
MD, FRCPath, FIAC
Joined June 2023
- Tweets 488
- Following 116
- Followers 1,141
- Likes 345
248 Photos and videos




Pleural fluid cytology.
👉 75-year-old female with:
▫️History of advanced anal squamous cell carcinoma (treated with chemoradiotherapy in 2012)
▫️History of breast carcinoma on follow-up
#PathTwitter #Cytopathology #Surgpath #TRPS1
5
4
12
756
🗳️ What is your leading diagnosis based on the available history immunophenotype?
0%
Breast carcinoma mets
0%
SCC mets
0%
Mullerian adenoca mets
0%
Need more IHC/clinical
0 votes • Final results
2
2
228
⚠️ Apologies for the intentionally incomplete history in the original post.
The aim was to demonstrate how even a useful marker such as TRPS1 can be misleading when interpreted without the full clinical context.
🔬 No IHC marker is perfect.
📋 Clinical history matters.
🧩 Correlation matters.
The full diagnostic journey and take-home lessons are shared below 👇

🔬 A Cytology Lesson:
One Marker • Two Histories • Three Primaries !!!
👩⚕️ Patient
• 72-year-old female with pleural effusion
• Initial history provided: Previous h/o anal squamous cell carcinoma and breast carcinoma
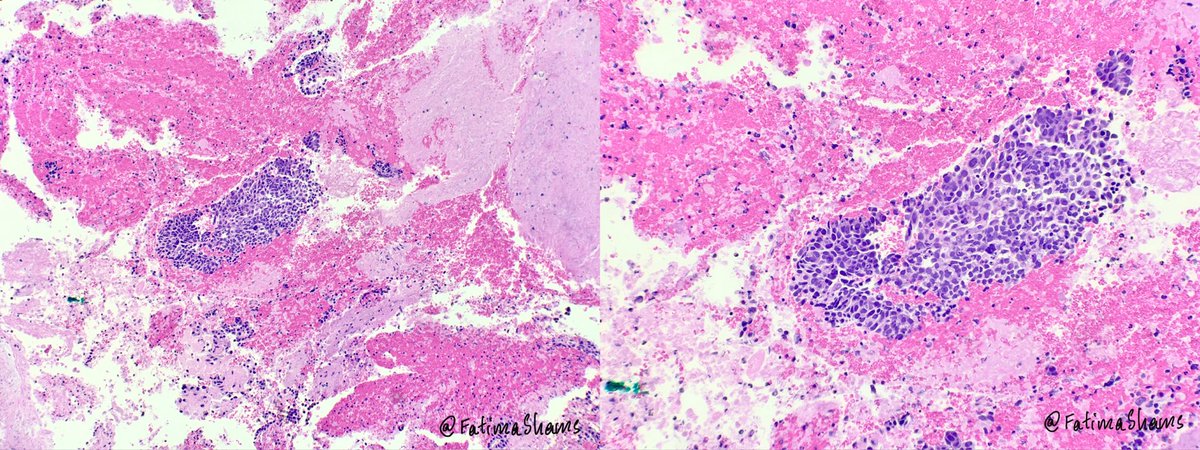
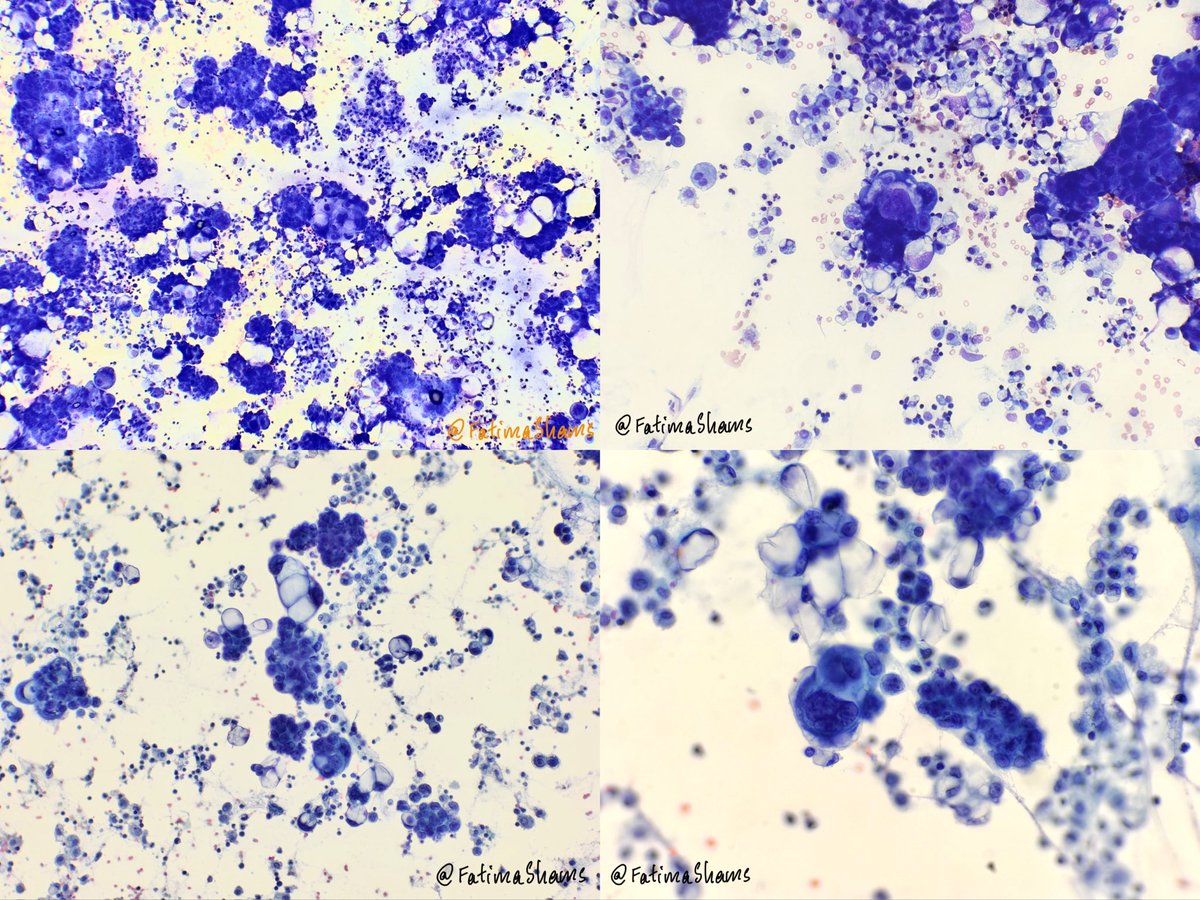
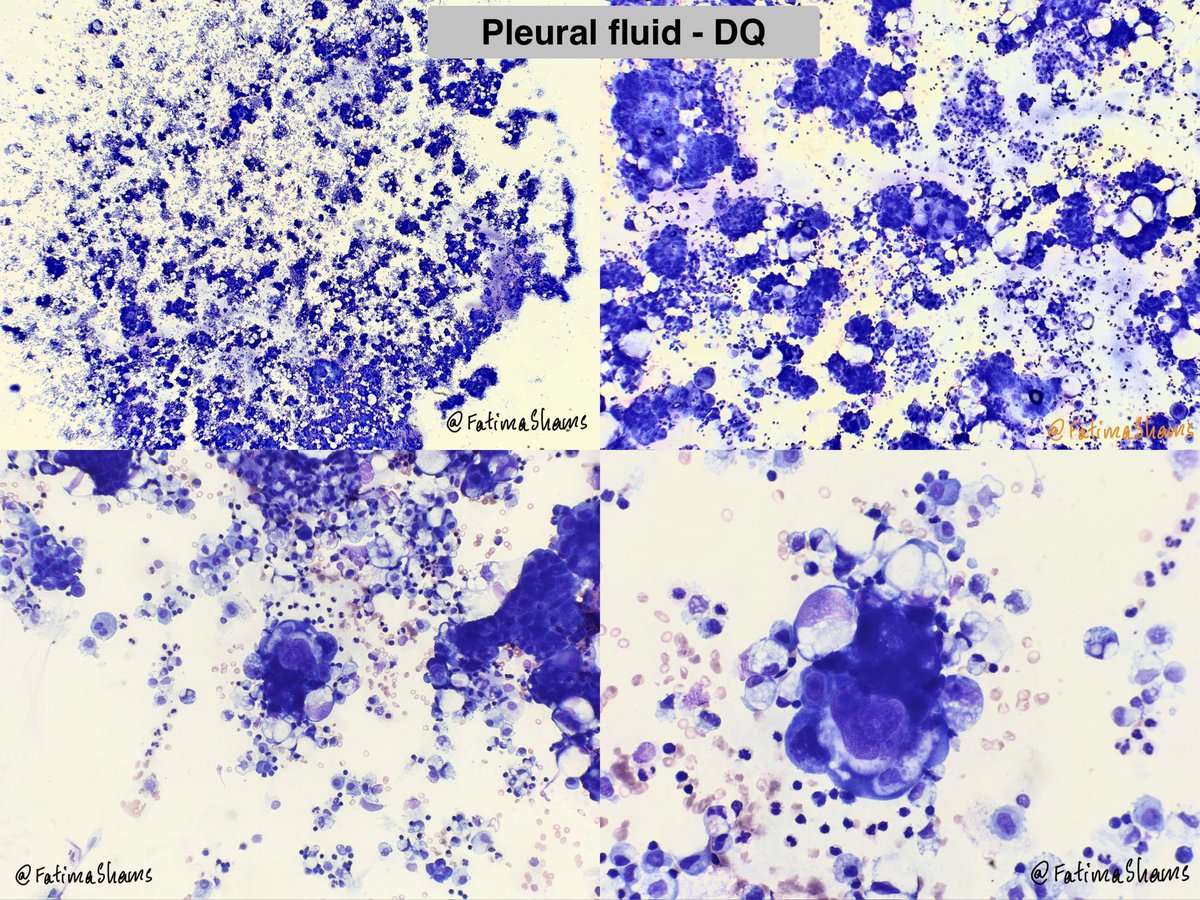
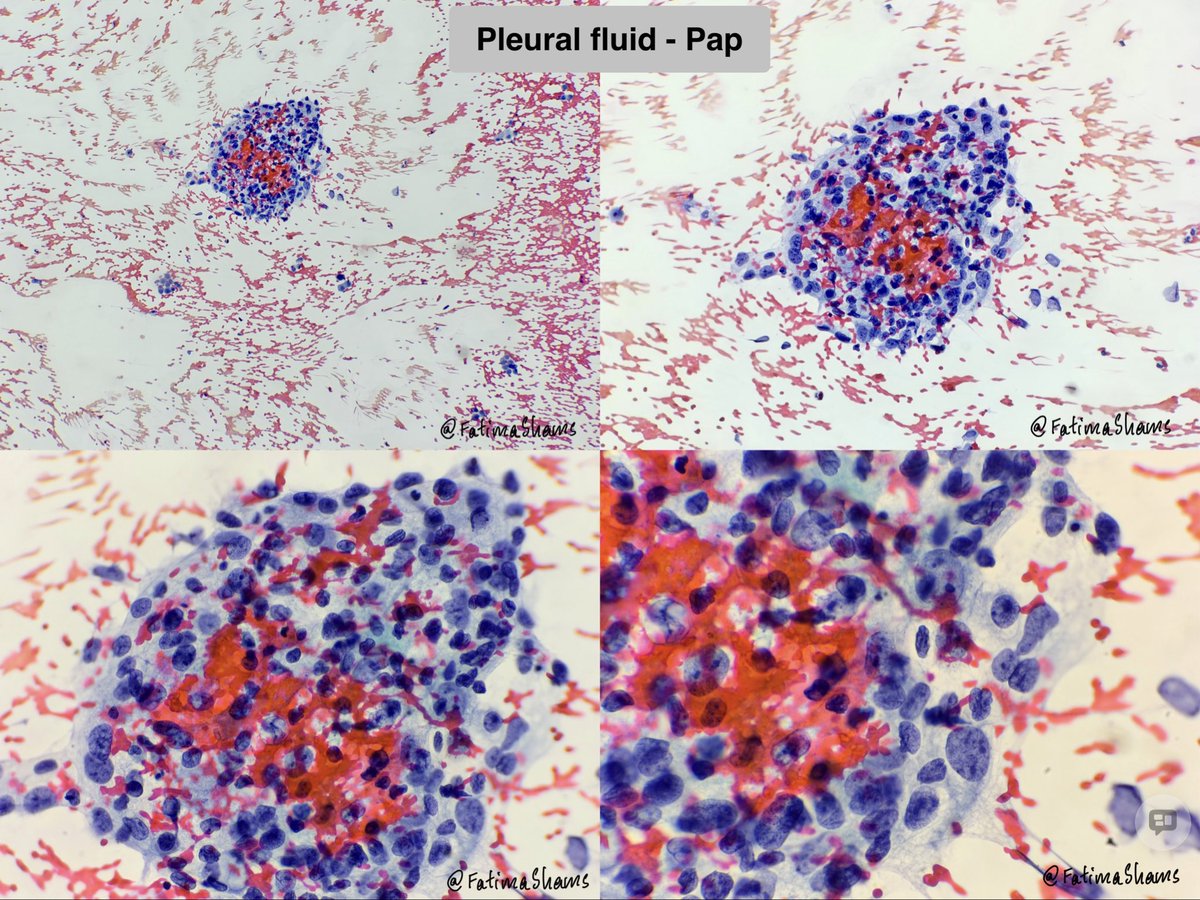
