
Author of the Internet Book of Critical Care 🖋️ Board certified in critical care, pulmonology, and neurocritical care 🤓 Zentensivist 🧘♂️ No COI 💰
Joined October 2012
- Tweets 14,183
- Following 549
- Followers 64,905
- Likes 19,201
3,660 Photos and videos









Jun 13
I've blogged about this in the past, and my position remains the same:
🤖 Specialized vs general AI models have different strengths and weaknesses. Asking which one is the "best" is probably the wrong question.
🤖 Specialized AI (eg OpenEvidence) is great for searching PubMed & guidelines. A drawback is that it may tend to anchor towards slightly older studies (rather than the cutting edge).
🤖 General AI (eg OpenAI) has superior reasoning capacity and picks up a broader range of sources. The drawback may be a higher hallucination rate and occasionally using less reputable sources.
🤖 The ideal practice is probably combining your judgement plus two LLMs. If everything is consistent, that's probably a reasonable answer. If there are inconsistencies, dig deeper into the source materials.
(Link in the post below)
Jun 12

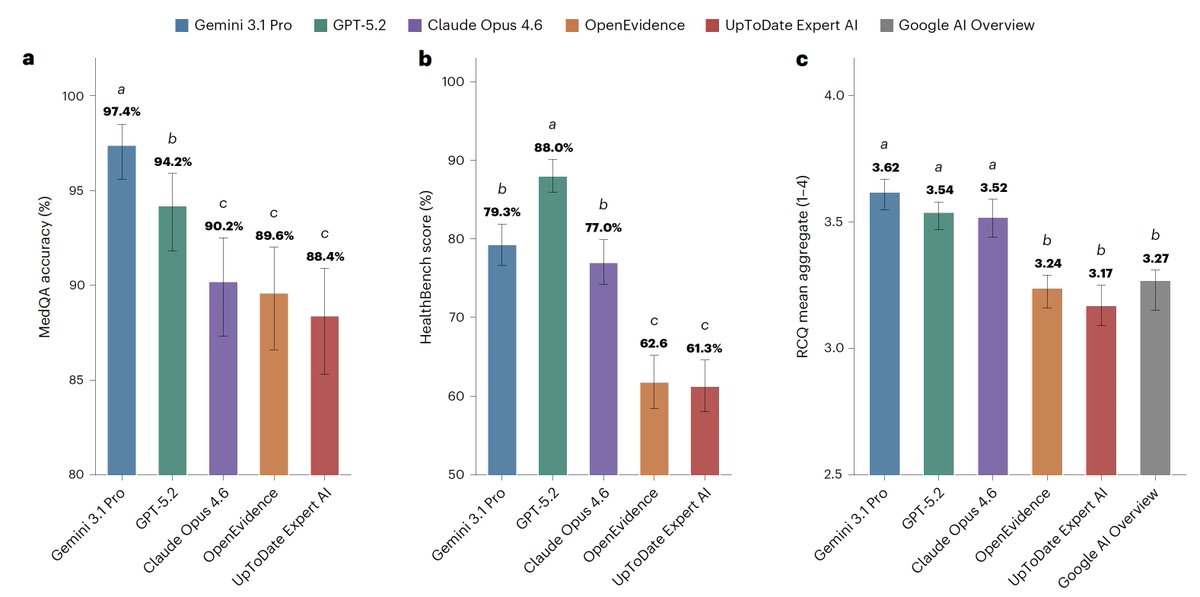
For medical information, general AI frontier models (Google, OpenAI, Anthropic) outperformed specialized @EvidenceOpen and @UpToDate as assessed by 12 US clinicians, randomized and blinded to which model and extensive testing/benchmarks. This was not anticipated. @NatureMedicine
nature.com/articles/s41591-0…
