
Associate Professor @utswcancer. Alumni myeloma @UAMSMyeloma, heme/onc @bcmhouston, clinical research/biostat @UMich.Focus on plasma cell disorders
Joined August 2012
- Tweets 7,418
- Following 310
- Followers 5,880
- Likes 8,250
3,405 Photos and videos





Pinned Tweet

17 May 2024
Myeloma is a curable malignancy #mmsm
Yes it is curable
The cure rate is not ideal (not all/most patients are cured)- there is still work to be done to improve
We estimate that one out of three patients with standard risk myeloma (vast majority of cases) are cured
🧵

13
34
196
51,872
Samer Al Hadidi, MD,MS,FACP retweeted

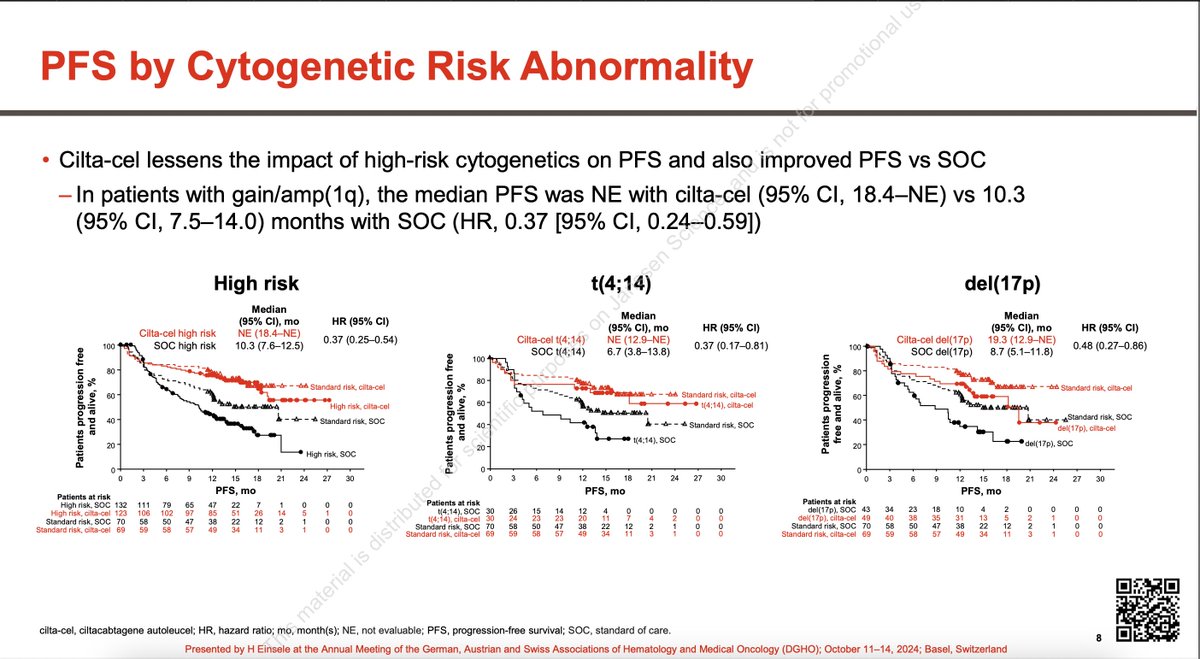
Wow! These curves in 1 and 2 HRCA are amazing! In patients who are CD38 naive or exposed (not refractory), based on these data, I would recommend Tec-Dara over Cilta-cel in both standard-risk and high-risk!
For patients who are CD38-refractory, both Cilta-cel and Tec monotherapy are reasonable.
#EHA26

#mmsm #EHA26
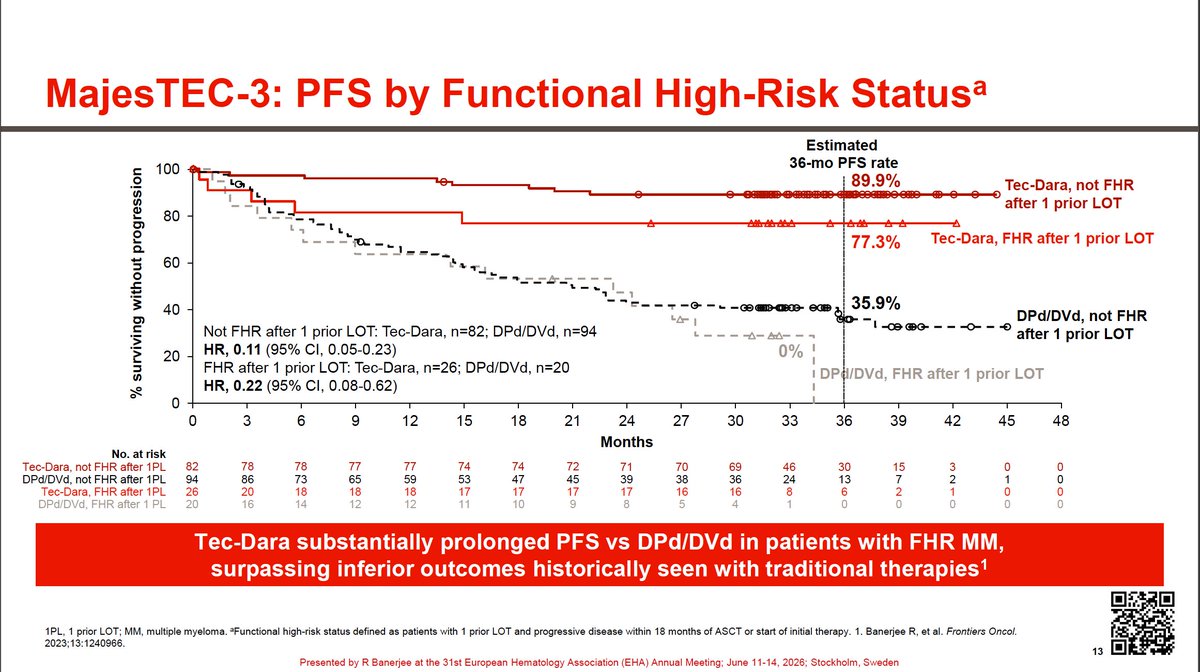
MajesTEC-3 high risk post hoc analysis @RahulBanerjeeMD
Tec-Dara worked well in patients with 2HRCA or more as well as functionally high risk
Really good results in hard to treat patients

2
4
19
1,739
Samer Al Hadidi, MD,MS,FACP retweeted

Wow 🤩
#mmsm #EHA26
MajesTEC-3 high risk post hoc analysis @RahulBanerjeeMD
Tec-Dara worked well in patients with 2HRCA or more as well as functionally high risk
Really good results in hard to treat patients
2
7
761
Samer Al Hadidi, MD,MS,FACP retweeted
I am all in favour of bispecifics in early lapse, but for me here the safety signal is concerning. A risk I might be willing to take for later relapse but have a hard time justifying it in early relapse.
