
Joined July 2019
- Tweets 267
- Following 142
- Followers 190
- Likes 201
6 Photos and videos



Laura Donlin retweeted

26 Nov 2023
Julian Voss-Andreae is a quantum physicist-turned-sculptor. His work is heavily influenced by his background in science and his blending figurative sculptures can vanish in front of our eyes
x.com/SalemTheCats/status/16…
583
18,477
145,735
14,449,779
Laura Donlin retweeted

17 Nov 2023
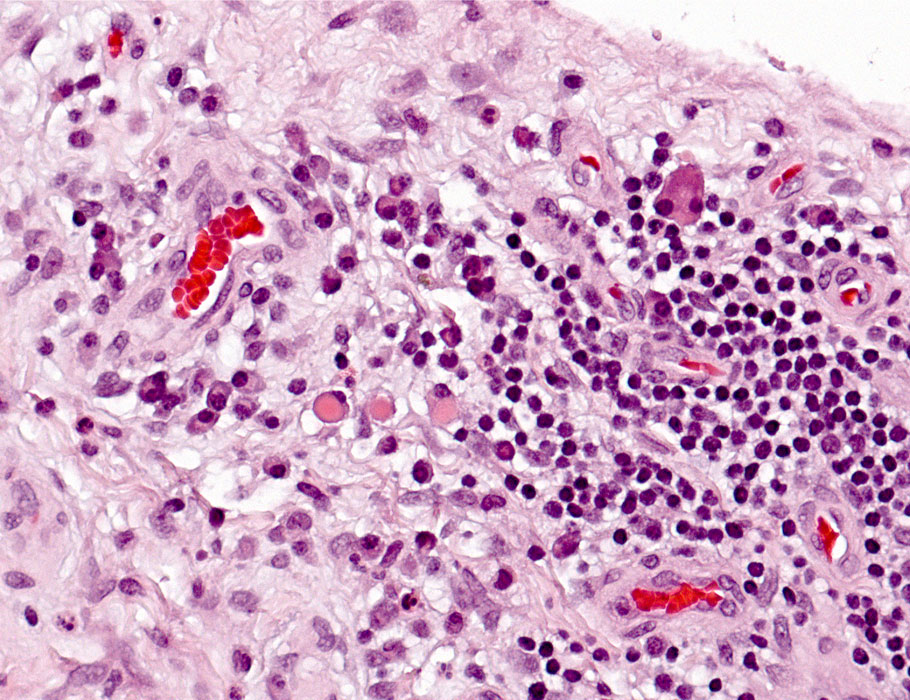
"This collaborative study - across HSS, MSKCC and Harvard University - now reports what cell types are activated in autoimmune arthritis caused by cancer immunotherapies." — Laura Donlin, PhD #RheumTwitter pubmed.ncbi.nlm.nih.gov/3750…
3
6
766
Laura Donlin retweeted

11 Nov 2023
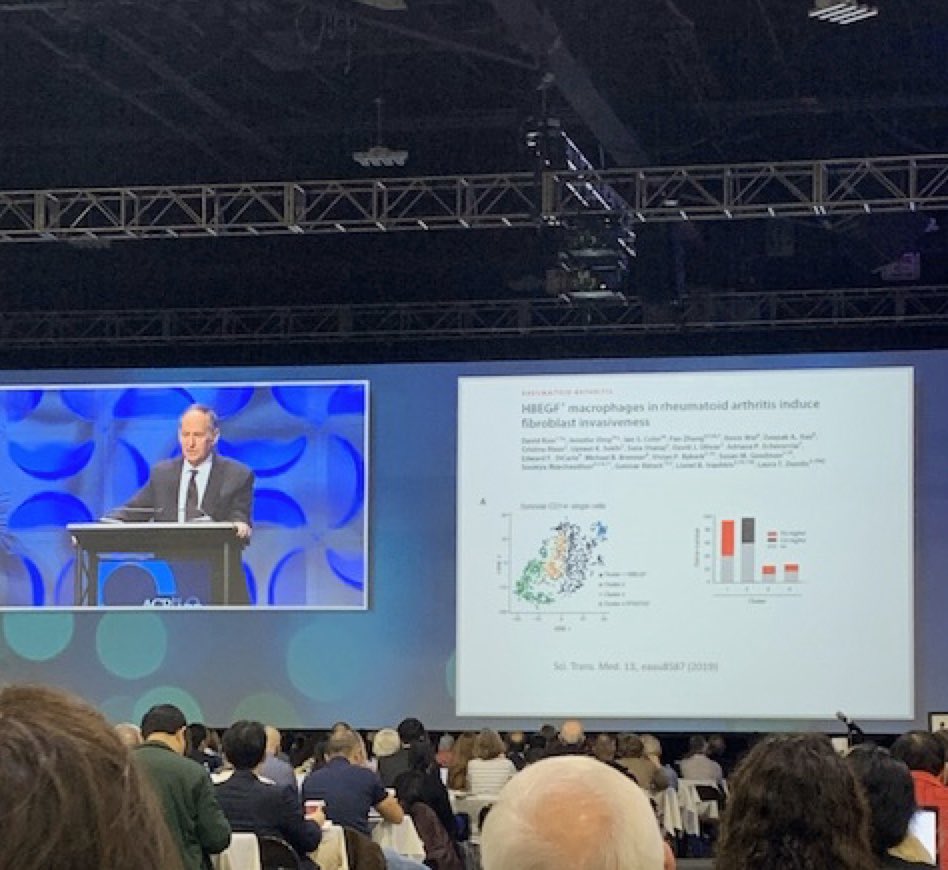
Glad to see that our #RheumatoidArthritis cell atlas could reveal some pain-related signaling pathways, like HBEGF @Donlinlab 🌟
11 Nov 2023