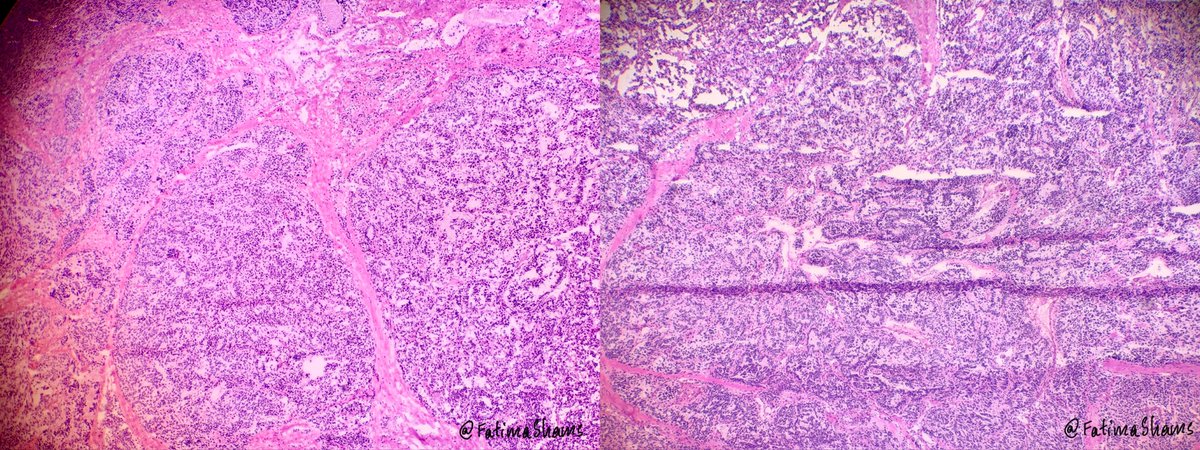
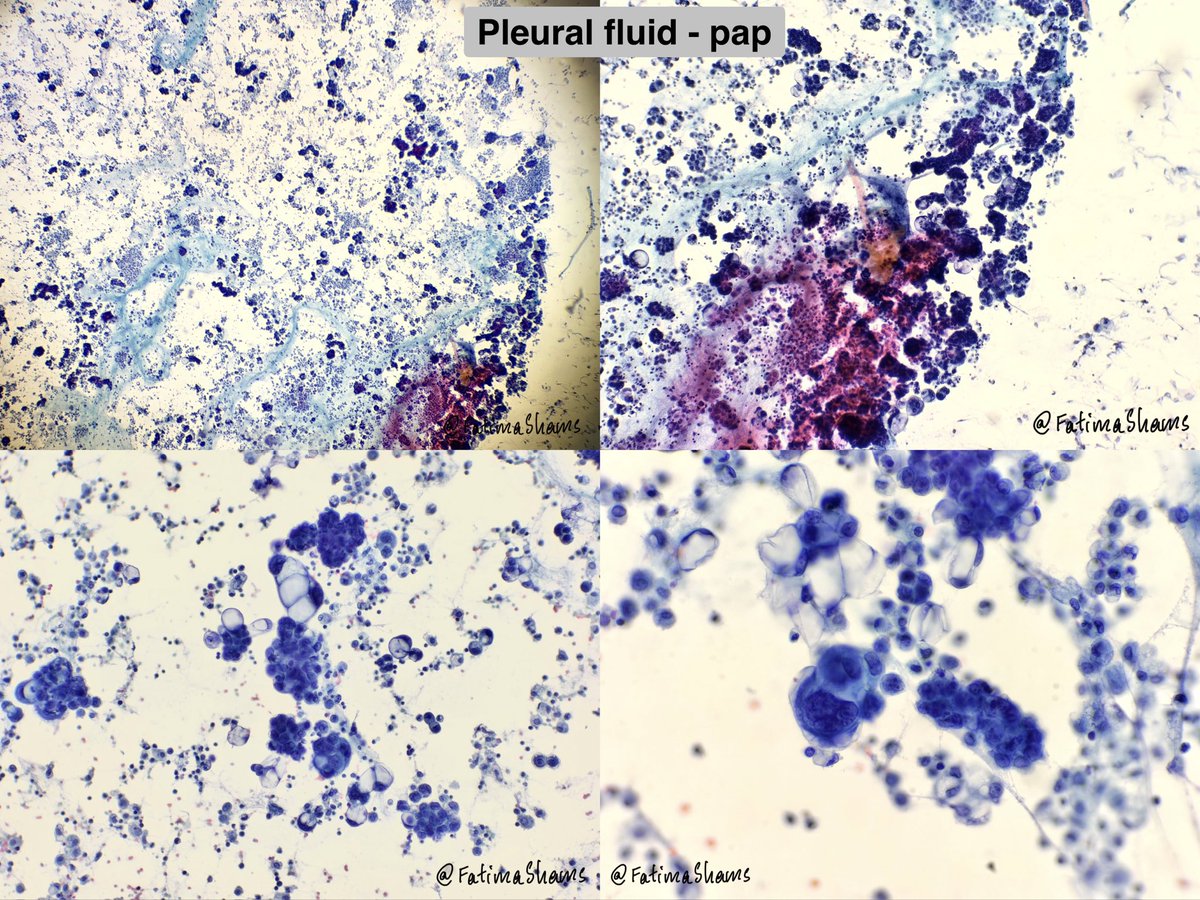
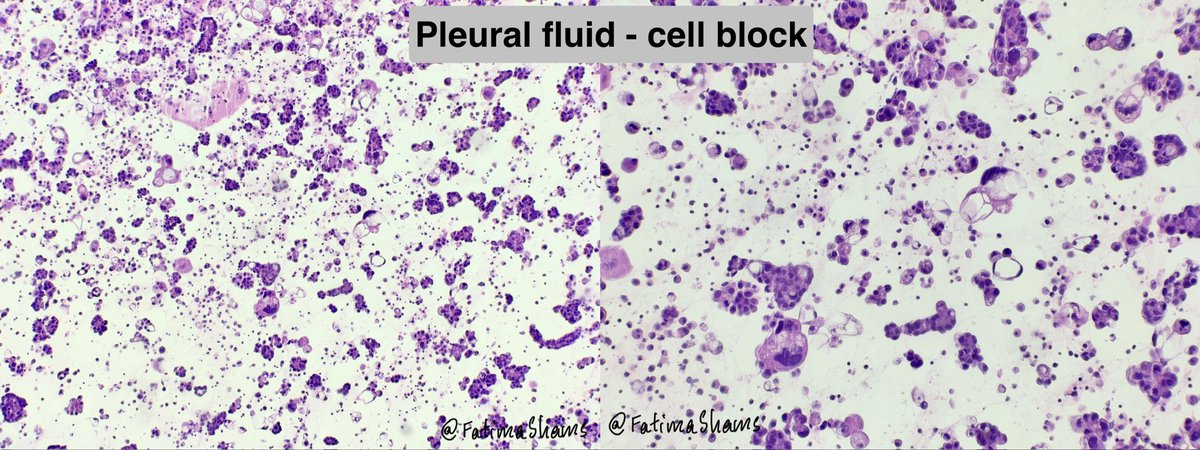
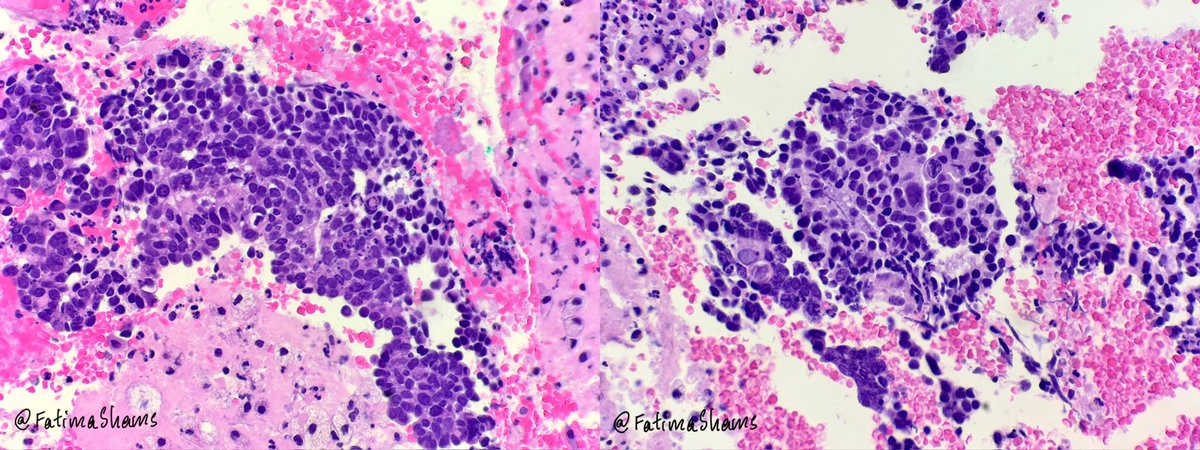
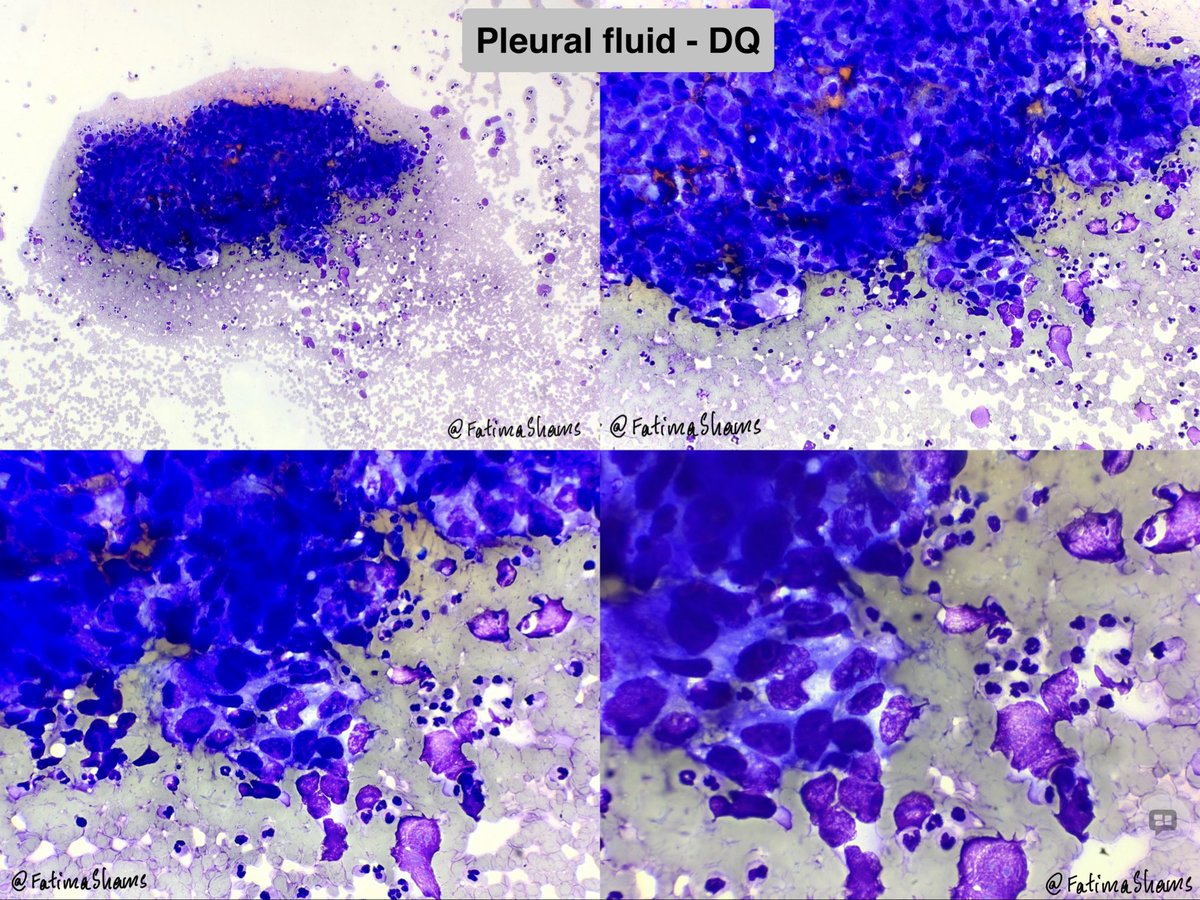
🔍 Cytology Findings
• Highly cellular specimen
• Malignant epithelial cells in clusters and 3D groups
• Marked nuclear atypia
• Occasional vacuolated cytoplasm
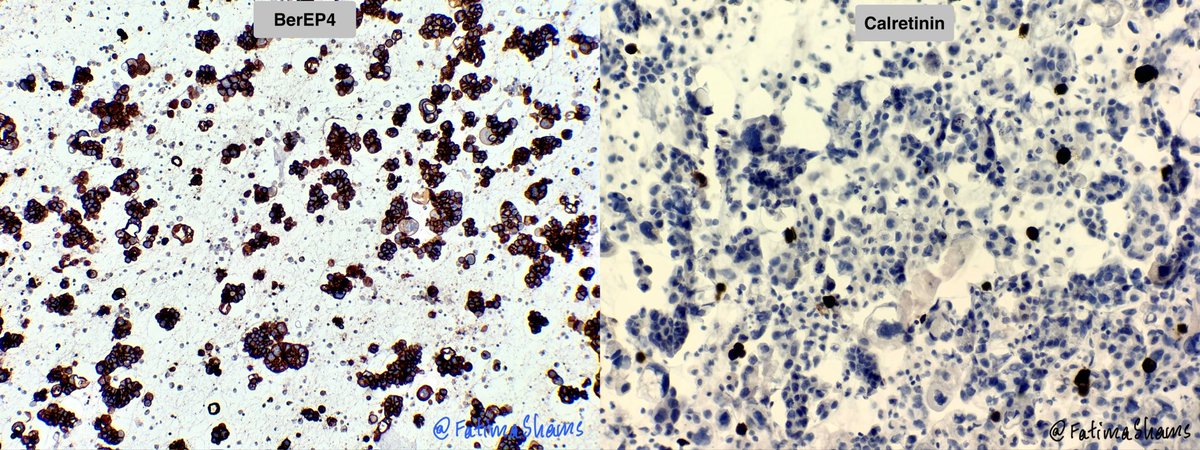
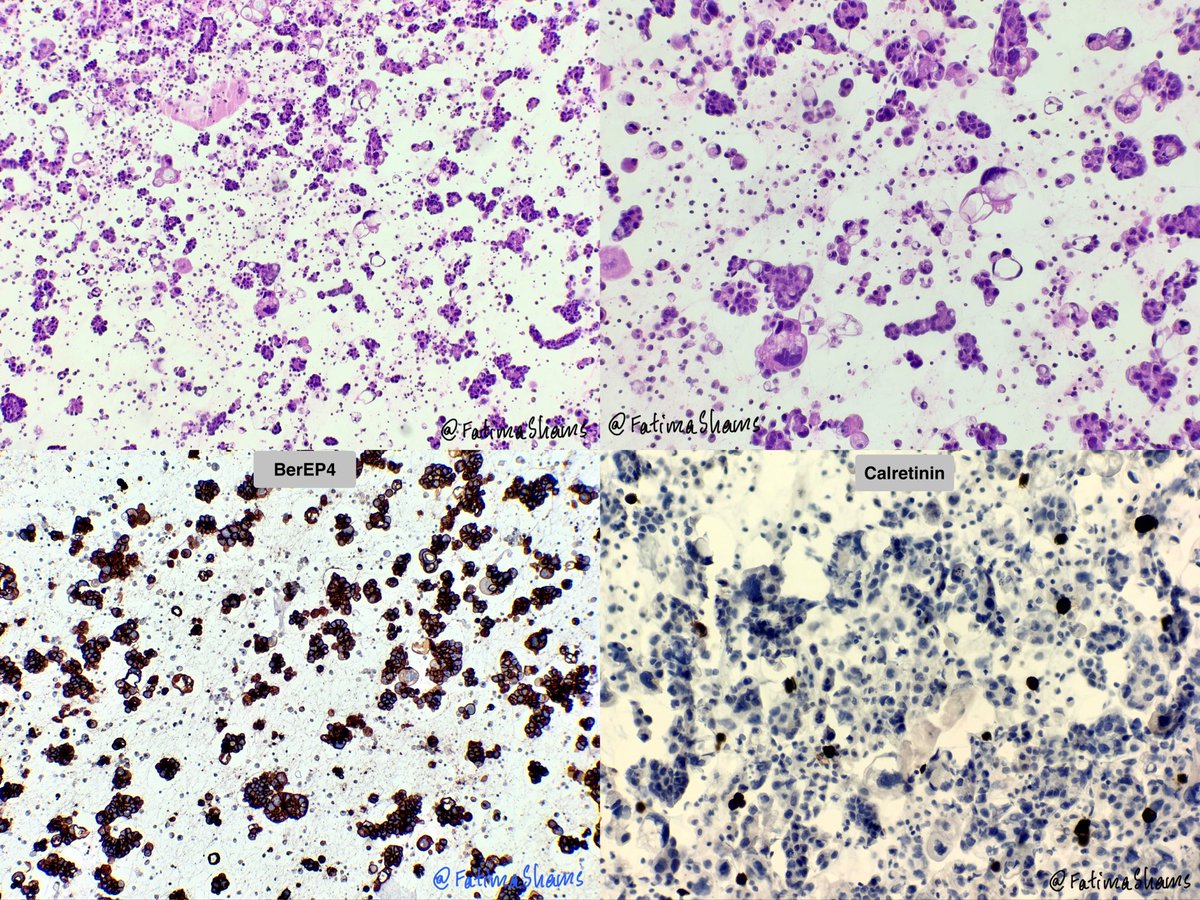
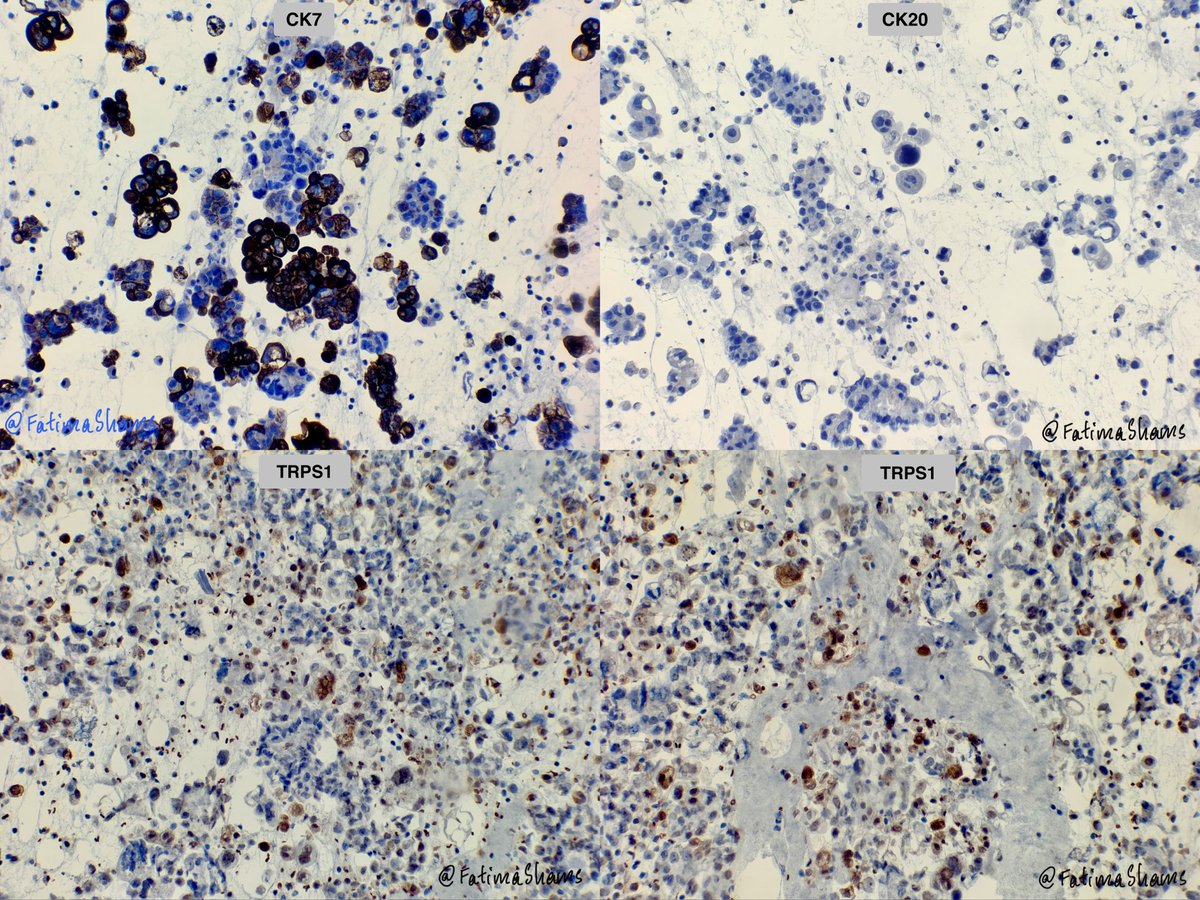
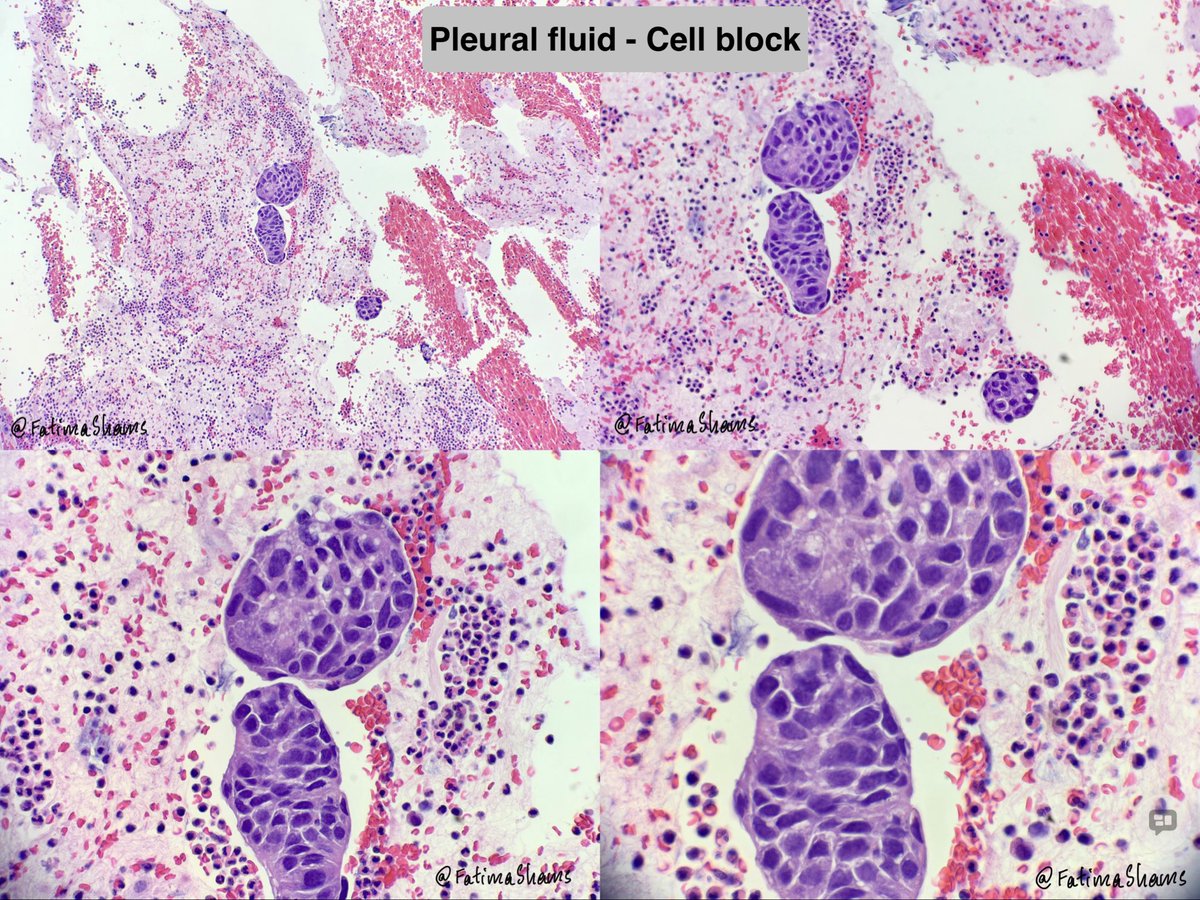
🧪 Initial Cell Block IHC
✅ BerEP4 positive
❌ Calretinin negative
✅ CK7 positive
❌ CK20 negative
🎯 Diagnostic Approach Based on Available History
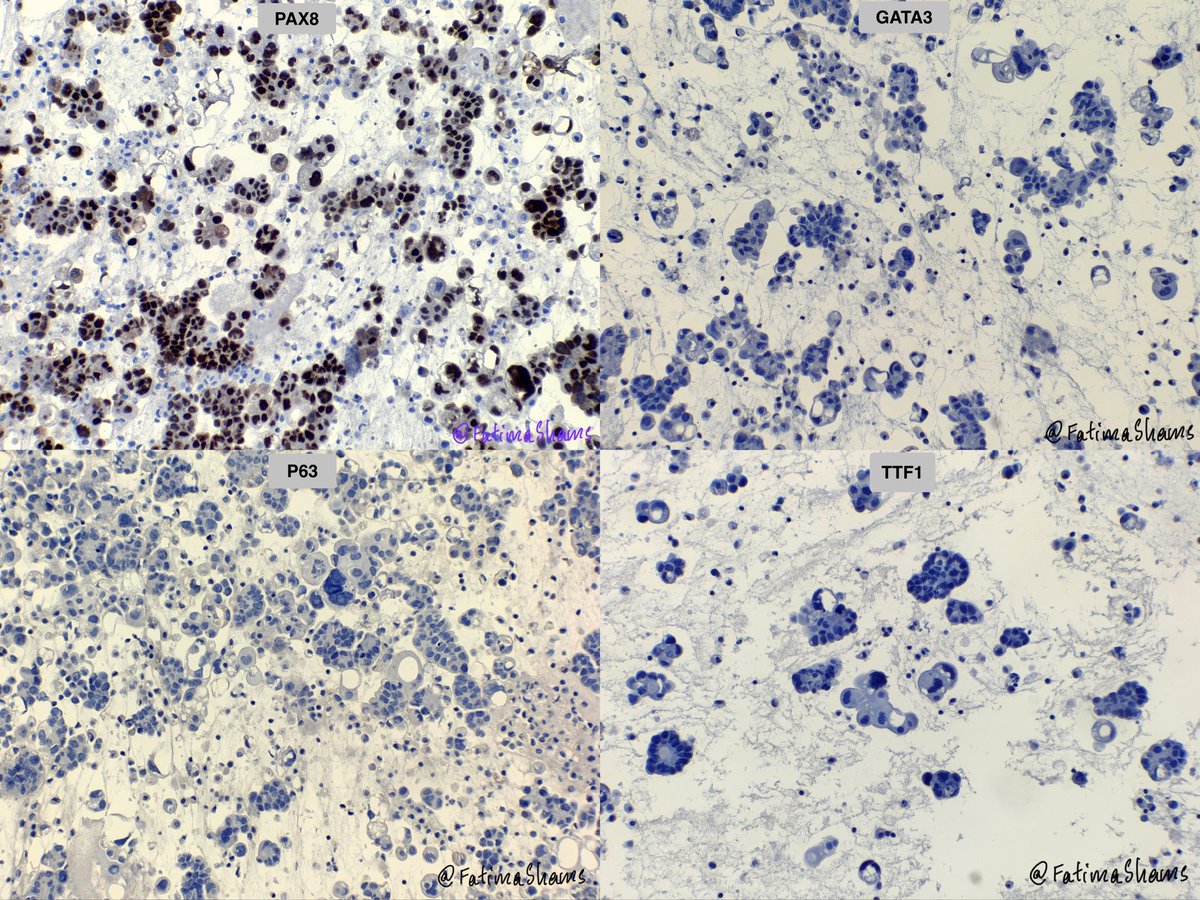
• TTF1 → to exclude primary lung adenocarcinoma
• p63 → to assess squamous differentiation
• TRPS1 → to evaluate possible breast origin
📋 Results
❌ TTF1 negative
❌ p63 negative
✅ TRPS1 patchy positive
⚠️ The Pitfall
With a history of breast carcinoma and a CK7 /TRPS1 profile, metastatic breast carcinoma seemed highly likely.
🔄 The Turning Point
• TRPS1 positivity was only patchy
• Additional clinical information was obtained
• Histologic correlation was performed
🧩 The Missing History
The patient also had a recently diagnosed endometrial malignancy with frozen pelvis and extensive local spread, a crucial piece of information that was not initially available.
