
GI & HPB Surgical Oncologist @apollo_ahd @scrc_clinic📍 Ahmedabad, 🇮🇳
Joined July 2018
- Tweets 1,742
- Following 62
- Followers 954
- Likes 1
1,297 Photos and videos








Jun 12
🤖 Robotic vs laparoscopic TME for mid/low rectal cancer.
Randomised trials only this time — 4 RCTs, 1,952 patients.
The pathology favours robotics:
📉 CRM positivity down (OR 0.58), complete mesorectum up (OR 1.55), conversion down (OR 0.41).
Early morbidity: no difference.
And the part to watch — 2 trials with 3-year data:
📉 lower locoregional recurrence (OR 0.43), a slight DFS edge (HR 0.78). OS unchanged.
Robotics doesn't change survival, but it makes a hard operation more reproducibly complete — and the oncology signal is finally starting to show.
doi.org/10.1007/s11701-026-0…
#RoboticSurgery #RectalCancer
22
Jun 11
💊 FGFR2-rearranged cholangiocarcinoma, first line.
Pemigatinib vs gem/cis. The response data are real.
🎯 ORR 47% vs 15%. PFS 8.3 vs 6.8 months, HR 0.58. Duration of response more than doubled.
And yet:
⚠️ overall survival was flat. 24.4 vs 25.0 months.
Why? Crossover. The chemo arm got pemigatinib later and caught up.
The lesson isn't that the drug fails — it's that moving an effective drug earlier doesn't buy survival when everyone gets it eventually.
First-line pemigatinib is for the patient who needs the response now.
doi.org/10.1200/JCO-26-00788
#JCO #Cholangiocarcinoma
32
Jun 10
🧬 BRAF V600E metastatic colorectal cancer. First line.
The original BREAKWATER paired encorafenib cetuximab with FOLFOX.
Cohort 3 pairs it with FOLFIRI — and it holds.
147 patients vs FOLFIRI ± bevacizumab.
🎯 Response rate 64% vs 39%.
📈 Median PFS 15.2 vs 8.3 months. HR 0.44.
OS prolonged too — HR 0.56.
So the backbone is now a choice, not a constraint: irinotecan or oxaliplatin, decided on toxicity.
BRAF V600E mCRC is firmly a first-line targeted-therapy disease.
doi.org/10.1016/j.annonc.202…
#AnnalsofOncology #ColorectalCancer
46
🧪 Resectable, PD-L1-positive gastric/GEJ cancer.
Add a PD-1 inhibitor across the perioperative window?
ASTRUM-006 says yes — and trims the adjuvant chemo.
Neoadjuvant serplulimab SOX → adjuvant serplulimab, vs placebo SOX → adjuvant SOX. 588 patients.
📈 EFS at CPS ≥10: not reached vs 42 months. HR 0.65.
ITT (CPS ≥5): HR 0.73.
The adjuvant half is immunotherapy alone — chemo-sparing.
⚠️ And grade ≥3 toxicity was lower, not higher: 47% vs 59%.
OS still immature. But the perioperative case keeps building.
doi.org/10.1016/S0140-6736(2…
#TheLancet #GastricCancer
1
3
158
🧪 Second-line metastatic pancreatic cancer.
For years the honest answer was: more chemo, very little gained.
RASolute 302 changes the sentence.
Daraxonrasib — a pan-RAS(ON) inhibitor — vs investigator's-choice chemo. 500 patients, 92% RAS G12.
📈 Median OS 13.2 vs 6.6 months. HR 0.40.
PFS 7.3 vs 3.5 months.
And it was the better-tolerated arm:
⚠️ grade ≥3 events 62% vs 70%, discontinuations 1.2% vs 11%.
A HR of 0.40 in pretreated PDAC is a number this field has basically never produced.
doi.org/10.1056/NEJMoa260555…
#NEJM #PancreaticCancer
81
🔬 Intrahepatic cholangiocarcinoma. Who actually benefits from adjuvant therapy?
Maybe three stains can tell you.
Multi-omics found a high-risk, mucin-enriched subtype.
Marked by claudin-18, MUC1, MUC5AC.
Worst survival when left untreated.
📈 But in 174 resected patients, the marker-positive ones did markedly better with adjuvant chemo or chemoembolisation.
Marker-negative: no clear benefit.
💡 A small IHC panel to decide who to treat after resection. Needs prospective validation.
And claudin-18 keeps showing up across the biliary tree.
doi.org/10.1016/j.modpat.202…
#Cholangiocarcinoma
1
5
146
🤖 Robotic vs laparoscopic gastrectomy. Japan's national registry. 2023–24.
Nearly 11,000 matched pairs.
