
Associate Professor, FESC, FEHRA, Cardiac Electrophysiologist, Sports Cardiologist, Editorial board JICE, Surfer and Kitesurfer 🏄🏽♂️, Sarcoma Survivor
Joined December 2017
- Tweets 2,247
- Following 546
- Followers 2,210
- Likes 5,526
537 Photos and videos




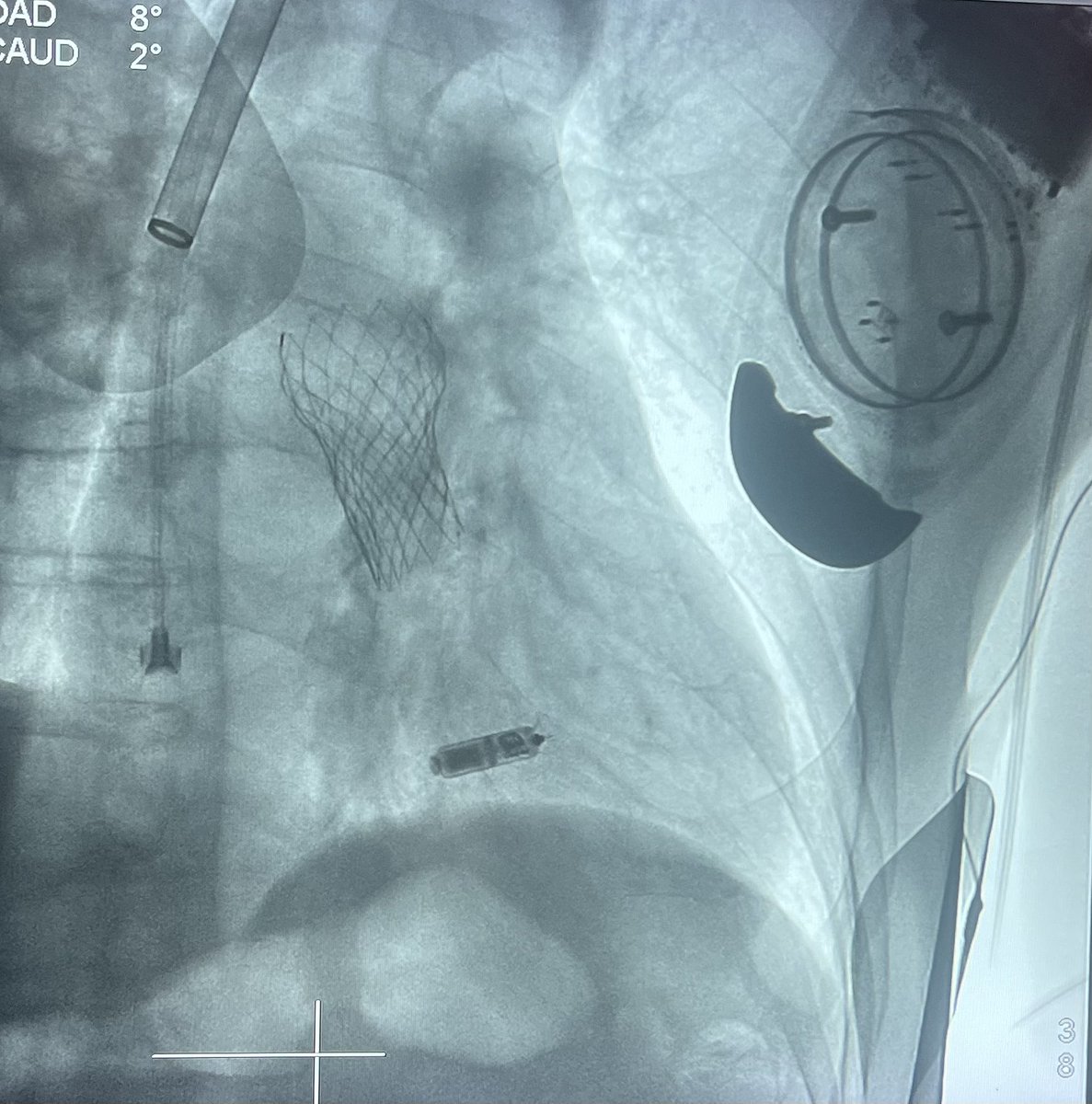




Concomitant #leadless #pacemaker #implantation & dual chamber #pacemaker lead #extraction #TLE for staphylococcus aureus #CIEDS #infection, in 95 y/o