🧬 Further Workup
✅ PAX8 positive - favor mullerian
❌ GATA3 negative - point against breast cancer
📌 Final Interpretation
Metastatic Müllerian carcinoma, with correlation favoring high-grade serous carcinoma.
💡 Take-Home Messages
✔️ TRPS1 is a useful marker, but not entirely specific for breast carcinoma.
✔️ Patchy TRPS1 positivity can be seen in Müllerian serous carcinomas and other non-mammary tumors.
✔️ Never interpret immunostains in isolation.
✔️ Morphology Clinical History Imaging Histology Correlation = Accurate Diagnosis.
✔️ Always question a result that does not perfectly fit the overall picture.
🏆 Lesson Learned
💎 The most important diagnostic tool in this case was not TRPS1—it was the missing clinical history.
#Cytopathology #PleuralFluid #DiagnosticPitfall #TRPS1 #BreastPathology #PathologyPearls #Cytology #ClinicopathologicCorrelation #PathTwitter #MedEd #LearningFromCases
1
56
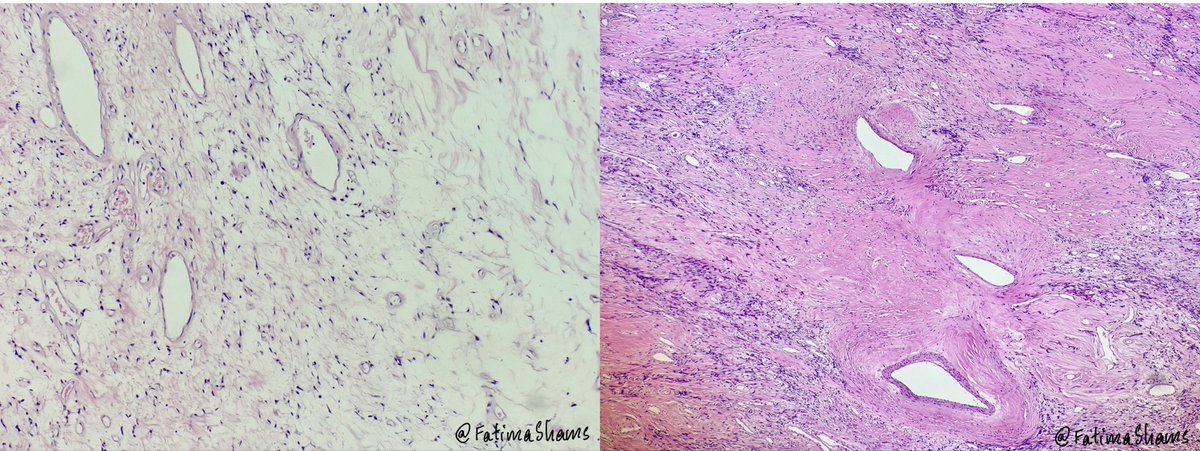
🔬 A Cytology Lesson:
One Marker • Two Histories • Three Primaries !!!
👩⚕️ Patient
• 72-year-old female with pleural effusion
• Initial history provided: Previous h/o anal squamous cell carcinoma and breast carcinoma
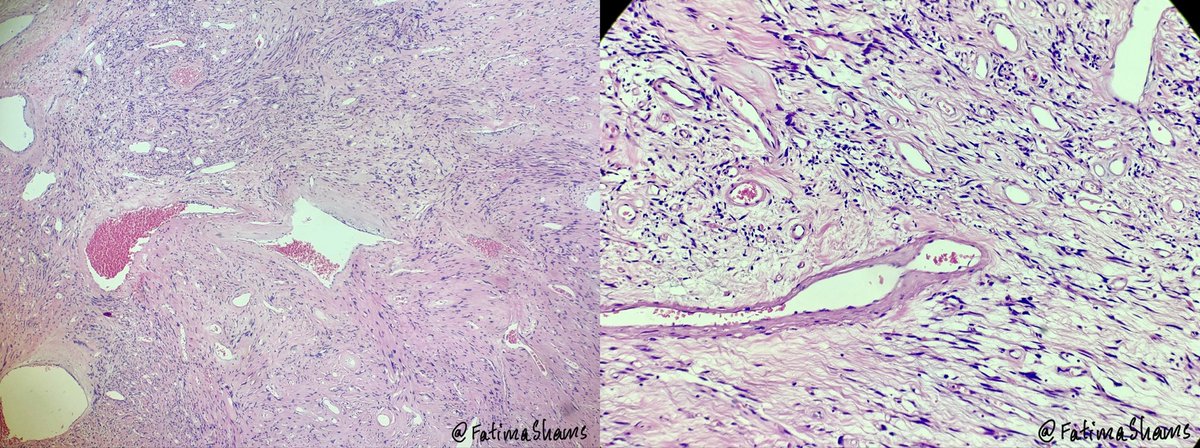
🔍 Cytology Findings
• Highly cellular specimen