Distal gastrectomy:
📉 Lower 30-day morbidity, robotic vs lap. 4.3% vs 4.9%.
Less blood loss, fewer conversions, shorter stay.
Total gastrectomy:
Morbidity the same. 8.7% vs 8.3%.
Robotic still bled less and converted less — but didn't move the main endpoint.
💡 The robotic edge in gastric cancer is real, but it's procedure-specific.
Long-term oncology and cost still open.
doi.org/10.1007/s10120-026-0…
#GastricCancer
2
144
🧠 A "low-risk" pancreatic cyst. Stable for years.
Safe to stop watching?
1,494 IPMNs under surveillance vs the SEER population:
📈 ~10x the pancreatic cancer risk overall.
Main duct ≥5 mm: 26x. BMI ≥30: 21x.
Here is the part that matters:
Even guideline-negative cysts ran 8x the risk.
After 5 stable years, the curve kept climbing. No plateau.
⚠️ "Low-risk" is not "no-risk." And year 5 is not a finish line.
doi.org/10.1097/SLA.00000000…
#AnnalsofSurgery
3
71
🩺 Oesophageal cancer.
Restaging after chemoradiation comes back "uncertain."
Watch, or operate?
SANO looked at 272 uncertain responders. 205 went to surgery.
Only 15% had no residual tumour.
So 85% still had cancer. 🎯
"Uncertain" is not "complete." Default to surgery.