6
12
54
8,316
Jun 13
Link to my blog on narrow vs broad-spectrum AI in medicine:
emcrit.org/pulmcrit/triple-t…
1
5
943
Josh Farkas MD 💊 retweeted

Jun 11
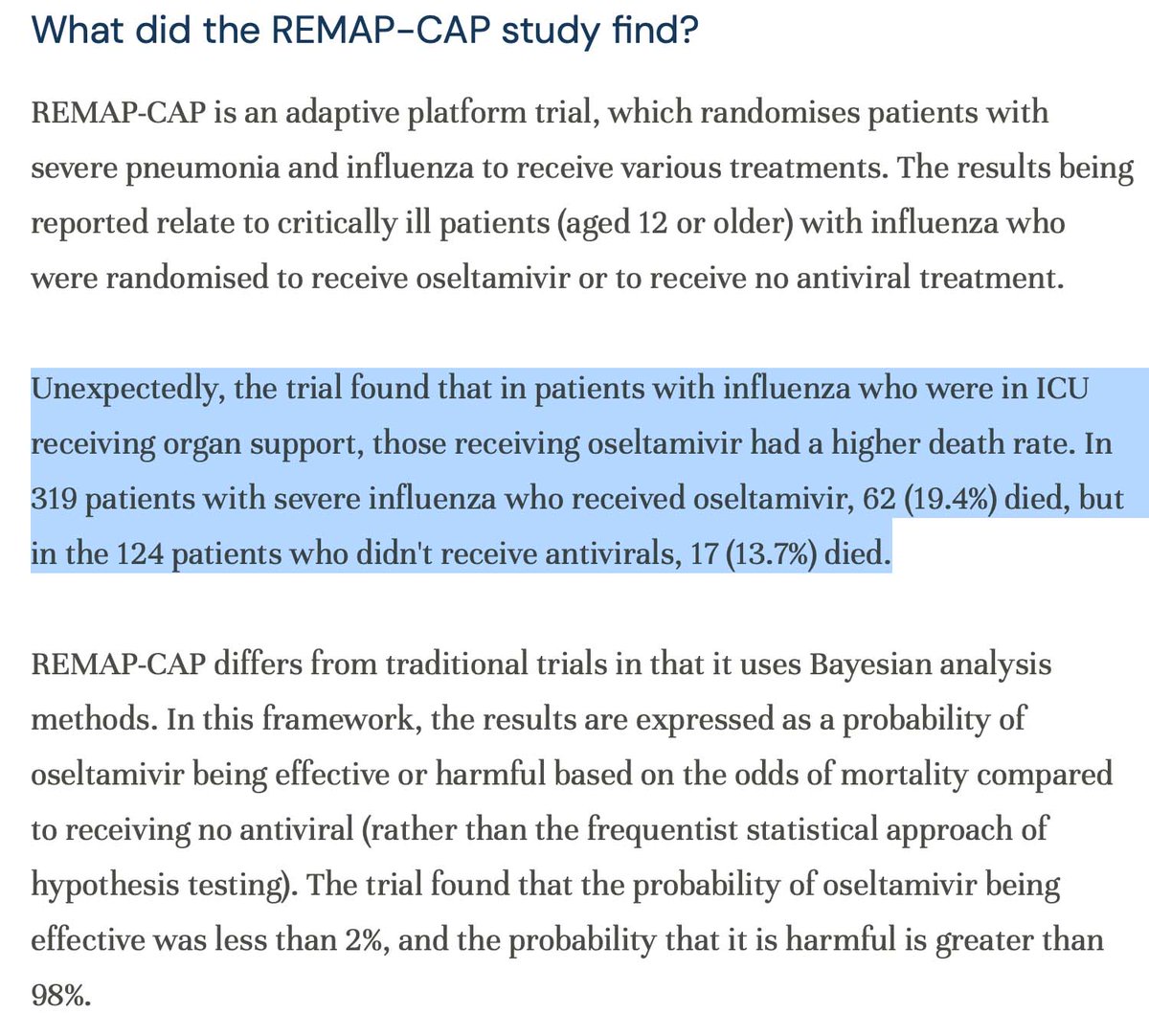
I want to talk about REMAP-CAP and the Oseltamivir data. I disagree with stopping of the trial [on the data that I have], and I think the reporting of this should have been accompanied with a preprint or more information. First, this is clearly an unexpected result
4
5
25
9,290
Jun 11
Facts, now proven in a MC-RCT.
Jun 11

30 mL/kg has never been supported by evidence and physiologically it is nonsensical to think a weight-based prescription would be beneficial. Assess the hemodynamics in front of you and treat accordingly
4
7
48
7,134
Jun 11
ARISE-FLUIDS has arrived and it's awesome 🥳
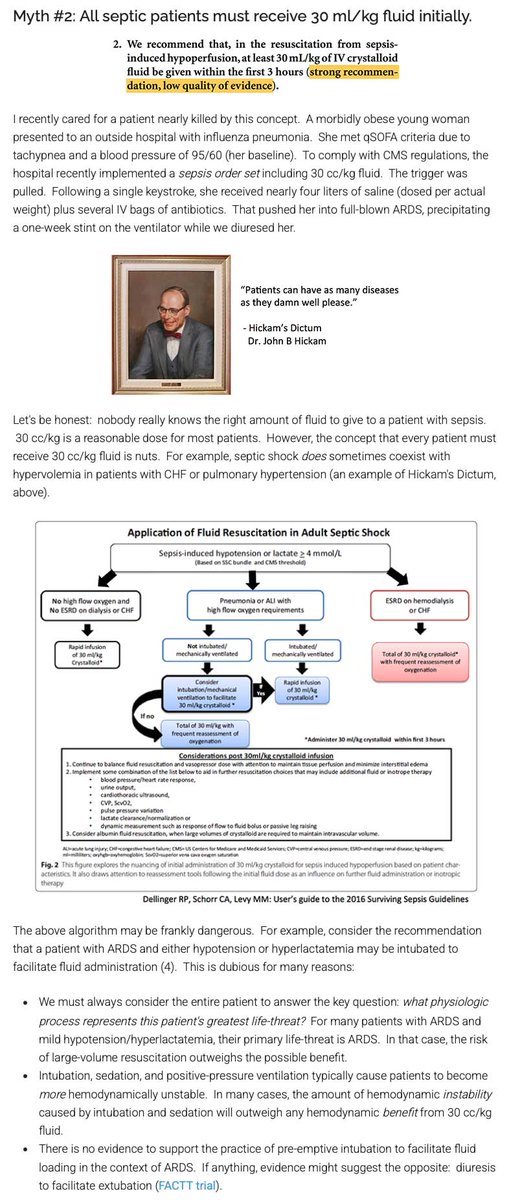
For over a decade, the Surviving Sepsis Guidelines recommended that septic patients get at least 30 cc/kg fluid. In the United States, these guidelines were weaponized into performance metrics, pressuring clinicians to prescribe arbitrary volumes to every patient.
Evidence-based clinicians have LONG known that this guideline lacked evidentiary support. For example, I've attached a picture of a blog I wrote about this back in 2017. Despite the lack of evidentiary support and some evidence of harm, the Surviving Sepsis Guidelines INSISTED on perpetually recommending 30 cc/kg fluid resuscitation.
