
Joined March 2013
- Tweets 5,428
- Following 334
- Followers 7,179
- Likes 6,729
172 Photos and videos










Rory Spiegel retweeted

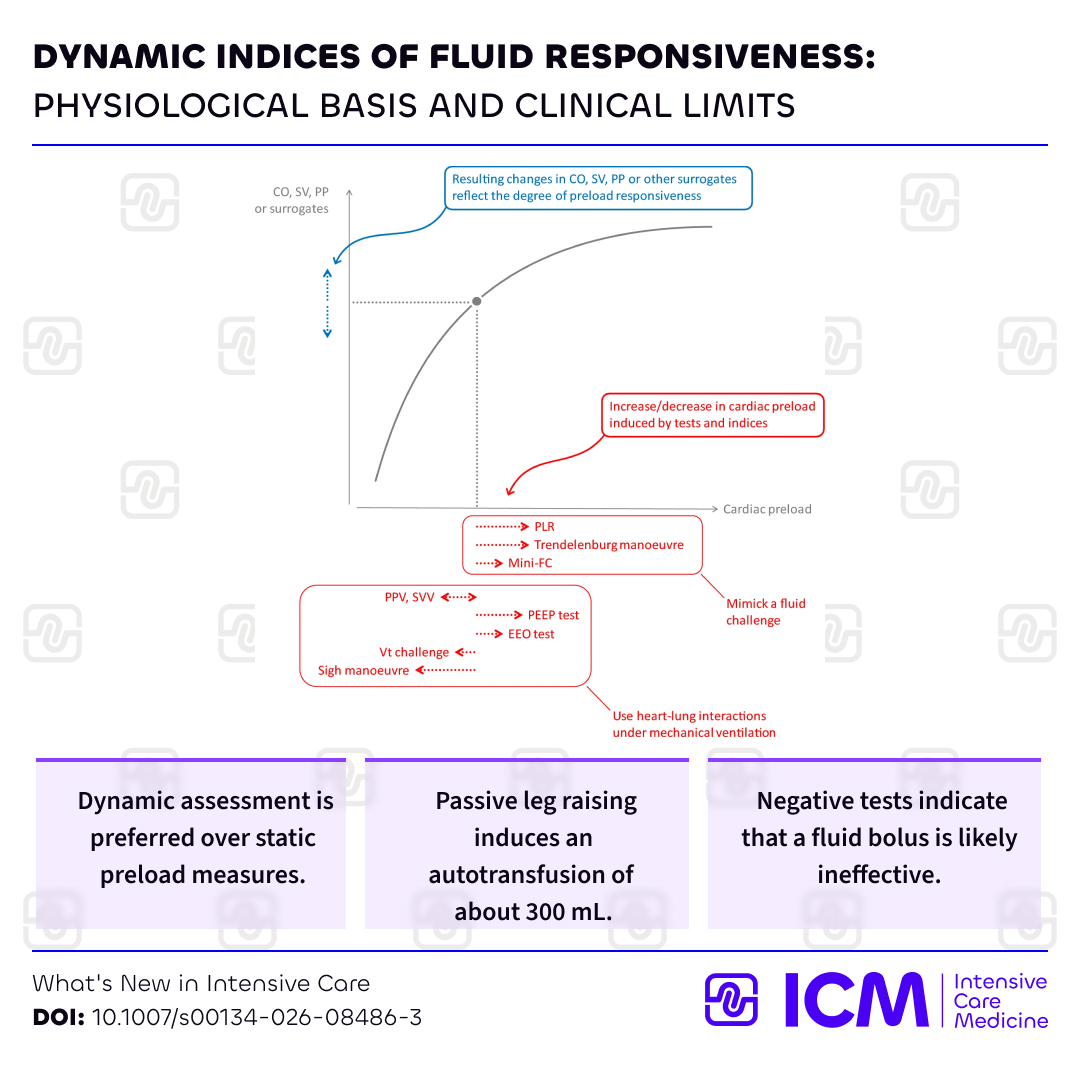
No. Check for tolerance first. Responsiveness does not equal need, nor benefit. Maximizing output was shown decades ago to not be a viable strategy. Optimize tissue perfusion. Learners, please reconsider a forward-flow-centric approach. Focus on tissue perfusion, and the two do NOT have a linear relationship. Understand hemodynamic interfaces. Ping @icmteaching @khaycock2 @EMNerd_ @edu_kattan @ross_prager

Dynamic indices of fluid responsiveness in @ICM
w/ @Prof_XMonnet @MichelleChew
💧Physiology of fluid responsiveness
📈Tests to predict fluid responsiveness
⚠️Clinical limits of these tests
Check for potential benefits before giving #fluids!
🔗rdcu.be/fnlTm #FOAM
4
16
56
5,081