lady, 10 y after initial implantation and 1 month after gen change. Smooth procedure w Francesco Montereggi #Epeeps @rdschaller
2
3
27
2,915
#Genetics 🧬 is playing an increasingly important role for #Epeeps. Participating in this interuniversity diploma course in inherited cardiac diseases was a great opportunity to deepen my knowledge in #cardiogenetics. Merci beaucoup to everyone involved.
4
293
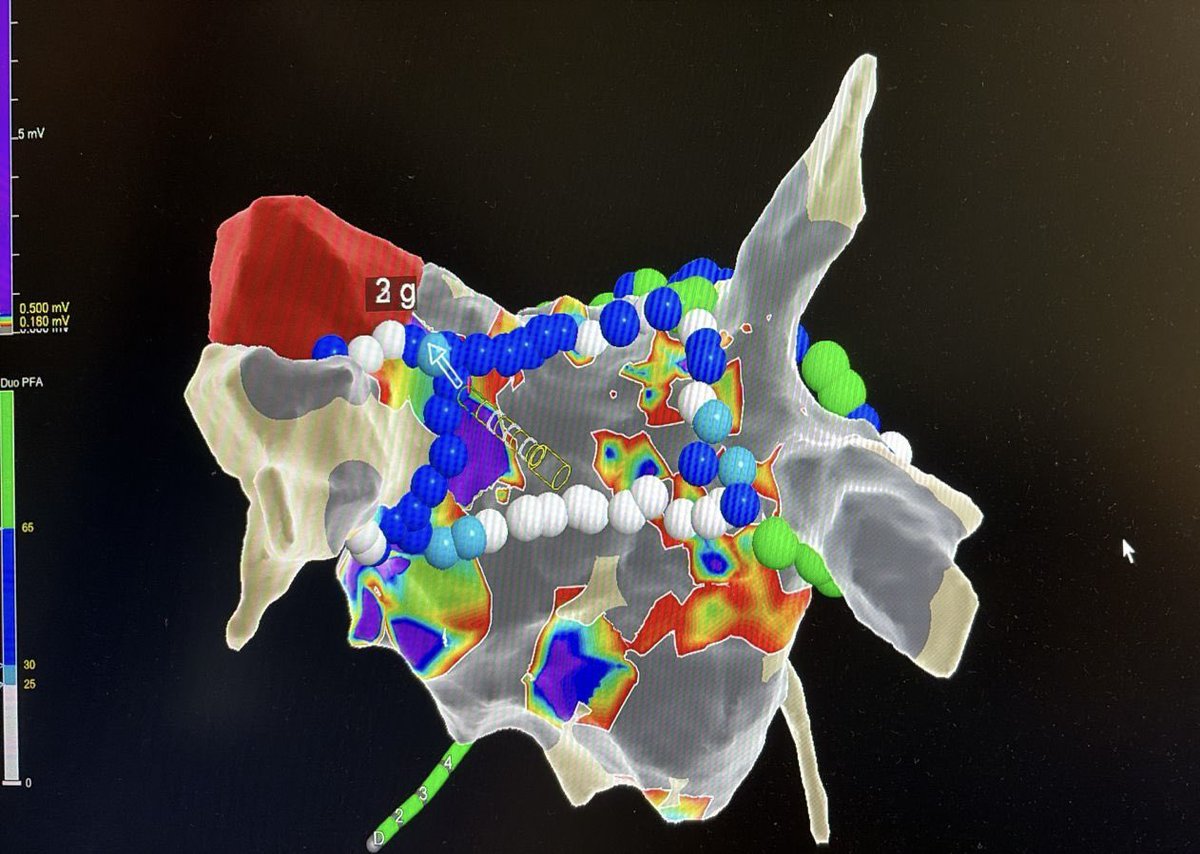