Work from @CURheumatology by @FanZhang_Jessie and @AHelenaJonsson1 already being referenced at #ACR23 Basic & Clinical Research Conference! Super proud of the work by our faculty. 🤩

1
2
645
Laura Donlin retweeted

15 Nov 2023
The #checkpoints enjoying a last night out after #ACR23 @Donlinlab @Deepakarao @cappelliMD . Science takes a village

1
17
1,222
Laura Donlin retweeted

Finally, I thank all of my amazing colleagues for putting this resource together. Too many to list by name, but especially @FanZhang_Jessie, @AHelenaJonsson1, @aparnanathan, @nghia_millard along with Kevin Wei, @Deepakarao, @Donlinlab, @jenanolikMD, and Michael Brenner.
1
2
585
Laura Donlin retweeted
8 Nov 2023
Excited 🙌 to see our highly collaborative work out today at @Nature @FNIH_Org @NIH_NIAMS nature.com/articles/s41586-0… with @AHelenaJonsson1 @soumya_boston @jenanolikMD @Deepakarao @Donlinlab and Brenner and NIH AMP network!! @CURheumatology @CUBiomedInfo @CUAnschutz
8 Nov 2023

🆕 New in @Nature!
Dr. Raychaudhuri (@soumya_boston) and collaborators including @jenanolikMD, @Donlinlab, and @Deepakarao constructed a comprehensive RA #synovial tissue reference that revealed diverse cellular composition. @BrighamWomens
📖 Full story: bit.ly/46a8V70



12
39
9,177

Nature research paper: Deconstruction of rheumatoid arthritis synovium defines inflammatory subtypes go.nature.com/49vlhJO
1
22
67
32,816
Laura Donlin retweeted

8 Nov 2023
🆕 New in @Nature!
Dr. Raychaudhuri (@soumya_boston) and collaborators including @jenanolikMD, @Donlinlab, and @Deepakarao constructed a comprehensive RA #synovial tissue reference that revealed diverse cellular composition. @BrighamWomens
📖 Full story: bit.ly/46a8V70
1
10
32
14,268
Laura Donlin retweeted
26 Oct 2023
"Moving towards a liquid biopsy for Rheumatoid Arthritis synovitis–analysis of computer-automated histology reveals tissue inflammation is associated with immunoglobulin skewing in blood." — Dana Orange, MD, MS #RheumTwitter pubmed.ncbi.nlm.nih.gov/3746…
2
2
598
Laura Donlin retweeted

14 Aug 2023
Moving towards a liquid biopsy for Rheumatoid Arthritis synovitis-our updated computer-automated histology pipeline revealed immunoglobulin skewing in synovium is reflected in the blood….
acrjournals.onlinelibrary.wi…
4
25
2,830
Laura Donlin retweeted

