
We're stardust. Always have been and always will be.
Joined May 2011
- Tweets 20,214
- Following 497
- Followers 592
- Likes 179,713
254 Photos and videos



Cyrus retweeted

May 17
europe simply wasn’t ready for the extraordinary and beautiful piece of art that is liekinheitin



10
222
1,868
22,331


Cyrus retweeted

May 11
In contagion prevention, you’re only a strong as your weakest link.
Apart from the absolutely MORONIC decision to not quarantine the ship centrally, there isn’t even coordination on how to correctly quarantine these people in their respective countries.
What does it help if the British or the Japanese do the right thing, if the Dutch would let this spread in the community? It’s only a matter of time before it would spread from there to other countries.
This is an absolutely failure of the WHO to do its job. They are not just being useless, they are being harmful. If it wasn’t for them, the ship wouldn’t have docked anywhere for a long time, creating a natural quarantine. The guy on the street has more common sense than the WHO.
3
17
148
7,925
Cyrus retweeted

May 9
😄 The situation on Russian Telegram channels now…
39
731
7,791
115,369
Cyrus retweeted

May 8
If there was just one single lesson we should have learned from covid, it's that people don't understand airborne pathogen transmission.
We should have learned that and then taught everyone how airborne transmission works and how to stop it.
43
411
1,710
16,197
Cyrus retweeted

“It’s more important to feel safe than it is to actually be safe”
-Modern public health
2
106
400
3,351
Cyrus retweeted

Lifeboats To Be Removed From Cruise Ships Because They Remind People Of Titanic Sinking

ALT LIfeboats Headline:Lifeboats To Be Removed From Cruise Ships Because They Remind People Of Titanic Sinking Story by Melanie Fork and Jacx Pinkietown Photo from Adobe
31
514
1,573
33,926
Cyrus retweeted