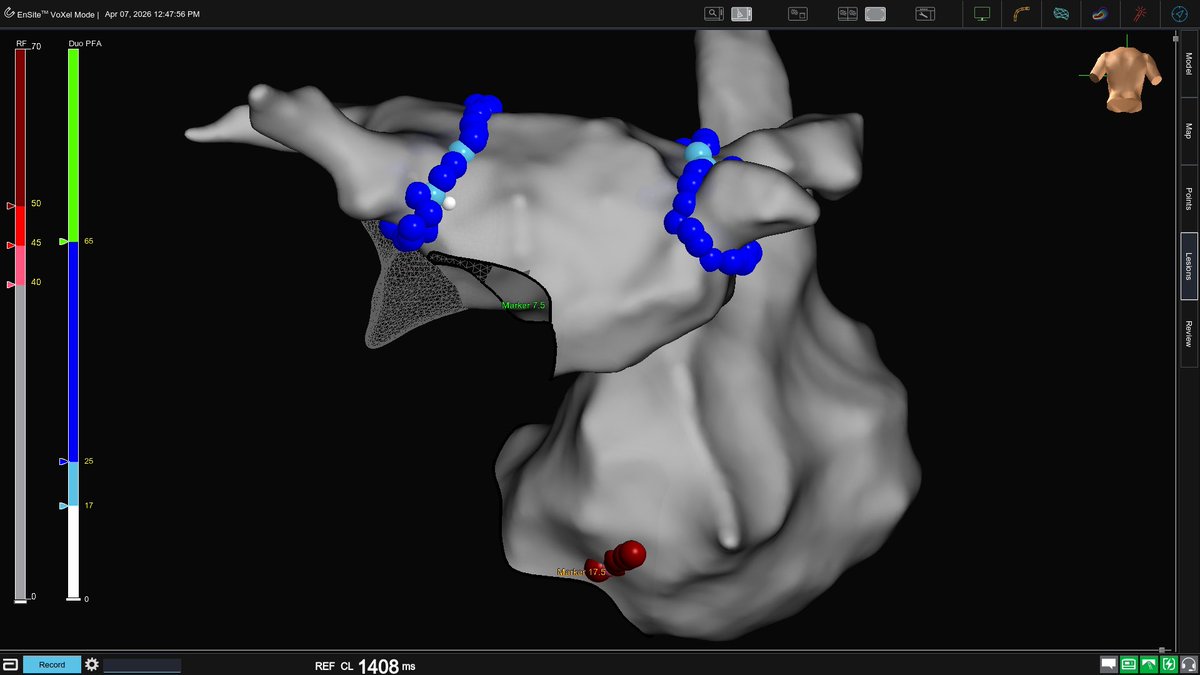
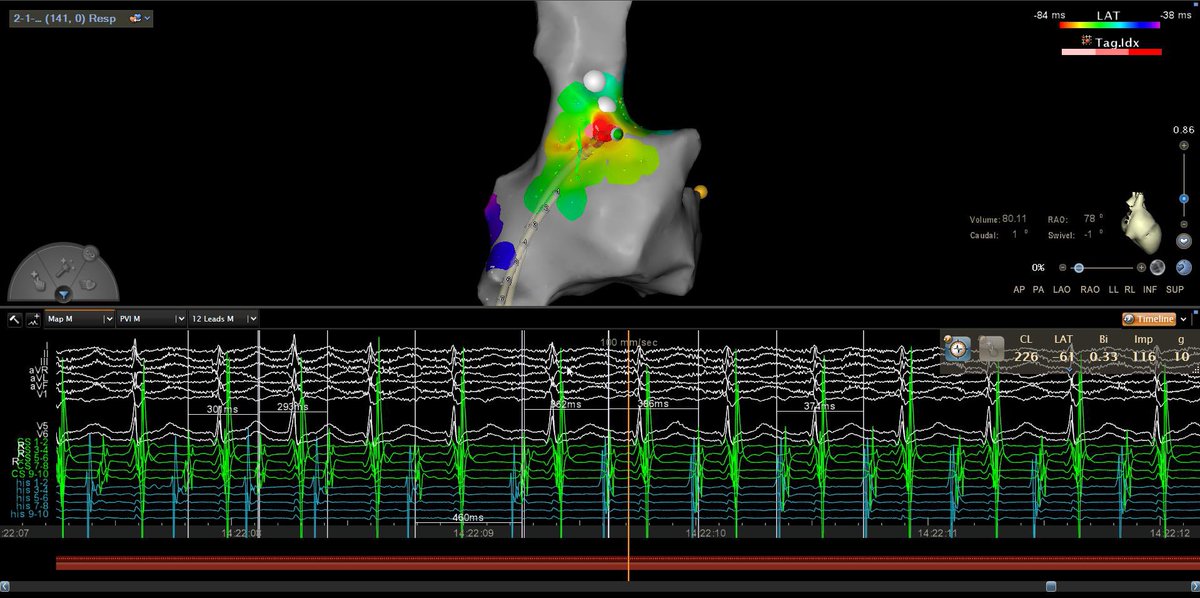
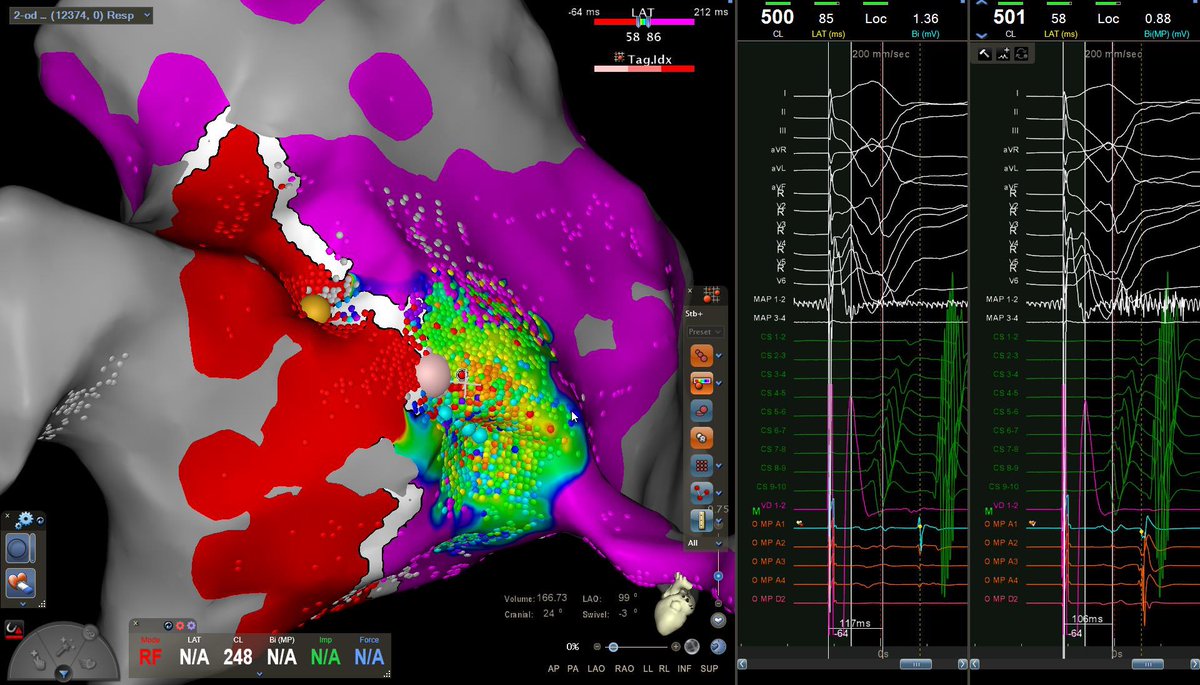
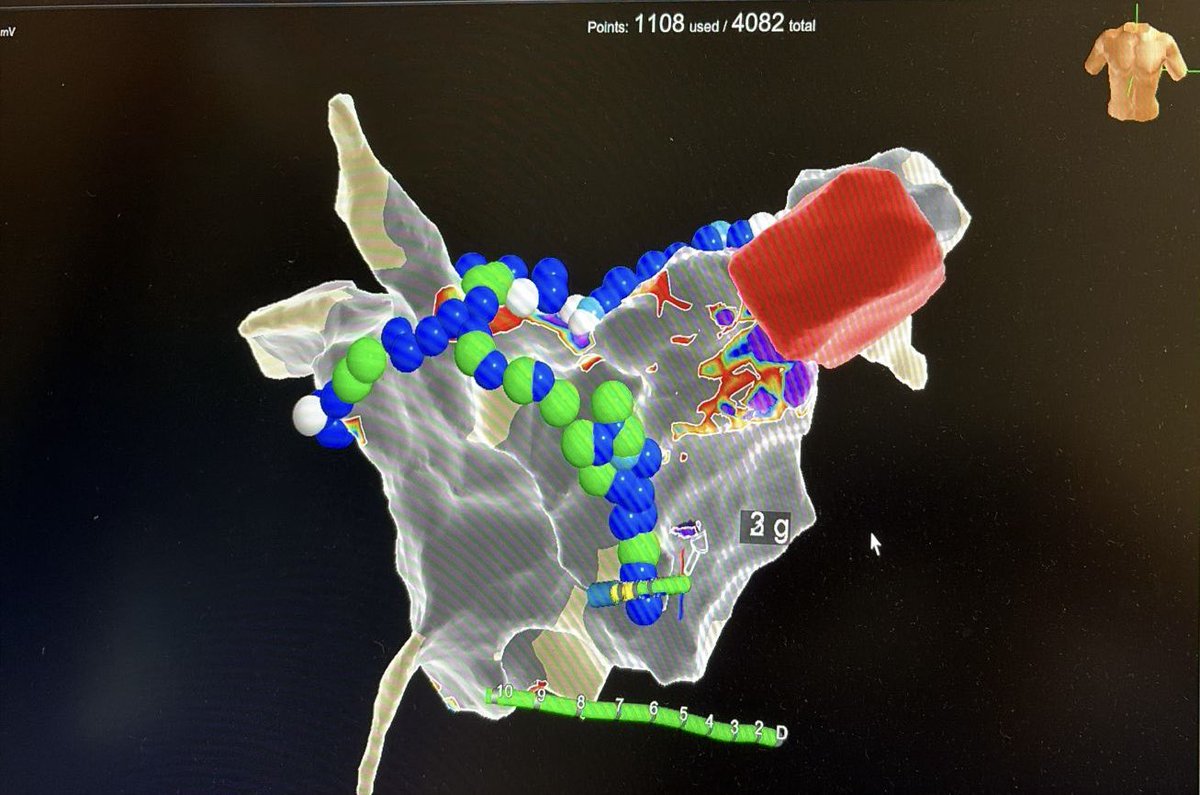
60F with longstanding AF after rheumatic valve disease. Bioprosthetic MVR. Extensive LA scar, unstable flutters limiting mapping. Empirical point-by-point PFA: first-pass PVI PWI anterior line with block. Will SR hold? 🤞 What would have been your strategy, #Epeeps ?
2
4
530
Andreas Müssigbrodt retweeted