#mmsm #EHA26 MonumenTAL-3
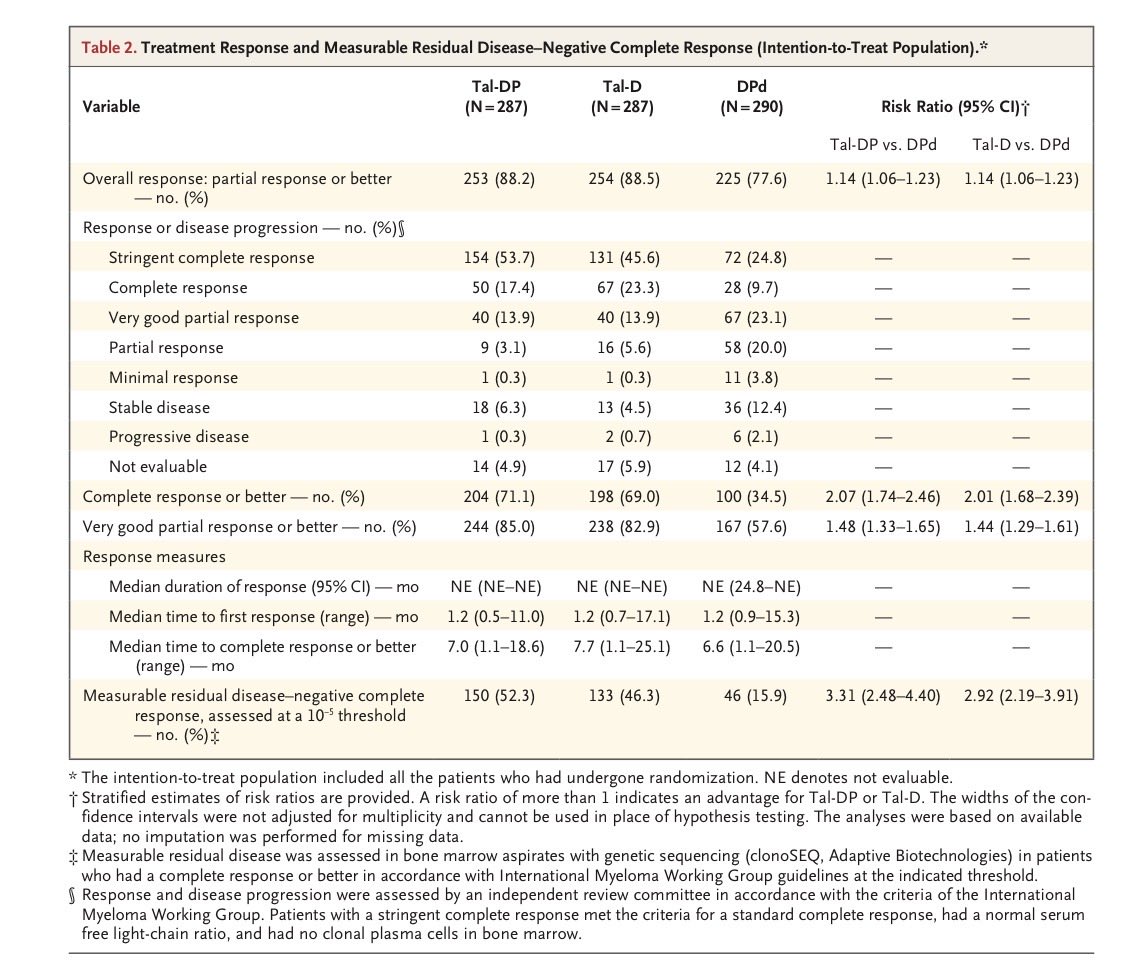
Published @NEJM
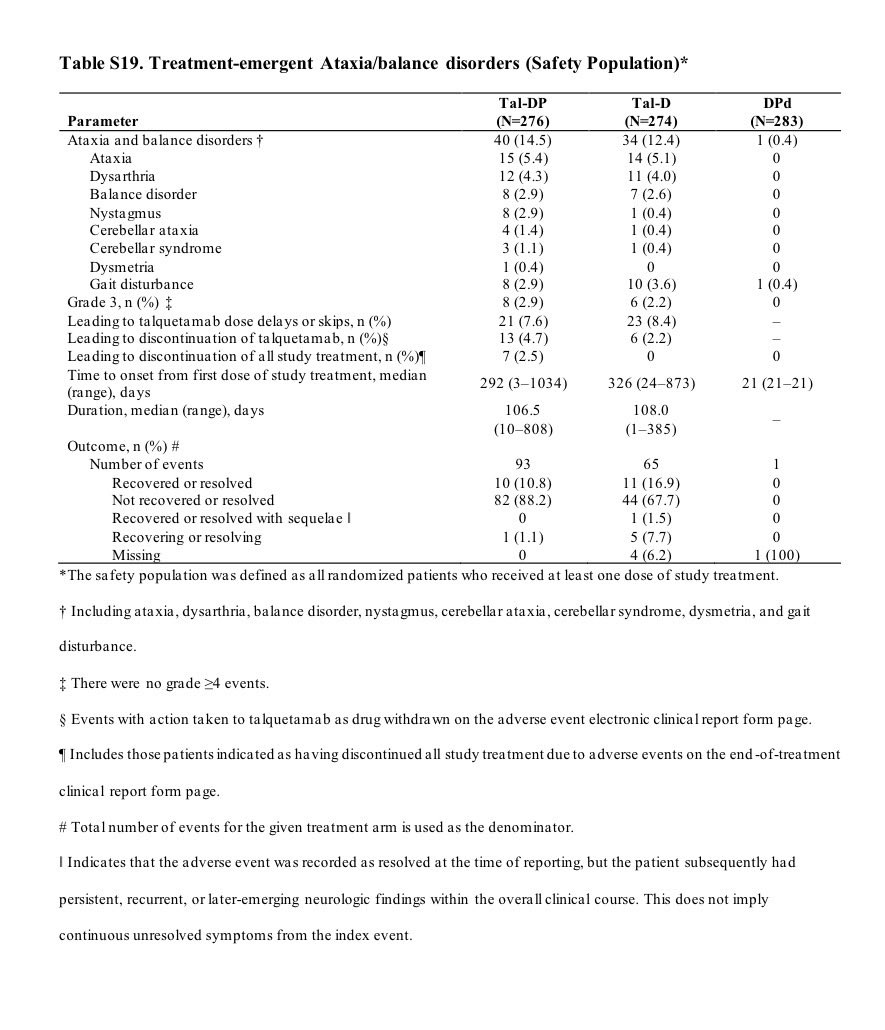
🛑Ataxia/balance disorders: Tal-DP 15%, Tal-D 12%, DPd 0.4%.
🛑Onset is late: median ~292–326 days, increasing from cycle 7 onward (11% Tal-DP, 10% Tal-D)-Led to talquetamab discontinuation: 5% (Tal-DP) vs 2% (Tal-D)
The major issue with it is that reversibility is poor: 88% Tal-DP and 68% Tal-D events not recovered/resolved at data cutoff with median duration ~107–108 days, imp table 👇
🛑 ICANS occurred in 3% (Tal-DP) vs 2% (Tal-D), all resolved
4
18
1,339
Samer Al Hadidi, MD,MS,FACP retweeted
#mmsm #EHA26 MonumenTAL-3
Published @NEJM
➡️ nejm.org/doi/full/10.1056/NE…
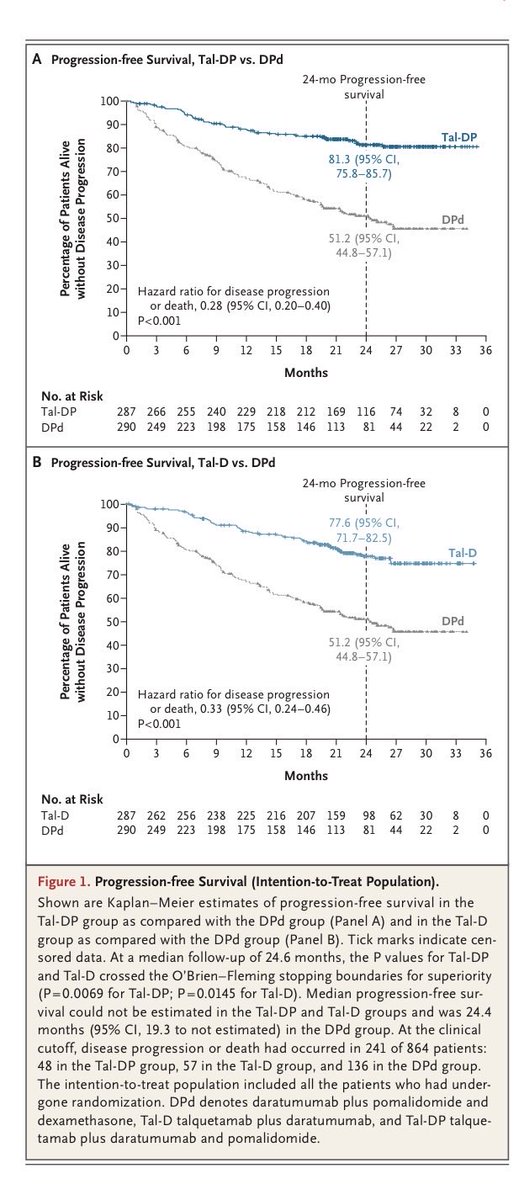