7 Aug 2023
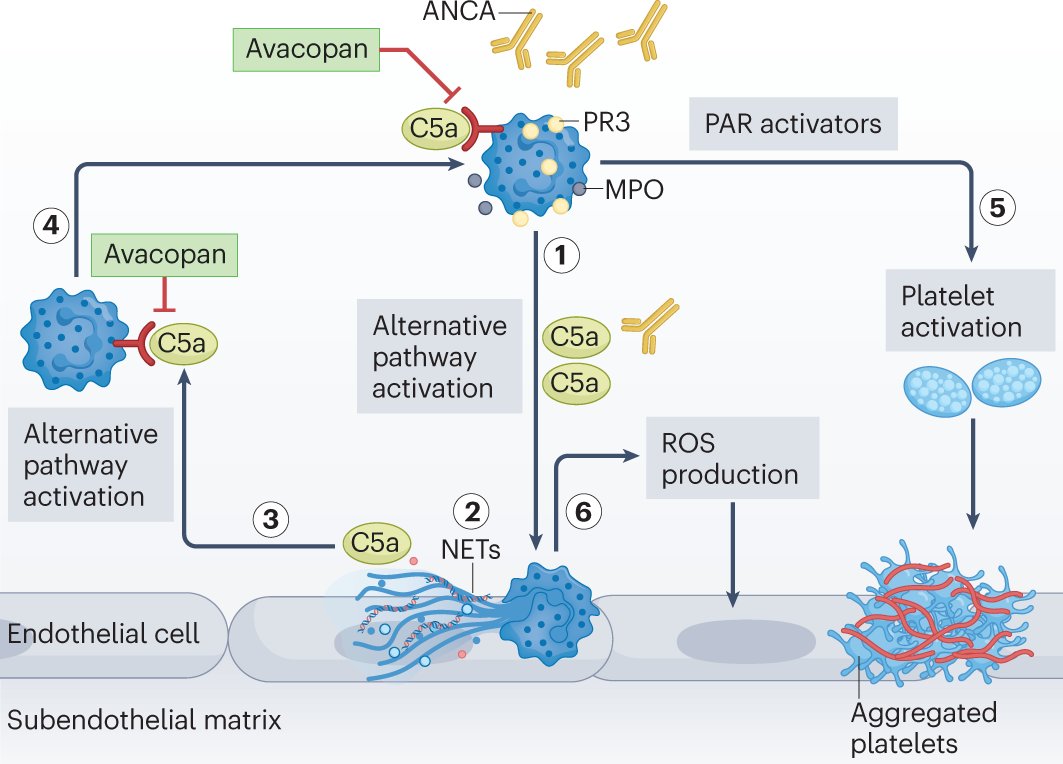
#AugustIssue | Michael Holers describes the #complement system and its role in #rheumatic and #autoimmune diseases, and discusses complement #therapeutics in these settings, as well as prospects for improving their clinical use.
go.nature.com/3rVoNvH
40
100
10,519
Laura Donlin retweeted

29 Jul 2023
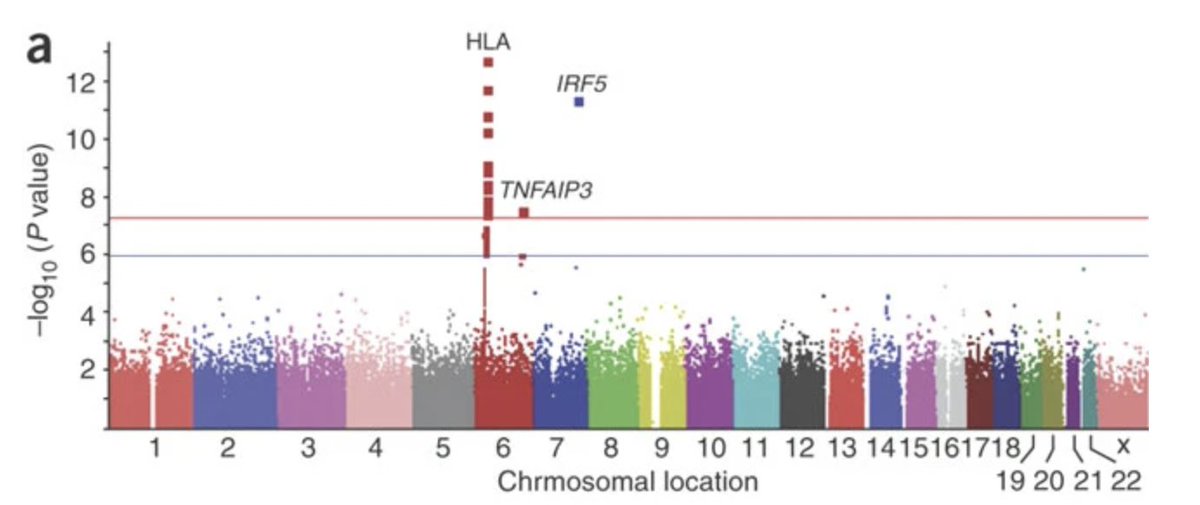
Glancing through a review of SLE genetics (tandfonline.com/doi/full/10.…), I bumped into a familiar plot, which made me revisit the beautiful work by Kamitaki et al. from 2020 on the elegant dissection of the HLA GWAS signal (nature.com/articles/s41586-0…), which is one of the fine demonstrations of the value of non-European populations, particularly Africans, in fine-mapping GWAS loci to pinpoint the causal variants.
One of the strongest GWAS signals of SLE erupts out of the HLA region in chromosome 6. Here is a Manhattan plot from a 2008 study (nature.com/articles/ng.200).
The well-known complexity of the HLA region posed a significant challenge for scientists to decode the chr 6 signal. Given that SLE is an autoimmune disease there was a valid reason to believe that SLE, like other autoimmune diseases, might be bearing a HLA risk variant. The HLA-DRB1*03:01 allele was assumed to be that variant.
But at the same time, scientists couldn't stop looking at a nearby pair of genes--C4A and C4B--that codes for one of the strongest genetic risk factors of SLE known since ages: complement 4. The earliest documentations of complete C4 deficiency in SLE patients date back to 1974 (pubmed.ncbi.nlm.nih.gov/4212…).
But then, scientists had their reasons for not betting on the C4 genes, despite its historical links to SLE. As opposed to complete C4 deficiency, partial C4 deficiency had conflicting reports of its links with SLE, which weakened the argument that commonly observed copy number variations of C4 genes (that could only partially reduce the C4 gene dosage) drive the SLE risk in the population.
Of course, one could ignore their biological intuitions and play the who's the causal variant game purely from a statistical angle. But there was a problem. The C4-B(S) allele (that lacked any C4A gene) with the highest SLE risk effect was in high LD with the HLA-DRB1*03:01 allele in the European populations. Is there a way to break this LD friendship? It turned out there is.
Unlike in the European populations, in the African Americans, the LD between C4-B(S) and HLA-DRB1*03:01 was very weak. Meaning, you can separate individuals who carry only C4-B(S) alleles and those who carry only HLA-DRB1*03:01 alleles and compare the disease risks. In doing so, the authors were clearly able to see that SLE risk was driven by C4-B(S) alleles but not by the HLA-DRB1*03:01 alleles.

