
Joined August 2020
- Tweets 2,797
- Following 2,747
- Followers 3,385
- Likes 4,351
234 Photos and videos











Pinned Tweet

28 Apr 2024
You have to be always drunk. That's all there is to it; it's the only way. So as not to feel the horrible burden of time that breaks your back and bends you to the earth, you have to be continually drunk.
But on what? Wine, poetry or virtue, as you wish. But be drunk
Baudelaire
26
6,679
Morocco played better.
That said, you and Laura are now blacklisted.

I don’t know if @ASkarbnik will talk to me anymore once I admit I want Morocco to win this evening @FIFAcom @FIFAWorldCup
At least @GuiperiniMD will understand,
@iHematologo @HemSandoval @Dr_AmerZeidan @laura_korin @karima_oualla @NaglaAKarimMD
4
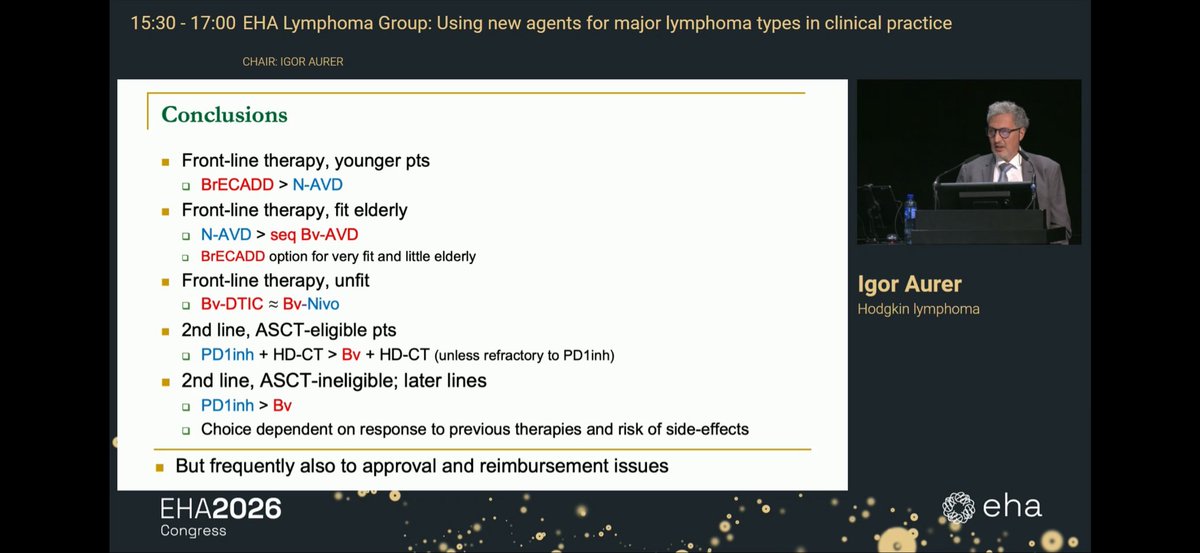
This is crazy.
There is truly no data to favor BreCADD over N-AVD.
A lot of countries have zero experience with BEACOPP plataform.
At least BRECADD should be = Nivo-AVD.

7
6
48
4,802
Jun 12
Thanks for so many friends cheering for me.
It was truly special.

Excelente presentación!!
Felicitaciones @GuiperiniMD !
Muy feliz de ver a un investigador de LATAM como primer autor en una sesión tan destacada. 👏🌎 #EHA2026
3
5
36
2,167
Jun 10
The most iconic solo of all times.

And at #IMFIMWG26, Mr. New York takes on “Hotel California”…
And not just crushes it, he knocks it to MRD neg at 10^-8 in 30 seconds 👏
Bravo @JoshuaRichterMD for 🎸 performance of the year!
2
7
1,794
One of the most relevant Lymphoma meetings (I go every year), @LymphomaEx has also a session where we discuss new data and how it should be applied in LatAm.
It is not an easy task: therapies are far from being ZipCode-Agnostic. So, in a 4 hour session, we discuss with multiple experts from different regions how we should approach these therapies.
The result is our LexAct. And it is open to discussion for everybody now.
I am already confirmed in 2027! Join me in beautiful Puerto Varas for great science, amazing wine and late-night lakeside Karaoke.
lexmeet.org/lexact-2026
3
4
20
1,886
Btw, I read it on Twitter the term zipcode-agnostic and I loved it. Cant remember who said it to give credit due. But if someone reclaim it, I will gladly do it. Perfect term!
2
5
379
Interesting.
Some GCB may eventually benefit from Tafa Len? But who?
Jun 3

