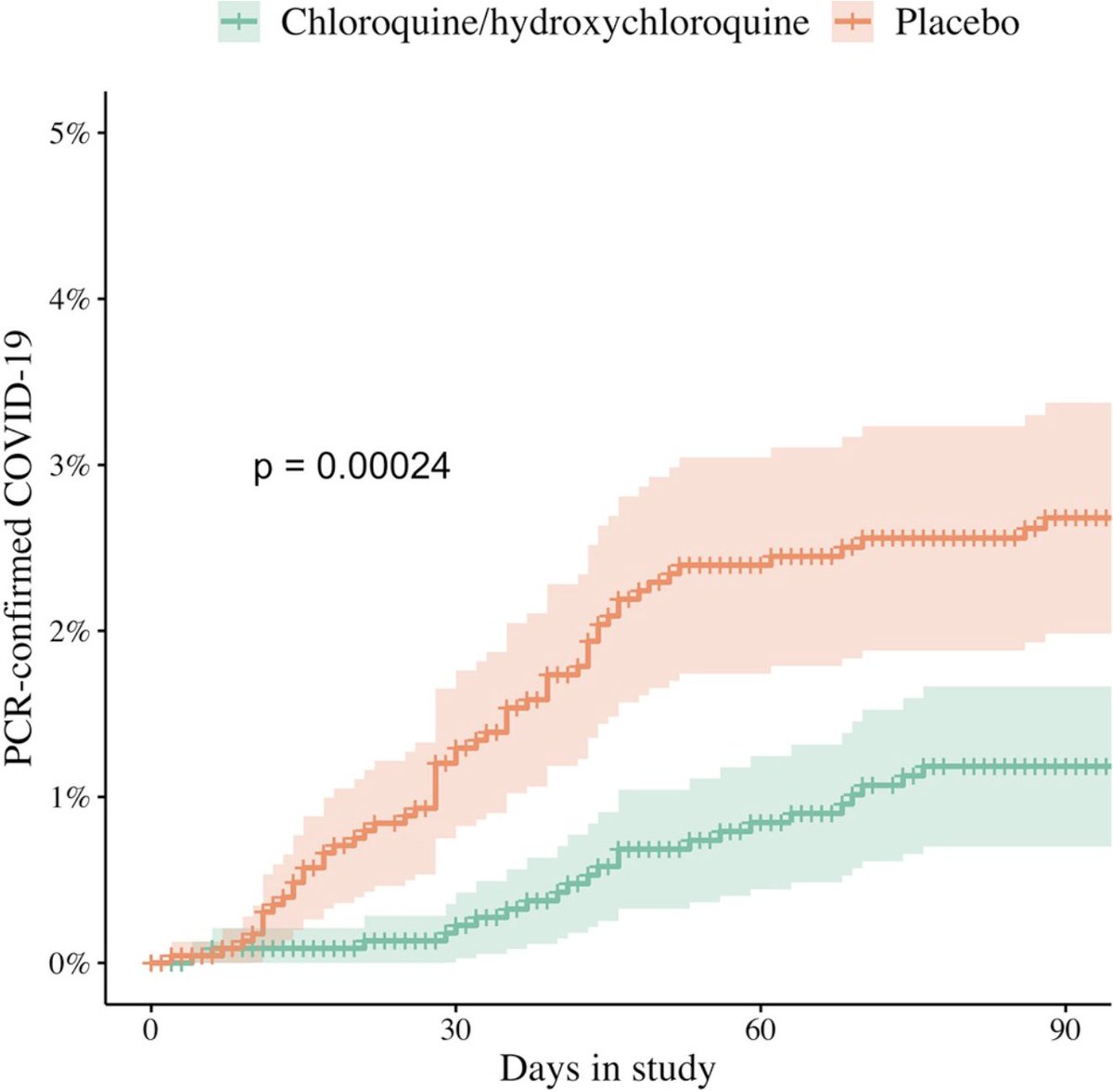
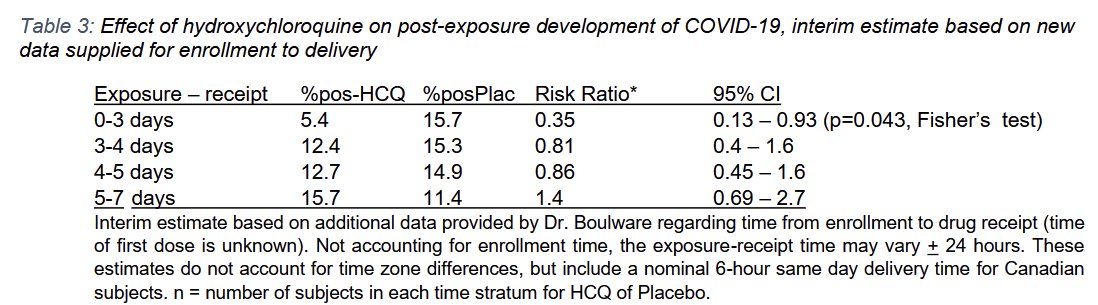
Look at ensitrelvir, a drug which has similar effect as HCQ in PeP: it is effective only when you give it early after exposure.
osf.io/h4p9j/files/vz8a7
@AdhesionsOrg , @PierreKory you should tell Boulware.