2
17
96
36,528
Laura Donlin retweeted

28 Jul 2023
When dreams come true.. 😊
773
23,823
192,400
11,689,618
Laura Donlin retweeted

26 Jul 2023
Anyone who wants to study #HLA but feels hesitant as HLA is too complicated☹️? Happy to share our paper @NatureProtocols describing the up-to-date knowledge on HLA #genetics and step-by-step tutorial for HLA imputation and association with @soumya_boston🥳
nature.com/articles/s41596-0…
6
123
500
53,582
Laura Donlin retweeted
Really excited to share our latest from @kalaga27 analyzing alpha-beta paired TCR single cell data, linking T cell receptor sequence features to T cell fates. #genomics #Immunotherapy!
26 Jul 2023

Excited to share our preprint studying T cells at single-cell resolution– we find a TCR signature that makes some T cells more likely to respond to any antigen! With @soumya_boston, at @broadinstitute and @harvardmed
🧵
biorxiv.org/content/10.1101/…
3
17
4,408
Laura Donlin retweeted

28 Jul 2023
Very happy to share a part of my PhD work!
28 Jul 2023

A new study by @SingarajuAnvita @KB_PhD @Deepakarao @Donlinlab and colleagues identifies a T cell population as a reason for why some types of immune checkpoint inhibitor immunotherapies can cause arthritis to emerge in some patients.
📄: scim.ag/3wO
5
3
15
2,866

28 Jul 2023
A rewarding team effort to define how T cell activation by checkpoint therapy can result in an INDUCIBLE HUMAN AUTOIMMUNE CONDITION - which resembles rheumatoid arthritis.
28 Jul 2023
A new study by @SingarajuAnvita @KB_PhD @Deepakarao @Donlinlab and colleagues identifies a T cell population as a reason for why some types of immune checkpoint inhibitor immunotherapies can cause arthritis to emerge in some patients.
📄: scim.ag/3wO
7
30
6,913
Laura Donlin retweeted

22 Jul 2023
Penicillin kills bacteria by making them explode.
67
665
5,057
740,044
Laura Donlin retweeted

5 Jun 2023
Excited to share our work in @NatureImmunol on synovial fibroblasts in rheumatoid arthritis! A wonderful collab between @HSpecialSurgery @MSKCancerCenter with @GaoVianne @DonlinLab, Tom Norman, Christina Leslie and Sasha Rudensky. nature.com/articles/s41590-0…
4
24
94
11,718
Laura Donlin retweeted

26 May 2023
Claude Shannon was the first person to mathematically quantify how efficiently a message can be communicated. Here’s how he did it: quantamagazine.org/how-claud…
1
121
434
60,497