May 22
Most important trial in modern EP and cardiology -- I'd be recruiting if the trial was in the US. A brave trial.
May 22

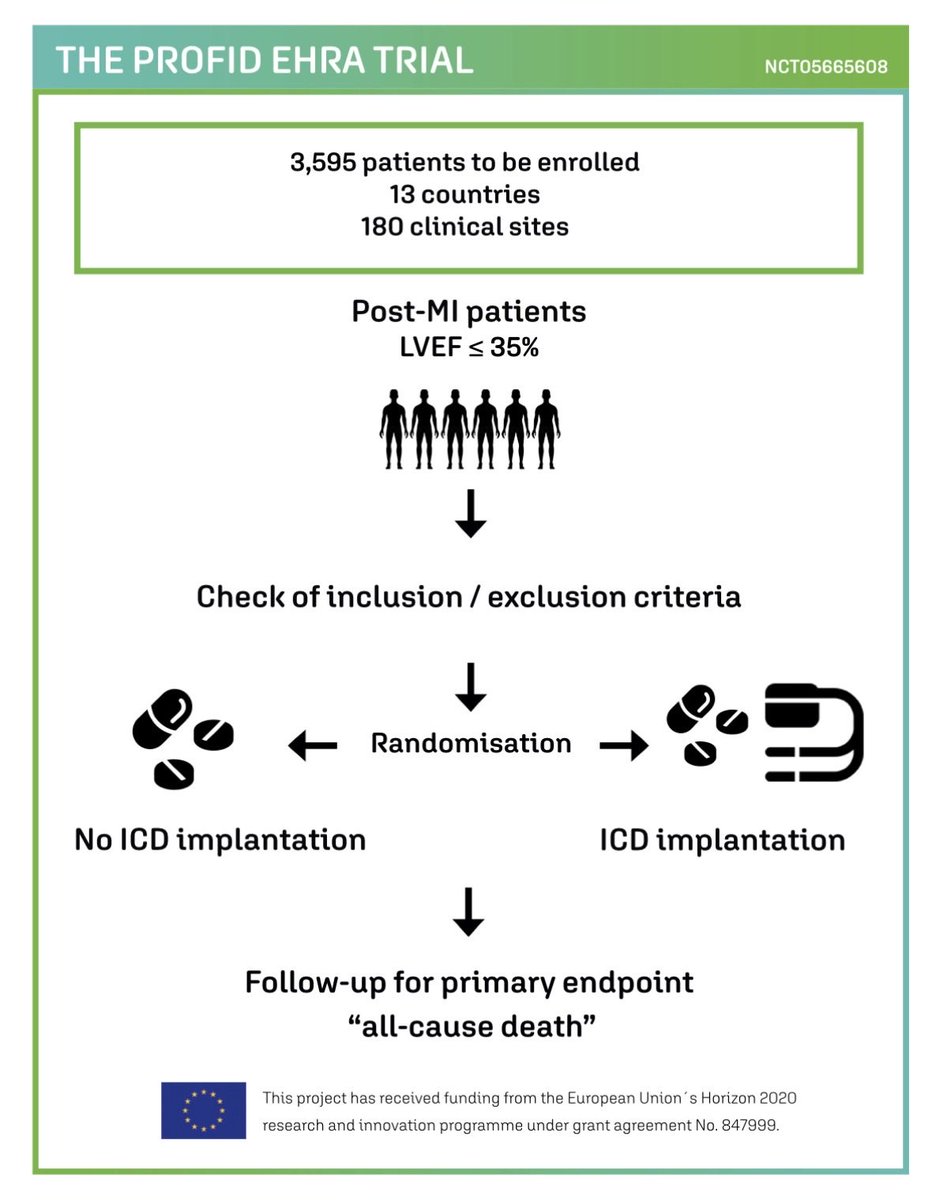
Encouraging all NHS Trusts to participate in the PROFID-EHRA randomised clinical trial testing the effectiveness of primary prevention ICD after #heartattack in severe #heartfailure on optimised pharmacotherapies.
Contact me if you would like to join.
5
16
104
29,450
Great event for #Epeeps! Thanks for sharing your knowledge.

Happy to attend today‘s online lead #extraction symposium #TALES2026 #TLE with @rdschaller @dredcronin and many other #Epeeps
1
434
Andreas Müssigbrodt retweeted

May 3
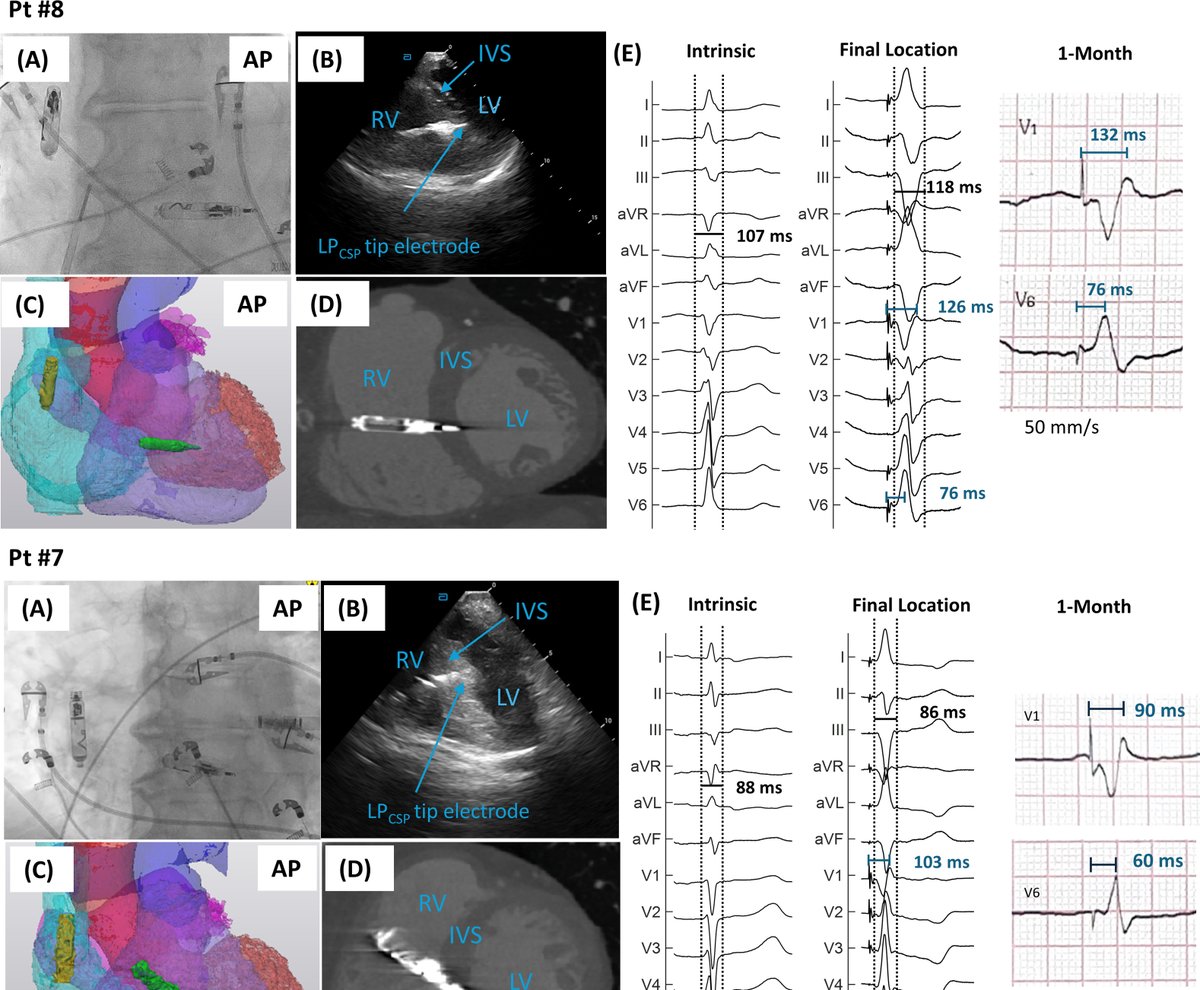
LEAP2: A First-in-Human Evaluation of a Chronically-Implanted Novel Leadless Pacemaker for Conduction System Pacing #OpenAccess
heartrhythmjournal.com/artic…
1
20
43
3,333
Andreas Müssigbrodt retweeted