1
4
361
Covid Analysis: 200 COVID-19 treatments retweeted

May 13
What???
@CovidAnalysis
It looks like this wonderful japanese drug is really effective only... in Japan.🤔


In the phase 3 SCORPIO-PEP trial, the 3C-like protease inhibitor ensitrelvir was more effective than placebo in preventing Covid-19 in household contacts of patients with SARS-CoV-2 infection. Full trial results: nej.md/4npQqG7
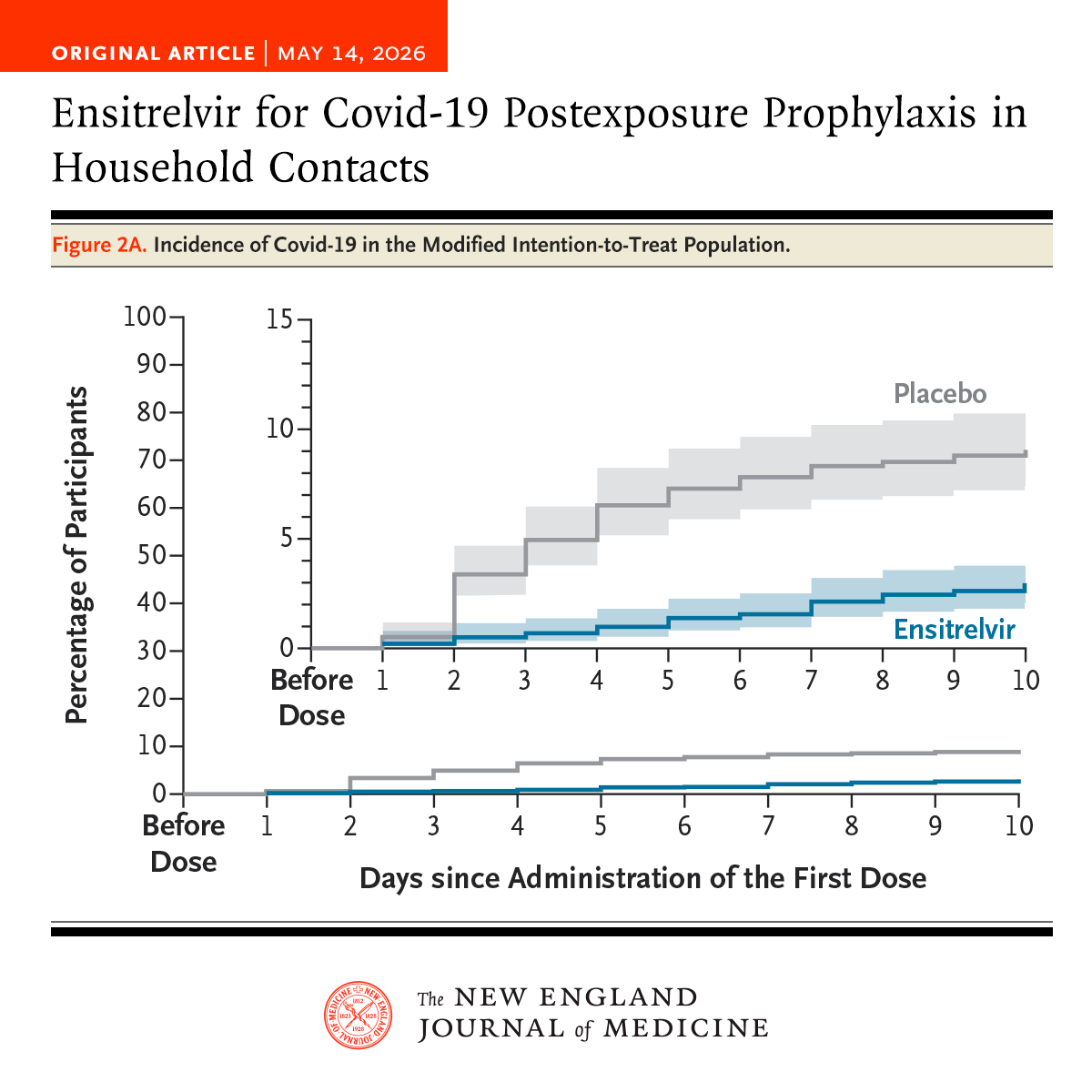
ALT Graph illustrating the incidence of Covid-19 in the modified intention-to-treat population. The x-axis represents days since the first dose, and the y-axis shows the percentage of participants. Two lines are depicted: one for the placebo group and another for the ensitrelvir group. The ensitrelvir line is consistently lower. This figure appears in the article "Ensitrelvir for Covid-19 Postexposure Prophylaxis in Household Contacts" published in the New England Journal of Medicine.
2
3
9
619
Covid Analysis: 200 COVID-19 treatments retweeted

Why do we let pharma companies experiment on people?
Why isn't there blind funding from pharma for independent trials?

