
General internal medicine resident @ University of Manitoba
Joined December 2019
- Tweets 242
- Following 612
- Followers 55
- Likes 18
Photos and videos
David Snider retweeted

21 May 2021
💥What is Monoclonal Gammopathy and when does it’s presence indicate presence of cancer?
💥What is MGUS and MGRS?
#Onconephrology
1/
10
106
276


David Snider retweeted

28 Mar 2021
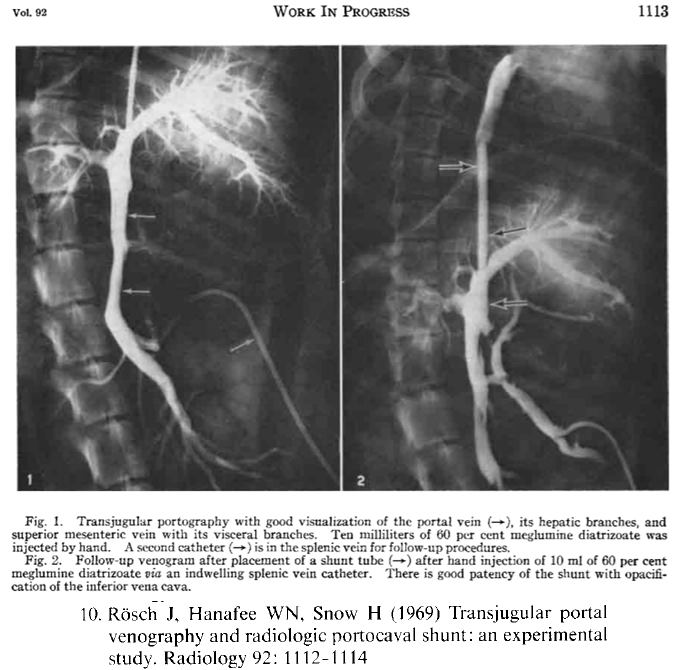
1/
HOW long do you live with #cirrhosis?
WHERE did MELD Score come from?
WHAT is a "TIPS"?
ARE you ready for re-#tweetorial
#livertwitter #medtwitter #meded
17
187
484

21 Mar 2021
Nephro attending: You'll always be surprised at what an NSAID will do to the kidneys in a volume depleted state
1
21 Mar 2021
Screening in ED o/n: How to screen in 1-2min
- referral reason
- HPI: substrate (function, relevant comorbidities), CC tempo of illness -> severity at 1st medical contact (VS pertinent labs/rads) -> tx(s) and responses
- your exam
1/
1
21 Mar 2021
2/
- provisional dx with key supporting features and focused ddx focused on life-threatening, treatable, and common conditions
- dispo (admit vs. not, ward, tele, ICU) w/ comment on anticipated course
1
5 Mar 2021
In neuro clinic:
- role of EEG in seizure is to delineate pattern of epilepsy, prognosticate first time seizure and rule out NCSE
- if unprovoked seizure, normal neuroimaging and equivocal EEG, repeat once with sleep-deprived EEG and if nothing don’t tx with AED
1/
1
5 Mar 2021
2/
- if two unprovoked sz >24h apart, EEG isn’t going to change management so don’t order
- it’s possible to get secondary migraines (I.e. AVM associated) so there’s a role for neuroimaging as you may be able to cure it
- abn neuroimaging and/or EEG in setting of sz warrant AED
1
David Snider retweeted
4 Mar 2021
💥 Tweetorial on ‘Cryoglobulinemia’
⚡️What are Cryoglobulins?
⚡️When should a clinician suspect Cryoglobulinemia & Cryoglobulinemia vasculitis?
⚡️How to establish the diagnosis?
⚡️Significance of Rheumatoid Factor
1/
@GlomCon
#Onconephrology
18
232
521
David Snider retweeted

3 Mar 2021
1/ Typical clinical reasoning exercises start with patients who give symptoms —> other historical information —> one-time physical exam —> one-time labs/imaging (sometimes more) —> diagnosis
4
11
42
David Snider retweeted