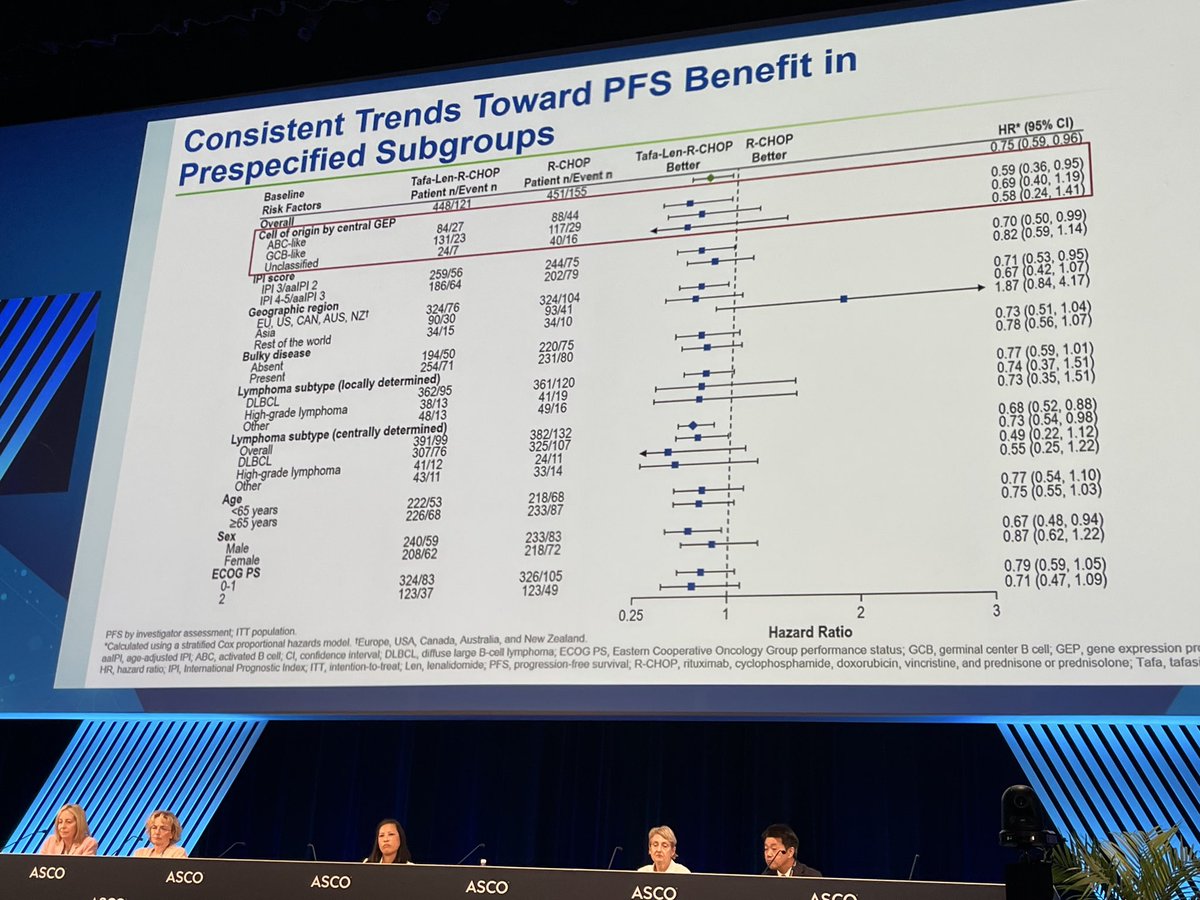
Striking difference in cell-of-origin effect between
POLARIX trial (PolaRCHP vs RCHOP) and
frontMIND trial (tafa-len-RCHOP vs RCHOP)
In POLARIX, zero benefit to GCB pts, and significant heterogeneity by COO
frontMIND does not show statistically significant heterogeneity

2
7
1,643
Lonca-R is superior to R-GEMOX.
ir.adctherapeutics.com/2026-…
3
27
2,106
It was amazing!
Congrats, my dear friends!
Cerramos la serie LATAM de @WomenInLymphoma, coronando este ciclo con una inspiradora sesión sobre Linfoma de Hodgkin.
Un honor haber coorganizado este webinar junto a un grupo excepcional de colegas. ¡Gracias a todos los participantes! #WomenInLymphoma