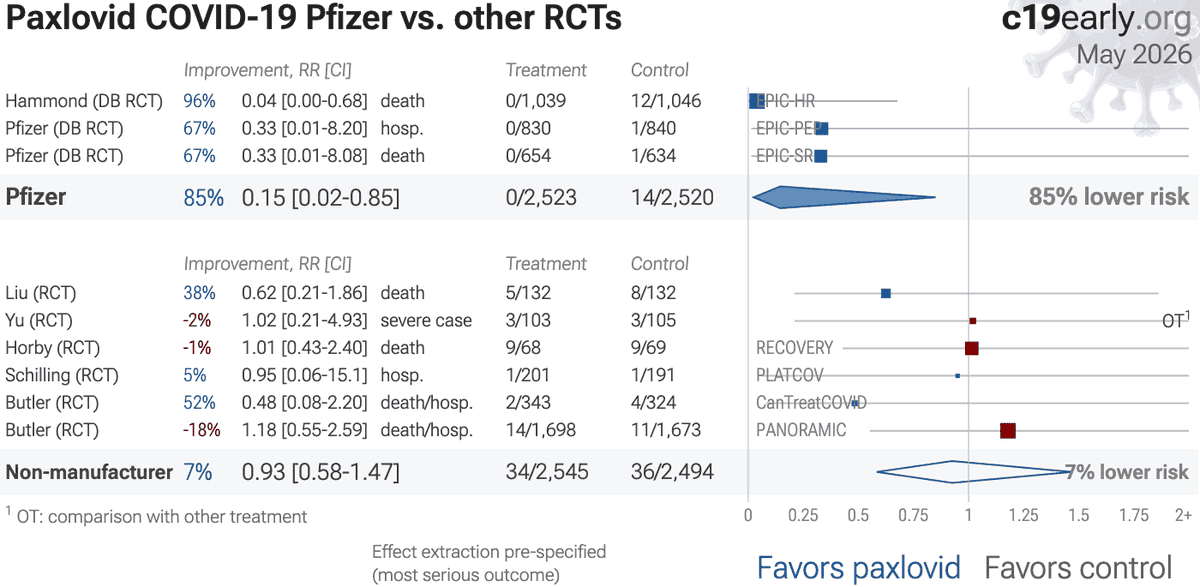
Results were very good in the manufacturer RCTs, but third-party RCTs show poor results for serious outcomes.
2
14
41
2,119
This is why effective treatments are denied.
A misleading statement becomes a false denial. If future data confirms benefit, the lethal error cannot be corrected.
Authorities should have real-time analysis for all disease treatments. The hantavirus ivermectin entry would report no clinical data but potential benefit based on extensive evidence (see below).
Failure to proactively analyze data in real-time guarantees delayed recognition of efficacy or harm, by which time moral, legal, career, and reputational liabilities strongly disincentivize any admission of error.
The WHO spokesperson below reports no clinical data showing efficacy, but leaves out all context: not mentioning that clinical data showing efficacy is impossible because there is no clinical data, and not mentioning the extensive data that suggests potential efficacy.
The news outlet changes this to a denial of efficacy, a false statement that can never be corrected. No matter how much future data shows efficacy, they will not admit to a lethal error.
The same thing happened for many COVID-19 treatments - poorly worded and incomplete statements quickly became unsupported denials, and those denials will not be corrected by the current generation of officials.
--
Preclinical data suggesting potential benefit of ivermectin for hantavirus:
Host-directed anti-inflammatory/lung-injury effects are relevant to severe hantavirus disease characterized by endothelial dysfunction, vascular leakage, pulmonary edema, and cytokine-mediated injury. Preclinical ivermectin data shows reduced acute lung injury, pulmonary fibrosis/inflammatory infiltration, NF-κB/p65-mediated inflammation, and cytokine production.
Inhibition of importin-α/β-mediated nuclear transport - hantavirus N protein interacts with importin-α and can modulate NF-κB signaling. As hantavirus replication is mainly cytoplasmic, this is more relevant to viral protein trafficking or host immune-signaling modulation.
Broad-spectrum activity against dengue, Zika, West Nile, yellow fever, Japanese encephalitis, chikungunya, Semliki Forest, Sindbis, HIV-1, COVID-19 and influenza is also supportive. Hantaviruses are also enveloped RNA viruses, although biologically distinct from flaviviruses, alphaviruses, coronaviruses, retroviruses, and influenza viruses.
--
References in COVID-19 context - many are also relevant for hantavirus:
Ivermectin, better known for antiparasitic activity, is a broad spectrum antiviral with activity against many viruses including H7N7 (1), Dengue (2-4), HIV-1 (3), Simian virus 40 (5), Zika (4,6,7), West Nile (7), Yellow Fever (8,9), Japanese encephalitis (8), Chikungunya (9), Semliki Forest virus (9), Human papillomavirus (10), Epstein-Barr (10), BK Polyomavirus (11), and Sindbis virus (9).
