
Medical Oncologist. "Targeted therapies for targeted populations”
Joined June 2014
- Tweets 1,947
- Following 372
- Followers 2,873
- Likes 3,475
236 Photos and videos





Pinned Tweet

23 Jan 2021
Personalized Antibodies for Gastroesophageal Adenocarcinoma (PANGEA): A Phase II Study Evaluating an Individualized Treatment Strategy for Metastatic Disease cancerdiscovery.aacrjournals…
5
25
105
11 Jun 2025
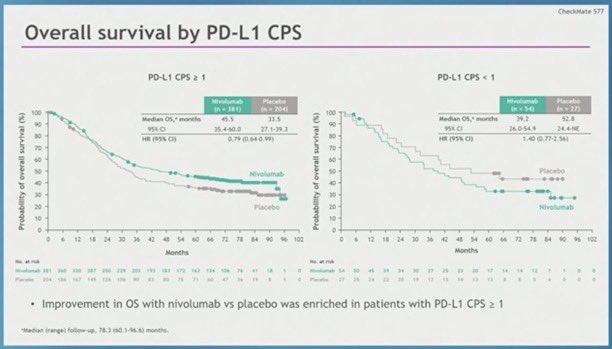
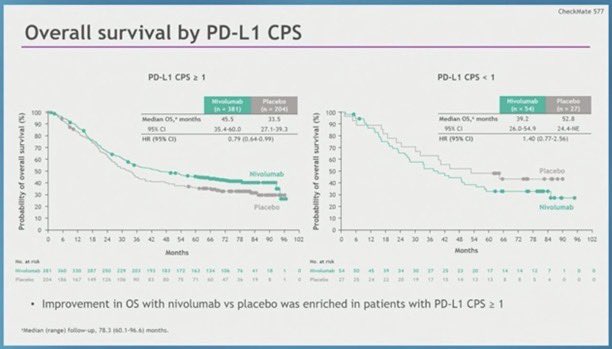
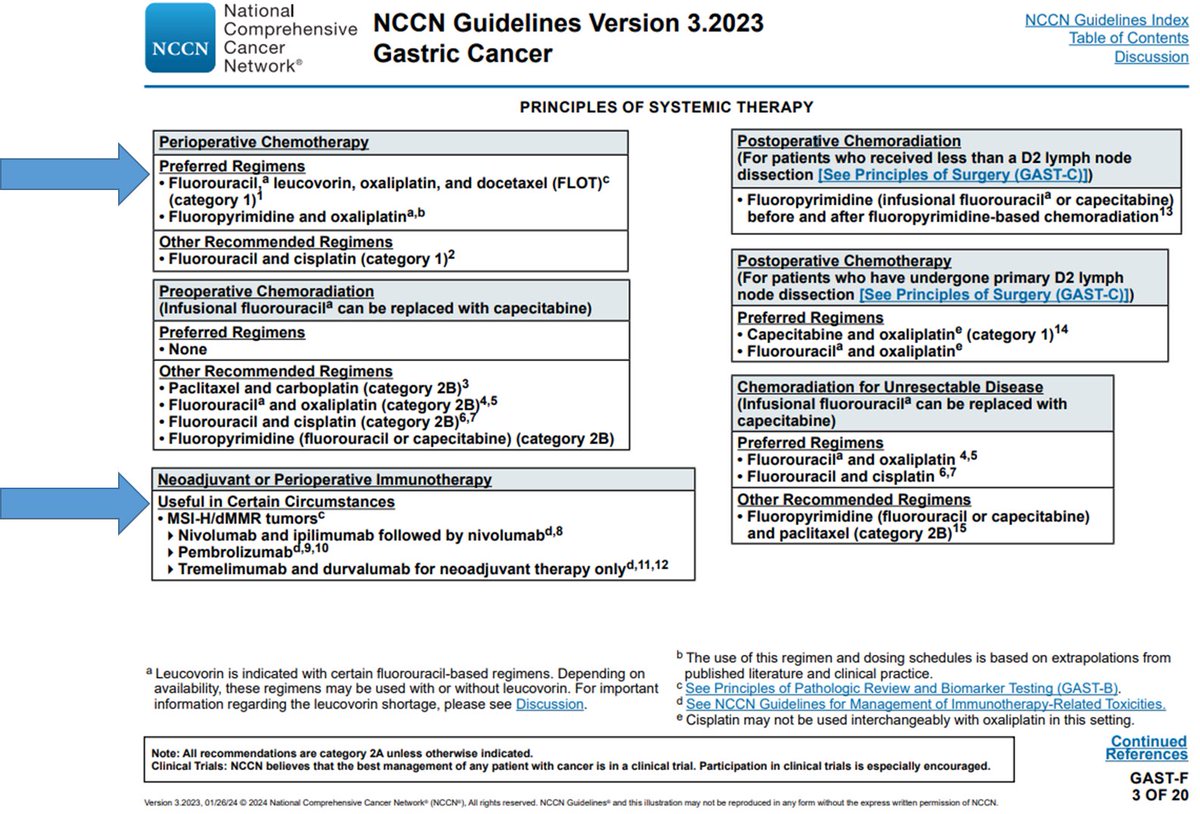
#CM577
If only we could have known years ago, maybe we could’ve spared all those patients ineffective (worse than nothing?), toxic expensive therapy.