1
11
748
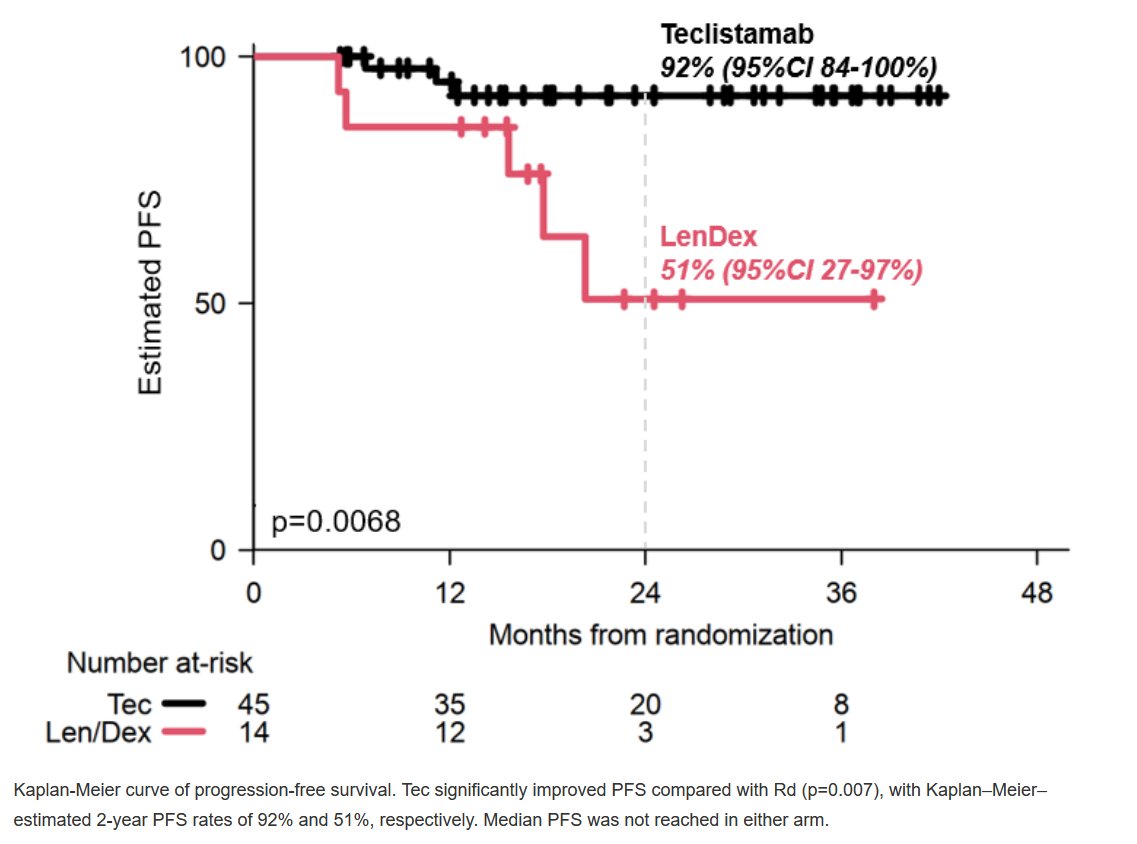
Amazing results.
We may avoid a full blown cancer with 12 months of teclistamab.
I know what my friend @Papa_Heme
will say about it, but this might be a game changer if longer follow up maintains the benefit.

TECLISTAMAB IMPROVES DEPTH OF RESPONSE AND PFS VERSUS LENALIDOMIDE-DEXAMETHASONE IN HIGH-RISK SMOLDERING MULTIPLE MYELOMA library.ehaweb.org/eha/2026/… #mmsm #EHA26
4
7
43
9,589
Very well balanced take on FrontMind and Polarix.
My call is: molecular stratification. We need to identify which mutations will respond to each drug better.
Probably Polarix for C5/MCD.
TafaLen R-CHOP for others.
We cannot add $$$$$ for all if benefit is for few.