Mar 19
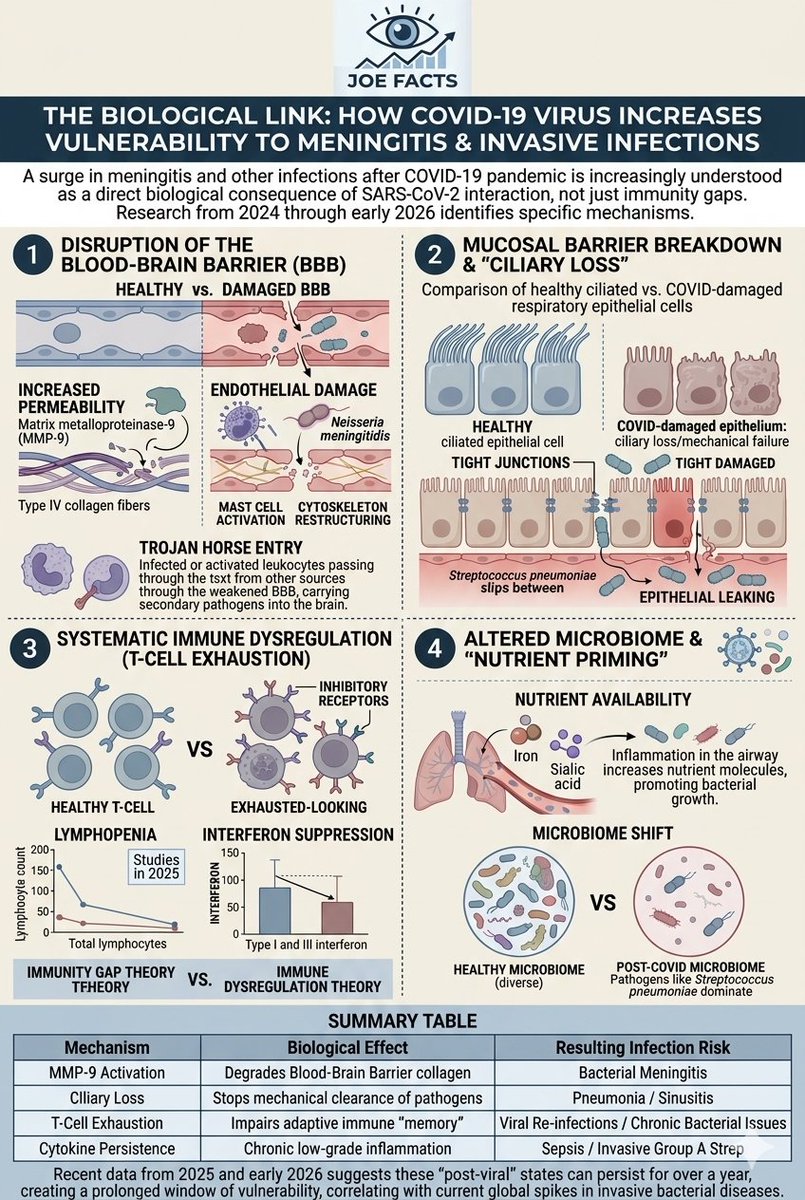
⚠️🦠The surge in meningitis and other invasive infections following the COVID-19 pandemic is increasingly understood not just as a result of "immunity gaps" from lockdowns, but as a direct biological consequence of how the SARS-CoV-2 virus interacts with the human body.
Research from 2024 through early 2026 has identified several specific physiological mechanisms—ranging from the degradation of physical barriers to long-term immune remodeling—that explain why individuals may be more susceptible to bacterial and viral pathogens after a COVID-19 infection.
1. Disruption of the Blood-Brain Barrier (BBB)
The most direct link to meningitis is the virus's impact on the brain's protective lining. SARS-CoV-2 doesn't just affect the lungs; it significantly compromises the integrity of the Blood-Brain Barrier.
* Increased Permeability: The virus increases the expression of matrix metalloproteinase-9 (MMP-9), an enzyme that degrades type IV collagen in the basement membrane of the BBB.
* Endothelial Damage: By infecting neurovascular cells, the virus triggers "mast cell activation" and restructuring of the cellular cytoskeleton. This creates "gaps" in the barrier that normally keep bacteria like Neisseria meningitidis (meningitis) out of the central nervous system.
* Trojan Horse Entry: COVID-induced inflammation increases the transmigration of infected or activated leukocytes. These cells can "carry" secondary pathogens across the weakened BBB into the brain.
2. Mucosal Barrier Breakdown and "Ciliary Loss"
Bacteria that cause meningitis often live harmlessly in the nasopharynx (the upper part of the throat). For these bacteria to become "invasive" and enter the bloodstream, they must bypass the mucosal immune system.
* Mechanical Failure: SARS-CoV-2 causes ciliary loss—the destruction of the tiny hair-like structures that sweep bacteria and mucus out of the airways. Without this "escalator," bacteria can settle and colonize the tissue more deeply.
* Epithelial "Leaking": The virus damages tight junctions (the "glue" between cells) in the respiratory lining. This allows bacteria to slip between cells and enter the bloodstream, a prerequisite for bacterial meningitis and sepsis.
3. Systematic Immune Dysregulation (T-Cell Exhaustion)
While the "immunity gap" theory focuses on a lack of exposure, the "immune dysregulation" theory focuses on the damage done by the virus to the immune system's architecture.
* T-Cell Exhaustion: Post-COVID patients often show signs of "T-cell exhaustion," a state where T-cells (the "generals" of the immune system) are functionally impaired and express high levels of inhibitory receptors. This limits the body's ability to mount a rapid defense against secondary viral and bacterial threats.
* Lymphopenia: SARS-CoV-2 frequently causes a drop in total lymphocyte counts. Studies in 2025 have shown that even 12 months after a "mild" infection, some patients retain a signature of immunological hypofunction, making them significantly more likely (up to 46% more likely in some cohorts) to test positive for non-SARS-CoV-2 infections.
* Interferon Suppression: The virus is highly effective at suppressing Type I and III interferon responses. These interferons are the body's first line of defense against both viruses and bacteria; when they are "dampened," the threshold for a secondary infection to take hold is much lower.
1/2
25
325
728
16,151
Cyrus retweeted

”Hyvä ilmanvaihto ja sairastuneena kotiin jääminen eivät heikennä immuniteettia – ne vähentävät turhaa sairastavuutta.”
Erinomainen kirjoitus. hs.fi/mielipide/art-20000118…
7
60
1,651
Cyrus retweeted
Ilmanvaihdon parantaminen sekä ilman puhdistaminen eivät tee hengitysilmasta steriiliä, vaan enemmän ulkoilman kaltaista. Lasten mikrobialtistusta kannattaisikin lisätä esimerkiksi metsäpohjaisella pihalla. hs.fi/mielipide/art-20000118…
1
17
74
2,077
1. Miksi pestä käsiä, eikö sillä kasvata immuunivelkaa?
2. Käsien pesu on tosiaan tämän päivän tiedoilla ylivoimaisesti paras keino estää hengitystieinfektioiden leviämistä.
Naurattaisi, jos ei itkettäisi.
Mar 4