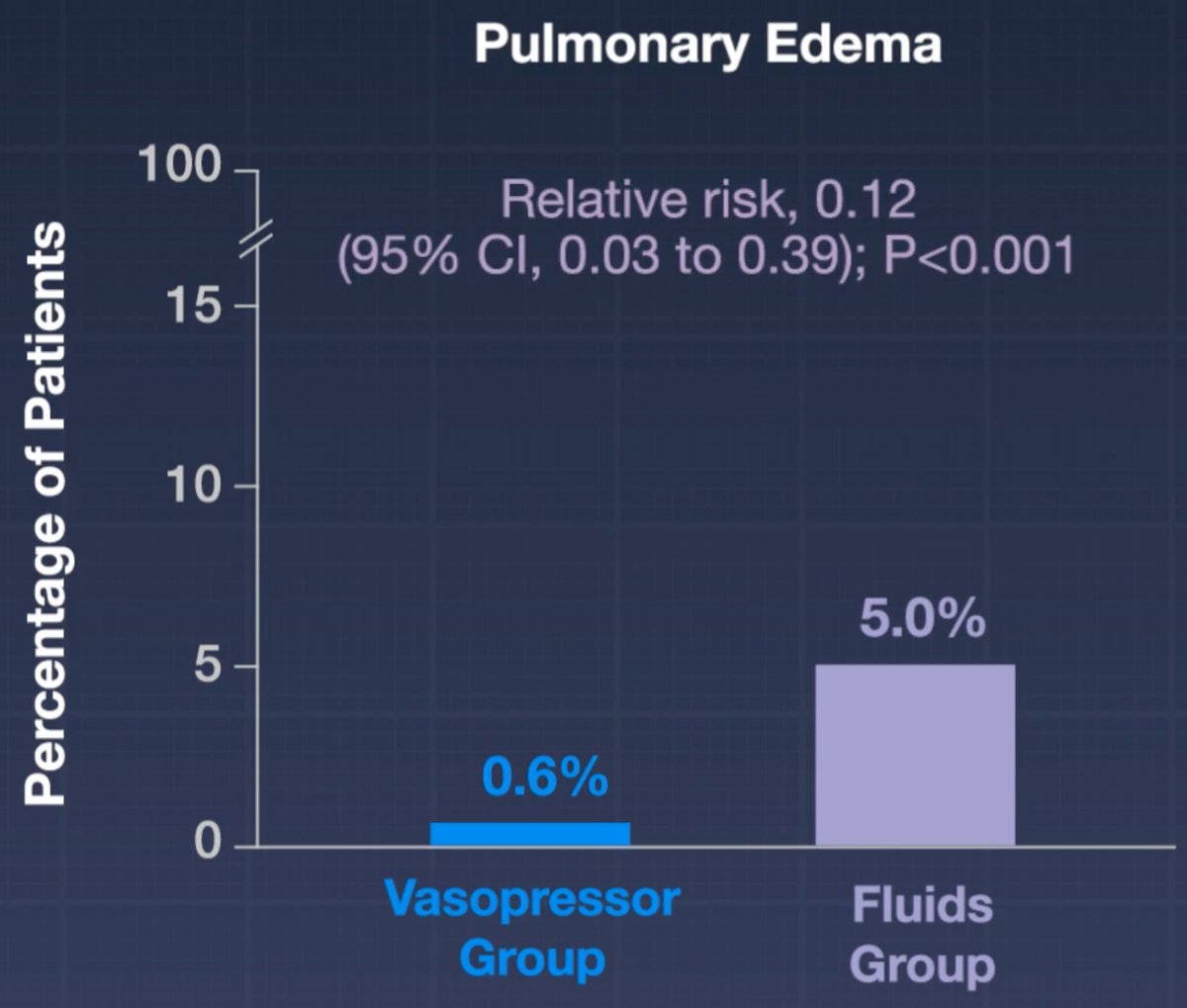
We finally have a prospective RCT demonstrating that mandating early administration of 30 cc/kg fluid (as compared to early vasopressors) doesn't help and may actually cause harm.
It's important to note that all of the hard endpoints in this trial were neutral (e.g., mortality, days free of organ support).
I still think that 30 cc/kg fluid is a pretty reasonable volume of fluid for *most* patients. But the study does suggest that giving too much fluid may promote edema - so we should be *thoughtful* about this intervention rather than mandating it for every septic patient.
Based on the subgroup analysis, the fluid-conservative strategy may have helped the subgroup of pneumonia patients the most. This is statistically nonsignificant but aligns with my expectation. ARDSy patients often don't respond well to fluid. (In contrast, I really doubt that a liter of fluids in either direction matters for most urosepsis patients.)
This is a great example of the over-reach of guidelines and protocoled medicine. People get all upset about practice variation, so sometimes they try to stomp it out using guidelines and protocols. But these guidelines are highly fallible, so what may occur is that you standardize care in a way that harms everyone equally. 🤦♂️

17
144
457
57,992
Jun 11
REMAP-CAP Oseltamavir arm:
Let me preface this by saying that I've never been a big oseltamivir fan (seriously, who is?).
I'd love to see oseltamivir proven ineffective so I'd never need to argue about it ever again.
But I don't think the math here works.
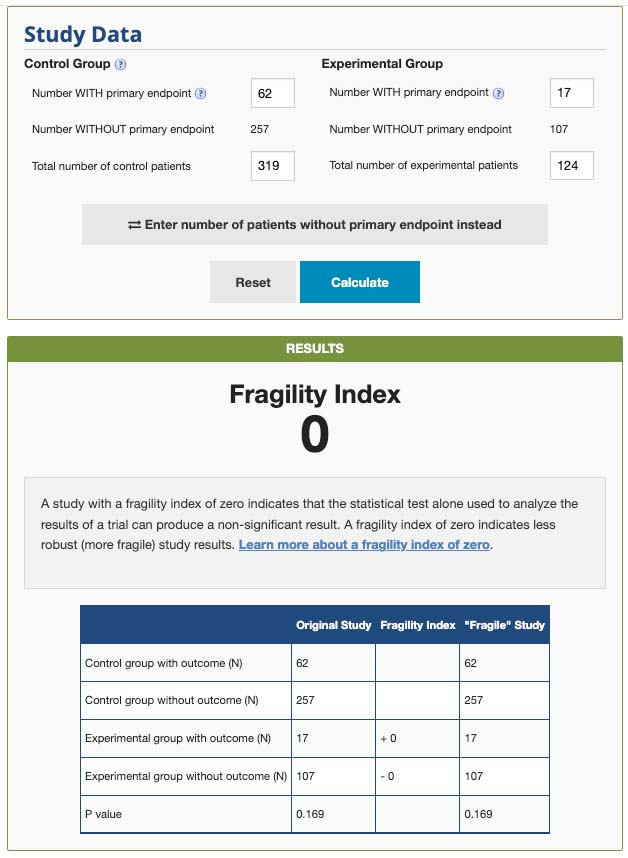
Applying a Fisher's exact score to the mortality difference yields a p-value of 0.17 which is nowhere *close* to statistically significant (by any standard).