1 Apr 2021

#CM577 there is no benefit (especially CPS0) in CPS low/neg tumors. 44% of pts. And this is not even by histology which would make adenocarcinoma look even worse. Why is this buried in the supplement? & Why would you give this drug for a year to people having no benefit?
1
5
17
3,402
11 Jun 2025
11 Jun 2025
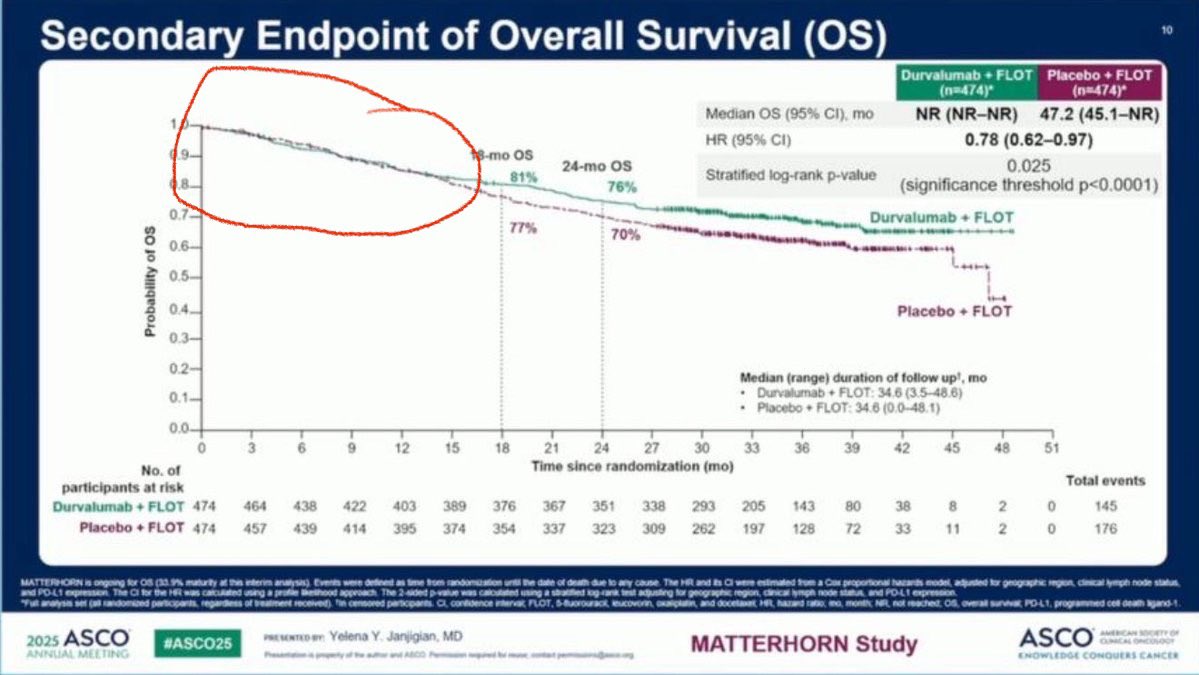
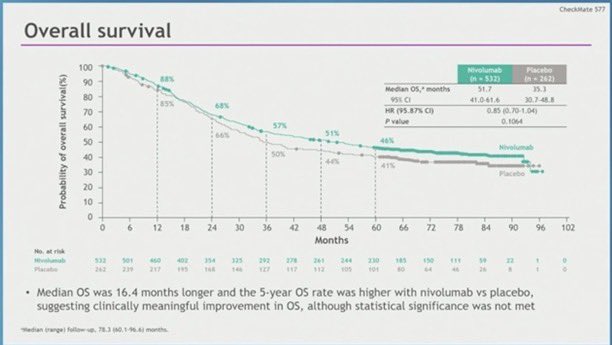
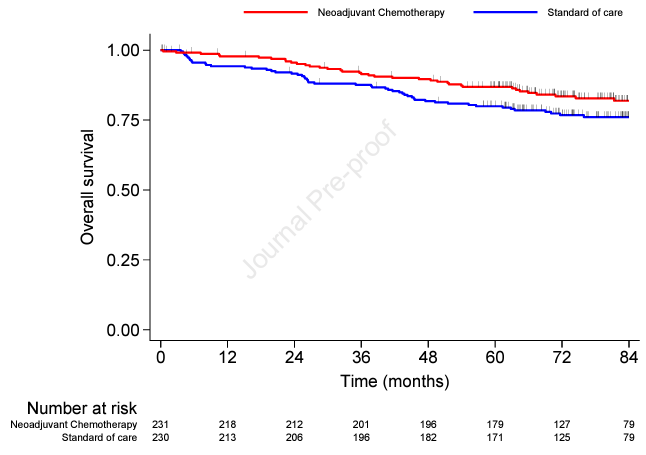
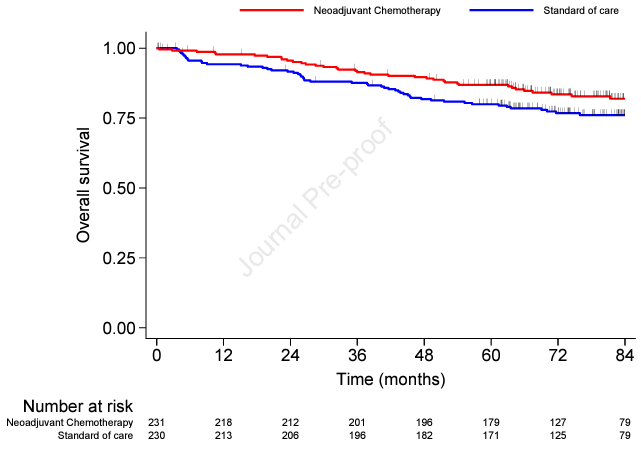
HR 0.78 NS per the presentation but not in the paper (rather HR 0.99 <12m HR 0.67) >12m)