Ivermectin inhibits importin-α/β-dependent nuclear import of viral proteins (1,3,5,12), shows spike-ACE2 disruption at 1nM with microfluidic diffusional sizing (13), binds to glycan sites on the SARS-CoV-2 spike protein preventing interaction with blood and epithelial cells and inhibiting hemagglutination (14,15), shows dose-dependent inhibition of wildtype and omicron variants (16), exhibits dose-dependent inhibition of lung injury (17,18), may inhibit SARS-CoV-2 via IMPase inhibition (4), may inhibit SARS-CoV-2 induced formation of fibrin clots resistant to degradation (19), inhibits SARS-CoV-2 3CLpro (20), may inhibit SARS-CoV-2 RdRp activity (21,22), may minimize viral myocarditis by inhibiting NF-κB/p65-mediated inflammation in macrophages (23), may be beneficial for COVID-19 ARDS by blocking GSDMD and NET formation (24), may interfere with SARS-CoV-2's immune evasion via ORF8 binding (25), may inhibit SARS-CoV-2 by disrupting CD147 interaction (26-29), may inhibit SARS-CoV-2 attachment to lipid rafts via spike NTD binding (30), shows protection against inflammation, cytokine storm, and mortality in an LPS mouse model sharing key pathological features of severe COVID-19 (31,32), may be beneficial in severe COVID-19 by binding IGF1 to inhibit the promotion of inflammation, fibrosis, and cell proliferation that leads to lung damage (33), significantly mitigates bleomycin-induced pulmonary fibrosis by reducing collagen accumulation and inflammatory cell infiltration (34), improves oxidative stress markers while suppressing myofibroblast proliferation (34), may minimize SARS-CoV-2 induced cardiac damage (35,36), may counter immune evasion by inhibiting NSP15-TBK1/KPNA1 interaction and restoring IRF3 activation (37), may disrupt SARS-CoV-2 N and ORF6 protein nuclear transport and their suppression of host interferon responses (38), reduces TAZ/YAP nuclear import, relieving SARS-CoV-2-driven suppression of IRF3 and NF-κB antiviral pathways (39), increases Bifidobacteria which play a key role in the immune system (40), has immunomodulatory (41) and anti-inflammatory (42,43) properties, and has an extensive and very positive safety profile (44).
References
1. Götz et al., Influenza A viruses escape from MxA restriction at the expense of efficient nuclear vRNP import, Scientific Reports, nature.com/articles/srep2313…
2. Tay et al., Nuclear localization of dengue virus (DENV) 1–4 non-structural protein 5; protection against all 4 DENV serotypes by the inhibitor Ivermectin, Antiviral Research, sciencedirect.com/science/ar…
3. Wagstaff et al., Ivermectin is a specific inhibitor of importin α/β-mediated nuclear import able to inhibit replication of HIV-1 and dengue virus, Biochemical Journal, portlandpress.com/biochemj/a…
4. Jitobaom et al., Identification of inositol monophosphatase as a broad‐spectrum antiviral target of ivermectin, Journal of Medical Virology, onlinelibrary.wiley.com/doi/…
5. Wagstaff (B) et al., An AlphaScreen®-Based Assay for High-Throughput Screening for Specific Inhibitors of Nuclear Import, SLAS Discovery, sciencedirect.com/science/ar…
6. Barrows et al., A Screen of FDA-Approved Drugs for Inhibitors of Zika Virus Infection, Cell Host & Microbe, sciencedirect.com/science/ar…
7. Yang et al., The broad spectrum antiviral ivermectin targets the host nuclear transport importin α/β1 heterodimer, Antiviral Research, sciencedirect.com/science/ar…
8. Mastrangelo et al., Ivermectin is a potent inhibitor of flavivirus replication specifically targeting NS3 helicase activity: new prospects for an old drug, Journal of Antimicrobial Chemotherapy, academic.oup.com/jac/article…
9. Varghese et al., Discovery of berberine, abamectin and ivermectin as antivirals against chikungunya and other alphaviruses, Antiviral Research, sciencedirect.com/science/ar…
10. Li et al., Quantitative proteomics reveals a broad-spectrum antiviral property of ivermectin, benefiting for COVID-19 treatment, J. Cellular Physiology, onlinelibrary.wiley.com/doi/…
11. Bennett et al., Role of a nuclear localization signal on the minor capsid Proteins VP2 and VP3 in BKPyV nuclear entry, Virology, sciencedirect.com/science/ar…
12. Kosyna et al., The importin α/β-specific inhibitor Ivermectin affects HIF-dependent hypoxia response pathways, Biological Chemistry, degruyter.com/document/doi/1…
13. Fauquet et al., Microfluidic Diffusion Sizing Applied to the Study of Natural Products and Extracts That Modulate the SARS-CoV-2 Spike RBD/ACE2 Interaction, Molecules, mdpi.com/1420-3049/28/24/807…
14. Boschi et al., SARS-CoV-2 Spike Protein Induces Hemagglutination: Implications for COVID-19 Morbidities and Therapeutics and for Vaccine Adverse Effects, bioRxiv, biorxiv.org/content/10.1101/…
15. Scheim et al., Sialylated Glycan Bindings from SARS-CoV-2 Spike Protein to Blood and Endothelial Cells Govern the Severe Morbidities of COVID-19, International Journal of Molecular Sciences, mdpi.com/1422-0067/24/23/170…
16. Shahin et al., The selective effect of Ivermectin on different human coronaviruses; in-vitro study, Research Square, researchsquare.com/article/r…
17. Abd-Elmawla et al., Suppression of NLRP3 inflammasome by ivermectin ameliorates bleomycin-induced pulmonary fibrosis, Journal of Zhejiang University-SCIENCE B, link.springer.com/10.1631/jz…