I'm increasingly tired of seeing these studies where the p-value is ginormous but the study claims to be a slam-dunk (98% risk of harm!).
Stopping a trial prematurely for harm with a p-value of 0.17 will ultimately lead to a lot of confusion about what this study means (spoiler alert: probably not much).
Hopefully the manuscript will clarify this, but the math doesn't seem to be mathing. If you're going to claim 98% certainty of a result, then the results should be consistent regardless of how you run the statistics.
Just to be clear, I despise oseltamivir, but I'm worried that we're going down a slippery slope when a Bayesian wonderland somehow converts p=0.17 into 98% certainty.
5
11
71
12,316
Jun 10
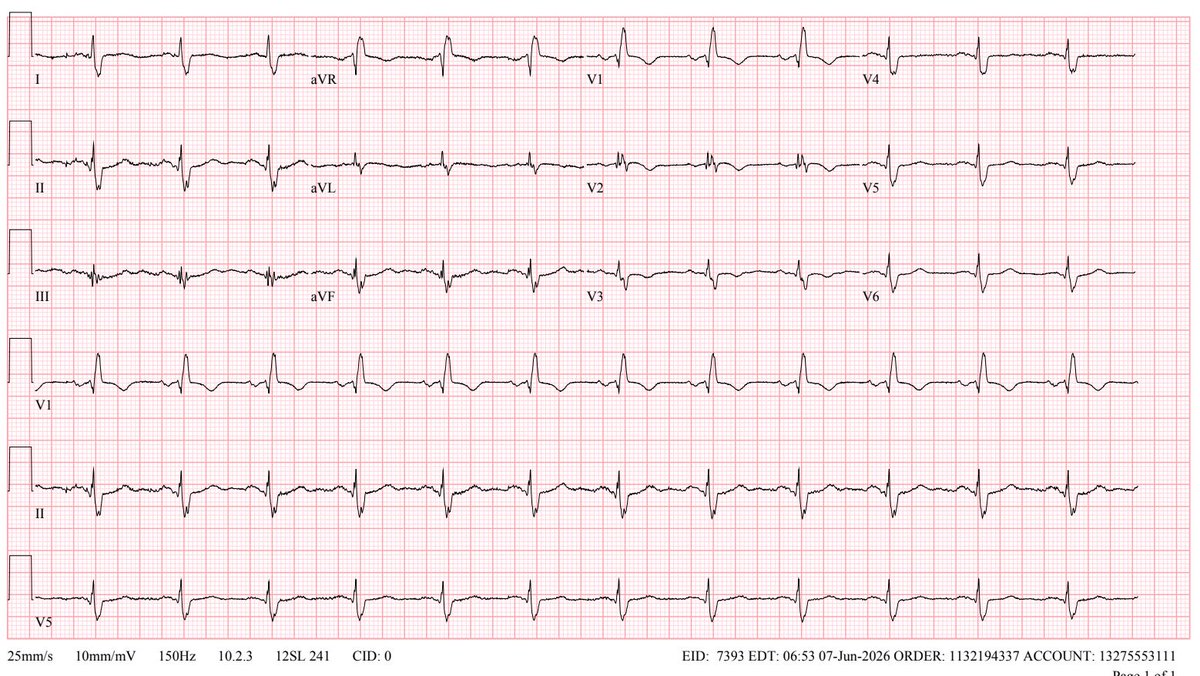
I love POCUS and ECG. For interest, lets take a look at this case from more of an ECG perspective (with extra analysis of these ECGs by the Queen of Hearts @PMcardioApp):
1st ECG:
1⃣ NSR with RBBB
1⃣To my eye this is nonspecific (could be PE, CTEPH, or ischemia).
1⃣ The queen doesn't see ischemia either. But she does flag this as reduced LVEF (<40%) which is unexpected and should be a red flag that something weird is happening.
2nd ECG:
2⃣ RBBB has resolved and now we can discern ischemic STE with TWI in V1-V4. Resolving chest pain and emerging TWI suggest that he may have experienced a transient occlusion overnight with re-perfusion.
2⃣ Could the right precordial TWI be due to PE? It's possible but less likely. Absence of TWI in the inferior leads argues against PE. Significant STE with mild TWI seems more consistent with MI than PE.
2⃣ The queen flags this as a high-risk NSTEMI with 88% probability and continues to flag a reduced LVEF.
2⃣ At this point it's increasingly clear that we're dealing with LAD-territory ischemia. Transient LAD ischemia explains the transient RBBB seen on the 1st ECG (septal perforators from the LAD perfuse the right bundle). The queen keeps on telling us the EF is low. Cardiac cath needed.
In retrospect, I think the RBBB pattern may have camouflaged a subtle Wellens pattern in the first ECG.
Overall, the ECG and echo data play out in parallel.
Jun 10

Reason number 78958 why #pocus is so important: sometimes a patient has multiple acute diseases at the same time.
A middle-aged man presented with acute chest pain that woke him from his sleep. He had a recent DVT diagnosed 2 weeks prior and had been on Eliquis without missing any doses.
His vitals were normal, and his initial ECG is shown below. His high-sensitivity troponin was mildly elevated, and his BNP was normal.
@im_crit_ @NephroP @RJonesSonoEM
2
9
46
8,089
Jun 9
Do PPIs cause COPD exacerbations? Meh. I doubt it.
PPIs are perpetually being *correlated* with poor outcomes, because they tend to be taken by multimorbid patients.
But PPIs are rarely proven to *cause* adverse events.
Over the years there have been a TON of these associative studies that got LOTS of interest, but subsequently aren't shown to be true (e.g., PPIs have been implicated in causing dementia, renal failure, hip fracture, MI, pneumonia, etc.).