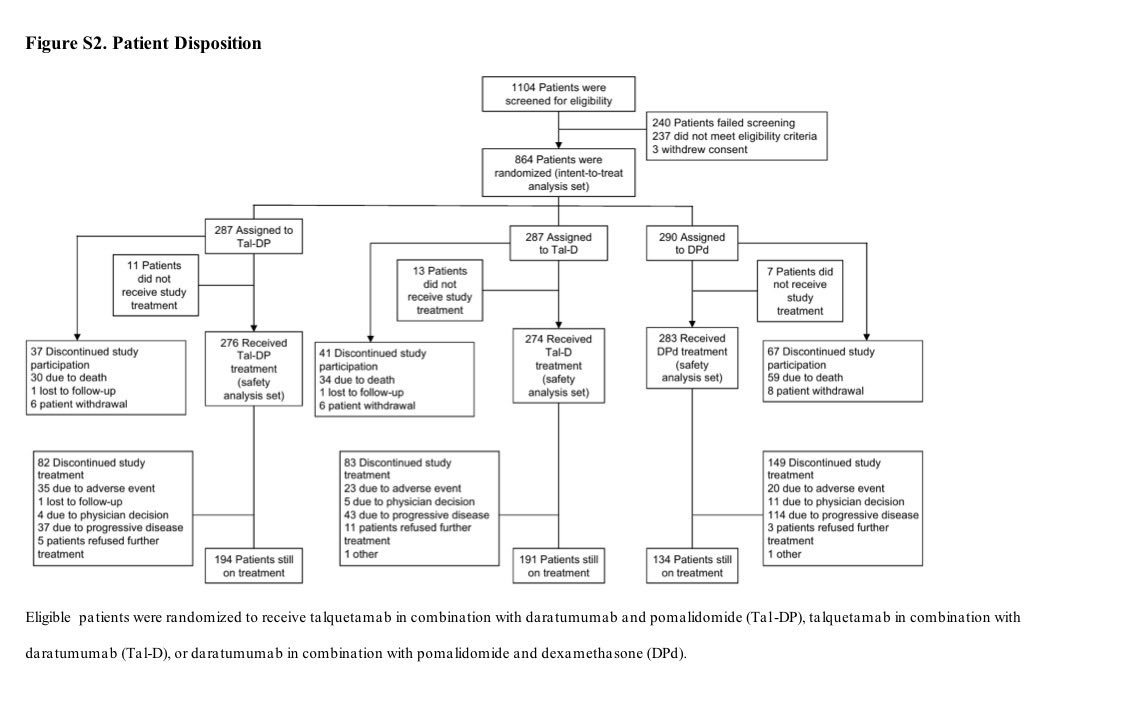
✅RCT, phase 3: Tal-DP vs Tal-D vs DPd
✅ Treatment was until progression or intolerance (not time-limited)
✅ Early relapse ≥1 prior line including lenalidomide PI ( no anti-CD38 refractory)
✅allowed for T-cell redirecting >3 months
🧵
1
11
21
1,346
Samer Al Hadidi, MD,MS,FACP retweeted

Which is why I haven’t changed approach to first relapse. With Talq I’m not even sure of second relapse. Best only after refractory to triplet and BCMA. Or as a short term therapy to reduce tumor burden prior to BCMA approaches especially BCMA CART. And in refractory BCMA sensitive EMD relapse with Tec.


2
3
17
592
#mmsm #EHA26
MajesTEC-3 high risk post hoc analysis @RahulBanerjeeMD