3 Mar 2021
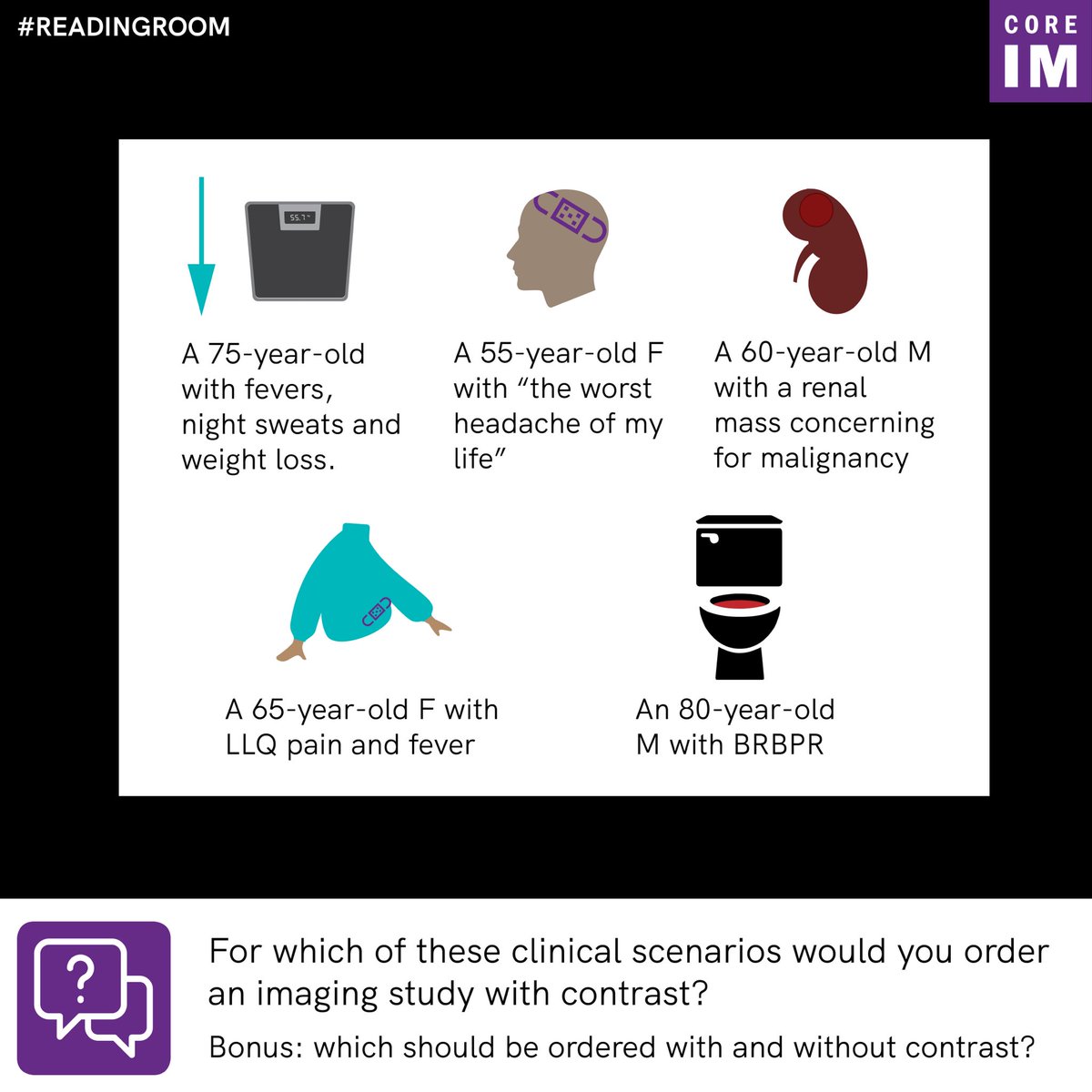
1/ Good evening, #MedTwitter, and welcome to the latest installment of #ReadingRoom! Our patient is about to head down to the scanner, and we need to protocol this CT with IV contrast. Of the options below, which ones would you want with IV contrast? Why?
2
20
51
2 Mar 2021
In endo clinic:
- think of TGs separately from other lipids: they are fuel for muscle and adipose tissue and travel in blood via chylomicrons
- insulin facilitates LPL which allows uptake of TGs into these tissues
- insulinopenic states generally have high TGs
1/
1
3 Mar 2021
3/
- I say all this because when I order a lipid panel I never now what to think of the TG level and how it pertains to the other cholesterol levels
- now I think of them as a separate and somewhat unrelated entity
2 Mar 2021
In heme clinic: HAS-BLED used for bleeding risk in pts being tx'd for VTE, but remember the HAS-BLED was studied in older pts and may overestimate risk of bleeding. #MedEd
1
1
David Snider retweeted

28 Feb 2021
Let's do a new tutorial
GI-Bleeding for non-endoscopists
#MedTwitter #GITwitter #livertwitter #ICU #FOAMed
@stevenbollipo @drkeithsiau @ebtapper @jaumebosch9 @GI_Pearls @DrHarryThomas (these are endoscopists)
2
18
71