4 May 2024
#EHRAtopicweek on electrical storm⚡
What to do when amiodarone and propranolol fail and catheter ablation is not feasible? Stellate ganglion block may be helpful.
Read more #Europace
doi.org/10.1093/europace/eua…
@EuropaceEIC

5
74
192
26,561



Andreas Müssigbrodt retweeted

Apr 25
🧵Should we use unipolar post wall mapping during AF ablation? Is endocardial silence in AF = posterior wall isolation?
Nice study in @CirculationEP by @Ed_Gerst et al. challenging both assumptions with human endo-epi mapping. Post wall = 3D substrate
ahajournals.org/doi/full/10.…
1
10
28
6,280
Andreas Müssigbrodt retweeted

Apr 23
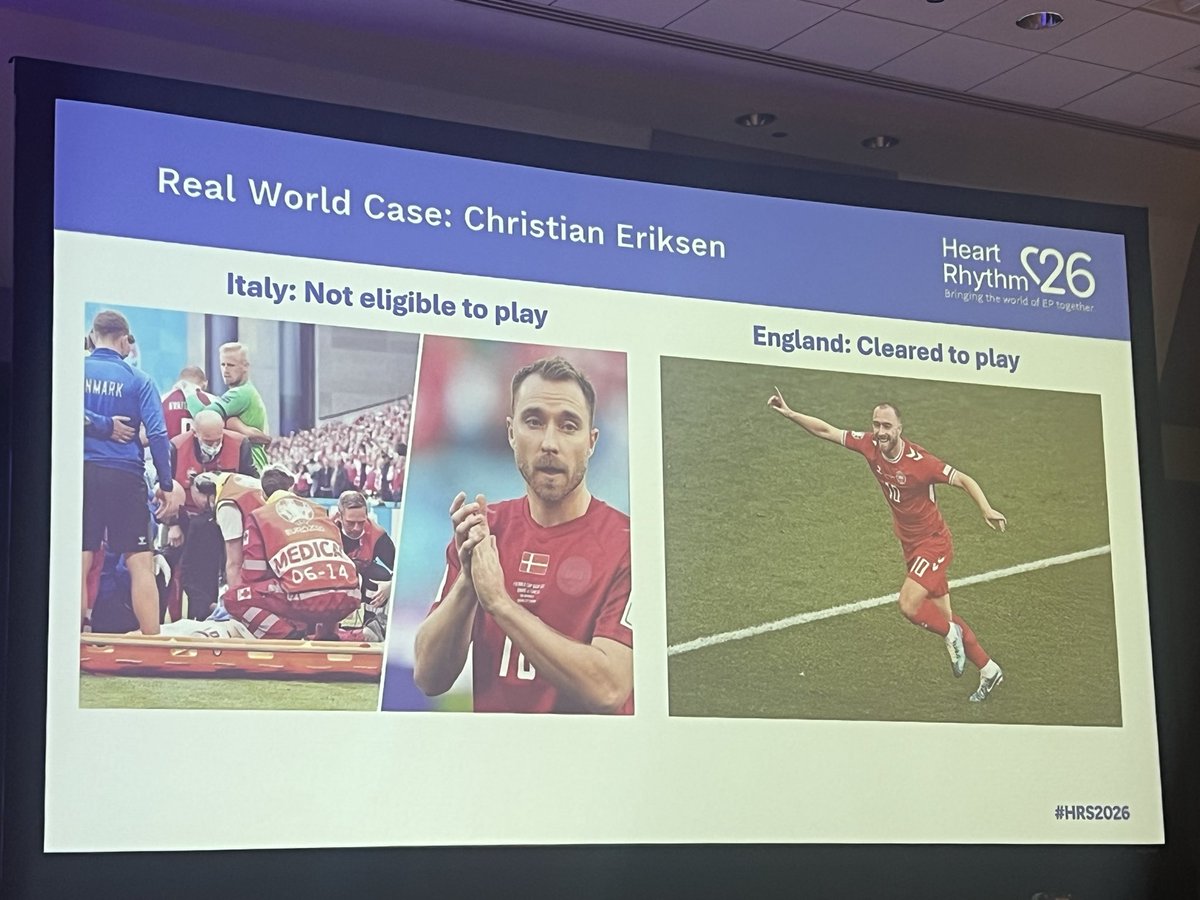
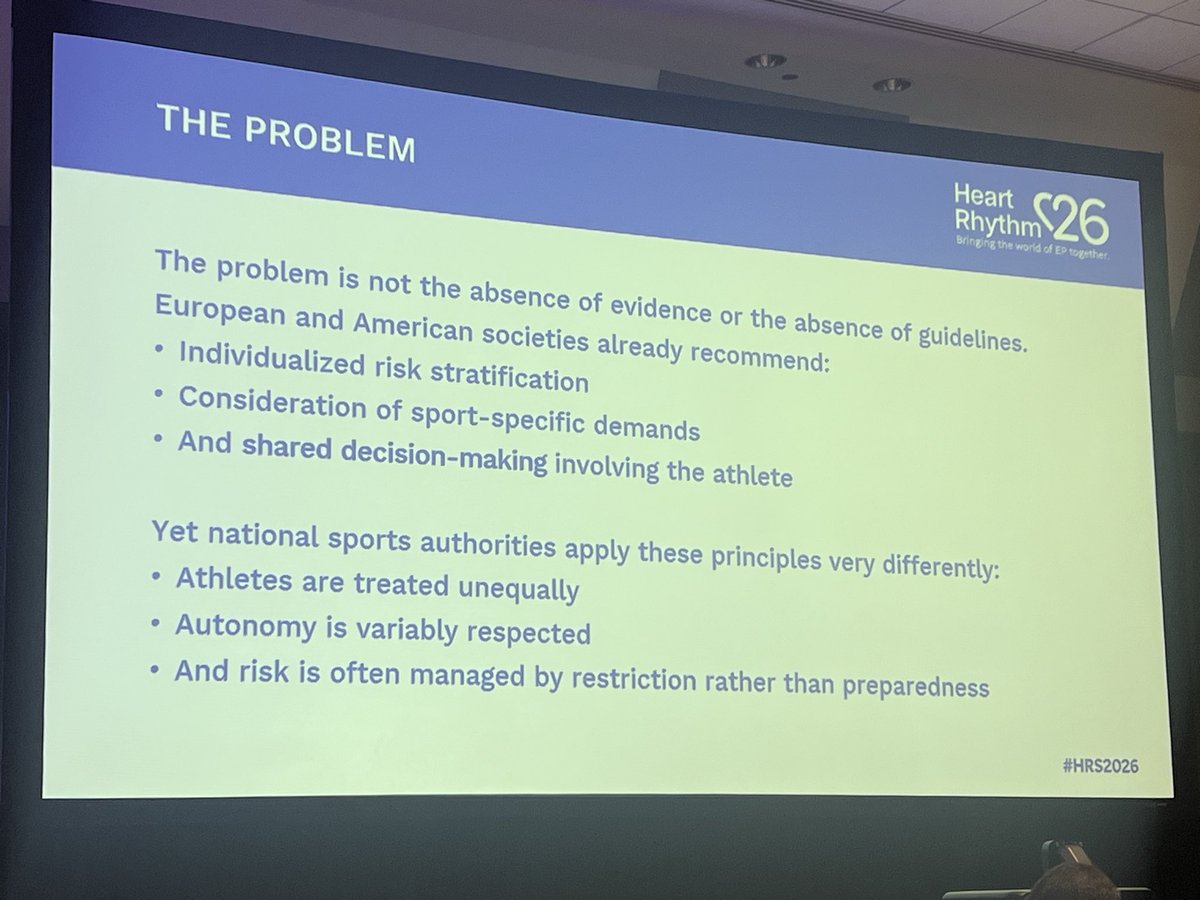
Same athlete, same heart condition,but different country- different career. Policies on professional sports participation for ICD carriers are NOT UNIFORM.
@EPWaveDoc at #HRS2026 :
❓Should athletes with ICDs be allowed to compete❓
Vote below and share your opinion!
@HRSonline