Where have we seen this tuning fork curve before? ~1/3 pts no diff. CM577
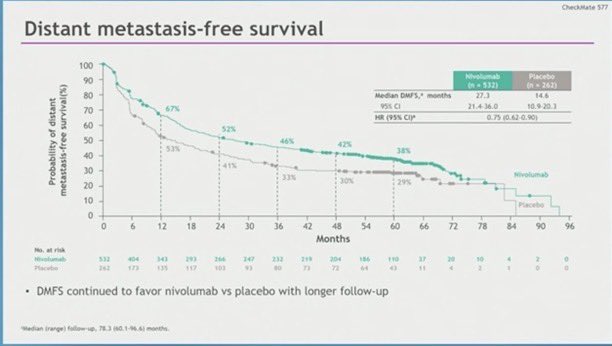
I think it’s a good idea to see the results by PDL1 1, 5, 10: will likely show same thing as all previous studies
4
12
892
28 Sep 2024
Better late than never, I guess.
28 Sep 2024

📢 FDA ODAC gets it ✅️ for patients
Immune checkpoint inhibitors are a PD-L1 targeted 🎯 therapy in GEA.
No target, no efficacy.
Let's focus on:
➡️ alternative targets (CLD 18.2, FGFR2b, MTAP...)
➡️ overcoming immune evasion (bispecifics, T-cell engagers, CAR-T..)
