Children’s Physiotherapist | Director @PTKidsUK Advocate for child health & movement. Helping children reach their full potential & other therapists to thrive
Joined February 2012
- Tweets 2,515
- Following 750
- Followers 689
- Likes 12,527
451 Photos and videos













May 16
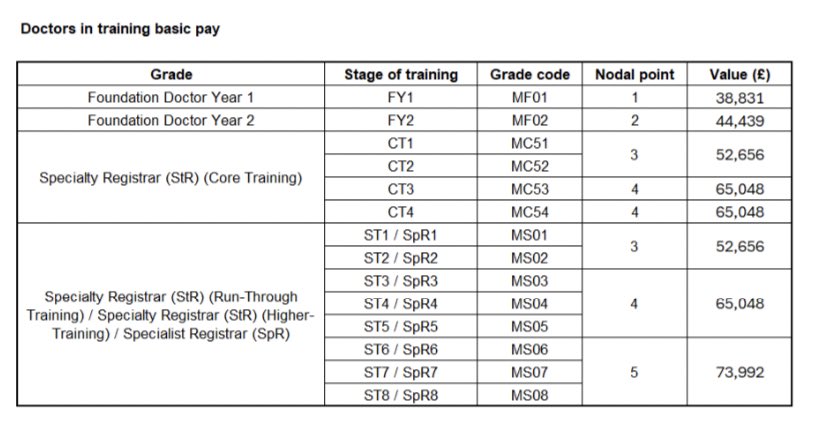
“Save Our NHS”…….🙈
Interesting to see doctors voting to support greater use of independent providers after years of protesting against “privatisation”. Imagine the reaction if a right-leaning government had proposed the same thing.
Perhaps this debate has always been a little more about pay and conditions than the slogans suggested.
bmj.com/content/393/bmj.s951
37
May 10
End of the league season 25/26 🤍
Sheffield vs Scunthorpe
Accession Play-Off Final 🩷
Henley Hawks vs Tunbridge Wells
All celebrated in traditional fashion 🥂🍺
No game and no occasion ever taken for granted 🙏

1
3
101
Apr 19
u18s Yorkshire Cup Final 🏆
Aireborough 36-24 West Park Leeds
Cracking afternoon at Castle Park
2
100
Mar 26
Please support Cameron’s fundraising effort if you can……
My name is Cameron & me and my carer Debbie are planning to cycle the 100 mile distance from Selby to Skegness on our exercise bikes.
I am 18 years old, and have a brain injury caused by a serious car accident.
@YorkshireAirAmb saved my life when I was 6 years old. I was in a serious car accident and the Yorkshire air ambulance transported me to Hull hospital where I was stabilised.
If I hadn’t been air lifted to hospital, I wouldn’t have survived.
I want to raise money to help them carry on doing the amazing work they do and helping other people like me across Yorkshire.
👇👇👇👇👇
justgiving.com/page/camerobc…
1
111
Mar 13
There is NO Head Injury Assessment (HIA) in community rugby!!
I recently watched the @benyoungs09 @BBCSport documentary “How Safe is Rugby” and noted some potentially misleading comments on junior rugby concussion protocols.
A first aid leader stated: “Much like a HIA in the professional game, we follow the same guidance.”
This simply isn’t accurate and can lead to confusion.
There is NO HIA in community rugby-including juniors, amateurs, and national leagues.
4
8
24
10,258
Mar 13
Players cannot return to play under Recognise & Remove guidelines until they’ve completed the full Graduated Return to Activity and Sport (GRAS) programme.
More details:
englandrugby.com/run/player-…
1
1
376
Mar 13
And to answer the question, would I let me children play rugby..,,,
100%, yes!!
🧵end.
1
304
Jan 25