Tec-Dara worked well in patients with 2HRCA or more as well as functionally high risk
Really good results in hard to treat patients
3
13
28
4,109
Samer Al Hadidi, MD,MS,FACP retweeted

This is an important toxicity which we are working on in the IMWG. The real world patterns are not the same and we will present more data at ASH. Also a class effect seen with arlocel also . I will create a seperate thread on this - identification and management of this toxicity
#mmsm #EHA26 MonumenTAL-3
Published @NEJM
🛑Ataxia/balance disorders: Tal-DP 15%, Tal-D 12%, DPd 0.4%.
🛑Onset is late: median ~292–326 days, increasing from cycle 7 onward (11% Tal-DP, 10% Tal-D)-Led to talquetamab discontinuation: 5% (Tal-DP) vs 2% (Tal-D)
The major issue with it is that reversibility is poor: 88% Tal-DP and 68% Tal-D events not recovered/resolved at data cutoff with median duration ~107–108 days, imp table 👇
🛑 ICANS occurred in 3% (Tal-DP) vs 2% (Tal-D), all resolved
2
7
14
1,644
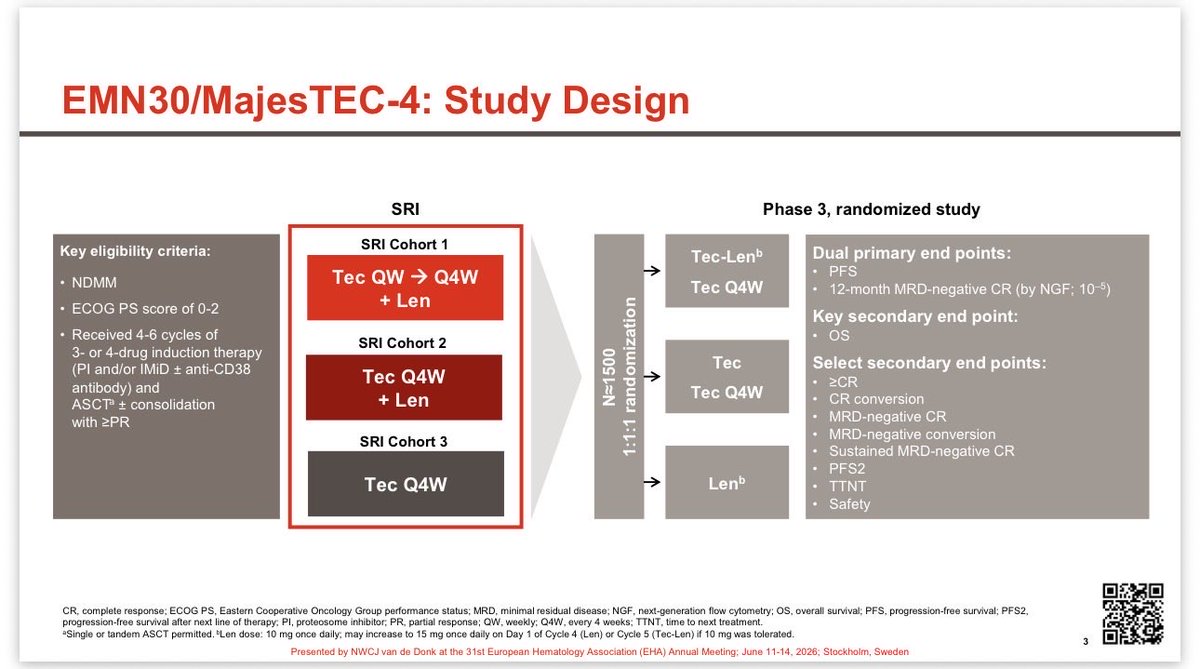
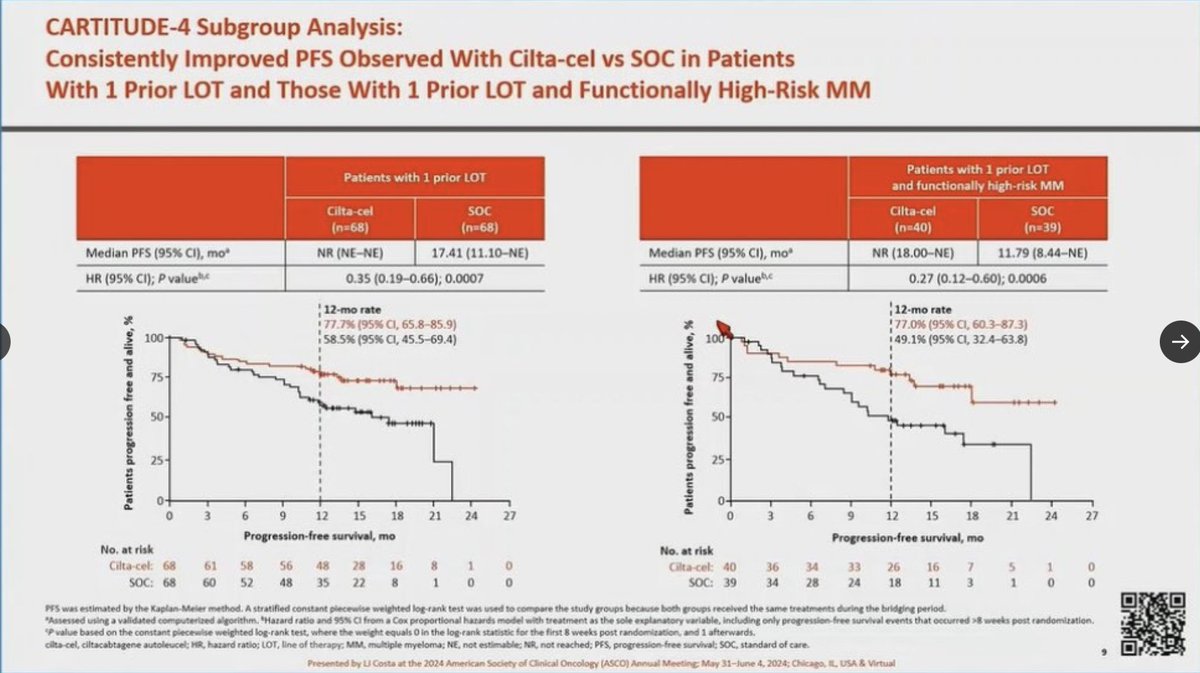
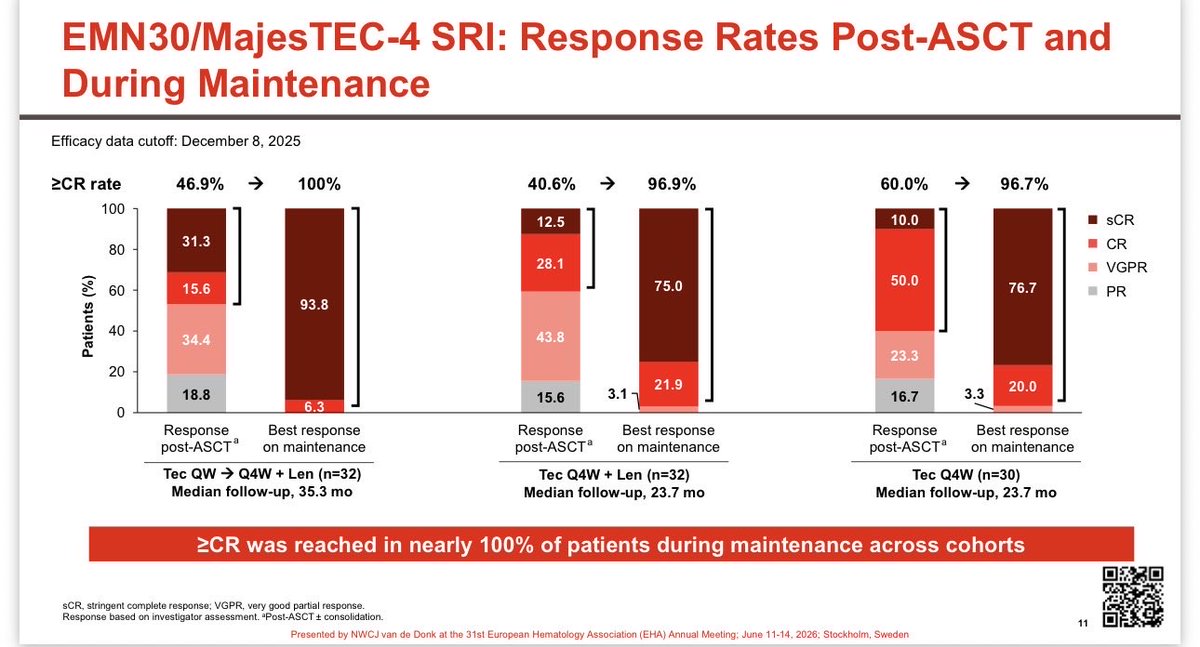
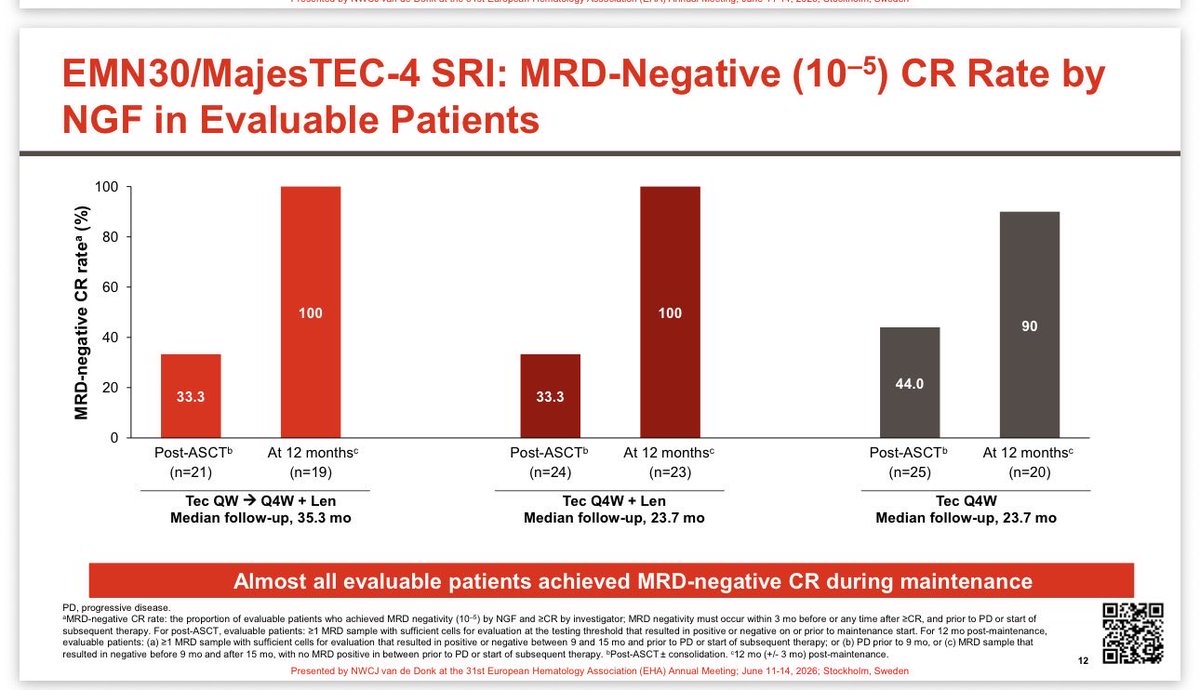
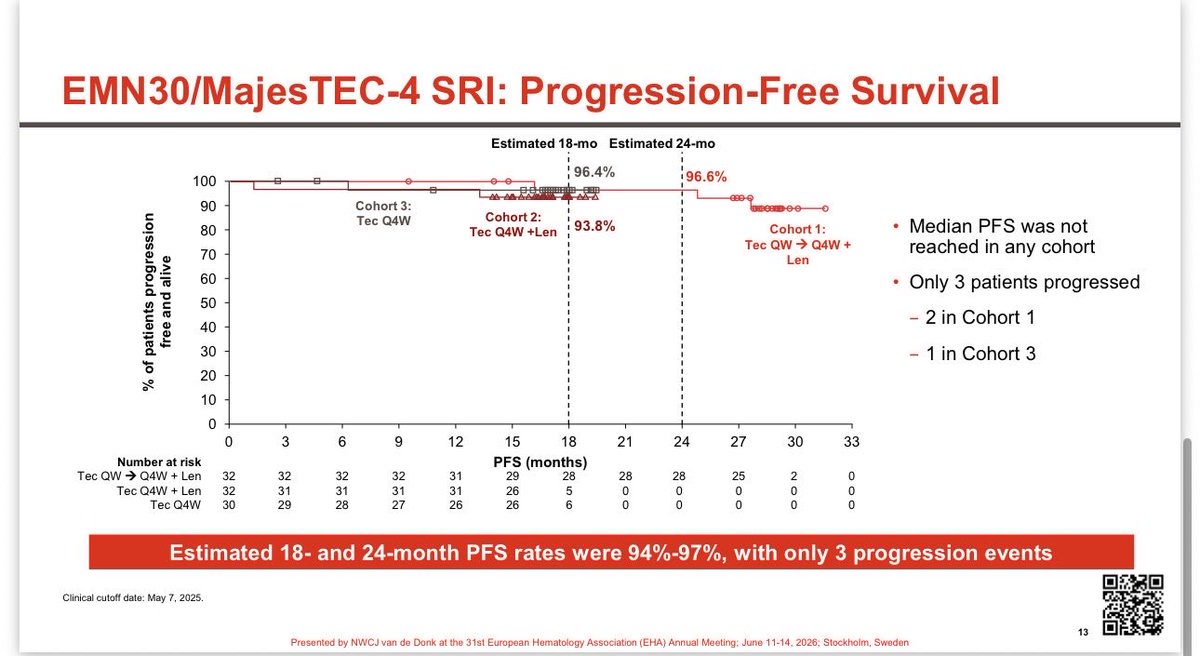
#mmsm #EHA26 MajesTEC-4
Amazing data
✅ ≥CR was achieved in nearly 100% of patients across all 3 cohorts (100%, 96.9%, and 96.7%), up from roughly 41–60% post-ASCT
✅ Median PFS was not reached in any cohort. Estimated 18- and 24-month PFS rates were 94–97%
Only 3 progression events across all 94 patients 👏
✅ Grade 3/4 infections were lowest in the Tec Q4W monotherapy cohort (27%) vs. ~35–38% in the combination arms
Beginning of an era of “no Lenalidomide maintenance and time limited BCMA maintenance
Teclistimab continues to be impressive addition to the myeloma treatments
1
8
29
1,303
#mmsm #EHA26 MonumenTAL-3
Published @NEJM
➡️ nejm.org/doi/full/10.1056/NE…
✅RCT, phase 3: Tal-DP vs Tal-D vs DPd
✅ Treatment was until progression or intolerance (not time-limited)
✅ Early relapse ≥1 prior line including lenalidomide PI ( no anti-CD38 refractory)
✅allowed for T-cell redirecting >3 months
🧵
1
11
21
1,346
#mmsm #EHA26 MonumenTAL-3
Published @NEJM
🛑Ataxia/balance disorders: Tal-DP 15%, Tal-D 12%, DPd 0.4%.