1
1
10
1,555
Daniel Catenacci retweeted

11 Jul 2024
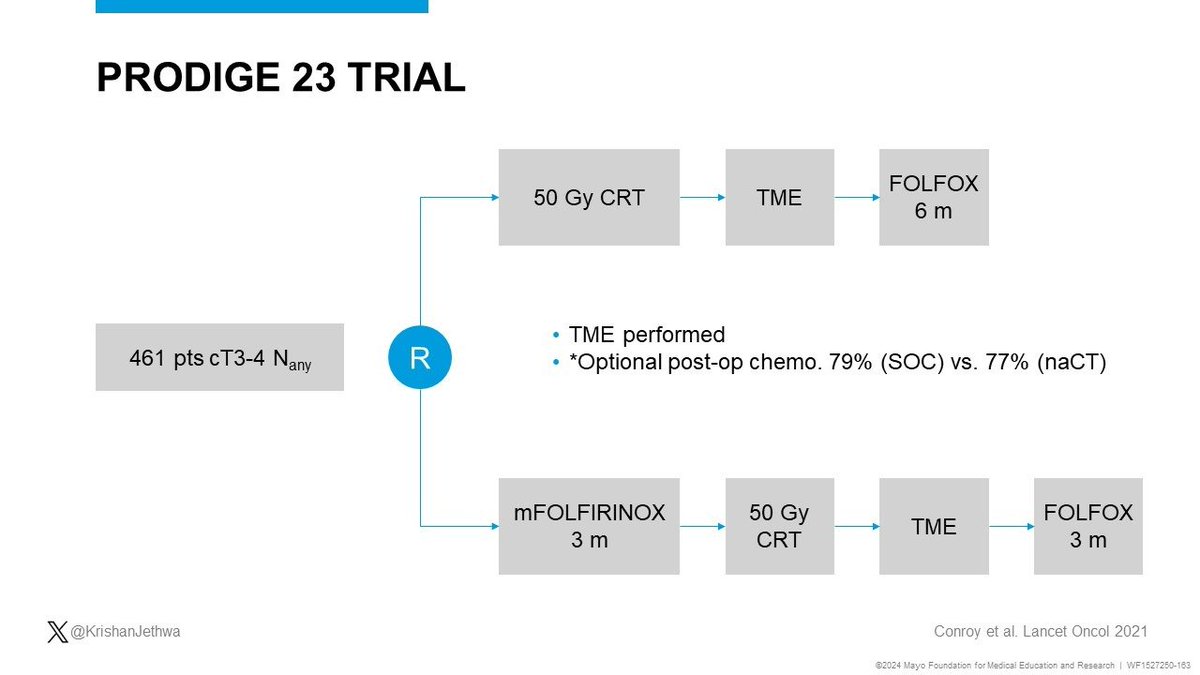
🚨PRODIGE23🚨
Long term results now published!
T3-4 rectal adenocarcinoma
Randomized:
CRT➡️🔪➡️FOLFOX
mFOLFIRINOX ➡️ CRT➡️🔪➡️FOLFOX
✅✅✅Improved OS!!!
Looking forward to JANUS clarifying if TNT with FOLFIRINOX vs. FOLFOX improves cCR and/or DFS/OS
pubmed.ncbi.nlm.nih.gov/3898…

2
97
216
18,943
10 Jul 2024
#SPOTLIGHT #GLOW #Zolbetuximab #Vyloy
"Zolbetuximab BLA resubmitted 5/9/2024, after CRL issued on 1/4/2024 by FDA due to 3rd-party manufacturer deficiencies seen during the pre-license inspection of the facility." Target Action Date: 11/9/2024
newsroom.astellas.us/2024-05….
1
1
10
1,429
10 Jul 2024
Already Approved in Japan 3/26/24. Different manufacturing sites for the two countries hopefully??