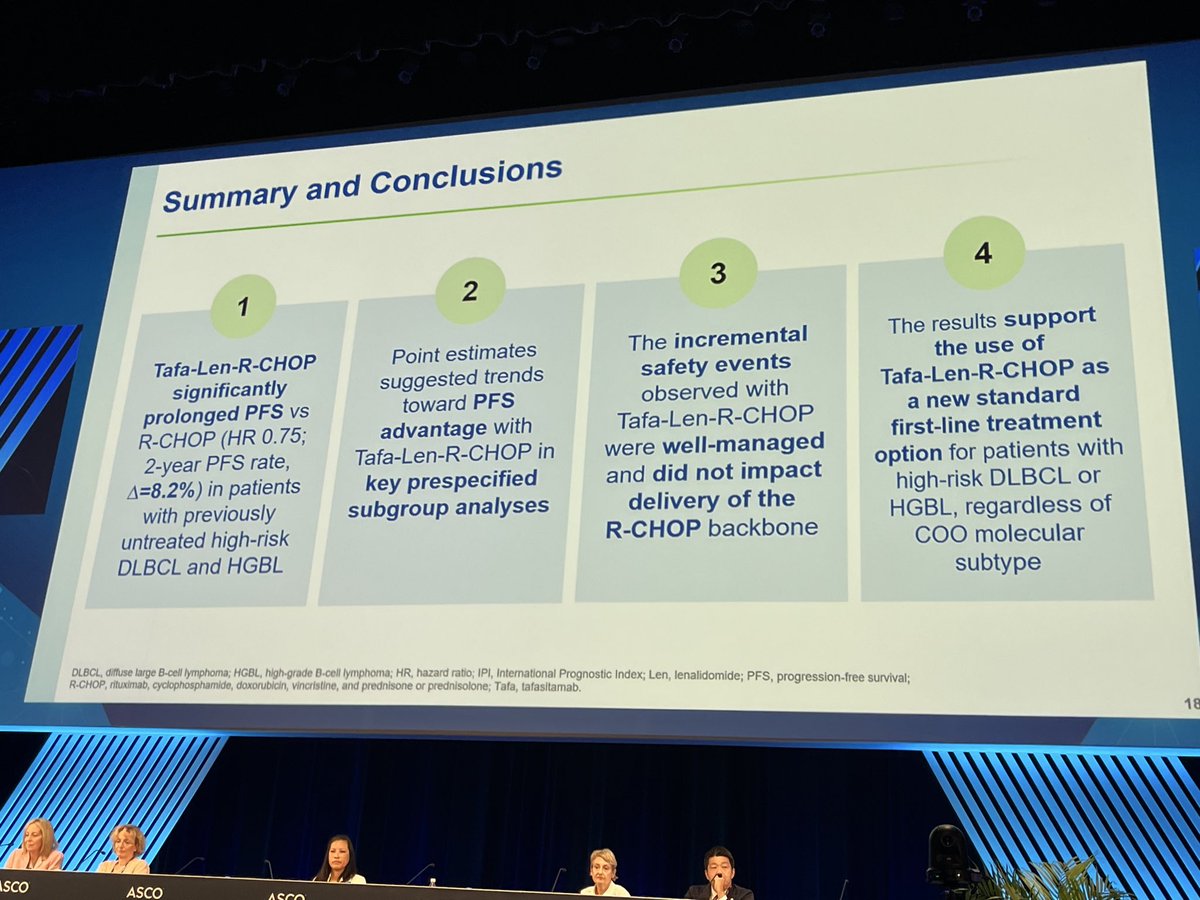
frontMIND: a new first-line regimen for high-risk DLBCL?
The phase III frontMIND trial (Lenz et al., Lancet) adds tafasitamab (an Fc-enhanced anti-CD19 antibody) lenalidomide to R-CHOP, in 899 patients with high-intermediate or high-risk DLBCL/HGBL (IPI 3-5 or aaIPI 2-3).
The results:
→ Improved PFS: HR 0.75 (0.59-0.96), p=0.019 — 2-year PFS 71% vs 63% ( 8.2 points)
→ Benefit driven by the ABC subtype (HR 0.59), more modest in GCB (0.69, CI crossing 1)
→ OS still immature, no significant difference (HR 0.85)
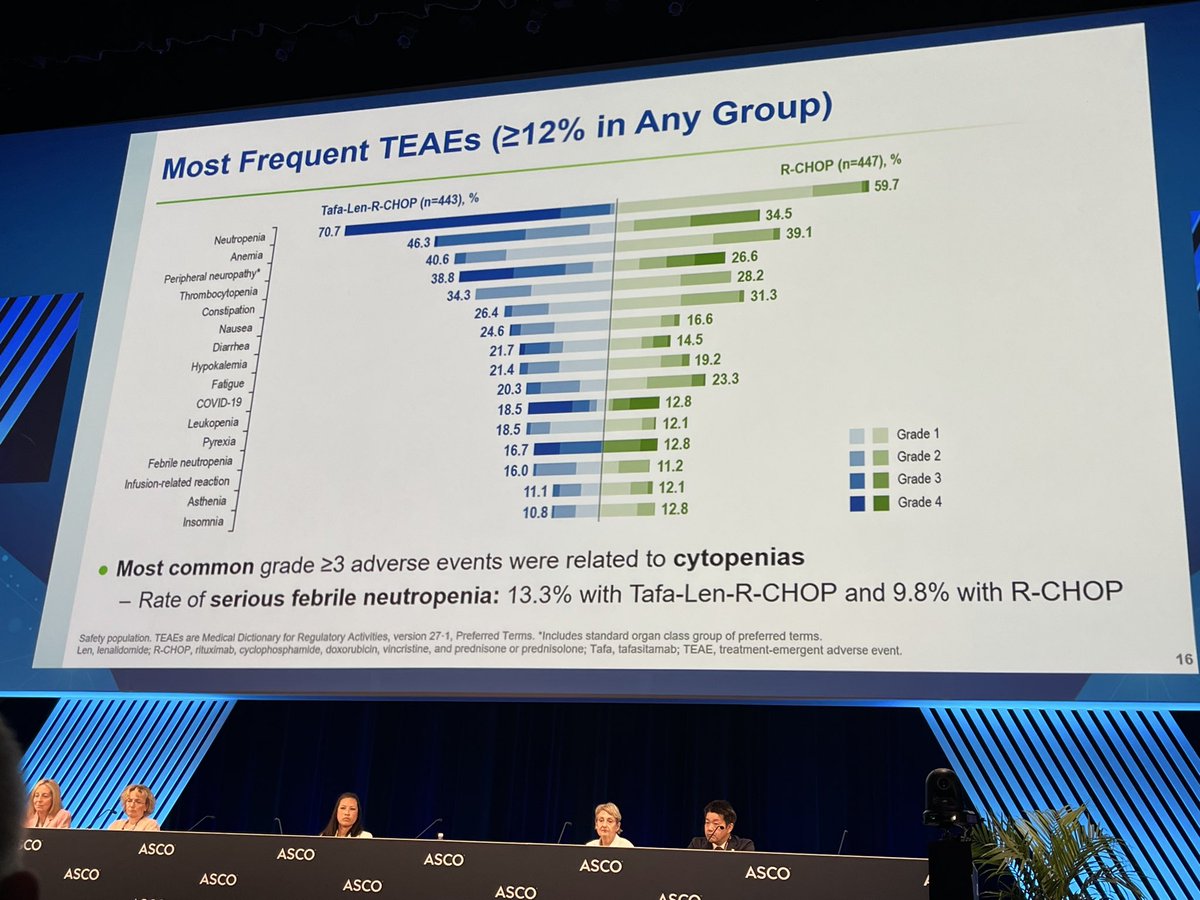
→ The price to pay: more hematologic and infectious toxicity, treatment-related mortality 6% vs 4% (partly COVID-related, as the trial ran during the pandemic)
The comparison with POLARIX is tempting, but should be handled with caution: no head-to-head data, and populations that resemble each other without overlapping — frontMIND enrolled higher-risk patients (IPI 3-5, 31% ECOG 2, vs IPI 2-5 and 16% in POLARIX).
At their core, the two stories echo each other: near-identical PFS HRs (0.75 vs 0.73), absolute benefit of the same magnitude, a clear signal in ABC, nothing convincing in GCB, and no demonstrated overall survival benefit.
That said, pola-R-CHP replaces vincristine without meaningfully adding to the toxicity profile, whereas tafa-len-R-CHOP adds two drugs and a weekly tafasitamab schedule, at the cost of what appears to be higher toxicity.
A question common to both trials: in the absence of an overall survival benefit, what place in our treatment algorithms?
#DLBCL #lymphoma #hematology
thelancet.com/journals/lance…
3
20
3,295
May 30
Another target-option for non-GCB DLBCL.
If ESCALADE is positive, we will have 3 great options for this population.
I would favor ibtk or Pola, though.
We need options now for GCB DLBCL. For now, R-DA-EPOCH for IPI >2 and MYC-R?
Let the controversy begins!🔥🔥🔥

