
Leukemia Trialist | Assist. Prof. @MCG_AUG @GACancerCenter| @UNCHemeOnc trained | Former Osler Resident @OslerResidency | Forever South Carolina Gamecock @UofSC
Joined November 2023
- Tweets 144
- Following 183
- Followers 161
- Likes 178
48 Photos and videos




Daniel Peters retweeted
Can’t wait to finally see the OPTI-AML data presented by @beatalleukemia at @EHA_Hematology on Thursday. An immense amount of effort by the Beat AML team @bcutd_research with highly impactful results 👇.

Excited to head to #EHA2026 where I will present results of the much anticipated OPTI-AML study on behalf of the BEAT AML investigators @bcutd_research Master Trial ,Thurs Jun 11-see details 👇🏾. Hope to see many of you there ! In the words of ABBA seeing as we are in Stockholm.

2
7
30
2,177

May 13
⚠️The @FDA has just approved the ALL-ORAL💊 chemo regimen Dec-C VEN for AML. Amazing for the "right" person, but anticipating more than a few details to be worked out as it hits clinics across the country. 🤔onclive.com/view/dr-dinardo-…
63
Daniel Peters retweeted

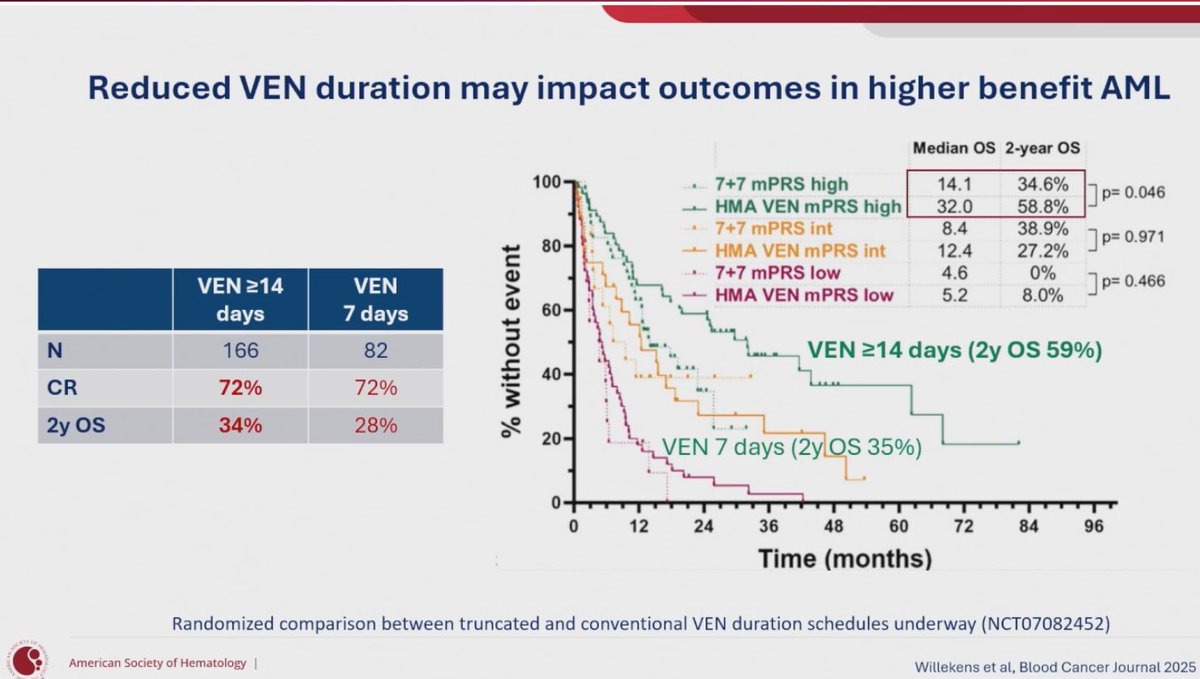
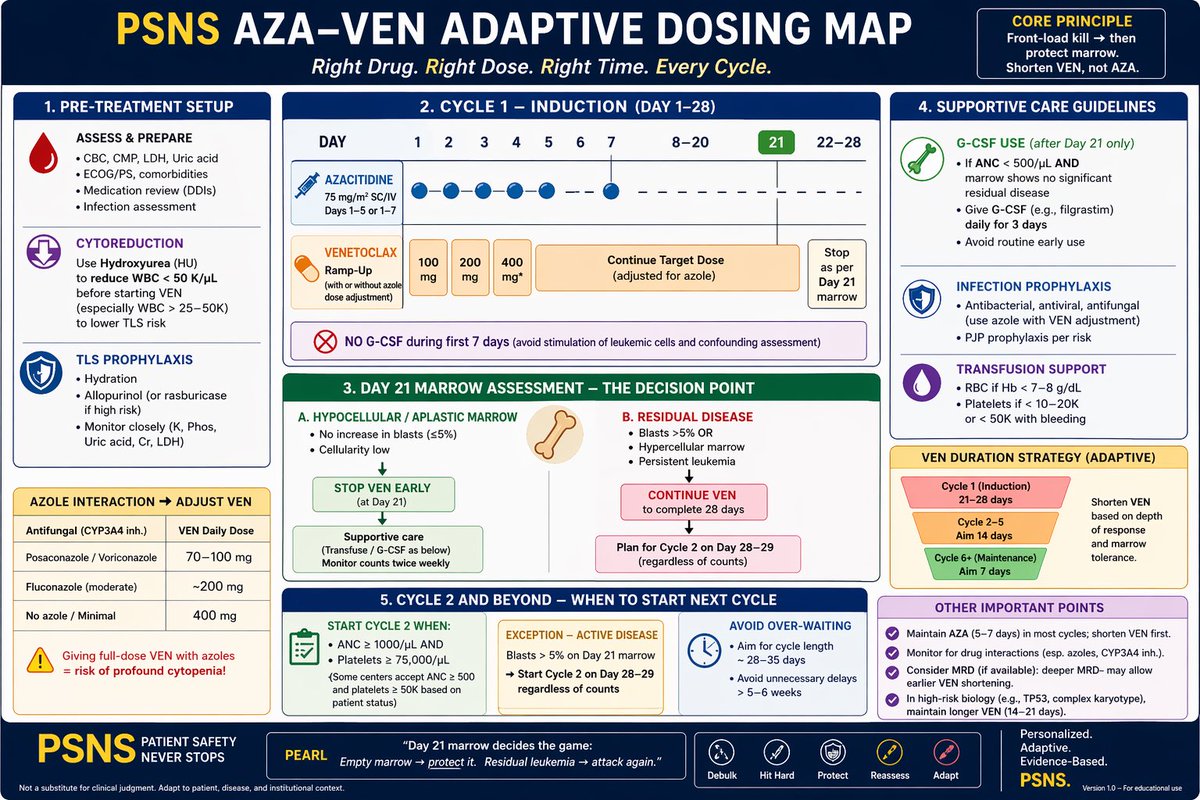
💣 AZA VEN doesn’t fail—execution does.
Day 21 marrow decides everything.
Shorten VEN, not AZA.
Don’t wait for perfect counts.
Here’s how we induce AML in 2026 👇
Please let us know your approach.
#AML #HemeTwitter
Dr Fun G
5
43
156
10,439
Apr 17
📝Scientists invented a fake disease. AI told people it was real 📝
I am all for patients empowering themselves with info online but…
“Don’t believe everything you read on the internet”
…very much applies to AI output.
Does this need to be said? 🗣️
nature.com/articles/d41586-0…
30
Daniel Peters retweeted