Getting back to PPIs and COPD:
A meta-analysis of prospective RCT data suggests that PPIs might even *reduce* COPD exacerbations (Yu et al PMID 35252272). Although very limited, this is the only prospective RCT data we have.
I don't think a retrospective study correlating PPIs with COPD exacerbations should affect clinical management (especially given the history of such studies rarely sustaining the test of time).
Of course, if the patient doesn't have a good indication for PPIs, then PPIs should be stopped! Indeed, unnecessary PPIs serve an index of thoughtless medical care (yet another source of confounding!).

Are PPIs Linked to COPD Flares?
@NEJMClinician Editor-in-Chief Raja-Elie Abdulnour, MD (@BageLeMage), explains a retrospective study investigating if proton pump inhibitor (PPI) use is associated with exacerbations of chronic obstructive airway diseases. Read the full summary by Molly S. Brett, MD: jwat.ch/4dXVvRp
Visit clinician.nejm.org for more Insights to Break Your Routine, including:
💊 Early Transition to Oral Antibiotics after Hospitalization for Serious Infection
🩸 Breaking the Unfractionated Heparin Habit in Acute VTE
🫘 Ablation for Small Localized Renal Cell Carcinomas
📈 How Helpful Are Continuous Glucose Monitors for Type 2 Diabetes?
6
8
46
10,381
Josh Farkas MD 💊 retweeted

Jun 8
broomedocs.com/2026/06/rant-…
Lactate - evolution is smarter than us?
#FOAMed
2
6
1,378
Josh Farkas MD 💊 retweeted

Sepsis AKI bradycardia home beta blocker or CCB = BRASH syndrome.
Anand Swaminathan, MD (@emswami) from ResusX:ReUnion:
This isn't an OD — their kidneys just stopped clearing the drug. Standard pressors won't work. What's your next move at the bedside? Comment below.👇
8
34
6,406
Josh Farkas MD 💊 retweeted

Jun 7
True x 1000. This is the disconnect b/w GDMT evangelists and every day HF care. Never forget: trials enroll the best pts. Table 1 tells an important story
Jun 7