astellas.com/en/system/files…
4
310
14 Jun 2024
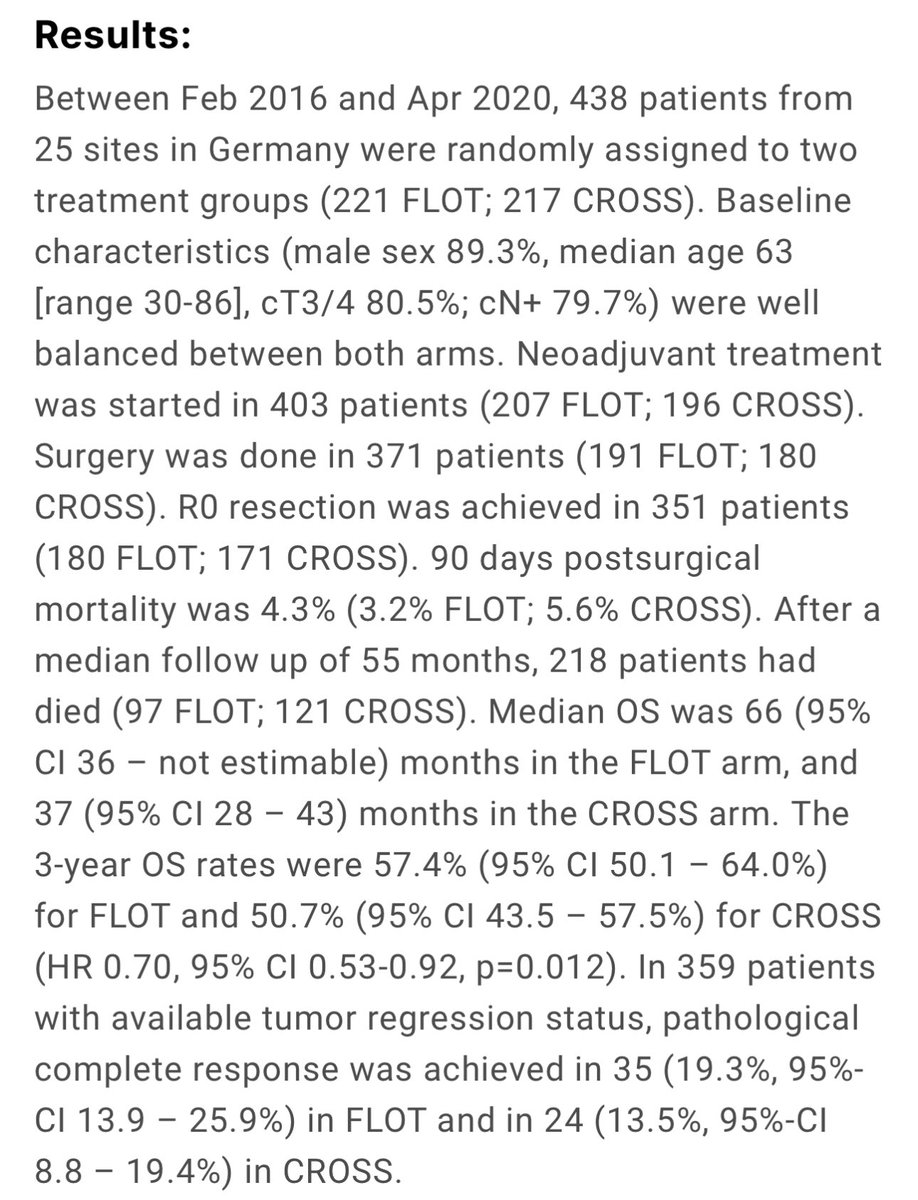
Thank you for this very pivotal study to streamline perioperative therapy for esophageal and gastroesophageal junction adenocarcinoma. #ESOPEC

🔥 ASCO 2024 Plenary: Prof Dr @JDekervel (UZ Leuven) and Prof Dr @FlorianLordick (University of Leipzig) discuss the ESOPEC trial, comparing FLOT perioperative chemotherapy with neoadjuvant chemoradiotherapy for adenocarcinoma of the oesophagus or oesophagogastric junction.
1
10
2,041

🔥 ASCO 2024 Plenary: Prof Dr @JDekervel (UZ Leuven) and Prof Dr @FlorianLordick (University of Leipzig) discuss the ESOPEC trial, comparing FLOT perioperative chemotherapy with neoadjuvant chemoradiotherapy for adenocarcinoma of the oesophagus or oesophagogastric junction.
1
3
13
4,290
Daniel Catenacci retweeted
4 Jun 2024
Yes research warranted, not SOC. Control here arm did very well compared to overt stage IV disease, as expected, since these are highly selected patients. This control arm is so critical because it normalizes and shows that they do well, but not due to the surgical intervention.