1
7
15
1,054
Andreas Müssigbrodt retweeted

Apr 21
There’s something uncomfortable about watching our field race forward with blinders on. Not out of ignorance, but because the path is familiar, the tools keep improving, and every new tech is met with celebration.
Stopping to question our direction has become harder than building the next catheter.
New tools are helpful, but they have not moved the needle enough to meaningfully change outcomes, and something important, I feel, is being missed.
I’ve had my share helping to build some of these technologies, and I believe in this work. But that’s exactly why I feel the responsibility to say this.
Take posterior wall isolation. It doesn’t help everyone. Trials keep coming back neutral, and they will continue to, until we understand which patients actually benefit and why.
We’ve spent decades refining how we record and read voltage and activation data, adding electrodes, improving algorithms. Indeed, the maps look better, but the outcomes, not so much.
PFA is a great advancement, easier to use, procedurally efficient, creates more consistent lesions. That matters, but it will not change the trajectory of clinical outcomes.
At some point, that pattern stops being a coincidence. It becomes a signal that we may not be solving the right problem. The real gap, I suspect, isn’t in our catheters or our maps. It’s in our understanding of the disease itself.
Why does an APC trigger AF in one patient and not another, or from one location and not from another? What is the true arrhythmogenic substrate- is it really scar? Is AF really a left atrial disease? We know it is not, so how do we identify who has right atrial disease, and how do we map and target it?
We don’t fully have those answers, and no new tool will give them to us.
Closing the mechanism gap, that’s the work we need to do. Everything else, is refinement within a paradigm that may have already reached its ceiling.
The blinders come off when we’re willing to slow down and ask whether we’re racing in the right direction.
I’m fortunate to have worked with an incredible team over the past many years, that has taken on some of these questions directly. We’ll be presenting our findings on April 25 at 9:30AM at the High Impact Science session, and I hope it’s the beginning of a longer conversation.
@HRSonline @BarkaganMichael @MilmanAnat @drjohnm
4
20
102
8,543
#Epeeps #Chicago is calling! At #HRS2026 I’ll talk about return to play of #athletes with #ICD: “Professional Sporting Organizations SHOULD Adopt Uniform Global Policies” I’ll defend my arguments against former #EHRA president Hein Heidbuchel @Heidbuchel60722
Feb 11

#SportsEP is having a moment, and we're all in!
Kicking off #HRS2026 in Chicago, Global Summit 2026 will bring together international leaders to tackle one of the biggest topics in EP today. Dive into fascinating conversations on:
🏈 Arrhythmias in Athletes
🏀 Exercise & Cardiovascular Health
⚽ Physiological Monitoring & Safety
⚾ SCA Prevention
Join the huddle and RSVP: bit.ly/3O6bB2p
Not registered for the meeting yet? Get in the game: bit.ly/3KzGmLs
@EduardoSaad3 @eugenechung01 @bdebneygray @SusanEtheridg12 @PrashSanders

6
7,264
Honoured that our case series on LMNA-related cardiac laminopathy was selected as Case of the Year 2025 (inherited conditions) in the European Heart Journal – Case Reports. Free access: academic.oup.com/ehjcr/artic…
Grateful to editors & co-authors especially Dr Patrice Bouvagnet 🙏
1
9
410
Pre-market release at CHU #Martinique: Abbott TactiFlex™ Dual Energy (#RF and #PFA) now in use. First cases by my colleagues while I was at #EHRA. Promising point-by-point approach to complement single-shot devices. #Epeeps #Cardiology

