
Emergency physician | Epidemiology PhD | Medical Flashnotes app creator
Joined June 2019
- Tweets 196
- Following 164
- Followers 212
- Likes 995
15 Photos and videos






Jun 12
ARISE FLUIDS: no difference of early pressors vs fluids in sepsis. When a trial finds no diff between 2 therapies, we commonly interpret them as 'equally effective'. We fail to sufficiently consider the equally valid interpretations: 'equally futile' or 'equally harmful' 1/5
1
12
44
7,662
Jun 12
Relatedly, a meta-analysis of RCTs of high vs lower MAP in distributive shock finds higher MAP targets increase mortality 4/5 link.springer.com/article/10…
1
9
880
Jun 12
75% of patients in ARISE FLUIDS had initial SBP >80. Maybe they didn't need fluids or pressors. Maybe mild hypotension isn't that harmful. Maybe some degree of mild 'shock' is part of an appropriate compensatory response to systemic infection that we don't yet understand. 5/5
2
2
15
796
Jun 11
RCT in ICU influenza, 443 patients: 19% mortality with oseltamivir vs 14% in control. Not significantly different with frequentist methods, but clearly futile and possibly harmful. Outrageous it's taken 30 years since drug licensed to establish this. 1/4
6
11
38
10,396
Jun 11
And of course all the big "high quality" observational studies of oseltamivir in hospitalised patients (including "target trial emulations") showed significant mortality reductions with the drug pubmed.ncbi.nlm.nih.gov/2481…, jamanetwork.com/journals/jam… 3/4
1
3
10
3,479
Jun 11