🛑Onset is late: median ~292–326 days, increasing from cycle 7 onward (11% Tal-DP, 10% Tal-D)-Led to talquetamab discontinuation: 5% (Tal-DP) vs 2% (Tal-D)
The major issue with it is that reversibility is poor: 88% Tal-DP and 68% Tal-D events not recovered/resolved at data cutoff with median duration ~107–108 days, imp table 👇
🛑 ICANS occurred in 3% (Tal-DP) vs 2% (Tal-D), all resolved
2
1
9
3,489
#mmsm #EHA26 MonumenTAL-3
Published @NEJM
Final thoughts
✅Excellent PFS benefit for non BCMA target: (HR ~0.28–0.33)
✅Pom addition not needed IMO, Talq-Dara is enough for combination. More neutropenia with Tal-DP and also more 2nd primary malignancies with Tal-DP (8%) vs Tal-D (4%) vs DPd (4%)
🛑Taste changes in ~74%, often persistent( QoL impact) weight loss ~38–46%
🛑 Cerebellar/balance toxicity in ~13–15%, delayed onset, often not reversible (should we limit the use of Talq to 1 yr given delayed onset with longer use?-MonumenTAL-6 will be helpful)
Field should move to time-limited therapy with such efficacious agents and work better to improve adverse events profile that may negatively affect QoL