2
1
13
1,202
#Leadless #pacemaker implantation via right internal jugular vein in 80 yo patient with paroxysmal AVB after
#TAVI. Smooth procedure with Veauthyelau Saint-Joy at CHU de #Martinique. Procedure included in #VAMPIRE registry #Epeeps #Cardiology #Micra
1
4
881
Andreas Müssigbrodt retweeted
Apr 9
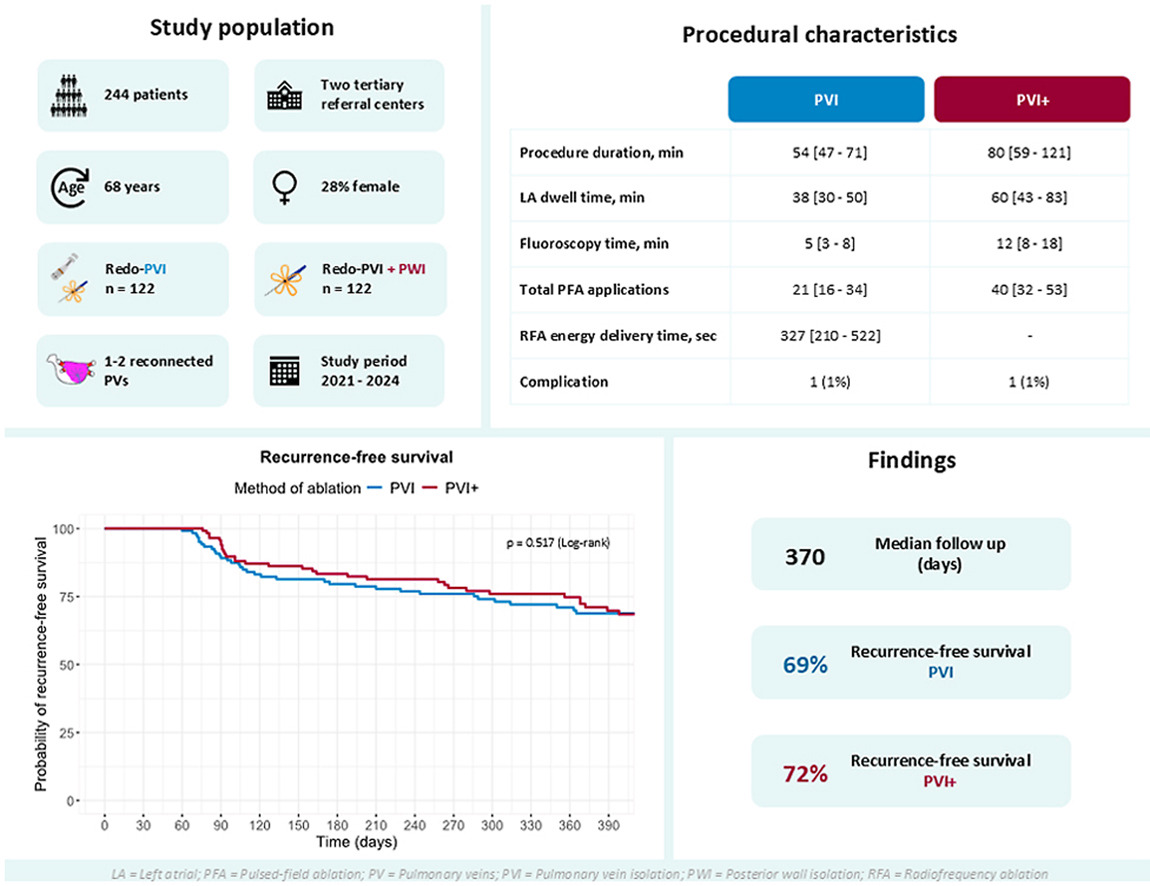
Small but nice study on LA posterior wall isolation. CAPLA trial found no benefit to PW isolation over PVI
Critics say you can’t durably isolate PW w RF. You need PFA. Well, w PFA in Switzerland, PFA posterior wall isolation also failed
Apr 9

Impact of Left Atrial Posterior Wall Isolation using Pulsed-field Ablation in Patients Undergoing Repeat Catheter Ablation for Atrial Fibrillation #OpenAccess
heartrhythmjournal.com/artic…
3
7
44
12,160