Jun 12
SODa-BIC just dropped in NEJM. The large, rigorous RCT examining the use of sodium bicarbonate ICU patients with shock and acidosis.
nejm.org/doi/full/10.1056/NE…
9
26
93
11,545
Jun 12
Three placebo-controlled trials. Bicarb corrects the pH. It does not improve hemodynamics, reduce mortality, or protect kidneys. The RRT signal is clinicians using the dialysis circuit as a substitute buffer drip.
1
3
11
1,022
Jun 12
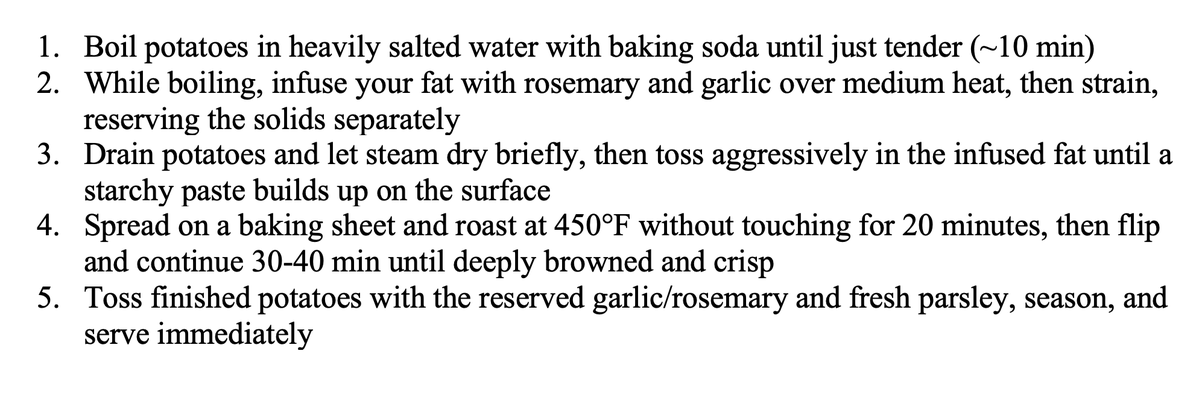
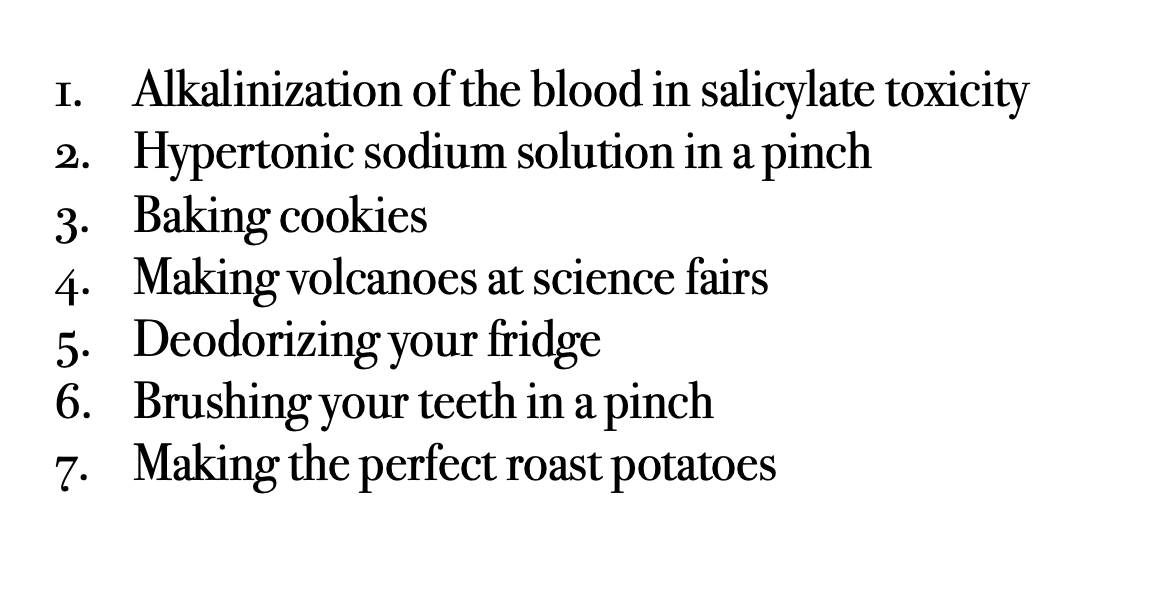
Finally I've included some times when bicarb is stil clinically useful.
7
15
53
1,619
Rory Spiegel retweeted

Jun 11
Facts, now proven in a MC-RCT.

Jun 11

30 mL/kg has never been supported by evidence and physiologically it is nonsensical to think a weight-based prescription would be beneficial. Assess the hemodynamics in front of you and treat accordingly
4
7
48
7,135
Jun 11
The ARISE FLUIDS trial was just published in the NEJM examining early IV fluids vs early vasopressors in septic shock. Just a reminder, fluids aren't the cure for sepsis
nejm.org/doi/full/10.1056/NE…
3
19
61
4,401
Jun 11
The vasopressor group received just 7 mL/kg in the first 6 hours of resuscitation and outcomes were identical. Because IV fluids are not the cure for sepsis!
3
11
961
Jun 11
30 mL/kg has never been supported by evidence and physiologically it is nonsensical to think a weight-based prescription would be beneficial. Assess the hemodynamics in front of you and treat accordingly
1
7
40
12,212
Rory Spiegel retweeted
May 27
my 2 cents on this:
1) agree w Rory
2) nonetheless, I still target 130-150. It’s impossible to fight guidelines here. This is an *improvement* to prior [disasterous] recs to target “SBP<140”
3) clevidipine would likely avoid overshoot (more intuitive to use than nicardipine)
May 27
1/A new study by Shi et al. (Ann Emerg Med 2026) questions the current AHA blood pressure recommendations for intracerebral hemorrhage.
pubmed.ncbi.nlm.nih.gov/4136…
1
9
69
24,660
May 27
1/A new study by Shi et al. (Ann Emerg Med 2026) questions the current AHA blood pressure recommendations for intracerebral hemorrhage.
pubmed.ncbi.nlm.nih.gov/4136…
1
7
34
28,361
May 27
4/ Nicardipine infusions overshot just as often as bolus dosing (55% vs 46%). When goal BP was achieved early without overshooting, outcomes were no different than never hitting goal at all.
1
1
7
1,614
May 27
5/ The retrospective design limits how certain we can be of this signal of harm. But consider INTERACT-2 and ATACH-2 found no meaningful benefit and this cohort showed what happens when these targets are actually implemented in the real-world and the potential harms associated.
1
1
8
1,481