1
16
253
Cyrus retweeted

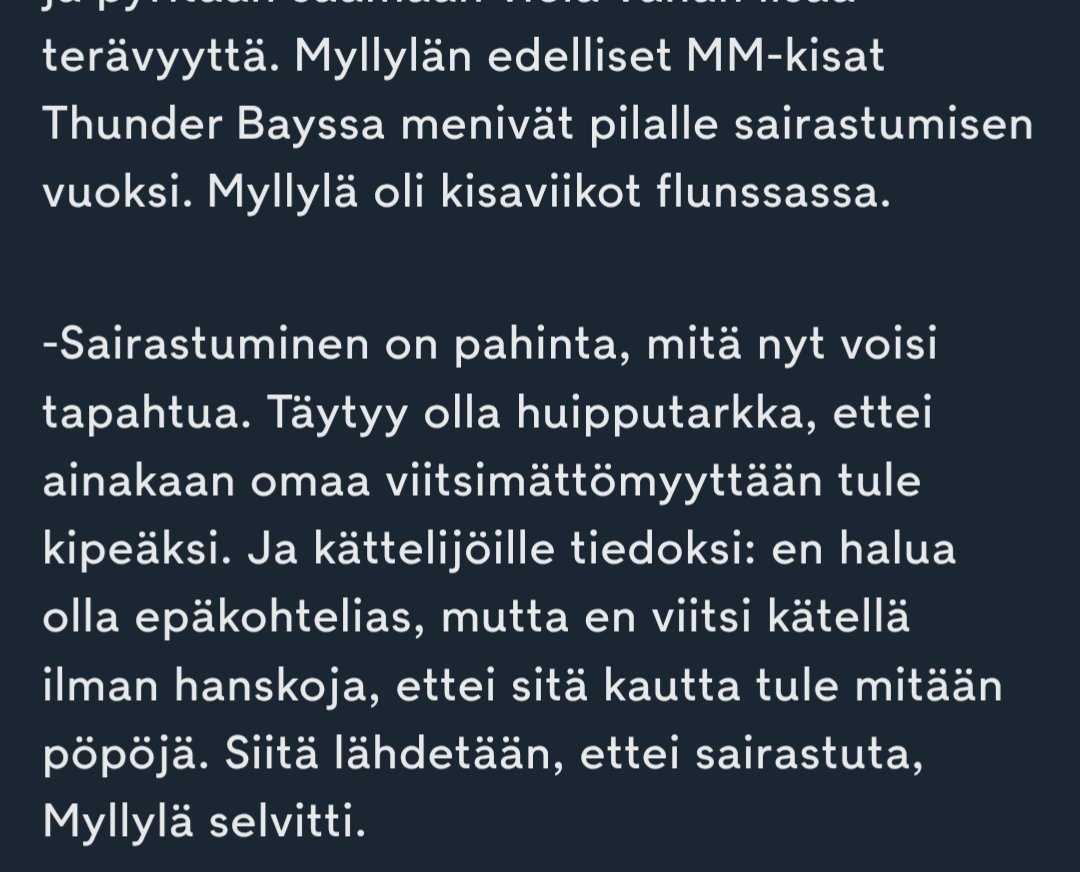
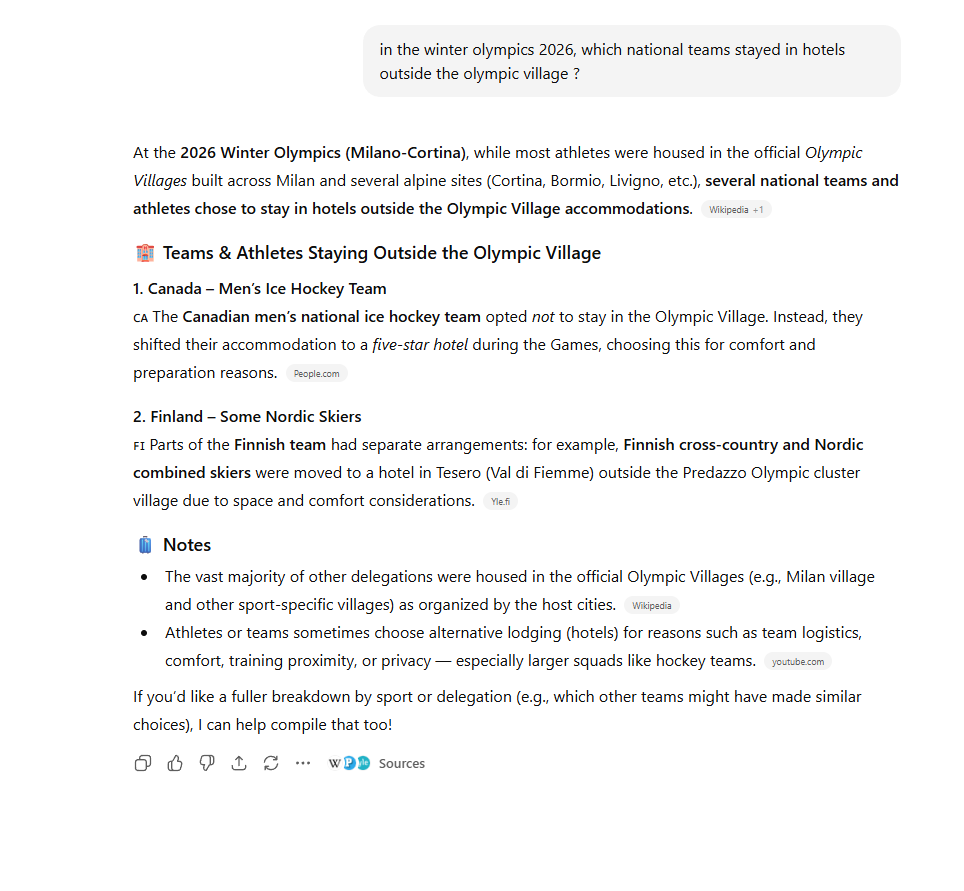
Feb 24
Here is the reason Finland had its worst-ever performance at the Winter Olympics.
1/x
4
13
74
4,150
Cyrus retweeted