1
1
593
4 Jun 2024
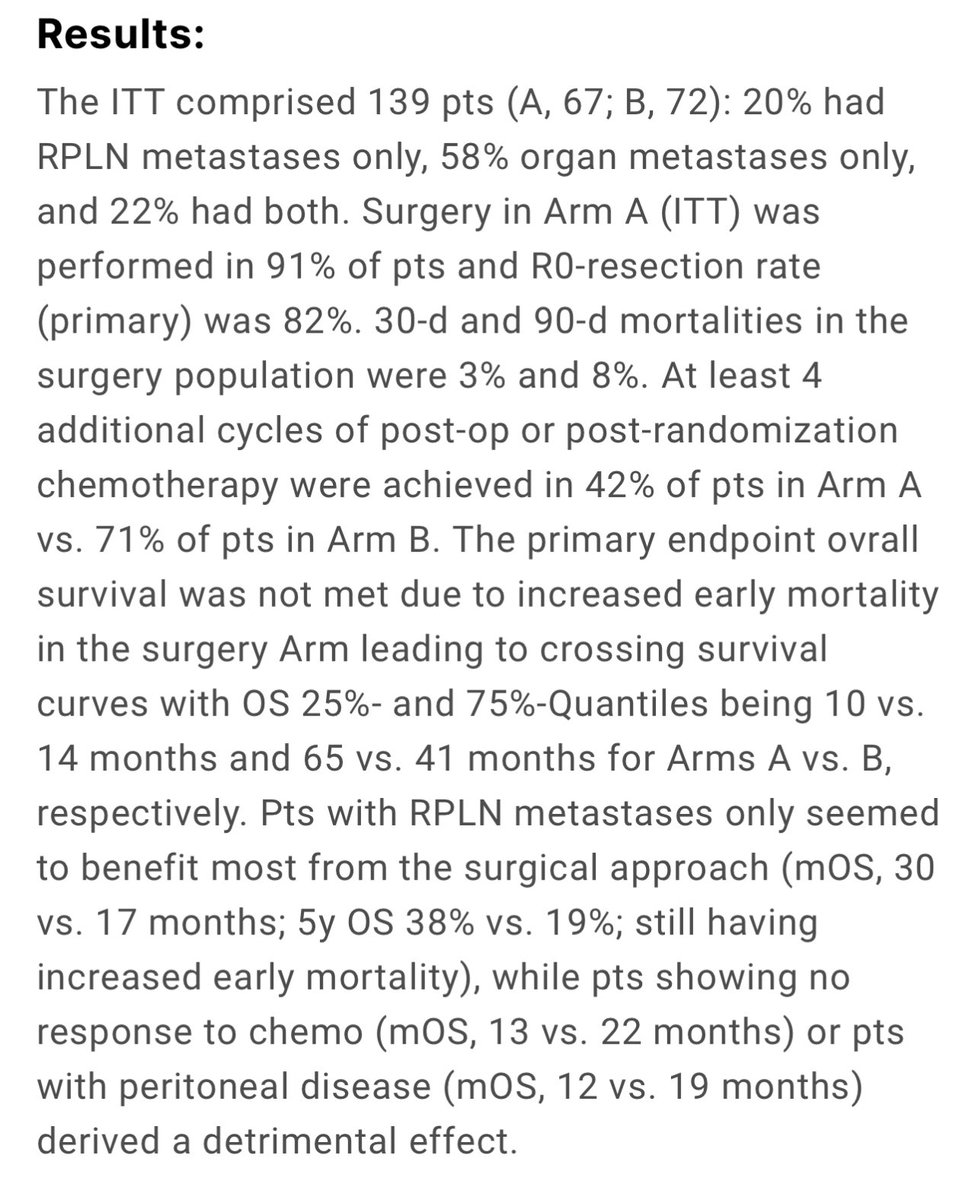
IKF-575/#RENAISSANCE phase III
Addressing #oligometastatic #GEA more aggressively, my heart said yes, but my brain said no:
3
10
1,753
Daniel Catenacci retweeted
15 Sep 2019
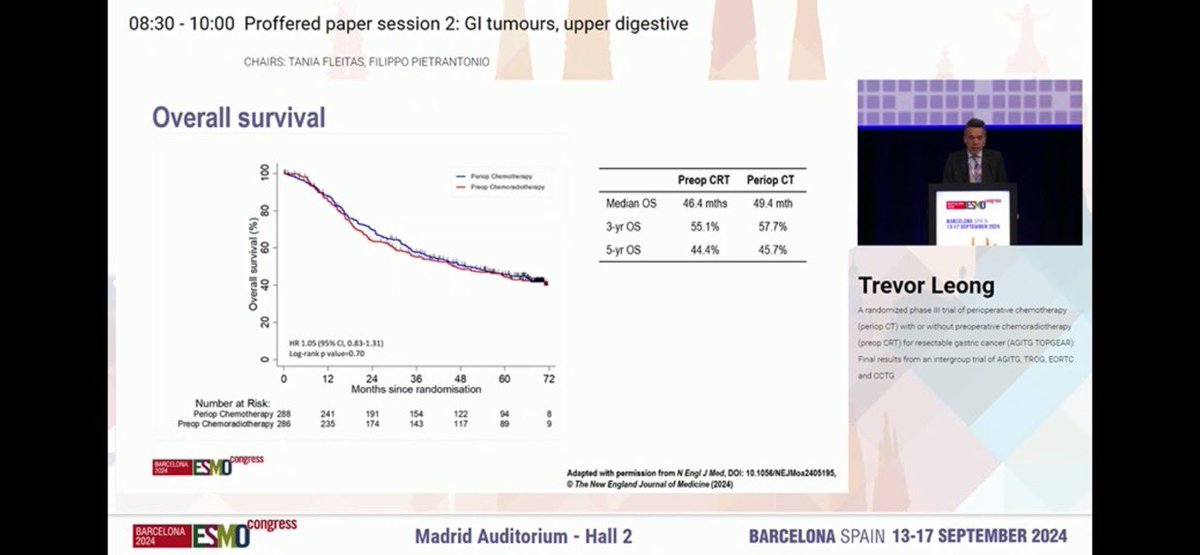
I guess we must agree to disagree until we see prospective phase 3 data. Thankfully others have actually done this study and asked this very pertinent question as to the utility of RT in EGJ AC and not danced around it for 20 years. Would you change your opinion based on esopec?
1
2
Daniel Catenacci retweeted
15 Sep 2019
Do you call the benefit of CROSS over surgery alone ‘modest’ with a HR of 0.75? FLOT had HR of 0.76 over ECF which previously had a HR of 0.74 over surgery alone. There is nothing more to say. Ultimately you either see it and it is obvious or you dont. But you eventually will.
1
2
4
Daniel Catenacci retweeted
15 Sep 2019