• Malignant epithelial cells in clusters and 3D groups
• Marked nuclear atypia
• Occasional vacuolated cytoplasm
🧪 Initial Cell Block IHC
✅ BerEP4 positive
❌ Calretinin negative
✅ CK7 positive
❌ CK20 negative
🎯 Diagnostic Approach Based on Available History
• TTF1 → to exclude primary lung adenocarcinoma
• p63 → to assess squamous differentiation
• TRPS1 → to evaluate possible breast origin
📋 Results
❌ TTF1 negative
❌ p63 negative
✅ TRPS1 patchy positive
⚠️ The Pitfall
With a history of breast carcinoma and a CK7 /TRPS1 profile, metastatic breast carcinoma seemed highly likely.
🔄 The Turning Point
• TRPS1 positivity was only patchy
• Additional clinical information was obtained
• Histologic correlation was performed
🧩 The Missing History
The patient also had a recently diagnosed endometrial malignancy with frozen pelvis and extensive local spread, a crucial piece of information that was not initially available.
🧬 Further Workup
✅ PAX8 positive - favor mullerian
❌ GATA3 negative - point against breast cancer
📌 Final Interpretation
Metastatic Müllerian carcinoma, with correlation favoring high-grade serous carcinoma.
💡 Take-Home Messages
✔️ TRPS1 is a useful marker, but not entirely specific for breast carcinoma.
✔️ Patchy TRPS1 positivity can be seen in Müllerian serous carcinomas and other non-mammary tumors.