I ran a heart failure clinic years ago with the goal of maximizing GDMT therapy for systolic HF patients. Most patients sent to the clinic were over 80 with frailty and high fall risk. It was hard for them to even ambulate into clinic in some cases. Increasing GDMT meds lowered their blood pressure and made some dizzy. There were a few falls after meds were increased. I wondered if we were doing some of the patients any good. This showed me the problem with clinical care aimed at a treatment outcome measure (GDMT) rather the patient’s overall health.
10
6
102
39,242
Jun 7
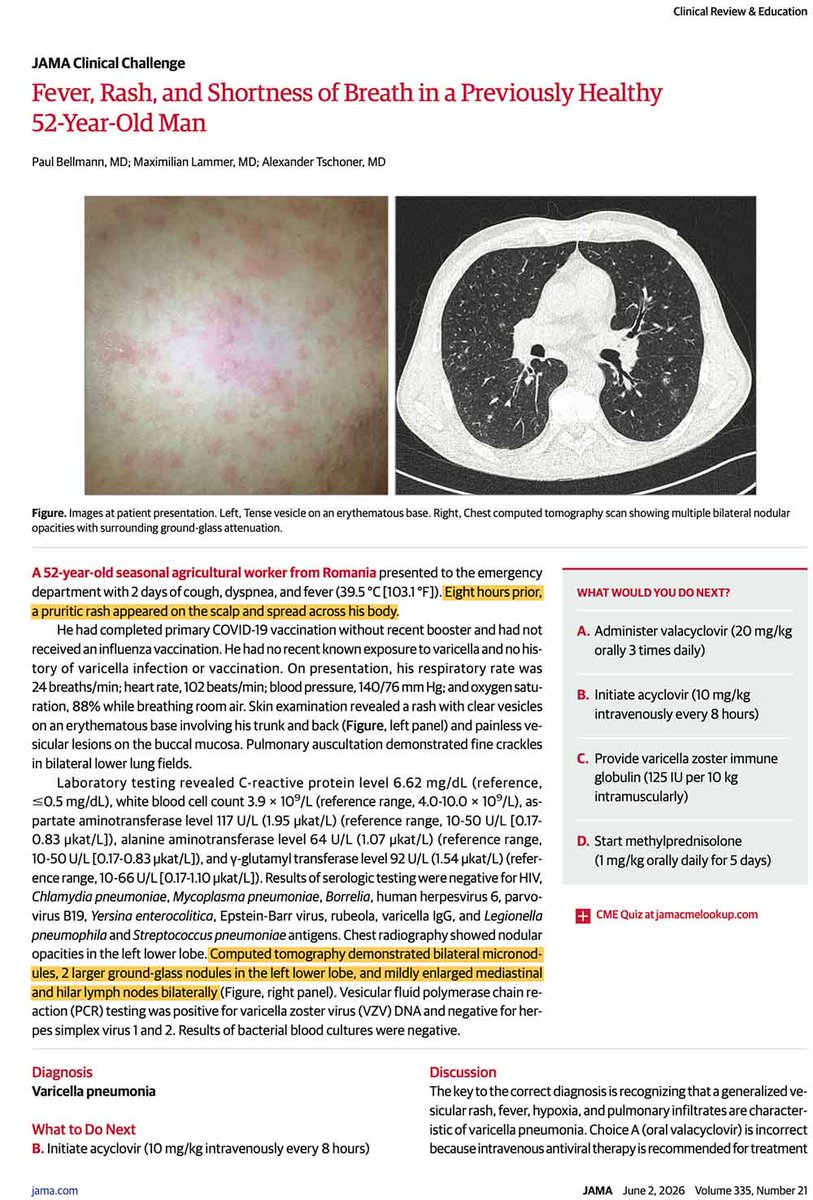
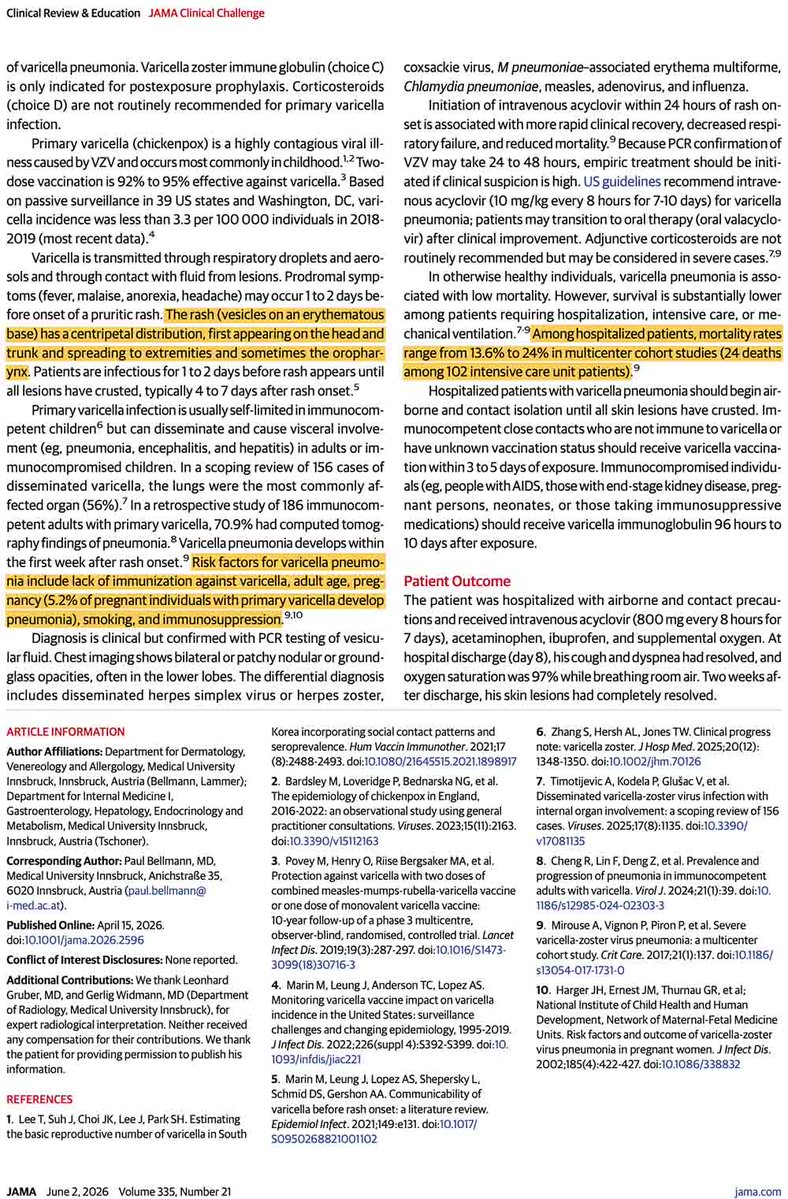
VZV pneumonia 😳
Epidemiology:
🧑🤝🧑 Usually occurs as a primary infection in someone not previously exposed or vaccinated.
🧑🤝🧑 Tends to be more severe in pregnancy, older age, or immunocompromised states.
Key clues:
🔍 "Chicken pox" rash: Usually starts on the trunk and spreads to the face and extremities.
🔍 CT shows a random distribution (miliary pattern) of nodules ~1-10 mm in size. Nodules are often ill-defined, or surrounded by ground-glass halos.
Diagnosis:
🧬Send skin fluid from vesicles for PCR.
🧬Honestly I'd probably consult dermatology because rashes are hard for intensivists (inadequate exposure).
Treatment: IV acyclovir (start empirically if high index of suspicion; PCR may take 48 hrs to turn around).
Prognosis: Mortality in ~15% of hospitalized patients.
1
15
61
4,709
Jun 6
looks like the ADA called the cops on one of their *own* members handing out journal articles ?!!?
I didn't think the ADA could disappoint me any further after bungling the distinction between AGMA and NAGMA in their DKA guidelines.
But here we are.

Far worse: seems the ADA called the police - on their own journal EiC and other well respected academics
See NYT coverage; nytimes.com/2026/06/05/well/…
#ADA2026
3
9
54
12,584
Jun 6
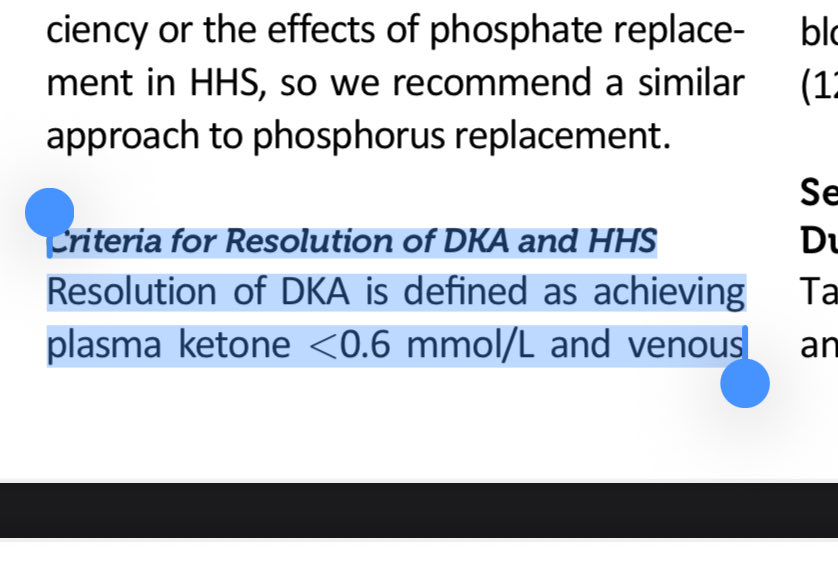
PS - the issue about NAGMA vs AGMA in the DKA guidelines is discussed here:
x.com/EMNerd_/status/2036570…
Mar 24
Okay got in a discussion with Endo at work about the management of DKA on following the AG vs the serum Bicarb to assess for resolution. They cited the following guideline which recommends using the serum bicarb because the AG can be affected by the hyperchloremic acidosis.