Unfair comparison of ITT R0 in FLOT vs R0 of those going to surgery in CROSS. Also,Why compare surrogate endpnts of OS when we actually have the OS to compare? The controlled studies are coming.Will be some disappointed folks likely. See here: meetinglibrary.asco.org/reco… @RenoHemonc
14 Sep 2019

1
1
5
Daniel Catenacci retweeted
17 Sep 2020
Looking forward to debating Dr Ilson!! (FLOT vs CROSS #31.)@agrothey @ILSONDavid
17 Sep 2020

Looking forward to discussions with my colleagues during Great Debates in GI Malignancies next week! @GreatDebatesGI
4
5
29
Daniel Catenacci retweeted
11 Jun 2021
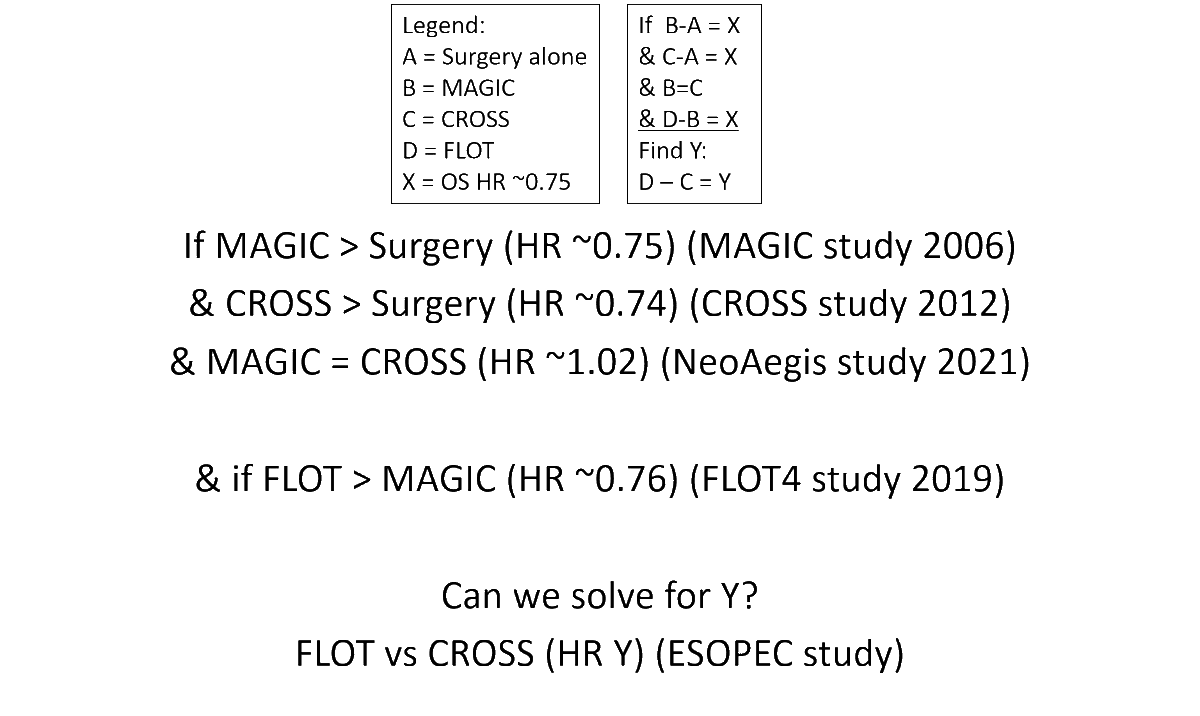
#justmath
I particularly like the comment that this is homework for 9-yr olds...@GermanBiotech
CROSS-trial comparisons r tricky, but it's the HR compared to controls that are useful here...
Of course we await ESOPEC, but for now, the evidence points in a certain direction...no?
3
4
21
Daniel Catenacci retweeted