🚨Newest #FreeRead Article in
@JICE_EP
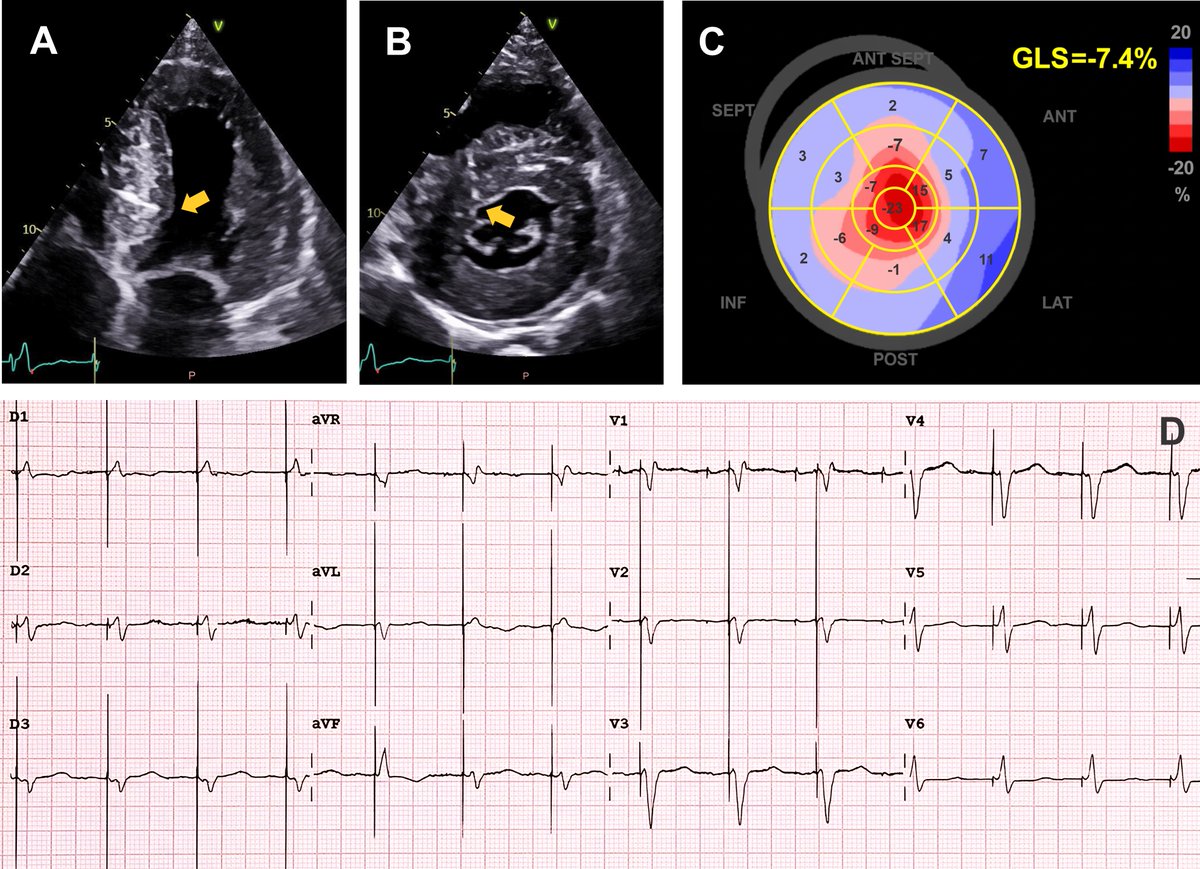
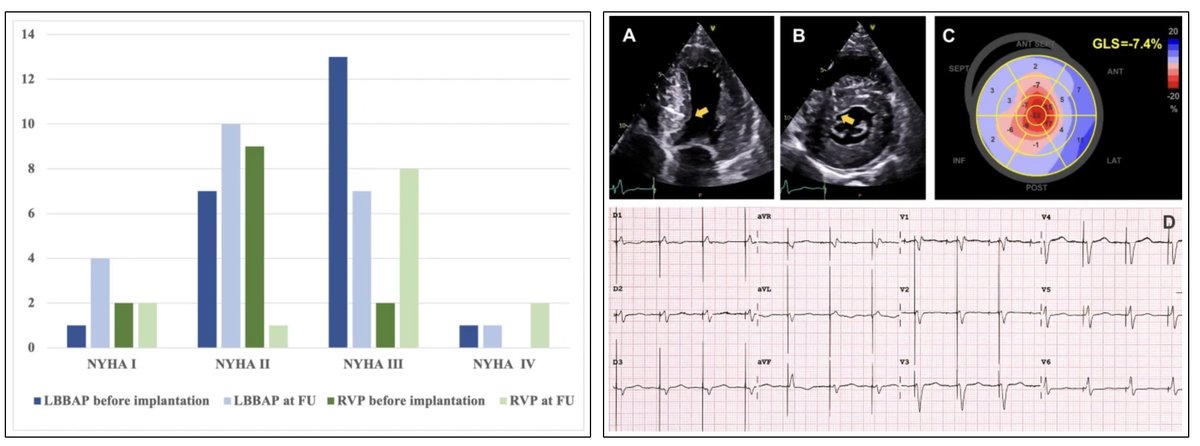
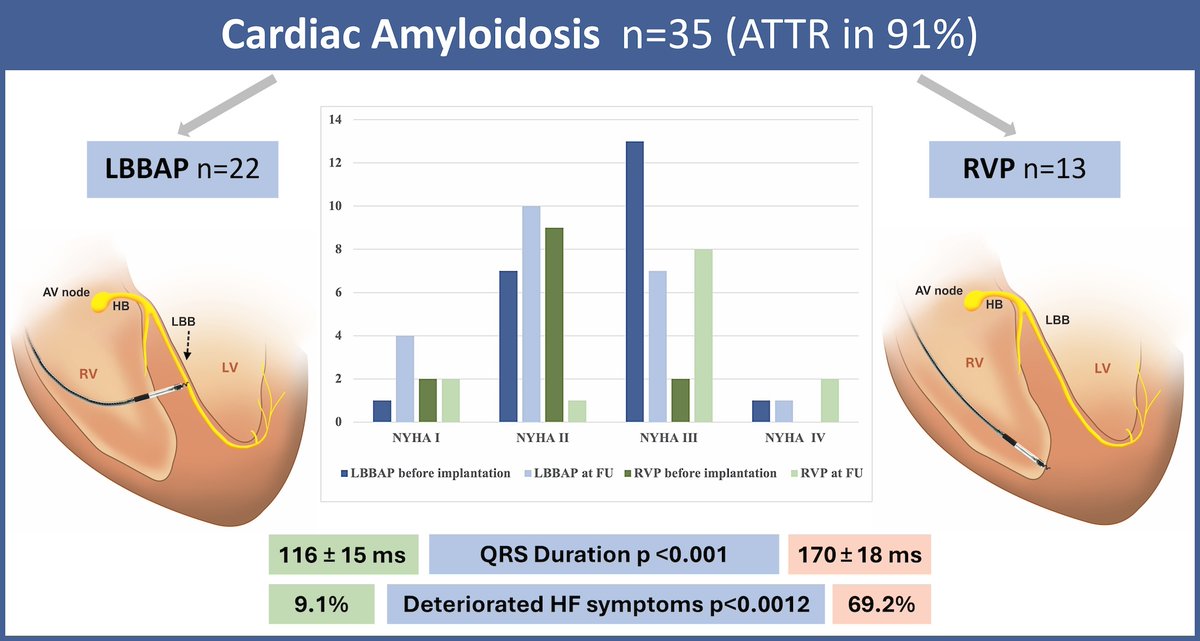
LBBAP versus RV Pacing in Cardiac Amyloidosis: the Left-Right CA study, a Single Center, Retrospective Comparative Non-Randomized Analysis
📖🧐rdcu.be/fbu4W
by @EPWaveDoc, Maria Herrera Bethencourt, Karima Lounaci, Francesco Montereggi, @RomainVergier, Mickael Cohen, Patrice Bouvagnet, Arnt Kristen & @GuramImnadze
#EPeeps
8
22
1,807
Sharing our recent work on pacing in cardiac amyloidosis mainly ATTR-CM. link.springer.com/article/10… In a retrospective single-center study, LBBAP was feasible & safe, with a signal toward improved HF outcomes vs. RVP. Findings are exploratory, need confirmation. #Epeeps #LBBAP #ATTR
5
16
849
Happy to attend today‘s online lead #extraction symposium #TALES2026 #TLE with @rdschaller @dredcronin and many other #Epeeps
3
4
1,081
#Leadless pacemaker implantation and dual chamber #pacemaker lead #extraction for CIEDS infection, in one procedure #Epeeps #Cardiology
1
4
24
2,542