🧬 HMA Venetoclax in Younger AML — 50 Pearls (2026 Meta-analysis)
📌 Credits: Perrone et al., Cancer 2026
⸻
🔥 Paradigm shift: VEN HMA moving beyond “unfit” → selected younger AML
🧬 Mechanism: BCL-2 inhibition → restores apoptosis → deep responses
👨⚕️ Population: Median age ~54 yrs (<70 included)
📊 Total data: 8 studies | 429 pts (RCT phase 2 real-world)
🎯 CR/CRi pooled: 66%
🧪 MRD negativity: ~69% → deep remission signal
📈 1-year OS: ~75% → > historical (~62%)
📉 1-year EFS: ~59% (low heterogeneity)
🧠 Key: EFS consistency strongest signal across studies
🔁 Bridge to transplant: ~66% proceed to HSCT
🧬 Decitabine trend > azacitidine (EFS/OS signal)
⚖️ Compared to IC: similar or better early outcomes in selected pts
🚫 Not replacing IC in favorable-risk AML
⚠️ More promising in adverse-risk AML
🧬 MRD-driven strategy emerging
🔄 Potential chemo-sparing induction approach
🏥 Less toxicity vs IC → fewer infections, cytopenias
📉 Lower hospitalization burden (outpatient feasible)
🧠 QoL advantage (less ICU, less long stays)
💰 Likely cost-effective (data extrapolated)
📊 CR heterogeneity high (I² ~89%)
🧪 MRD variability due to methods/timing
📉 OS heterogeneity low → robust outcome
🧬 Biology-driven response (TP53, FLT3, NPM1 matter)
🧪 ELN 2024 integrates VEN-based approaches
⚠️ Fitness > age → key selection principle
🧬 Favorable-risk AML → IC still gold standard
⚠️ PARADIGM excluded key subtypes → limits generalizability
🧬 Hybrid strategies (VEN HMA → IC consolidation) used
🔁 Continuous therapy needed if no HSCT
🧠 MRD-negative pts → may defer transplant (investigational)
📉 Relapse-free survival data inconsistent
🧬 Younger pts (≤45 yrs) → better EFS
📊 CR range wide: ~40%–89% across studies
📉 US real-world outcomes lower vs trials
🌍 Geography variation (China vs US vs EU cohorts)
🧪 Venetoclax duration impact unclear
⚠️ Dosing heterogeneity across studies
🧬 Transplant intent differs across trials
📊 HSCT rates vary widely (33%–100%)
🧠 Suggests strategy tailoring (not uniform)
🧬 VEN FLAG-IDA / VEN IC also emerging competitors
📉 Toxicity still present (cytopenias, infections)
🧪 Need standardized MRD assessment
📊 No strong randomized superiority vs IC yet
🧬 Strong rationale for phase 3 trials
🧠 Key concept: induction ≠ necessarily intensive chemo
🔬 VEN HMA = “biologic induction” approach
📌 Best role: bridge-to-transplant strategy
⚠️ Patient selection remains critical
🧬 Future: biomarker-driven allocation
📊 Meta-analysis limitation: heterogeneity mixed designs
🧠 Clinical takeaway: powerful option in non-favorable risk younger AML
⸻
#AML #Venetoclax #HMA #Leukemia #BMT #Transplant #Hematology #Oncology

11
35
1,346
Daniel Peters retweeted

🚨Out in @BCD_AACR today! "Models, Models, Everywhere: But Which One Should Guide Care?" our In the Spotlight piece with @CLachowiez is now online! We review therapy-specific prognostic models including the newly pulished model by Drekolias et al for #AML treated with #venetoclax-based regimens & chart the path forward.
shorturl.at/Je1VF

1
14
38
4,737
Daniel Peters retweeted

Azacytidine, our fantastic hypomethylating agent, used for treatment of MDS and AML, was discovered in 1964, and then fell into oblivion. Almost 40 years later it was FDA approved as the first effective MDS treatment.
A 🧵about an unusual revival:
5
33
113
18,530
Mar 17
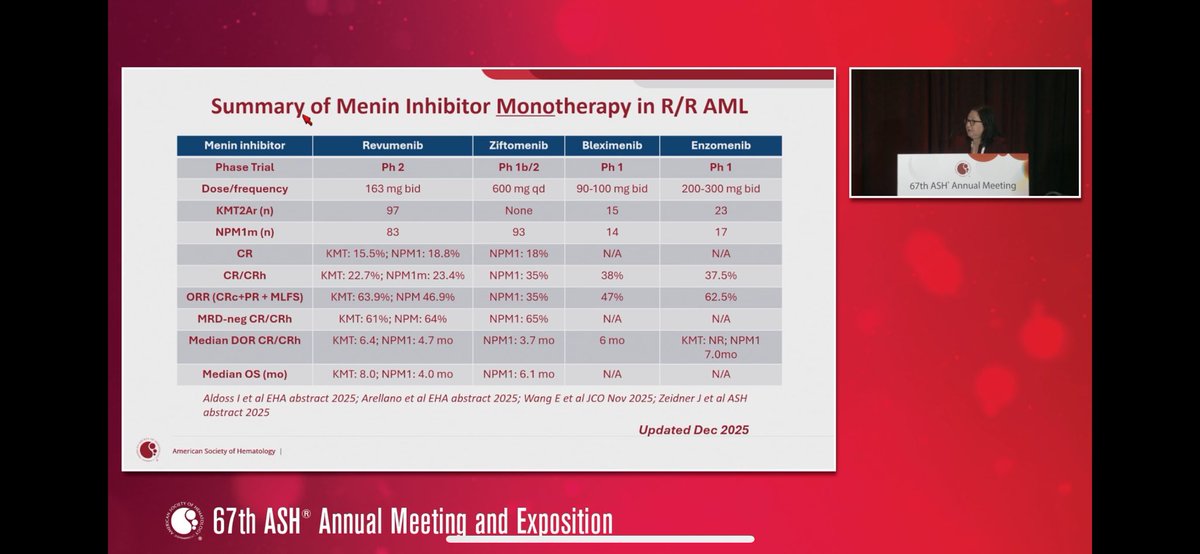
Really enjoyed putting this review together! The 💊Menin Inhibitor💊 field is evolving so quickly we had to rewrite half the 📝 2/2 all the updates the occurred 💡from submission ➡️ proof! Whew!😅
Mar 17