He, jotka haluavat pysyä terveinä, käyttävät hengityssuojaimia. Ja niiden suosittelu on lääkärin/hoitajan/terveysviranomaisten tehtävä kuten muukin infektioiden torjunta. @STM_Uutiset @THLorg @HUS_fi @valtioneuvosto

FROM THE OLYMPICS TO NASA, WEARING MASKS IS BACK - EXCEPT IN HEALTHCARE
Brilliant article on how masking is increasingly popular with Olympic athletes, actors & astronauts wanting to avoid illness…
…but sadly, in hospitals, masking is rare & those who do are often gaslit.
🧵

1
11
48
1,798
"Clean air, the school argues, is not a luxury. It is basic infrastructure, as fundamental to education as safe buildings, clean water, and nutritious food."

Headteacher of Hayling College [UK] introduced HEPA filtration units into classrooms 2 years ago. Goal was to reduce illness, keep children & teachers in school & support learning. According to school’s attendance data, the impact has been striking portsmouth.co.uk/education/t…
2
3
342
Cyrus retweeted

"You're way too extreme with your COVID precautions. It's too much."
Well, maybe we wouldn't need to be so extreme in our precautions if the majority of the world weren't so extreme in the opposite direction of doing absolutely nothing.
56
321
1,773
37,559
Cyrus retweeted

Feb 12
N95s could be a significant performance advantage
Not just in the Olympics
But in Life

ALT AI Image - Olympic medal winners wearing N95s
94
584
3,102
46,788
Cyrus retweeted

Merry Christmas!
2,956
9,128
61,196
858,799
Cyrus retweeted

20 Dec 2025
So many new soldier graves at our city cemetery in Bucha over the last few months.
Sometimes I come here to sit down with the guys, just to make sure each and every one of them gets a visitor time after time.
Remember these guys.
It is thanks to them that Ukraine keeps holding on no matter what, and the entire free world lives on and enjoys the coming Christmas in peace and freedom.
Please let's make sure this all was never in vain.
850
3,354
17,350
310,308
Cyrus retweeted