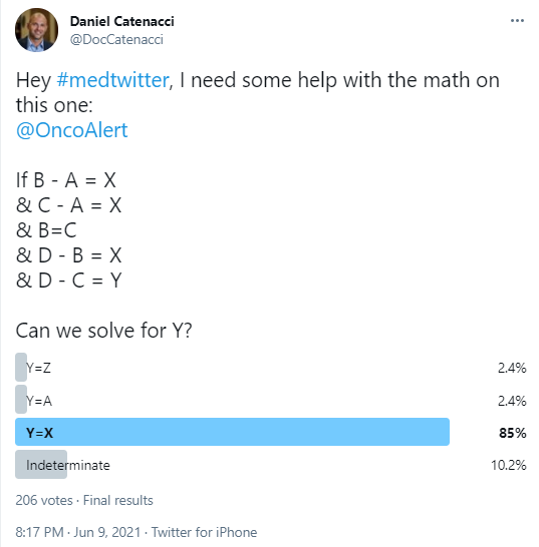
10 Jun 2021
Hey #medtwitter, I need some help with the math on this one:
@OncoAlert
If B - A = X
& C - A = X
& B=C
& D - B = X
& D - C = Y
Can we solve for Y?
2%
Y=Z
2%
Y=A
85%
Y=X
10%
Indeterminate
206 votes • Final results
8
2
9
Daniel Catenacci retweeted
3 Jun 2024
Last, I would say that ~90% of pts will have a PET response w FLOT, & we saw this also w FOLFIRINOX. These pts are not at risk for R1 resection. One might consider CROSS for those ~10% who don’t, with the caveat that those are the resilient tumors that may also be radioresistant.
1
1
6
682
Daniel Catenacci retweeted
3 Jun 2024
Tweet 6/6:
From tweet 5/6, if we have a prospective study that seeks organ preservation, documents differences in QOL, & risk of local/distant recurrence & OS comparing dCRT vs, hopefully what is now everyone’s standard, perioperative FLOT, then great, & pts can make a choice.
1
1
6
683