18. Ma et al., Ivermectin contributes to attenuating the severity of acute lung injury in mice, Biomedicine & Pharmacotherapy, sciencedirect.com/science/ar…
19. Vottero et al., Computational Prediction of the Interaction of Ivermectin with Fibrinogen, Molecular Sciences, mdpi.com/1422-0067/24/14/114…
20. Mody et al., Identification of 3-chymotrypsin like protease (3CLPro) inhibitors as potential anti-SARS-CoV-2 agents, Communications Biology, nature.com/articles/s42003-0…
21. Parvez et al., Prediction of potential inhibitors for RNA-dependent RNA polymerase of SARS-CoV-2 using comprehensive drug repurposing and molecular docking approach, International Journal of Biological Macromolecules, sciencedirect.com/science/ar…
22. Li (B) et al., Drug–Target Interaction Prediction via Dual-Interaction Fusion, Molecules, mdpi.com/1420-3049/31/3/498
23. Gao et al., Ivermectin ameliorates acute myocarditis via the inhibition of importin-mediated nuclear translocation of NF-κB/p65, International Immunopharmacology, sciencedirect.com/science/ar…
24. Liu et al., Crosstalk between neutrophil extracellular traps and immune regulation: insights into pathobiology and therapeutic implications of transfusion-related acute lung injury, Frontiers in Immunology, frontiersin.org/articles/10.…
25. Bagheri-Far et al., Non-spike protein inhibition of SARS-CoV-2 by natural products through the key mediator protein ORF8, Molecular Biology Research Communications, mbrc.shirazu.ac.ir/article_7…
26. Shouman et al., SARS-CoV-2-associated lymphopenia: possible mechanisms and the role of CD147, Cell Communication and Signaling, biosignaling.biomedcentral.c…
27. Scheim (B), D., Ivermectin for COVID-19 Treatment: Clinical Response at Quasi-Threshold Doses Via Hypothesized Alleviation of CD147-Mediated Vascular Occlusion, SSRN, europepmc.org/article/ppr/pp…
28. Scheim (C), D., From Cold to Killer: How SARS-CoV-2 Evolved without Hemagglutinin Esterase to Agglutinate and Then Clot Blood Cells, Center for Open Science, osf.io/sgdj2
29. Behl et al., CD147-spike protein interaction in COVID-19: Get the ball rolling with a novel receptor and therapeutic target, Science of The Total Environment, sciencedirect.com/science/ar…
30. Lefebvre et al., Characterization and Fluctuations of an Ivermectin Binding Site at the Lipid Raft Interface of the N-Terminal Domain (NTD) of the Spike Protein of SARS-CoV-2 Variants, Viruses, mdpi.com/1999-4915/16/12/183…
31. Zhang et al., Ivermectin inhibits LPS-induced production of inflammatory cytokines and improves LPS-induced survival in mice, Inflammation Research, link.springer.com/10.1007/s0…
32. DiNicolantonio et al., Ivermectin may be a clinically useful anti-inflammatory agent for late-stage COVID-19, Open Heart, openheart.bmj.com/content/7/…
33. Zhao et al., Identification of the shared gene signatures between pulmonary fibrosis and pulmonary hypertension using bioinformatics analysis, Frontiers in Immunology, frontiersin.org/articles/10.…
34. Zaher et al., Testing the Possible Protective Effect of Ivermectin on Bleomycin-Induced Pulmonary Fibrosis in Albino Rats: Histological and Immunohistochemical Study, Medicina, mdpi.com/1648-9144/62/3/560
35. Liu (B) et al., Genome-wide analyses reveal the detrimental impacts of SARS-CoV-2 viral gene Orf9c on human pluripotent stem cell-derived cardiomyocytes, Stem Cell Reports, sciencedirect.com/science/ar…
36. Liu (C) et al., SARS-CoV-2 viral genes Nsp6, Nsp8, and M compromise cellular ATP levels to impair survival and function of human pluripotent stem cell-derived cardiomyocytes, Stem Cell Research & Therapy, stemcellres.biomedcentral.co…
37. Mothae et al., SARS-CoV-2 host-pathogen interactome: insights into more players during pathogenesis, Virology, sciencedirect.com/science/ar…
38. Gayozo et al., Binding affinities analysis of ivermectin, nucleocapsid and ORF6 proteins of SARS-CoV-2 to human importins α isoforms: A computational approach, Biotecnia, biotecnia.unison.mx/index.ph…
39. Kofler et al., M-Motif, a potential non-conventional NLS in YAP/TAZ and other cellular and viral proteins that inhibits classic protein import, iScience, sciencedirect.com/science/ar…
40. Hazan et al., Treatment with Ivermectin Increases the Population of Bifidobacterium in the Gut, ACG 2023, acg2023posters.eventscribe.n…
41. Munson et al., Niclosamide and ivermectin modulate caspase-1 activity and proinflammatory cytokine secretion in a monocytic cell line, British Society For Nanomedicine Early Career Researcher Summer Meeting, 2021, web.archive.org/web/20230401…
42. DiNicolantonio (B) et al., Anti-inflammatory activity of ivermectin in late-stage COVID-19 may reflect activation of systemic glycine receptors, Open Heart, openheart.bmj.com/content/8/…
43. Yan et al., Anti-inflammatory effects of ivermectin in mouse model of allergic asthma, Inflammation Research, link.springer.com/10.1007/s0…
44. Descotes, J., Medical Safety of Ivermectin, ImmunoSafe Consultance, web.archive.org/web/20240313…
May 8

NOW - WHO confirms that Ivermectin is not an effective treatment for Hantavirus and reiterates that "the risk is low for the general population."