Reminding us once again that unless you can randomize or find plausibly unconfounded sources of treatment variation, your observational clinical epidemiology study should probably not be ethically approved, funded, or published. 4/4
1
4
20
2,294
May 22
TOWAR RCT replicates SWIFT finding no benefit of whole blood vs components for trauma shock. Quick meta-analysis of 30d mortality gives RR 1.17 (0.98-1.40), close to showing *harm* by whole blood. Huge credit to those who ran these RCTs; another physiology-based hype cycle falls
1
3
5
1,072
May 22
1
90
May 22
2 recent meta-analyses of mostly observational studies (one published this month!) found a significant *reduction* in mortality with whole blood vs. components pubmed.ncbi.nlm.nih.gov/4181… pubmed.ncbi.nlm.nih.gov/4102…, proving yet again the futility of most observational clinical epi
1
71
19 Dec 2025
Fully agree with this. Sadly the @Royal_College residency program requirements require each resident to make their 'own' research project - mostly low quality single centre observational studies or surveys - rather than encouraging multi centre collaborative RCTs.
18 Dec 2025

Check our viewpoint published @JAMA_current #MedEd
Abstract Factory—Research Culture Harming Medical Education
The "abstract factory" is destroying medical education. Trainees and junior faculty compete with abstract counts instead of meaningful research. Result: inflated CVs, diluted conferences. We shouldn't celebrate this—you don't need publications to be a great doctor.
➡️jamanetwork.com/journals/jam…