Hot off the press-> our new review of Menin Inhibitors in AML 🔥📰. This is such a rapidly evolving field & this review includes all relevant updates. A true tour de force with @DPetersMD, Jess Hatfield, and Mollie Reese @UNC_SOM @UNC_Lineberger
link.springer.com/epdf/10.10…
1
9
2,483
Daniel Peters retweeted
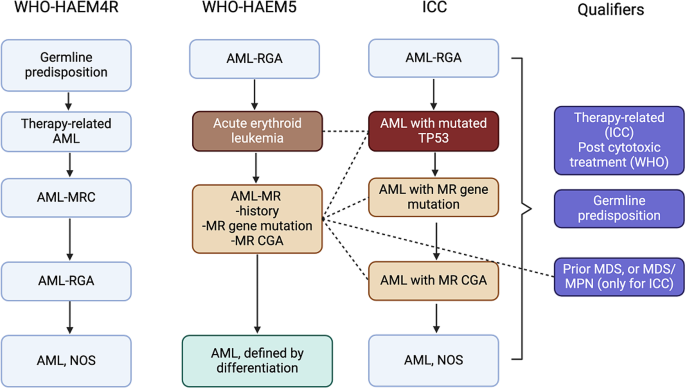
Divergent disease names, criteria, and even diagnoses (e.g., AML vs. MDS). It's time to end the division! This paper outlines a clear path forward: bridging gaps through evidence-based consensus to rally around the next WHO edition (WHO6).
link.springer.com/article/10…
1
21
56
5,380
Daniel Peters retweeted

Feb 26
One of my favorite things to write with two colleagues from whom I’ve learned a great deal. @MSKCancerCenter
ashpublications.org/blood/ar…
1
7
30
2,516
Feb 20
“If you have an ASXL1 mutation and smoke you have an increased risk of blood cancer” For too long we’ve known too little about 🩸 cancer risk. We need to do better to DETECT and PREEMPT AML/MDS. Thanks @beatalleukemia for this great talk! #leusm