✔️ Never interpret immunostains in isolation.
✔️ Morphology Clinical History Imaging Histology Correlation = Accurate Diagnosis.
✔️ Always question a result that does not perfectly fit the overall picture.
🏆 Lesson Learned
💎 The most important diagnostic tool in this case was not TRPS1—it was the missing clinical history.
#Cytopathology #PleuralFluid #DiagnosticPitfall #TRPS1 #BreastPathology #PathologyPearls #Cytology #ClinicopathologicCorrelation #PathTwitter #MedEd #LearningFromCases
3
7
24
916
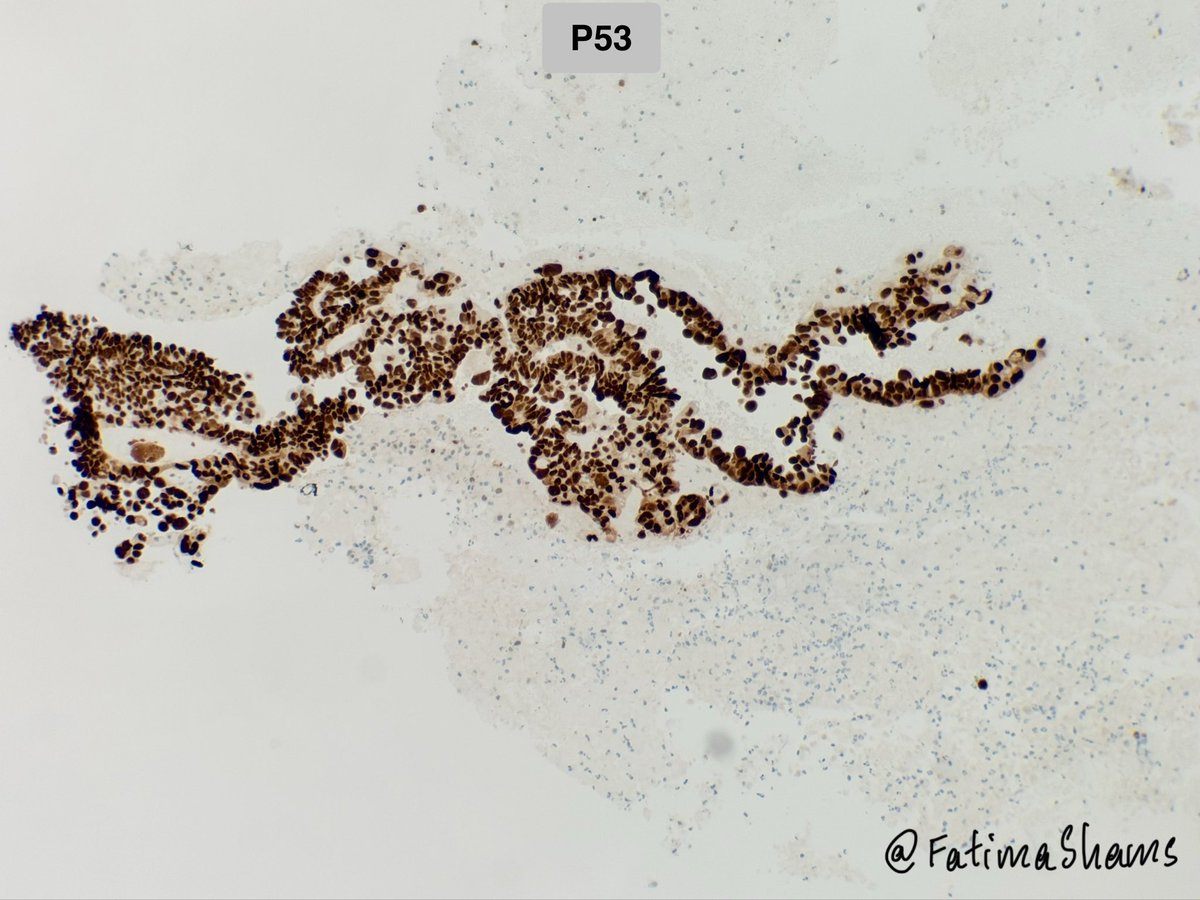
🔎 Histo-cyto correlation!
👉 74-year-old female with hematuria and bladder mass
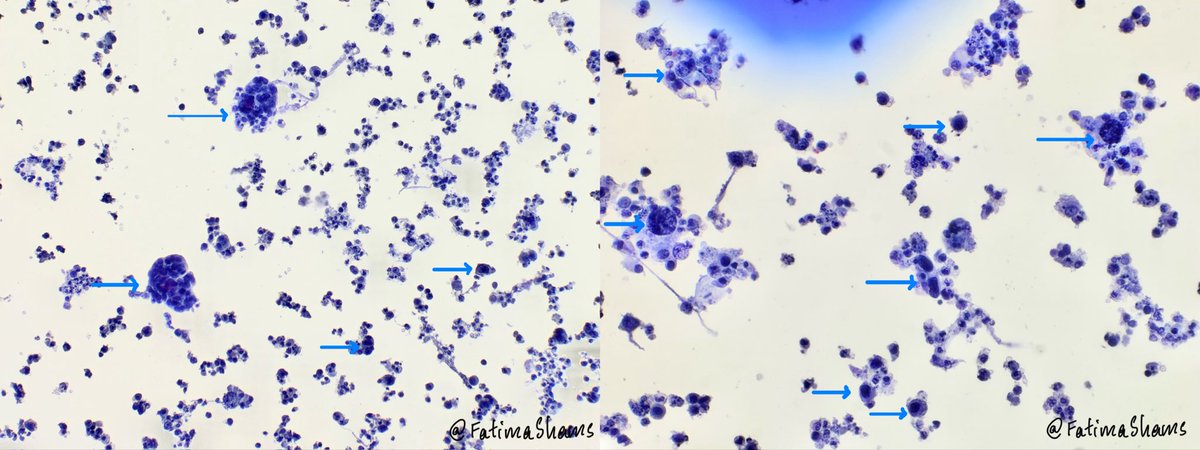
⚓️ Urine cytology showed features suspicious for High-Grade Urothelial Carcinoma (HGUC) with:
🔬 Hyperchromatic crowded cell clusters
🔬 Single scattered atypical cells
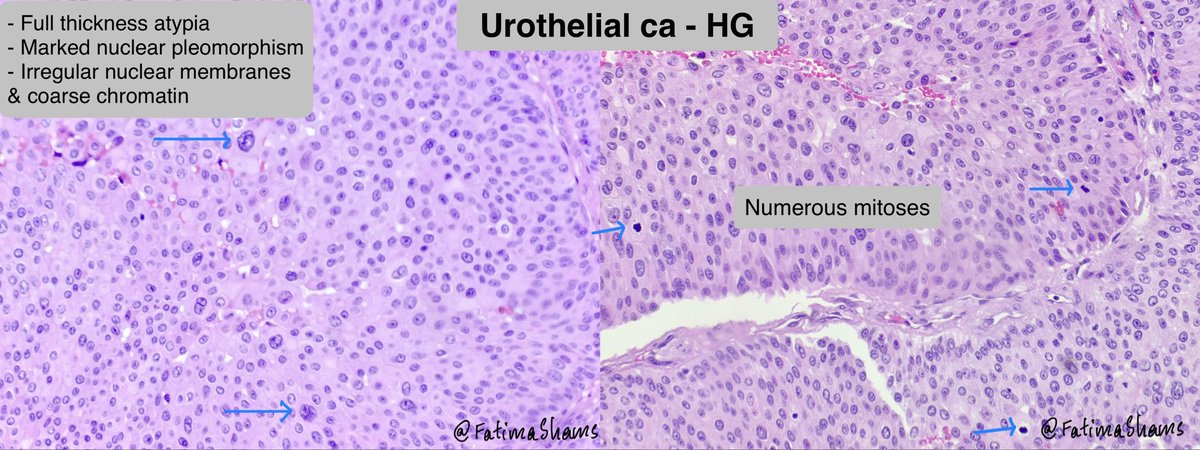
🔬 Marked pleomorphism, high N:C ratio
🔬 Irregular nuclear membranes & coarse chromatin
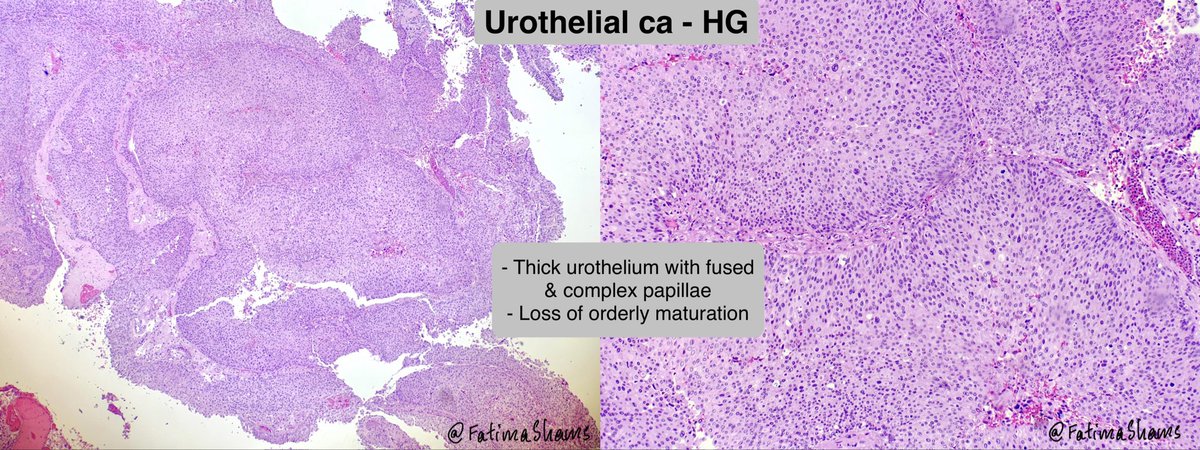
💎 Biopsy confirmed High-Grade Papillary Urothelial Carcinoma showing fused/complex papillae, loss of maturation, diffuse cytologic atypia, and numerous mitoses.
A nice histocytologic correlation case highlighting the importance of urine cytology in detecting HGUC.
#PathTwitter #Cytopathology #Uropath #Surgpath #UrineCytology #HGUC #UrothelialCarcinoma #Histopathology #MedEd #Pathology

11
36
1,368
🧵 Case: Histo–Cyto Correlation!
74-year-old female; Bladder biopsy and Urine cytology.
What is your diagnosis?
#PathTwitter #Cytopathology #UrineCytology #GUPath #Histopathology #Pathology #MedEd #Surgpath


2
4
15
1,002
Answer
👉 74-year-old female with hematuria and bladder mass
⚓️ Urine cytology showed features suspicious for High-Grade Urothelial Carcinoma (HGUC) with:
🔬 Hyperchromatic crowded cell clusters
🔬 Single scattered atypical cells
🔬 Marked pleomorphism, high N:C ratio
🔬 Irregular nuclear membranes & coarse chromatin
💎 Biopsy confirmed High-Grade Papillary Urothelial Carcinoma showing fused/complex papillae, loss of maturation, diffuse cytologic atypia, and numerous mitoses.
A nice histocytologic correlation case highlighting the importance of urine cytology in detecting HGUC.
#PathTwitter #Cytopathology #Uropath #Surgpath #UrineCytology #HGUC #UrothelialCarcinoma #Histopathology #MedEd #Pathology
33
👉 58-year-old male with a 5.5 cm left submandibular gland mass.
#PathTwitter #SurgPath #HeadNeckPath #SalivaryGlandPathology #SubmandibularGland #Pathology
Case courtesy @annsmiley78
1
5
16
733
What is your diagnosis and which IHC would support it?