9
14
982
COVID-19 studies show:
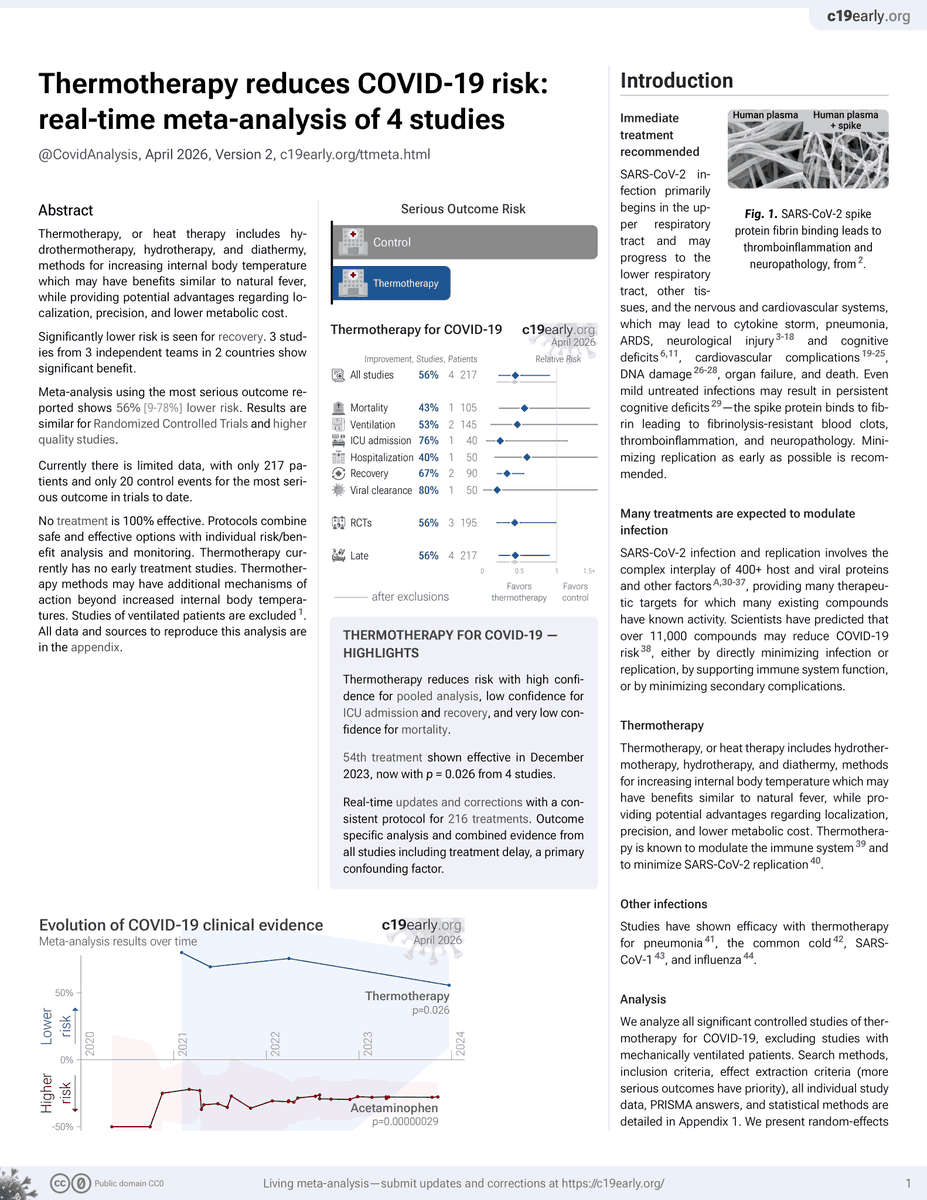
🛡️ Simulating natural fever with thermotherapy reduces risk: c19early.org/ttmeta.html
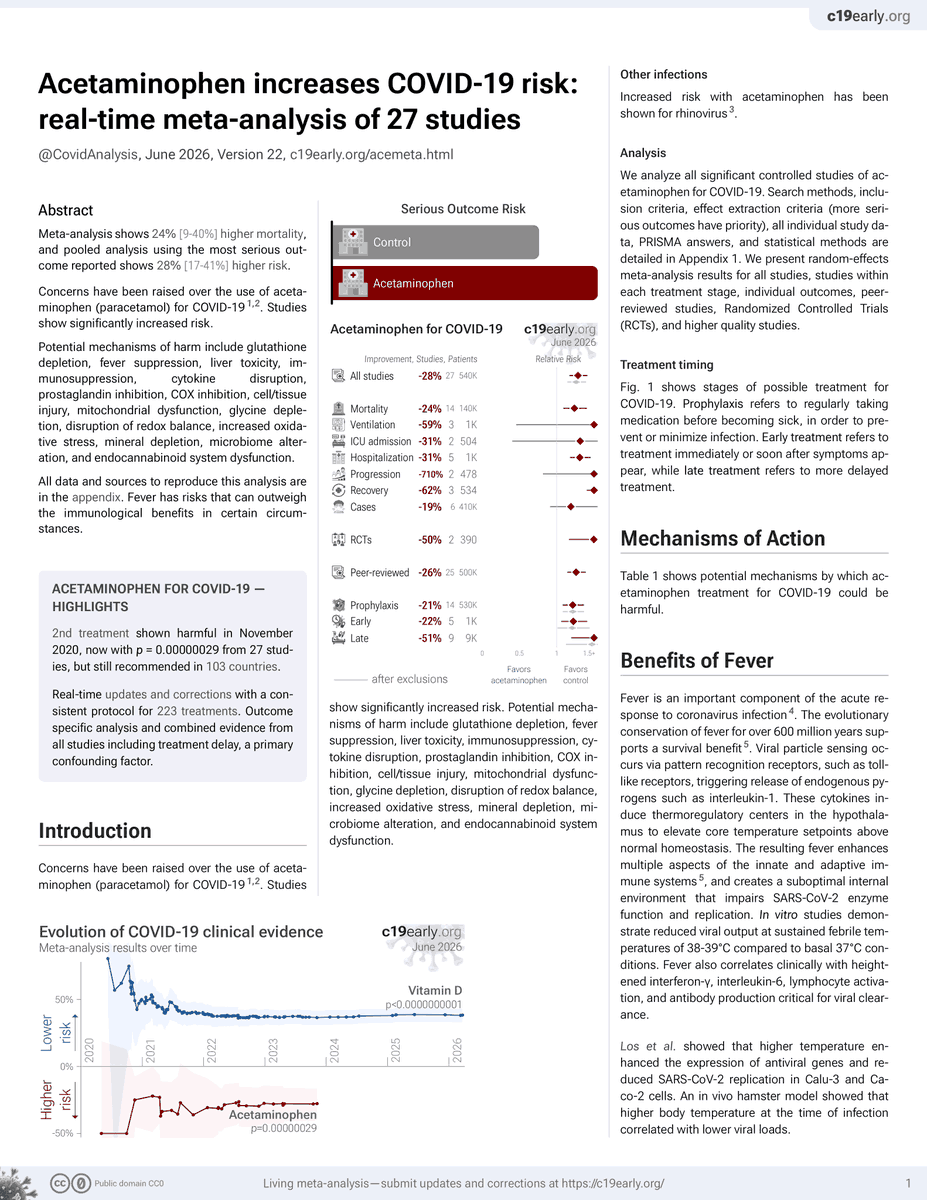
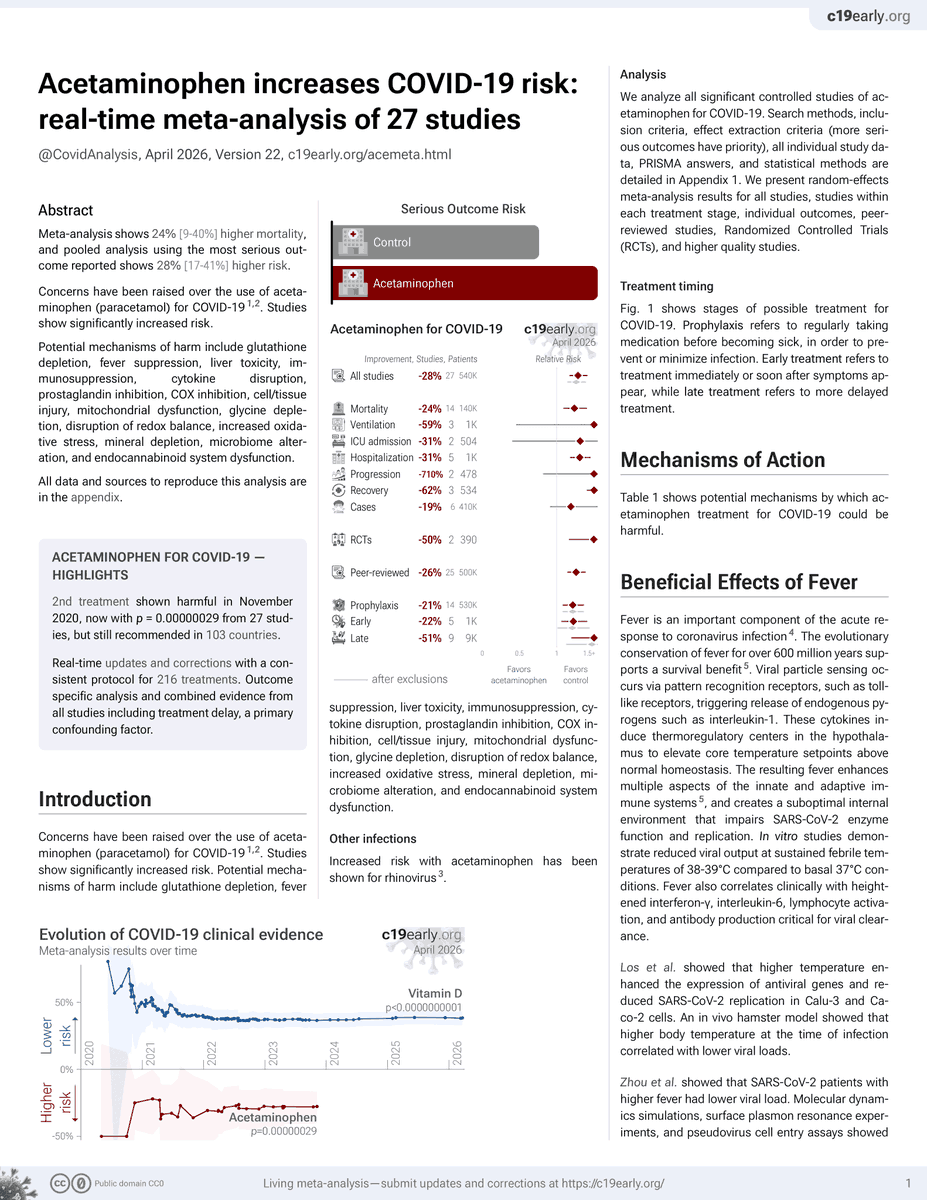