End 🧵
1
5
286
Samer Al Hadidi, MD,MS,FACP retweeted

Jun 11
Key Discussions from IMWG 2026 - Samer Al Hadidi
@HadidiSamer @SurbhiSidanaMD @VincentRK
oncodaily.com/voices/samer-a…

1
7
226
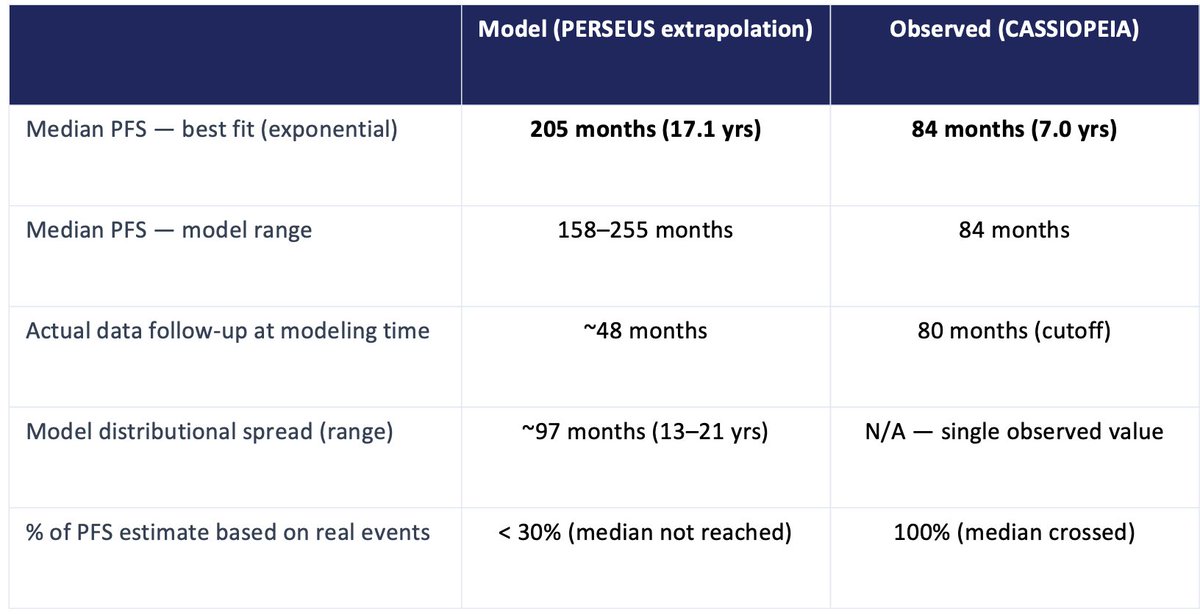
#mmsm #IMWG26
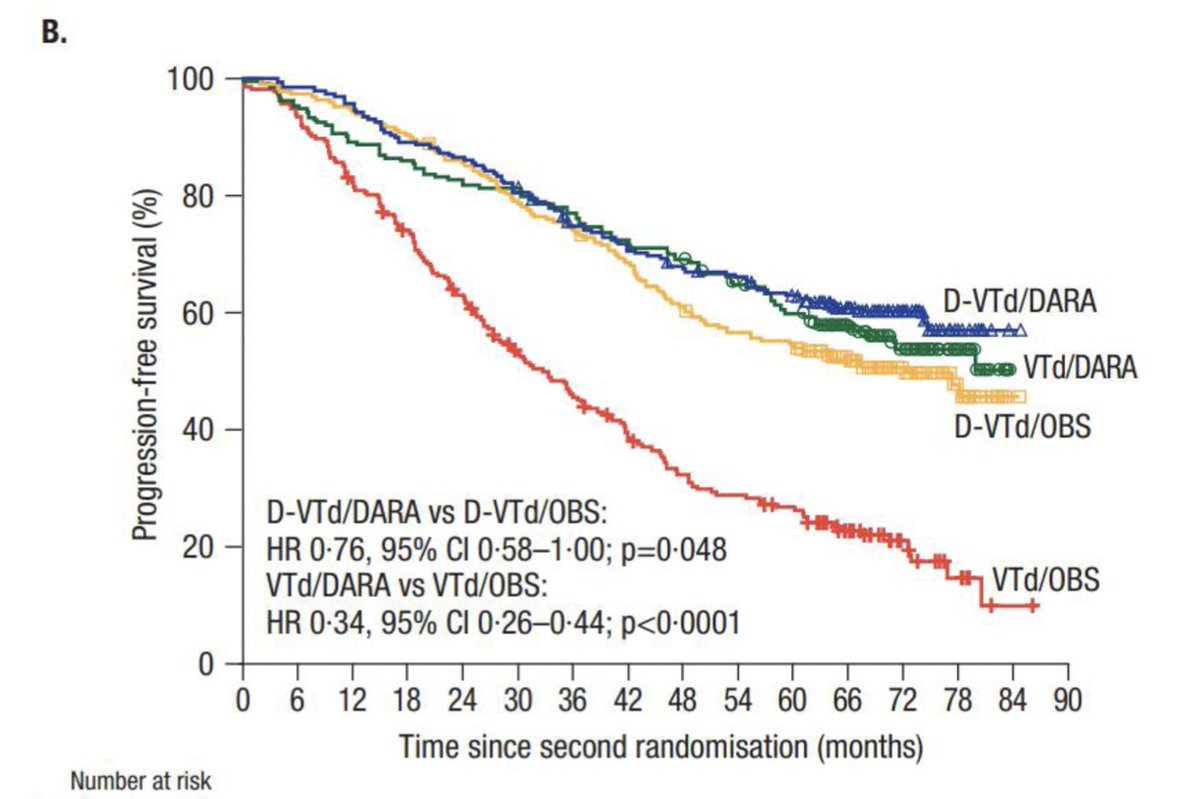
One important discussion point brought by @VincentRK was to be careful about the assumption that PERSEUS study PFS will be 17 yrs
While outcomes are great with quad based therapies in transplant eligible patients, such modeling need to be taken with grain of salt
Here is why
🧵
2
19
52
6,192
#mmsm #IMWG26
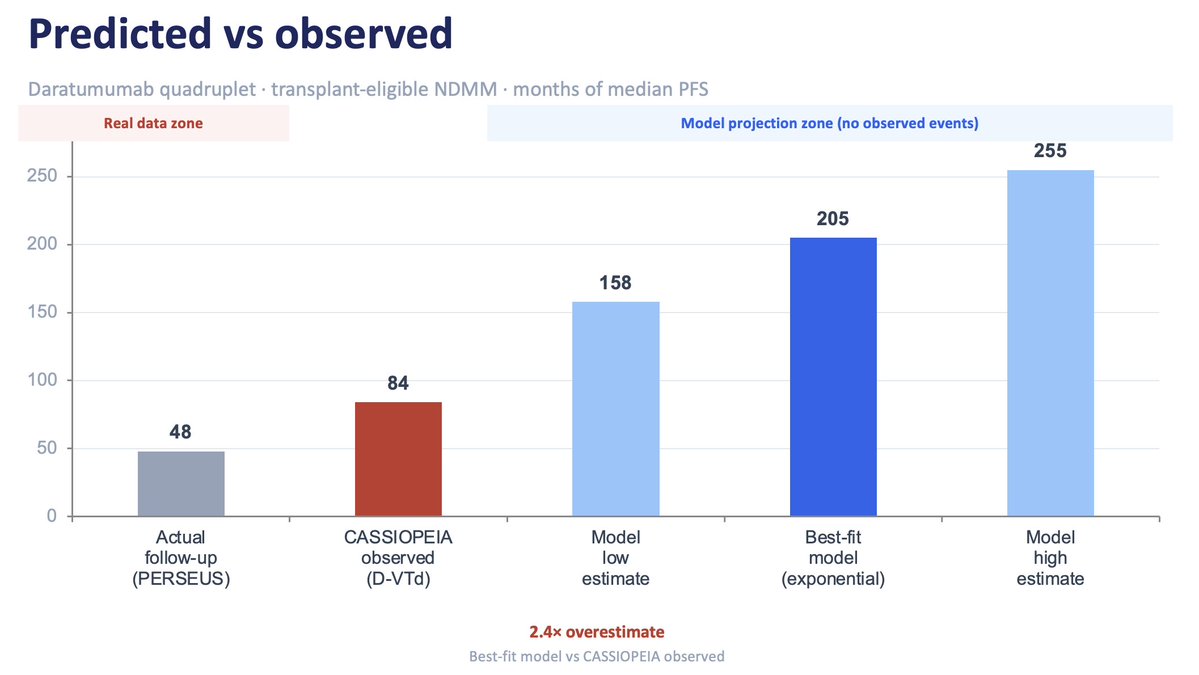
3⃣Why overestimation happens?
➡️The "best fit" model chosen was exponential, which assumes the risk of progression never changes over time
🛑That's not how myeloma progression occurs. Hazard increases over time. Patients who are still in remission at year 5 are a selected group
So the key issue is that exponential models on immature data systematically overestimate long-term PFS👇
1
1
11
1,441