0%
Pleomorphic adeno - PLAG1
20%
Schwannoma - SOX10
0%
Myoepithelioma - p63
80%
SFT - STAT6
5 votes • Final results
2
196
Answer provided here
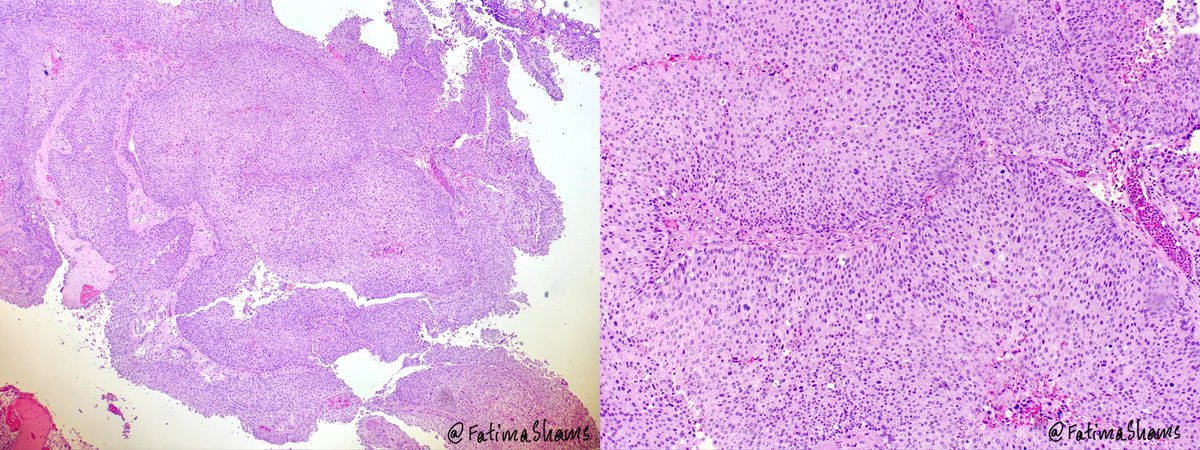
💎 Solitary Fibrous Tumor (SFT) involving the submandibular gland.
🔍 58-year-old male with a 5.5 cm left submandibular gland mass.
⚓️ Grossly, the lesion was a well-circumscribed, fleshy, firm white-tan mass with a solid whorled cut surface.
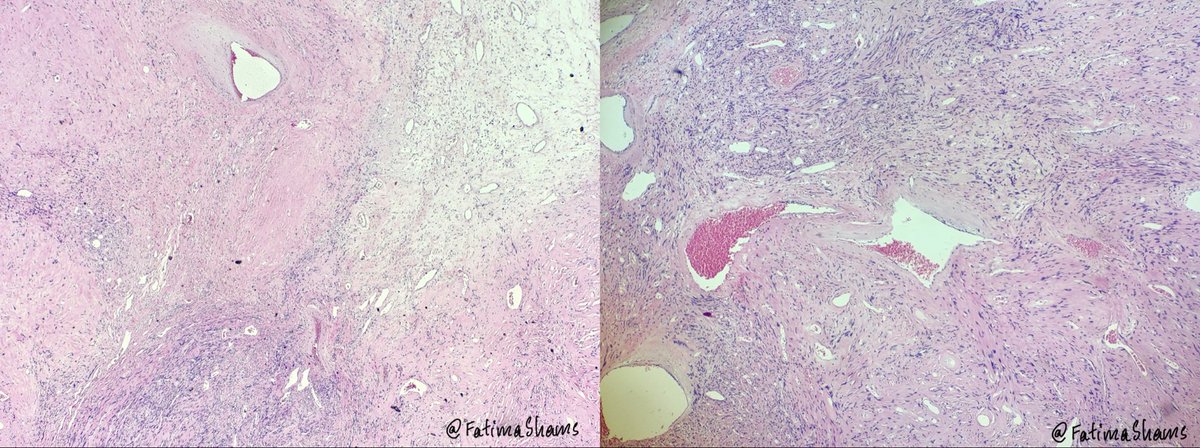
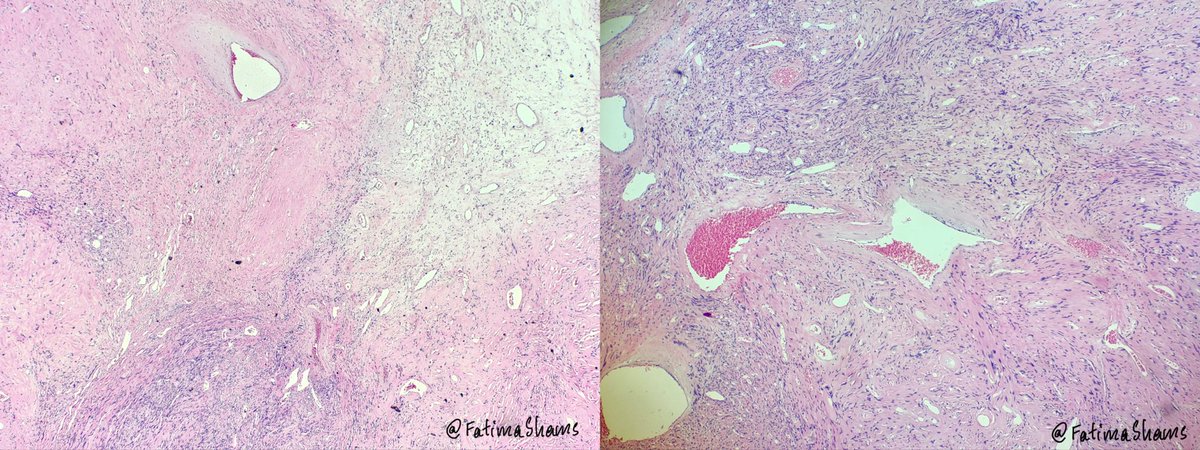
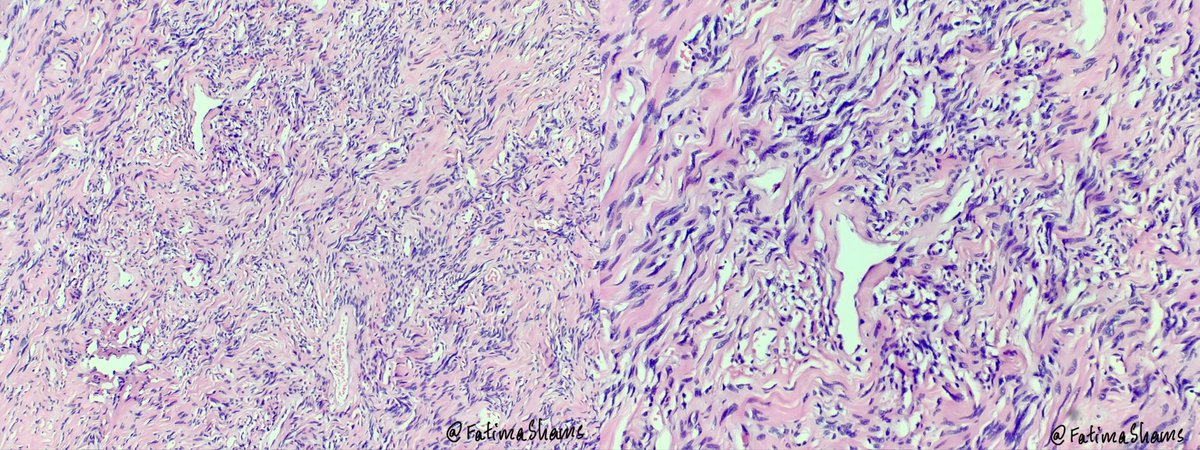
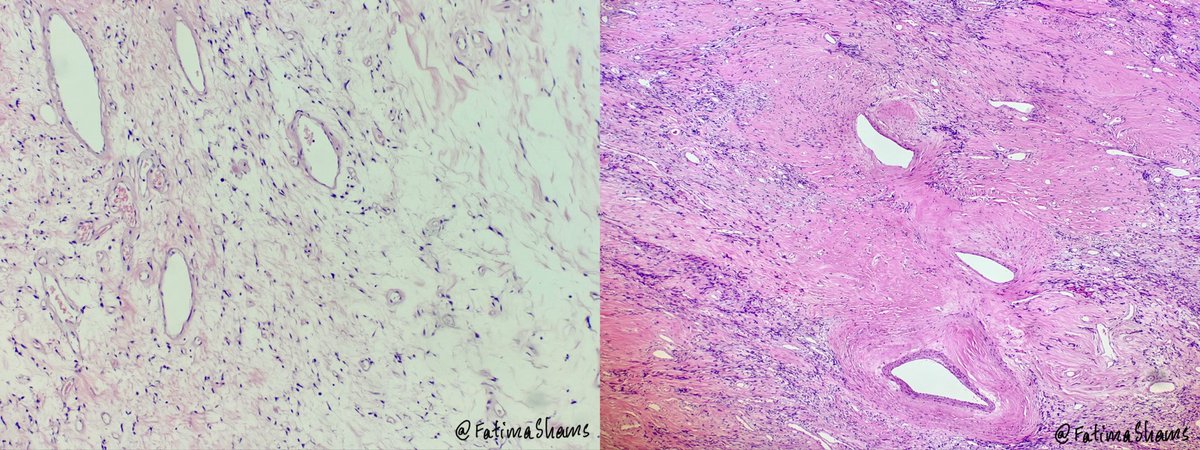
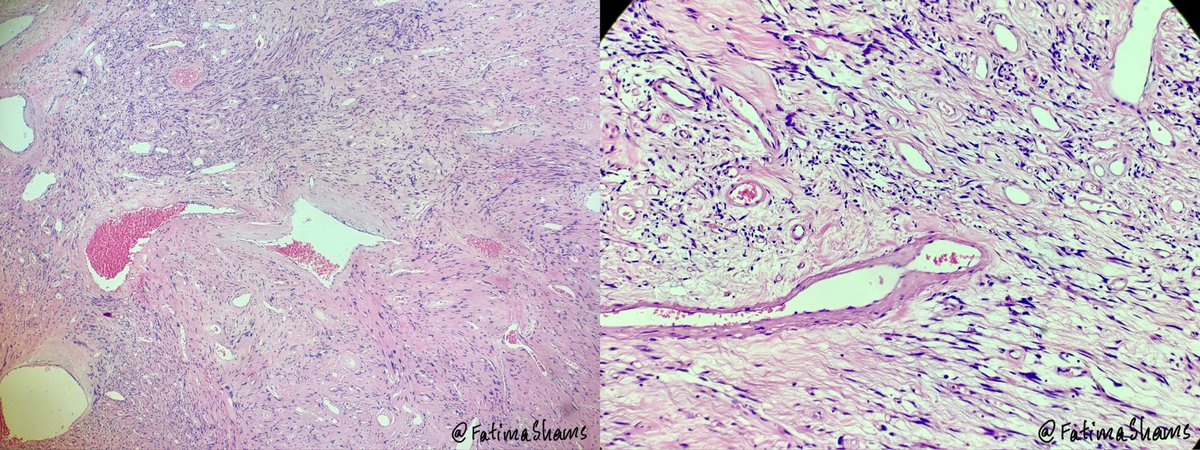
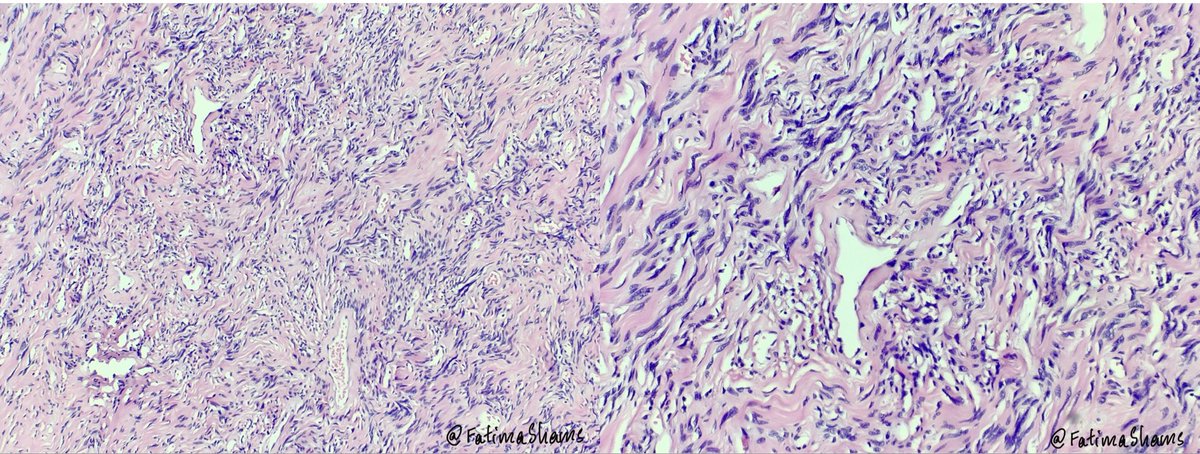
🔬 Microscopy showed a bland spindle cell neoplasm arranged in a “patternless pattern” with alternating hypo- and hypercellular areas, dense collagenized stroma, and prominent branching/staghorn-like vessels. Tumor cells showed minimal atypia and low mitotic activity.