📈 Acetaminophen increases risk - fever suppression is one of the potential mechanisms of harm: c19early.org/acemeta.html
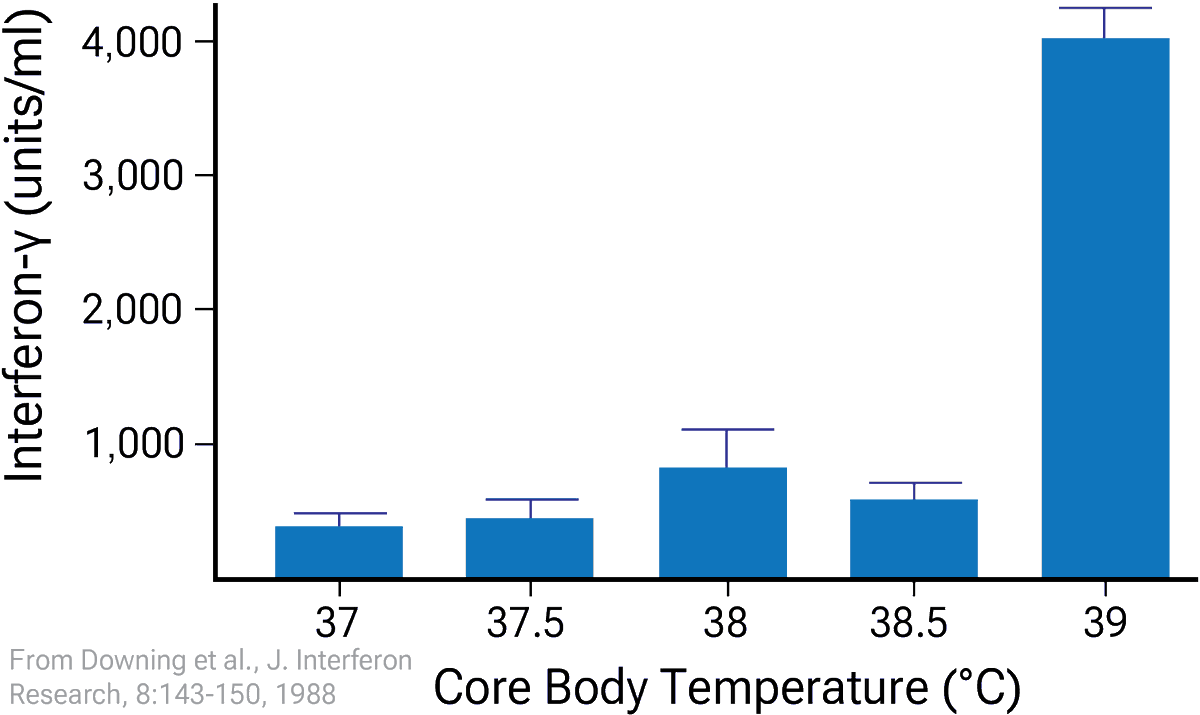
Fever enhances multiple aspects of the innate and adaptive immune systems, and creates a suboptimal environment that impairs SARS-CoV-2 enzyme function and replication.

People calling me a quack for talking about the importance of fever during an infection even to the point of not treating it or even promoting it.
They are the quacks for not reading enough scientific papers.
academic.oup.com/emph/articl…

1
7
15
888