2
2
14
4,613
Jun 5
SOHO trial in NEJM:
🏙️ Multicenter RCT comparing high-flow nasal cannula vs. low-flow oxygen among patients with acute hypoxemic respiratory failure (mostly pneumonia)
🏙️ Inclusion criteria required a respiratory rate >25 and substantial hypoxemia (P/F <200)
🏙️ No difference in the primary endpoint of mortality (not surprising, the mortality endpoint is nearly always neutral in modern RCTs evaluating the nuances of supportive care).
🏙️ HFNC reduced the rate of intubation and increased the number of ventilator-free days.
🏙️ No significant signals of harm from HFNC.
This is similar to the FLORALI trial (by the same group of investigators). However, FLORALI showed *improvement* in mortality, whereas the current study didn't.
Why do these studies disagree about mortality?
The FLORALI trial found no mortality difference between HFNC versus conventional oxygen among ALL PATIENTS. However, it DID find a mortality difference in the *subgroup* of patients with P/F <200.
So this is a classic tale in critical care - a subgroup analysis from one trial subsequently fails to replicate. (At least, in terms of the mortality benefit.)
But chasing mortality in these trials is a fool's errand. Overall, the SOHO trial still supports the use of HFNC in acute hypoxemic respiratory failure (in terms of reduced intubation and improved ventilator-free days).
Using HFNC for sick pneumonia patients is already standard care, so I don't see this changing practice very much. Keep calm and HFNC on. 🌬️
For patients with acute hypoxemic respiratory failure, whether high-flow oxygen is superior to standard oxygen in reducing mortality is unclear. Research findings from the SOHO trial are summarized in a new Quick Take video. nej.md/4x706JY
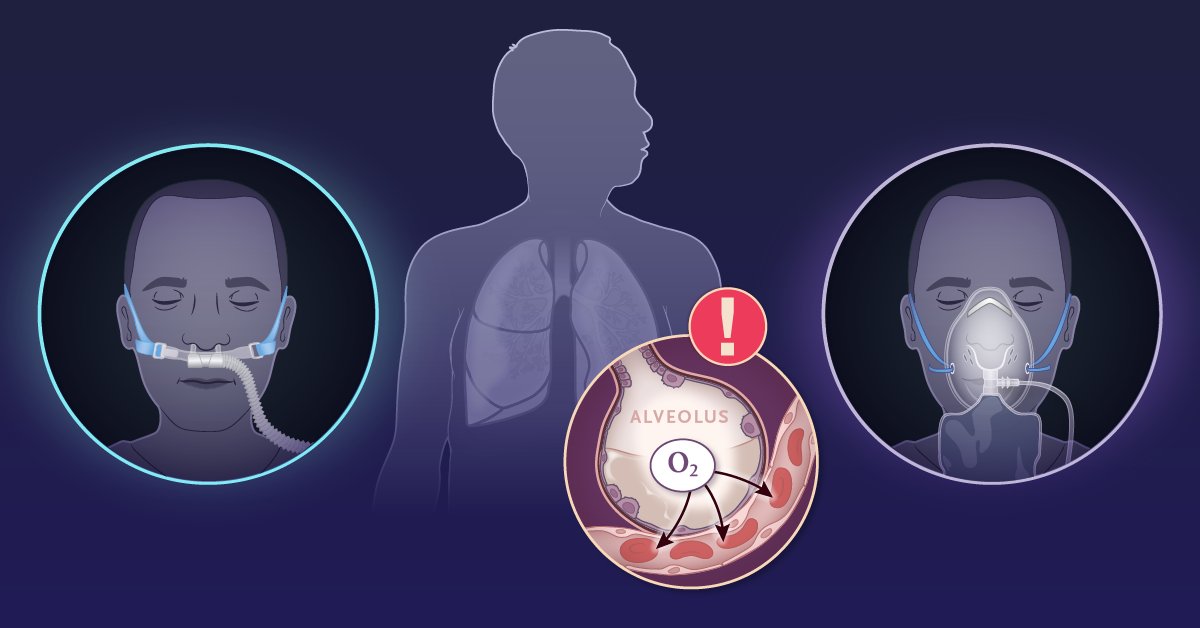
ALT An illustration showing a patient receiving oxygen through nasal cannula on the left and standard oxygen on the right. In the center, there is a diagram highlighting acute hypoxemic respiratory failure with an oxygen (O2) symbol and an exclamation mark, positioned against a silhouette of lungs.