🧪 IHC profile:
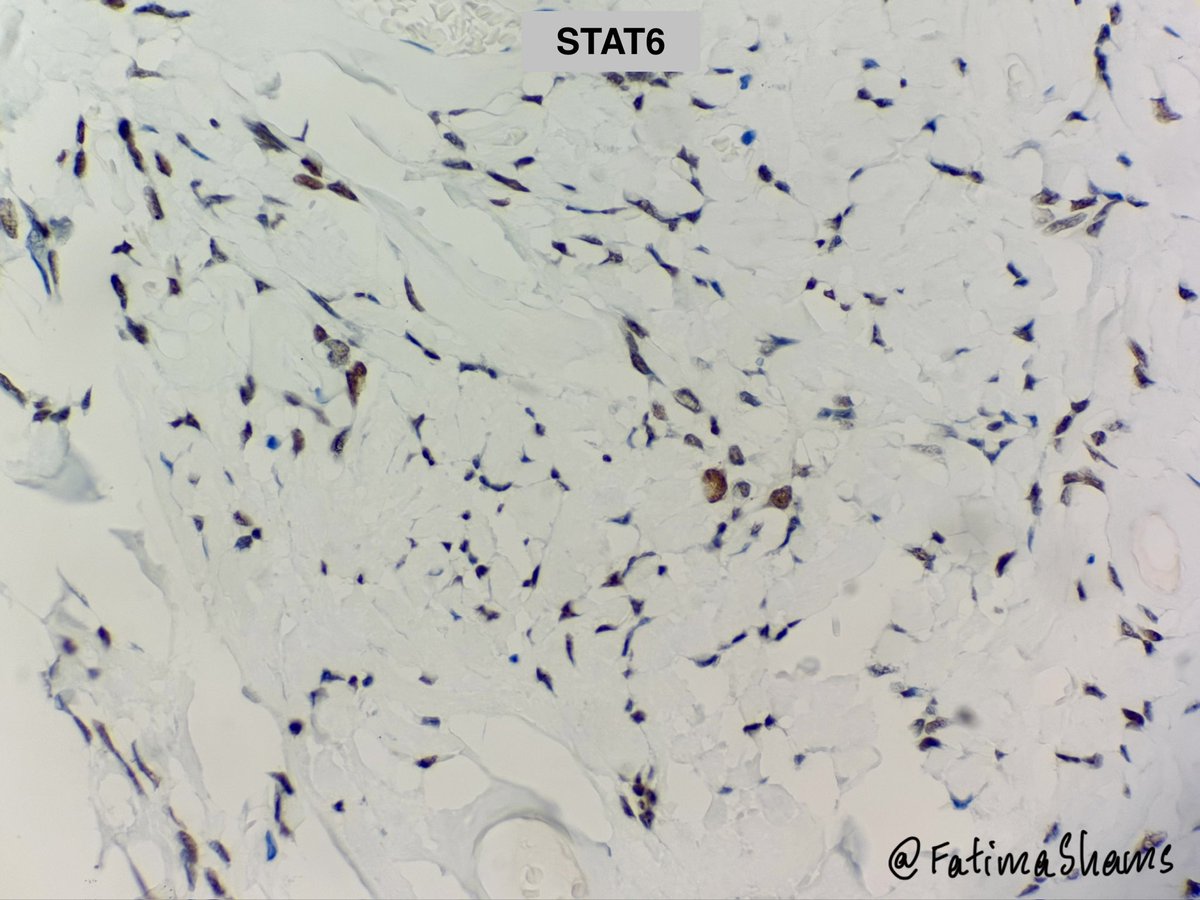
• STAT6 nuclear positive
•.CD34: diffuse positive
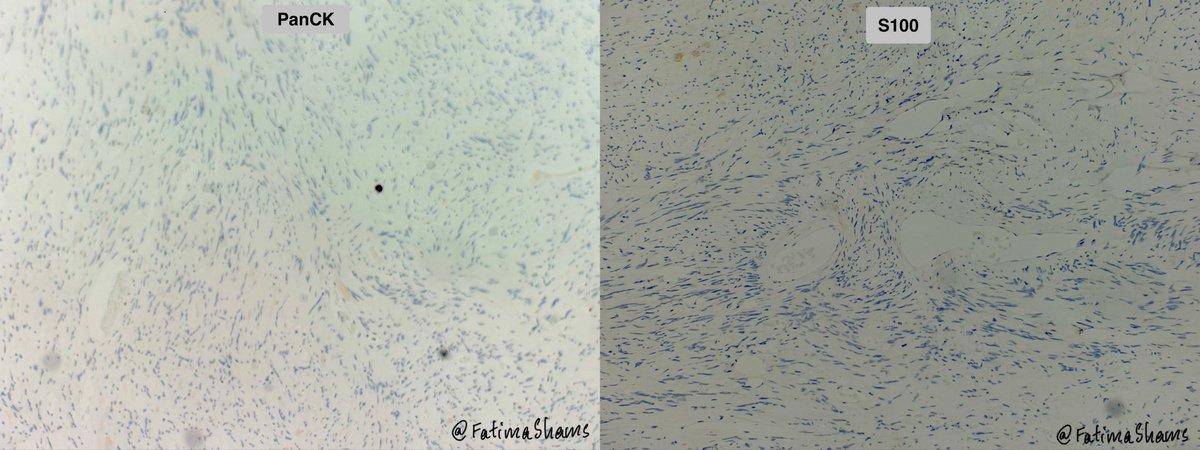
• PanCK & S100: negative
• SMA / Desmin: highlighted only vessel walls, negative in tumor cells
• Beta-catenin: cytoplasmic granular staining without nuclear positivity
💡 Key points:
• SFT is a rare mesenchymal neoplasm in salivary glands, most commonly affecting the submandibular gland and parotid.
• The characteristic molecular alteration is the NAB2::STAT6 fusion, resulting from inversion at chromosome 12q13 and leading to nuclear STAT6 expression which is highly sensitive and specific for SFT.
• Most SFTs behave indolently, but risk stratification depends on factors such as size, mitotic activity, necrosis, and patient age. Rare cases may recur or metastasize.
📚 Important morphologic clues favoring SFT:
✔ Patternless architecture
✔ Ropey collagen
✔ Staghorn vasculature
✔ Bland spindle cells
✔ Diffuse CD34 positivity & nuclear STAT6 positivity
Case courtesy @annsmiley78
#PathTwitter #SurgPath #HeadNeckPath #SalivaryGlandPathology #SoftTissuePathology #SolitaryFibrousTumor #SubmandibularGland #Histopathology #Pathology #MedEd
72
💎 Solitary Fibrous Tumor (SFT) involving the submandibular gland.
🔍 58-year-old male with a 5.5 cm left submandibular gland mass.
⚓️ Grossly, the lesion was a well-circumscribed, fleshy, firm white-tan mass with a solid whorled cut surface.
🔬 Microscopy showed a bland spindle cell neoplasm arranged in a “patternless pattern” with alternating hypo- and hypercellular areas, dense collagenized stroma, and prominent branching/staghorn-like vessels. Tumor cells showed minimal atypia and low mitotic activity.
🧪 IHC profile:
• STAT6 nuclear positive
•.CD34: diffuse positive
• PanCK & S100: negative
• SMA / Desmin: highlighted only vessel walls, negative in tumor cells
• Beta-catenin: cytoplasmic granular staining without nuclear positivity
💡 Key points:
• SFT is a rare mesenchymal neoplasm in salivary glands, most commonly affecting the submandibular gland and parotid.
• The characteristic molecular alteration is the NAB2::STAT6 fusion, resulting from inversion at chromosome 12q13 and leading to nuclear STAT6 expression which is highly sensitive and specific for SFT.
• Most SFTs behave indolently, but risk stratification depends on factors such as size, mitotic activity, necrosis, and patient age. Rare cases may recur or metastasize.
📚 Important morphologic clues favoring SFT:
✔ Patternless architecture
✔ Ropey collagen
✔ Staghorn vasculature
✔ Bland spindle cells
✔ Diffuse CD34 positivity & nuclear STAT6 positivity
Case courtesy @annsmiley78
#PathTwitter #SurgPath #HeadNeckPath #SalivaryGlandPathology #SoftTissuePathology #SolitaryFibrousTumor #SubmandibularGland #Histopathology #Pathology #MedEd
1
5
22
819



CYTOLOGY.
👉 83 YO male with pleural effusion.
Negative IHCs: CK20, Calretinin
#PathTwitter #Cytopathology #Cytology #PleuralFluid #EffusionCytology #SurgPath #Pathology
2
6
12
999
Diagnosis….Mets from?
12%
Lung
12%
SCC
8%
Upper GI/pancreatobiliary
68%
Urothelial
25 votes • Final results
2
174
Detailed answer provided here
Pleural fluid CYTOLOGY.
📌 Clinical: Male patient with known urothelial carcinoma of bladder with metastases to lung, chest wall, and bone, presenting with pleural effusion.