One exception: squamous cancer a non-traversable stricture.
There, 33% had a pathologic complete response.
That subgroup earns a real conversation — not a reflex resection.
doi.org/10.1097/SLA.00000000…
#AnnalsofSurgery
1
38
🧪 HER2-positive gastroesophageal cancer, first line.
For 15 years the answer was trastuzumab chemo.
HERIZON-GEA-01 says that can change.
Zanidatamab is a dual-HER2 bispecific.
It beat trastuzumab on PFS. HR 0.65.
📈 Add tislelizumab and median OS reaches 26.4 months. HR for death 0.72.
The catch: the survival win needs the PD-1.
Zanidatamab alone — OS 24.4 months, not significant.
⚠️ And grade ≥3 toxicity ~73%. Diarrhoea in a quarter.
Real gain. Real toxicity. Pick the patient.
doi.org/10.1056/NEJMoa251772…
#NEJM #GastricCancer
2
128
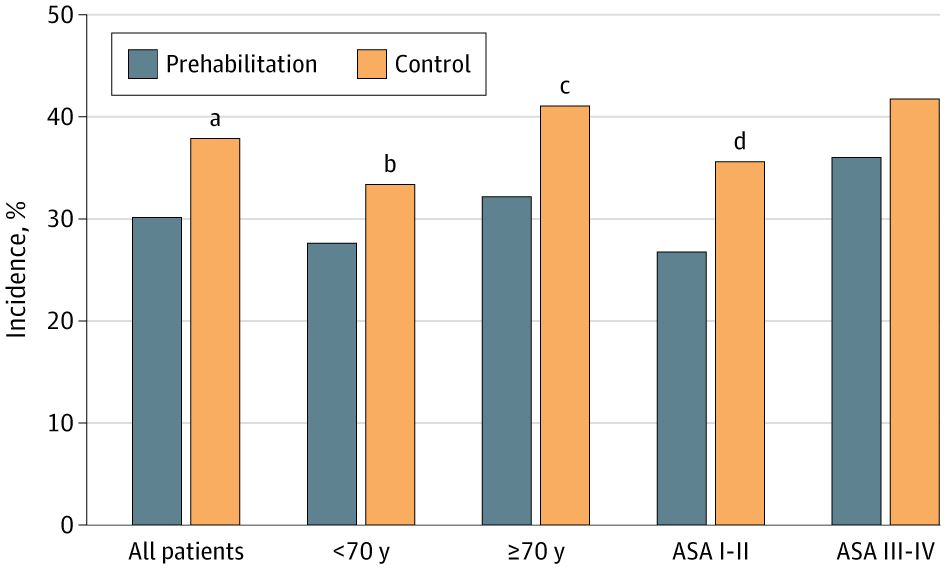
May 29
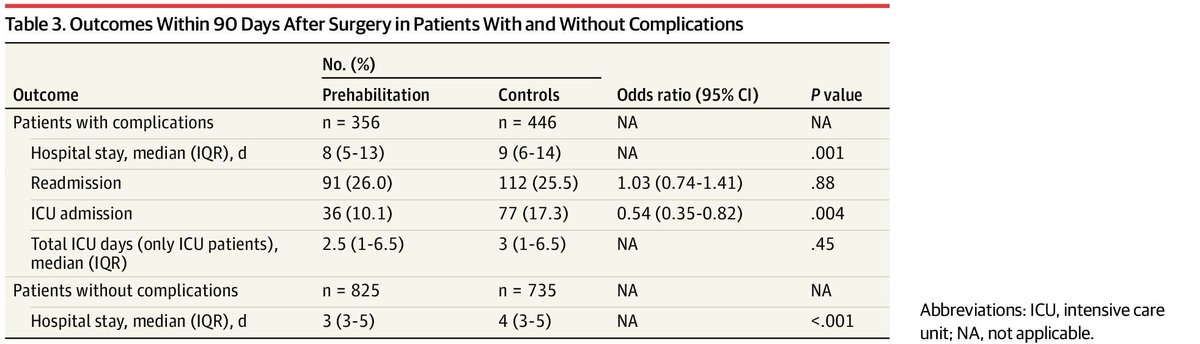
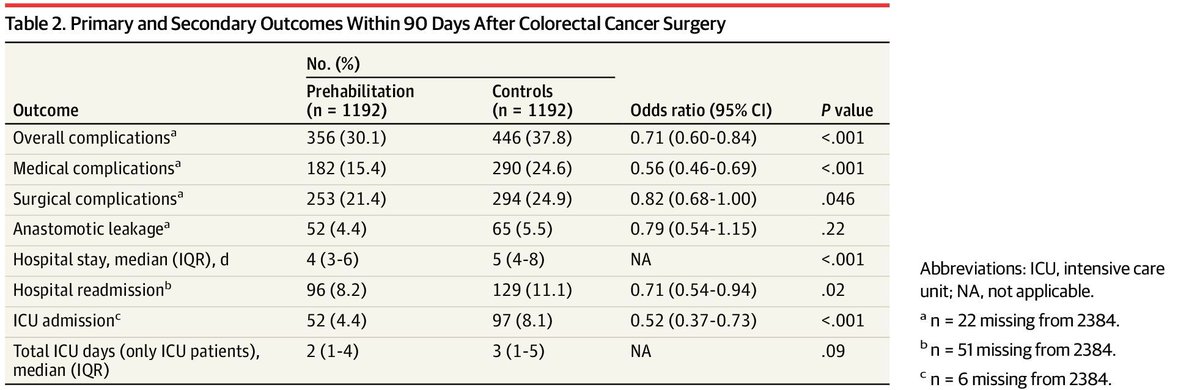
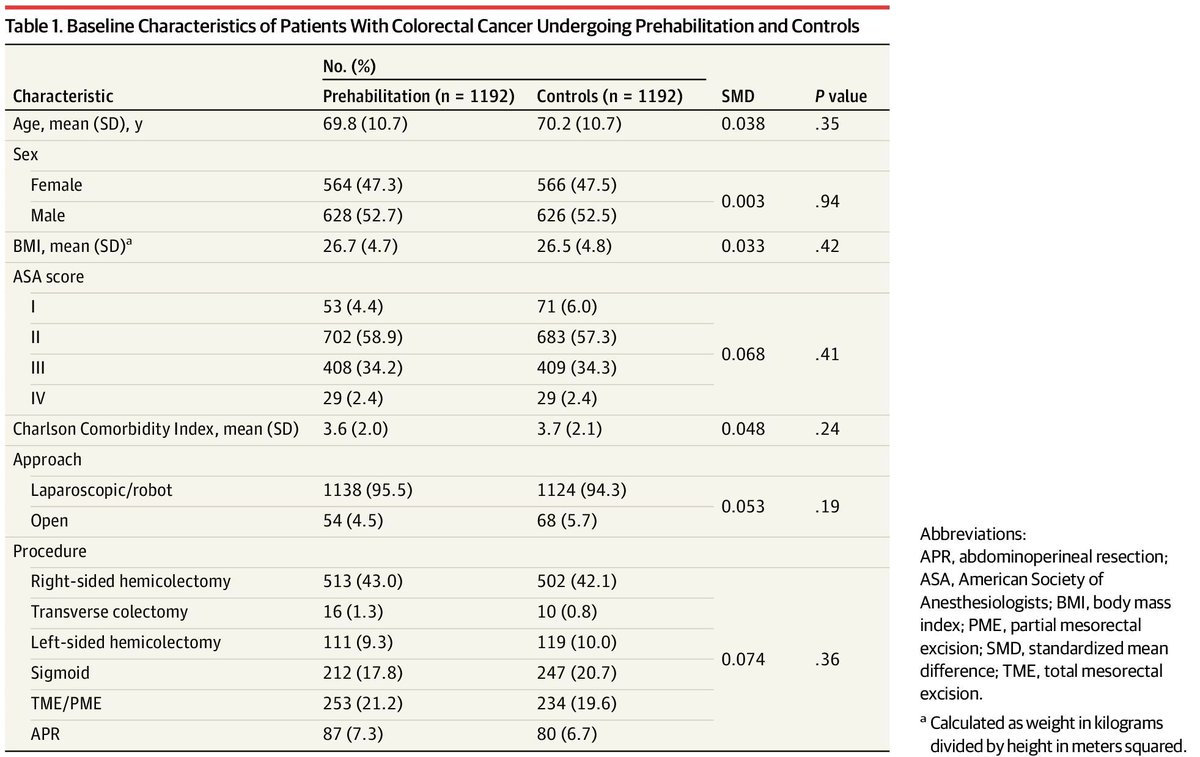
Nationwide Dutch data (18 hospitals, 2,384 patients): multimodal prehabilitation before colorectal cancer surgery cut overall complications from 37.8% to 30.1% (OR 0.71), nearly halved medical complications, and shaved a day off length of stay — across every age and ASA grade.