3
18
1,211
Feb 20
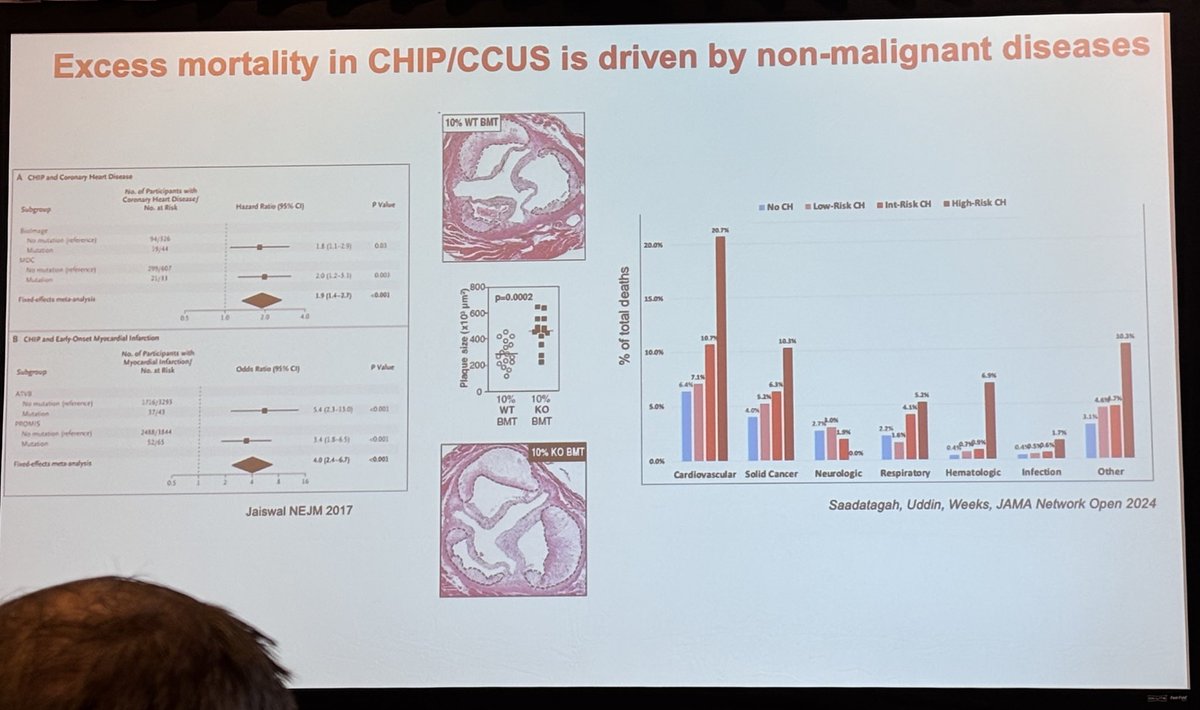
At the 3rd Annual Perri Symposium @UNC_Lineberger today and it’s been fantastic. Thoughtful talks on de-intensifying 1L AML tx, optimizing FLT3-mut dz 🧬, TP53 biology, and where menin inhibitors are headed 💊. Unlike AML triplets, year 3 is unquestionably the best. @LeukDocJZ
2
8
680
Feb 20
Wishing @jorgecortesmd all the best as he heads to Birmingham. 🎉 I’m genuinely grateful for your leadership at @GACancerCenter, and even in the short time I’ve known you I’ve learned a lot from your example & mentorship. 🎓@ONealCancerUAB is getting an outstanding leader. ⭐️
1
12
379
Daniel Peters retweeted

Feb 10
Hot off the press-> New @BloodCancerUtd Beat AML Analysis @BloodAdvances analyzing clinical outcomes of NPM1m or KMT2Ar AML in pts >60 y/o. This is an important historical reference prior to use of Menin inhibitors. @beatalleukemia @UNC_Lineberger
ashpublications.org/bloodadv…
1
3
25
3,453
Daniel Peters retweeted
🧬 Why Cyclophosphamide (PTCy) is given on D 3 (±D 4) — NOT D 2 post allo-SCT
🧵 Thread (mechanism-based, guideline-driven):
🕒 Day 0 = graft infusion
➡️ Donor T cells enter host
➡️ Antigen recognition starts but most alloreactive T cells are NOT yet dividing
🔄 Day 1 to 2
❌ Alloreactive T cells still in early activation phase
❌ Many NOT in S-phase
❌ Cyclophosphamide would MISS key pathogenic clones
🧪 Cyclophosphamide = cell-cycle dependent cytotoxicity
➡️ Kills rapidly dividing T cells
➡️ Needs cells in active DNA synthesis
📈 Peak alloreactive T-cell proliferation = Day 3
✅ Pathogenic GVHD-causing T cells enter rapid cycling
✅ Maximum susceptibility to cyclophosphamide
🎯 Day 3 (± Day 4) = SWEET SPOT
🔥 Deletes alloreactive donor T cells
🛡️ Preserves:
•🧫 Hematopoietic stem cells (↑ ALDH expression)
•🧑⚕️ Regulatory T cells (ALDH-high, slower cycling)
•🦠 Pathogen-specific memory T cells
❌ Why NOT Day 2?
⚠️ Too early
⚠️ Incomplete deletion of alloreactive clones
⚠️ → Higher risk of acute GVHD
❌ Why NOT later (D 5 or beyond)?
⚠️ Alloreactive T cells exit peak proliferation
⚠️ Less cyclophosphamide sensitivity
⚠️ Loss of selectivity → ↑ GVHD, ↑ toxicity
⚖️ Clinical balance achieved at D 3:
✔️ GVHD prevention
✔️ Engraftment preserved
✔️ GVL effect maintained
✔️ Immune reconstitution spared
📌 Bottom line:
🧠 PTCy timing is biologically timed to T-cell kinetics — not arbitrary
⏱️ D 3 targets the enemy when it’s most vulnerable
#PTCy #AlloSCT #GVHD #BMT #TransplantImmunology #Hematology #KFSHRC #SOHO_KSA #ESH_Emirates_Hematology_Society
15
44
1,960
Feb 6
This is important🚨 in #AML. Think we will (and already are) going to see similar themes in 🧬NPM1m AML treated with lower intensity therapy (💊AZA/VEN). #leusm #bmtsm. Awesome work. 👏🏻