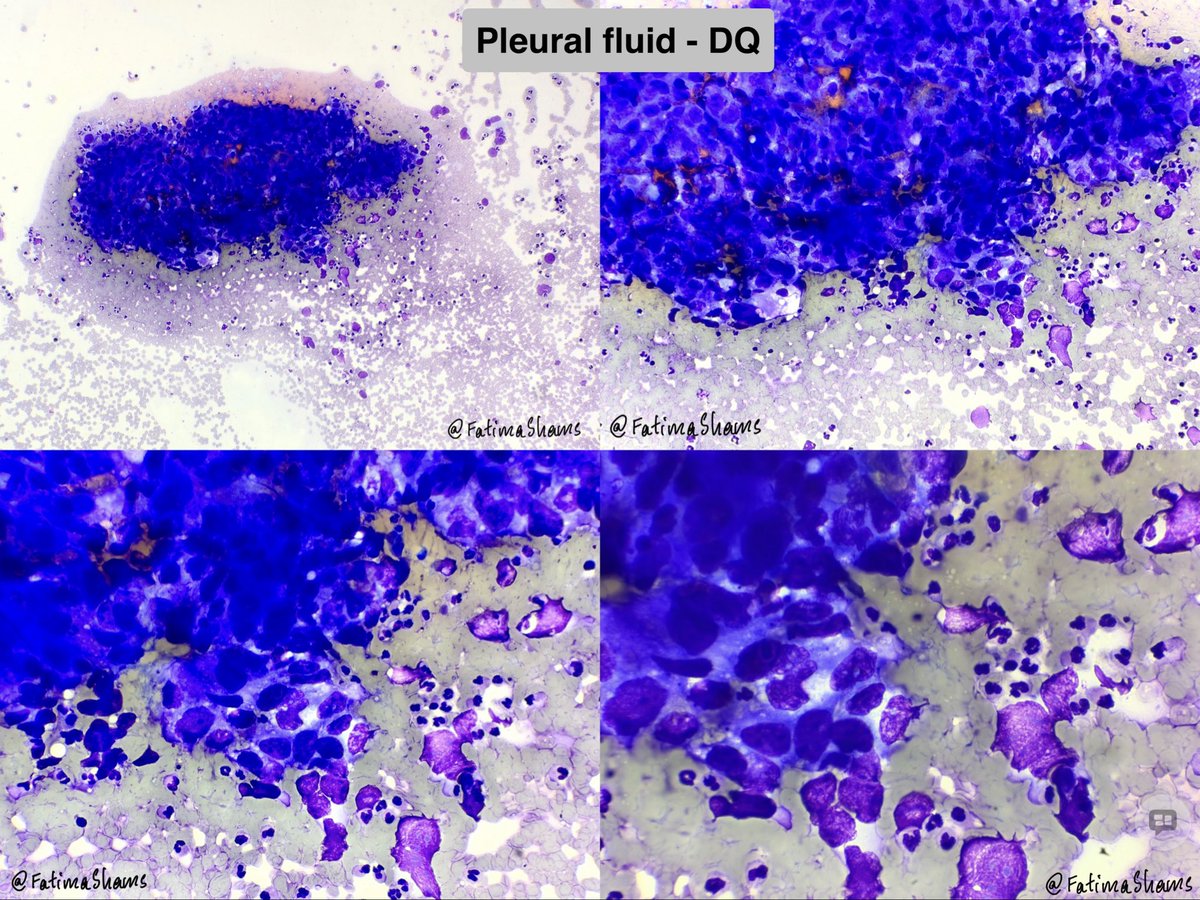
🔬 Cytology (Pap & DQ):
•Moderate cellularity
•Clusters and sheets of atypical epithelial cells in a hemorrhagic background
•Cells show high N:C ratio, nuclear irregularity, coarse chromatin, and prominent nucleoli
•No definite gland formation
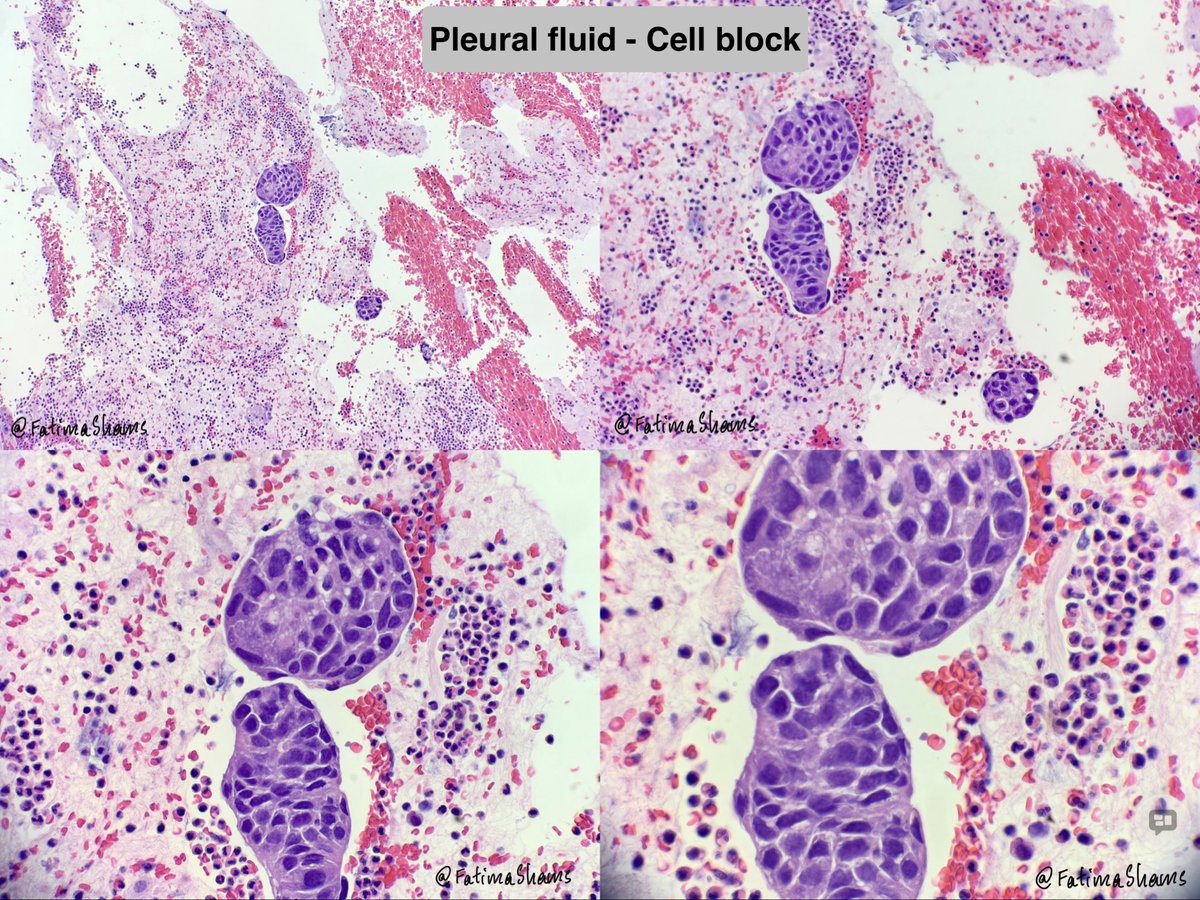
🧫 Cell block:
•Cohesive clusters of malignant epithelial cells with similar morphology
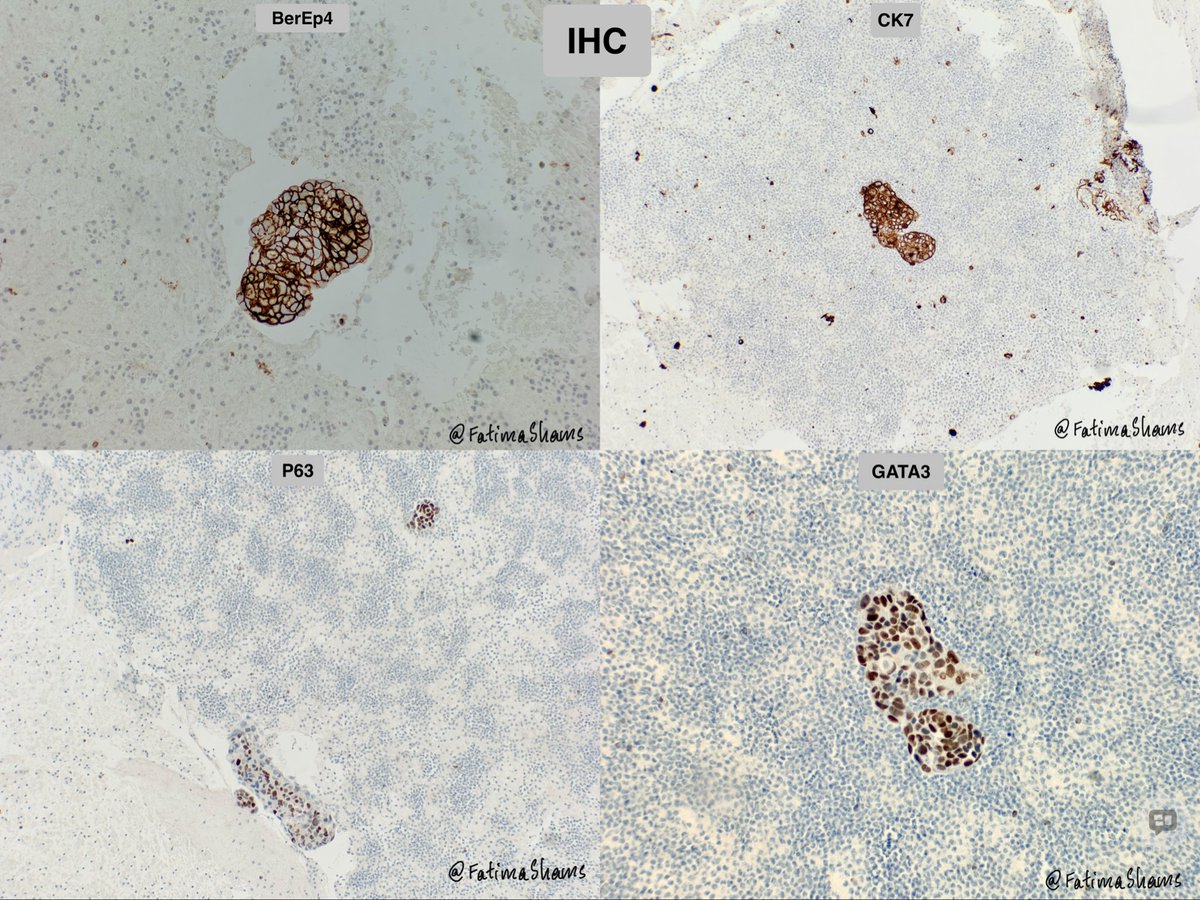
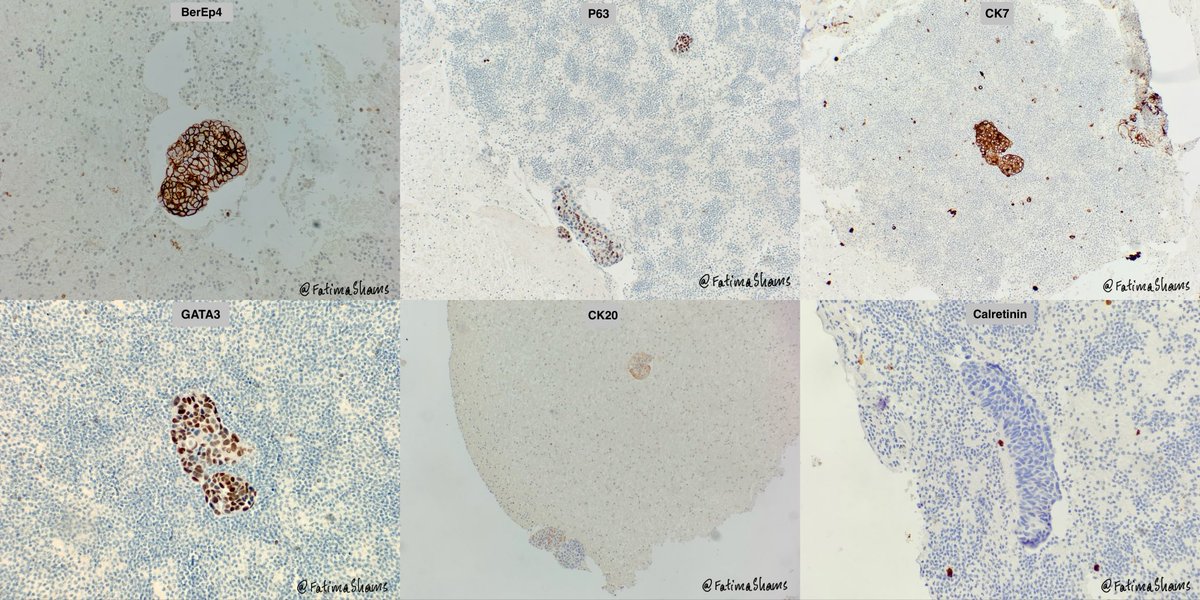
🧪 IHC:
•BerEP4 , CK7
•GATA3 , p63
•CK20: focal weak
•Calretinin– (excludes mesothelial origin)
🔹 Diagnosis: Malignant effusion – metastatic carcinoma consistent with urothelial origin
🔹 Teaching points 💡
✔️ GATA3 p63 co-expression → strong clue to urothelial carcinoma
✔️ In pleural effusion, always differentiate from lung adenocarcinoma & squamous carcinoma
✔️ BerEP4 / Calretinin –ve → epithelial, not mesothelial
✔️ CK20 may be variable/focal in urothelial carcinoma
#PathTwitter #Cytopathology #PleuralFluid #EffusionCytology #UrothelialCarcinoma #MetastaticCarcinoma #DiagnosticPathology
1
88
Pleural fluid CYTOLOGY.
📌 Clinical: Male patient with known urothelial carcinoma of bladder with metastases to lung, chest wall, and bone, presenting with pleural effusion.
🔬 Cytology (Pap & DQ):
•Moderate cellularity
•Clusters and sheets of atypical epithelial cells in a hemorrhagic background
•Cells show high N:C ratio, nuclear irregularity, coarse chromatin, and prominent nucleoli
•No definite gland formation
🧫 Cell block:
•Cohesive clusters of malignant epithelial cells with similar morphology
🧪 IHC:
•BerEP4 , CK7
•GATA3 , p63
•CK20: focal weak
•Calretinin– (excludes mesothelial origin)
🔹 Diagnosis: Malignant effusion – metastatic carcinoma consistent with urothelial origin
🔹 Teaching points 💡
✔️ GATA3 p63 co-expression → strong clue to urothelial carcinoma
✔️ In pleural effusion, always differentiate from lung adenocarcinoma & squamous carcinoma
✔️ BerEP4 / Calretinin –ve → epithelial, not mesothelial
✔️ CK20 may be variable/focal in urothelial carcinoma
#PathTwitter #Cytopathology #PleuralFluid #EffusionCytology #UrothelialCarcinoma #MetastaticCarcinoma #DiagnosticPathology
1
6
20
847