🖐️ Developmental note:
• Around 9–12 months: babies often begin turning pages (usually several at once).
• By 18–24 months: many can turn pages one at a time.
That’s fine motor skills independence developing.
183
The Decline of Therapeutic Walking in NHS Pediatric Physiotherapy: A Call for Advocacy
Therapeutic walking - once a cornerstone of promoting physical activity and potential - is increasingly being sidelined.
This isn’t merely a matter of reduced therapy sessions; it’s a systemic reluctance to prescribe essential equipment like walking frames, often justified by service pressures, limited budgets, commissioner cuts, and even the closure of key suppliers such as NRS Healthcare.
These constraints are compounded by an unwillingness to provide families and schools with the necessary training to integrate walking into daily life. The result? Children are denied opportunities to build strength, maintain posture, and prevent secondary complications.
Walking, for many, is an emotive goal deeply cherished by families. I fully understand the need to manage expectations and align on meaningful, documented goals. Yet, we must ask: Shouldn’t physiotherapists be champions of physical activity in all its forms? And shouldn’t senior leaders and experienced clinicians push back against these pressures rather than concede to them?
In my experience, this concession manifests in subtle but profound ways. I’ve intervened in numerous cases where, without my persistence and those “difficult conversations” with fellow therapists, walking would have been entirely removed from a child’s program. I’ve been labeled “unprofessional” or accused of “living in a different world” for advocating continued access. This pushback forces me to self-reflect: Am I out of touch? Or are we collectively failing to uphold our professional duty to explore every avenue for a child’s development?
One particularly concerning development is the emergence of scoring-based assessment forms in some services, designed to “objectively” determine eligibility for walking frames. These tools evaluate elements of standing and walking, assigning numerical scores that often lead to denial of equipment. Proudly shared in professional forums, they’re touted as evidence-based due to their structured format. However, having seen them in action, I find them deeply subjective and non-standardised. They undermine the therapist’s autonomy - the clinical reasoning we’re trained to exercise as independent professionals.
For instance, if a child’s walking requires support or isn’t deemed “functional,” it’s frequently dismissed. But how can we measure progress without exposure to the activity?
In one case, such a form was used to deny a walker, claiming the child didn’t meet criteria. Fortunately, due to the child’s home and school spanning different areas, another trust provided the equipment without hesitation. This stark discrepancy isn’t about clinical absolutes; it’s a postcode lottery driven by localized service pressures. If the issue were truly definitive, why would multiple professionals, including myself, disagree so vehemently?
The human impact of these decisions is heartbreaking. Consider a child whose walking program was halted in favor of increased sitting. Children with neuro conditions often progress slowly, or the goal may simply be maintenance of skills, which is equally valid. Why abandon this so readily?
Contrast that with a success story: A young person was advised by another therapist to stop walking therapy because he “doesn’t actively weight-bear.” By persisting with a tailored program and walker, however, he achieves standing transfers and small steps at home with his parents. This fosters not just mobility, but independence, confidence, and family empowerment.
1
1
2
406
I acknowledge that in adulthood, therapeutic walking may naturally diminish as bodies grow and support structures change. But while children are smaller, more manageable, and bolstered by frameworks like EHCPs, we must seize every chance to optimize their outcomes.
Reflecting on my early NHS days provides a stark contrast. I had the privilege of working under exceptional clinical leads and clinically active band 7 physiotherapists who modeled true advocacy. They spoke up in team meetings, pressuring senior leadership to justify and preserve specialised roles focused on child outcomes. Grounded in years of hands-on experience, they possessed the knowledge, skills, and verbal dexterity to challenge top-down decisions when they conflicted with the best interests of the children we served.
Sadly, over the last 5-10 years, this model has eroded. In many services, the highest purely clinical roles now cap at band 6. For pay progression, therapists must transition to non-clinical management, immersing themselves in “service redesign,” cost-cutting, and productivity metrics. They’re rewarded for trust-level outcomes, not those benefiting families directly. This shift has created a massive skill gap, leaving newly qualified staff without seasoned clinical mentors to guide them in pushing back against restrictive policies.
I’ve witnessed so-called team leaders evade leadership altogether, even hanging up the phone rather than engaging in a challenging discussion to explain their position. It’s no wonder advocates like me sometimes appear “alien” in this environment. Without strong clinical mentorship, the next generation lacks the tools to resist the corporate culture prioritising efficiency over excellence.
Ultimately, this trend risks a lost generation of physiotherapists - and, more critically, diminished futures for the children we serve.
We must reinstate rewards for clinical excellence, restore high-level practicing roles, and rebuild a culture of mentorship.
Fellow professionals, leaders, and policymakers: Let’s reflect on our core mission. Are we promoting physical activity and potential, or merely managing decline?
92
Feb 17
Today we celebrate Shrove Tuesday - a day of reflection, repentance, and maybe a few extra pancakes 🥞✨
As we prepare to enter Lent, it’s a time to pause, reset, and think about what we can let go of - and what we can grow into.
Whether it’s prayer, fasting, giving, or simply being more intentional, the next 40 days are an opportunity for renewal.
Wishing everyone a meaningful Lenten season filled with grace, discipline, and hope. 🌿✝️
81
4/
Play isn’t a break from learning — it is learning. Through play, children develop the physical foundations needed for writing, reading, attention, and self-regulation. You can’t separate learning from movement at this age.
1
1
71
8/
This isn’t about lowering standards or delaying learning. It’s about recognising that young children learn best when their bodies are allowed to move — not when movement is restricted too early.
1
50
9/
So the question is simple:
Should England follow the evidence — and the lead of Scotland and Wales — and protect play in early primary classrooms?
Or continue expecting five-year-olds to learn in ways their bodies aren’t ready for?
🔗 Read more: bit.ly/4qPpKiX
#PlayIsLearning #LearnThroughPlay #KS1 #ChildDevelopment #ParentCampaign #Netmums
1
42