18 Dec 2025
ABBA’s Bjorn Ulvaeus:
"What Christmas has taught me is, above all, to be grateful. Grateful that I can celebrate it in peace with my family. And that makes me think about all the brave Ukrainian men and women who are fighting tonight to defend their country against the ruthless Russian aggressor.
And remember that when they are defending their liberal democracy, they are, in fact, defending ours as well. And that they deserve all the support that they can have from us."
Thank you! ❤️🩹
152
2,670
11,899
120,372
Cyrus retweeted

16 Dec 2025
Nyrkkisääntö myös suomalaisille:
Vaikka kulkutauti leviää hengitysilman välityksellä, muista silti kuurata nyrkkejäsi niin, että nahka lähtee.
Älä missään tapauksessa käytä FFP2- tai FFP3-hengityssuojainta. Virus saattaisi pahoittaa mielensä.
Ja luota viranomaisten ohjeisiin!
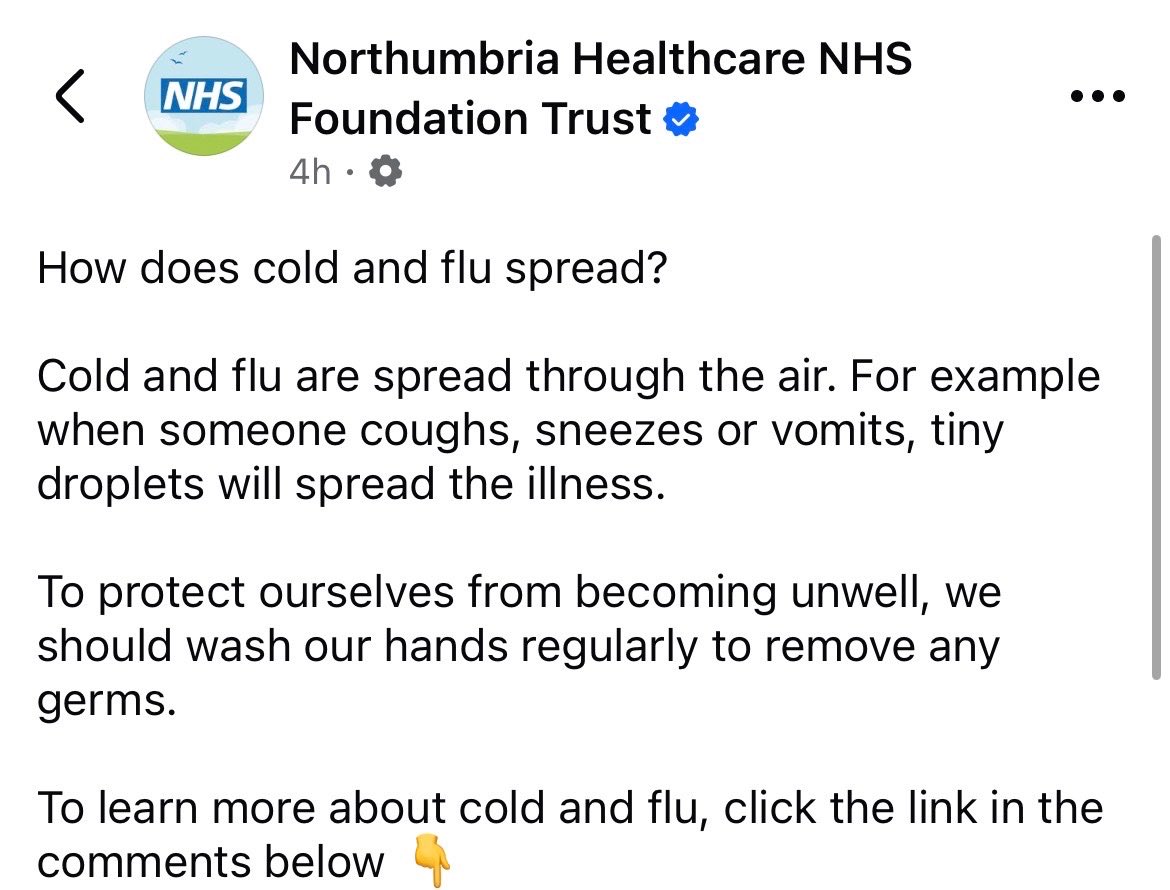
15 Dec 2025

Direct from the NHS:
“Flu spreads through the air, so please wash your hands”
I can’t deal with this level of stupid anymore… 🤯
6
7
44
2,762