🚨New in Leukemia: HARMONY NPM1 classification reassigns >40% of NPM1-mut patients into a different risk category with potential clinical impact on allo-HSCT decision-making
🔓Free access link:
nature.com/articles/s41375-0…
@HarmonyFoundEU @LeukemiaJnl @HematoCAUSA
2
185
Feb 6
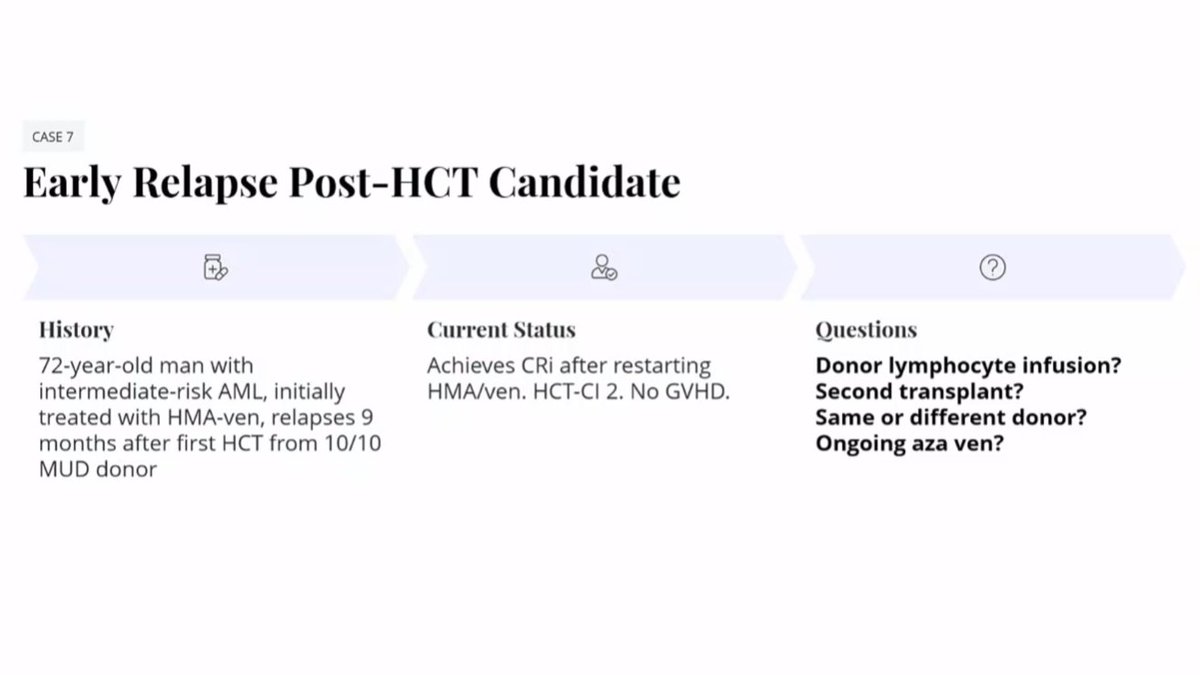
A: HMA-“based" 💊 with DLI.
Why "based"?
⚠️Open Q: Does VEN kill/impact the new lymphocytes?
❔What DLI dose do others consider? Great Q.
1
1
40
Feb 6
Giralt 👨🍳 for DLI (MUD)
🩸Donor apheresis = 10-12M cells. 1-2M per bag.
🤏Start low: 0.5-1M CD3/kg, then go up next dose
⏱️Give q3-4 months. Closely monitor GVHD
🥼Based on EBMT (expert cons. only) MAY give 5M CD3/kg cell doses in future
1
41