4
38
148
33,737
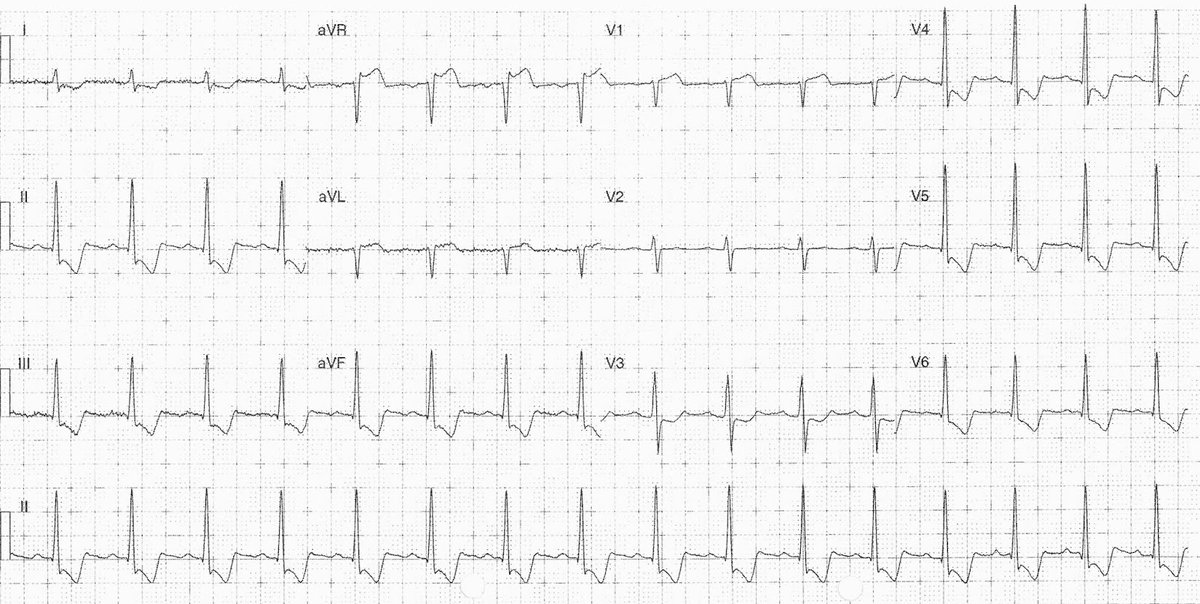
Jun 5
diffuse subendocardial ischemia from GI bleed
make sure to call GI & provide volume/blood resuscitation immediately
avoid calling cardiology up-front (this may scare away GI)
key: repeat ECG should normalize after resus
troponin may go uncomfortably high

A 70 y/o male with palpitations, fatigue, dizziness, epigastric, chest pain, and melena for one week.
Past medical history: ischaemic heart disease requiring stents 10 years ago.
His hemoglobin was 72 g/L.
- What’s your interpretation ?
#medtwitter #foamed #ecg #cardioed
4
43
6,604
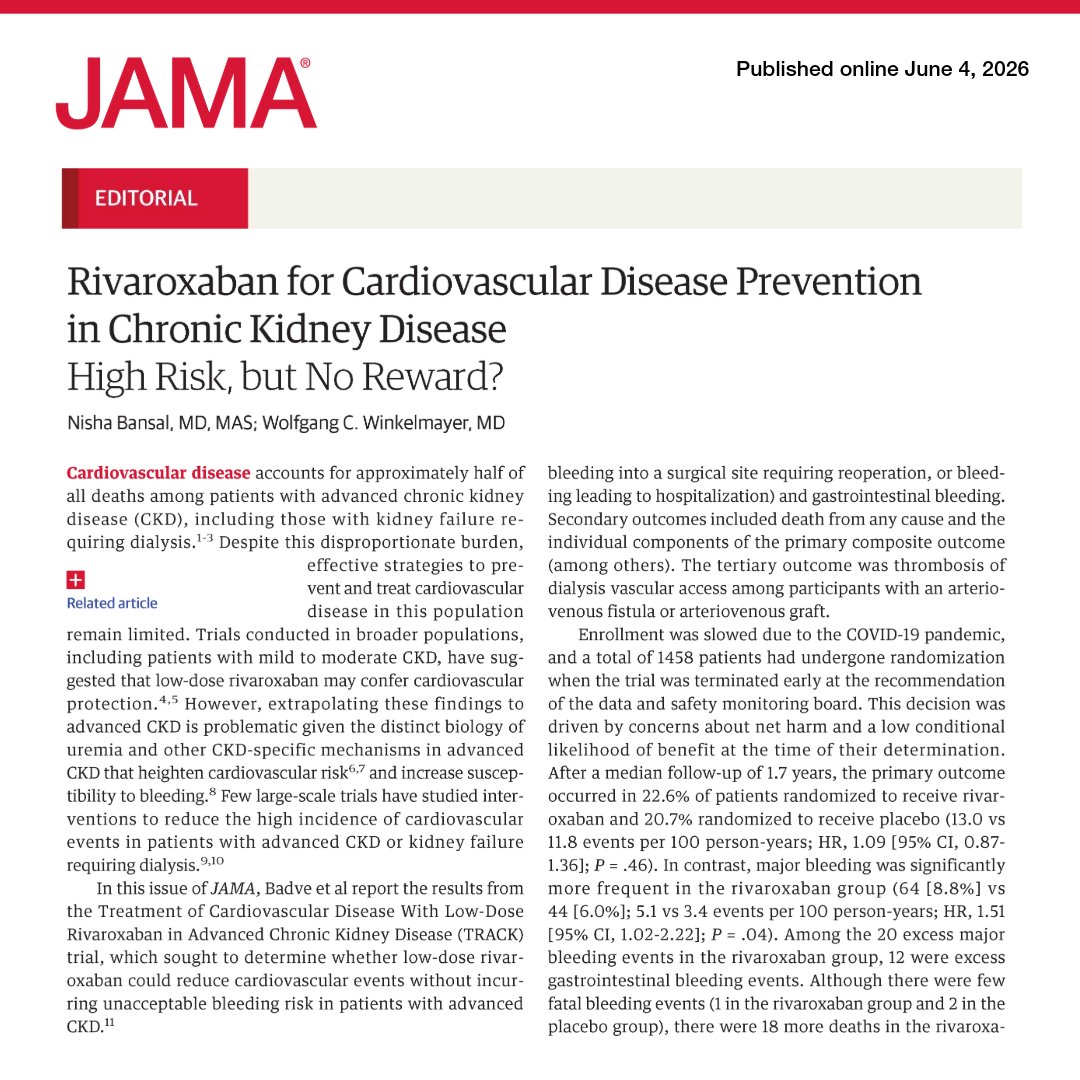
Jun 4
apixaban would have been pharmacokinetically superior in renal failure
it's curious how this editorial very subtly implies this, while skirting gingerly around the issue
it avoids using the word "apixaban"
these editorials often seem biased in favor of the trial & sponsor
Jun 4

💬 Editorial: In advanced #CKD, low-dose rivaroxaban did not reduce cardiovascular events and increased major bleeding risk. The TRACK trial highlights the necessity of disease-specific evidence before adopting preventative therapies.
#ERA26 @ERAkidney
ja.ma/4dOR4d6
2
3
35
11,012