The complication you prevent in clinic is the one you don't fight in the ICU.
doi.org/10.1001/jamasurg.202…
#JAMASurgery
1
2
128
May 28
Intraoperative AI that flags the pancreas, common hepatic artery, left gastric artery and vein during robotic gastrectomy cut unsafe incision-line choices (OR 0.25) and found the hepatic artery faster — across 67 videos and 20 surgeons.
Vessel recognition is still modest. A cognitive aid for suprapancreatic dissection, not an autopilot.
doi.org/10.1007/s10120-026-0…
#GastricCancer
1
2
114
May 27
RESPONDER (n=844, 8 centres): in rectal cancer, when lateral pelvic nodes ≥5 mm shrink to under 5 mm after chemoradiation, omitting lateral node dissection gave the same 5-year local recurrence (5.3% vs 3.1%) and disease-free survival — with less operative morbidity.
The response carries the prognosis. Dissect the node that doesn't shrink; spare the one that does.
doi.org/10.1097/SLA.00000000…
#AnnalsofSurgery
1
68
May 26
Tissue-free ctDNA in stage III colon cancer, validated in 2,260 patients from Alliance N0147.
Detectable after surgery in 1 in 5. Recurrence HR ~6. Five-year disease-free survival 27.7% if positive vs 77.1% if negative — and the gap was widest in the lower-risk and dMMR patients we're least certain about.
No tumour block required. Clearly prognostic now; whether acting on it improves outcomes is the next trial.
doi.org/10.1200/JCO-25-02086
#JCO
1
63
May 25
DRAGON-01 (phase 3, n=222, gastric cancer with peritoneal-only metastasis): adding intraperitoneal to IV paclitaxel S-1 improved median OS from 13.9 to 19.4 months (HR 0.67), and 3-year OS from 12% to 25%.
Conversion surgery 51% vs 35%; positive cytology cleared in 84% vs 53%. No extra grade 3–4 toxicity.
First positive phase 3 for intraperitoneal chemo here — PHOENIX-GC was negative. The backbone predates chemo-immunotherapy, so integration is the next question.
doi.org/10.1001/jamaoncol.20…
#JAMAOncology
2
356
May 22
MATTERHORN final OS: durvalumab FLOT beats FLOT alone in resectable G/GEJ. HR 0.78; p=0.021.
🎯 The first checkpoint regimen to move OS in this curative-intent setting. KEYNOTE-585 couldn't.
doi.org/10.1056/NEJMoa250370…
1
68
May 20
One dose of pembrolizumab. 44% pCR in stage I–III dMMR colon cancer. RESET-C in JCO.
💡 The non-operative-management trial design writes itself from here.
doi.org/10.1200/JCO-25-02274
1
80
May 18
NORDICC, 13-year follow-up.
Distal CRC: RR 0.79.
Proximal CRC: RR 0.91, not significant.
⚠️ The right colon remains the screening problem nobody has solved.
doi.org/10.1016/S0140-6736(2…
81
May 12
A 2026 community study mapped gallstone disease across India in 28,395 people.
The geographic difference is 35-fold.
Five things every Indian adult should know — all backed by data published this year.
🧵
1
97
May 12
5/ When to act:
— Pain after fatty meals
— Right upper abdomen tenderness
— Yellow eyes/skin
— Fever chills abdominal pain
These are not "gas." Get an ultrasound.
In high-risk regions, even silent stones deserve a surgical conversation.
1
149
May 12
Sources (peer-reviewed, 2024–2026):
— Mohite et al, BMJ Public Health 2026: doi.org/10.1136/bmjph-2025-0…
— Gupta et al, JGH Open 2026: doi.org/10.1002/jgh3.70380
— Parveen et al, Indian J Gastroenterol 2024: doi.org/10.1007/s12664-023-0…
56