@utswcancer @rajshekharucms @HiraSMian @ManniMD1 @HemOncFellows @ASCOTECAG

2
6
635
10 Dec 2025
Interesting to see people jumping to 'we should use etomidate' based on the RSI trial surrogate 2ry outcome of less post intubation⬇️BP. But we only care about that surrogate outcome based on years of confounded retrospective studies, which RSI study itself has disproven. 1/2
1
2
2
277
10 Dec 2025
RSI trial in shows transient post RSI ⬇️BP does *not* lead to increased mortality; the point estimate is in fact in the opposite direction. Using previous RCTs as priors, Bayesian interpretation still favours ketamine as the preferred induction agent. 2/2
1
2
158
8 Dec 2025
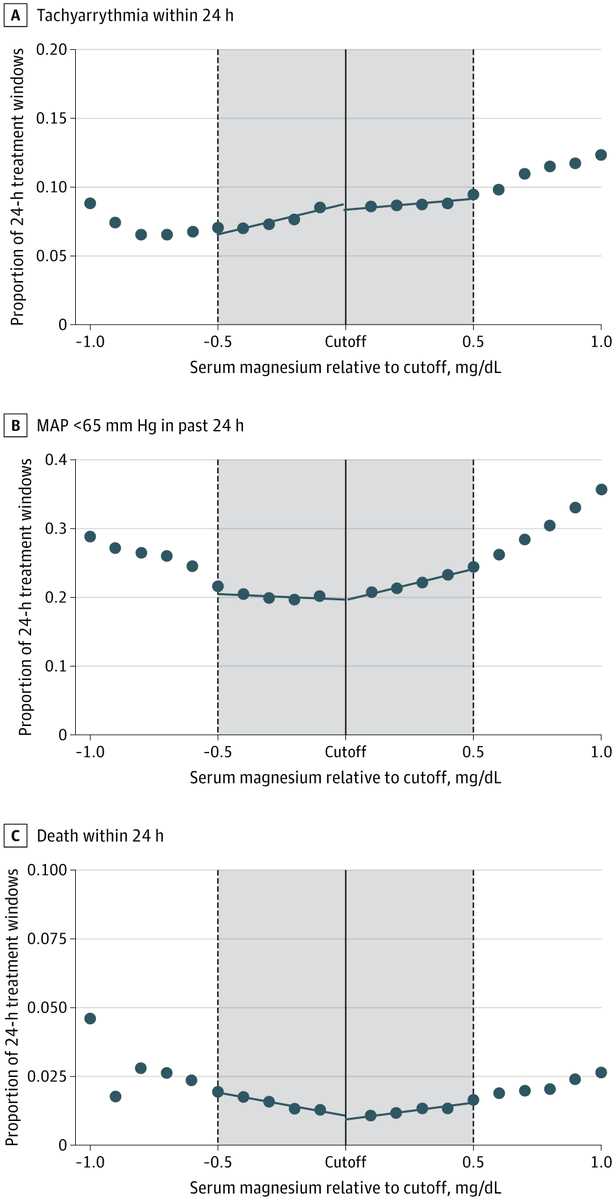
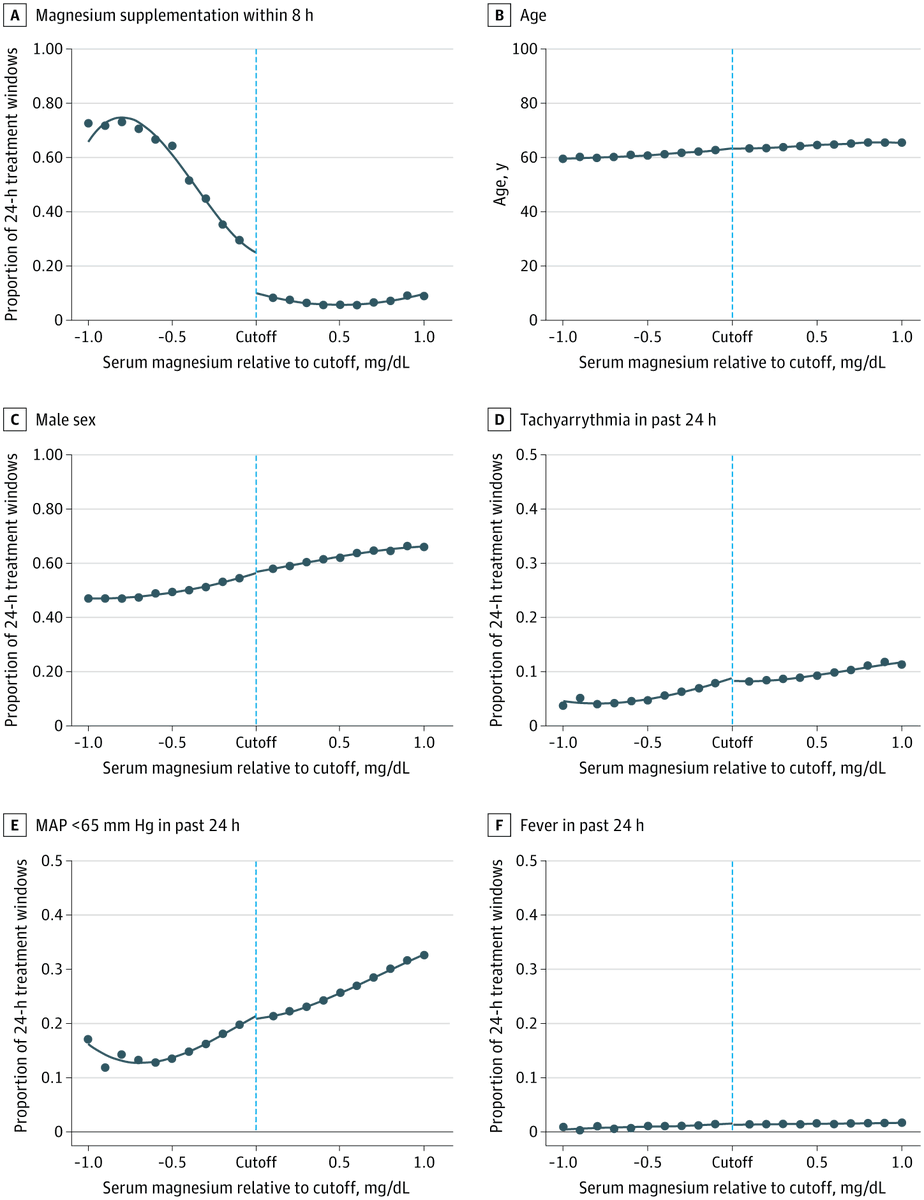
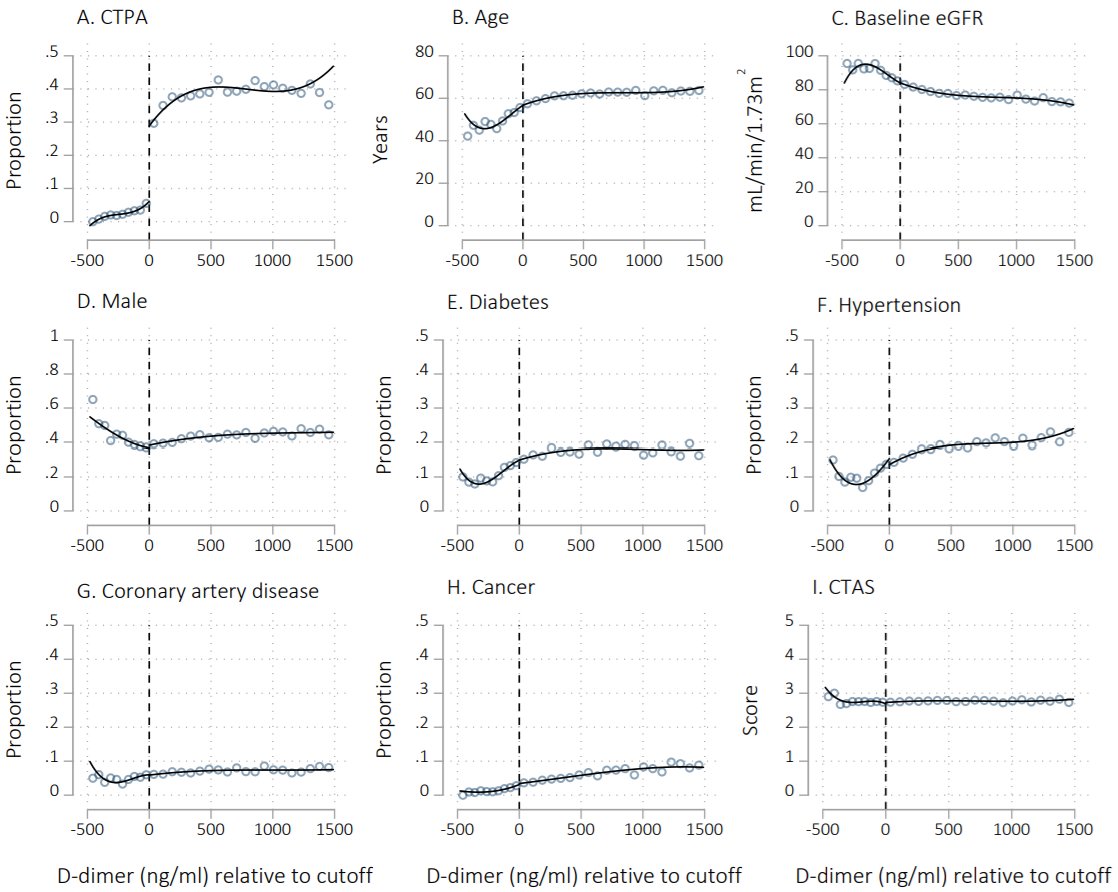
We have a new study in JAMA IM asking: do all 'hypomagnesemic' patients need supplementation? Many reflexively prescribe Mg when the number is below the reference range, but is this indicated? We used a quasi-experimental design to find out. jamanetwork.com/journals/jam…
1
103
8 Dec 2025
All this suggests that routine Mg supplementation of everyone falling below the reference range may be another example of low value care. Very low levels and high-arrythmia risk patients likely still need treatment, but not everyone who's number is red on the EMR. RCTs needed.
1
63
8 Dec 2025
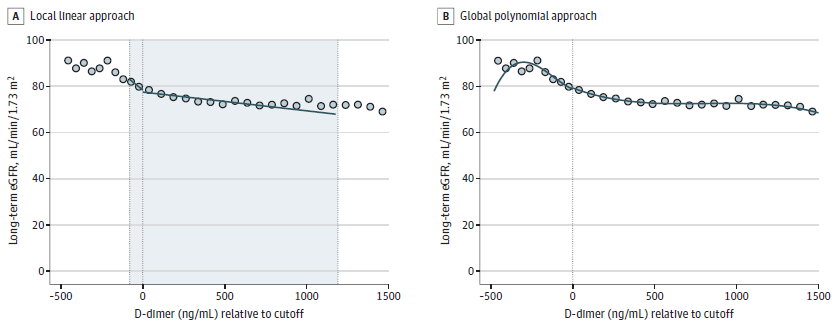
Great commentary on the paper and RDD in general jamanetwork.com/journals/jam…, and podcast discussion edhub.ama-assn.org/jn-learni…
53