ABC dominated responses with higher Gr3/4 neutropenia and thrombocytopenia

3
4
19
3,444
May 30
Best booth in ASCO.
Go for the pão de queijo.
Stay for the great people!
May 30

Come by Einstein’s booth to eat some pão de queijo and brigadeiro #asco26 @ASCO @hosp_einstein @PestanaRC

1
1
11
840
May 29
There are 2 types of DLBCL who relapse in CNS
MCD
MYC-R
Thats why all trials will be negative.
What I would do?
IBTK for all MCD
IT HDMTX for MYC-R
meetings.asco.org/meetings/2…
2
9
39
7,122
May 28
Great work from @andreemeireles and @palomamresende, former fellows who have joined our team at Einstein.
Very well balanced review, with the help of my friends from 🇦🇷 and 🇨🇱.
Very Proud!
May 28

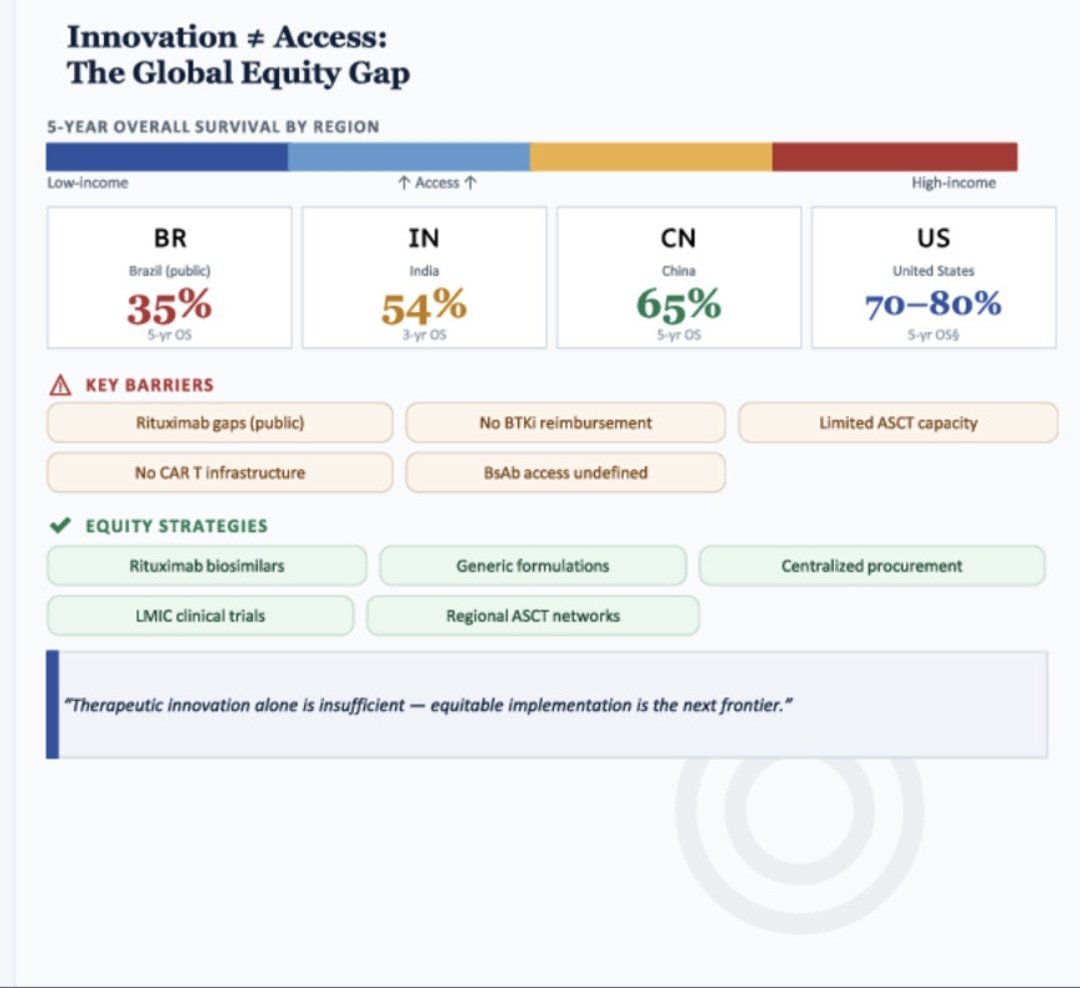
Access may increasingly become a dominant determinant of outcomes, rivaling disease biology itself.
(This is probably applicable across all of medicine)
doi.org/10.1016/j.clml.2026.…

1
6
22
3,555
May 28
👀👀👀👀
Great news for countries where GEP is not avaliable.
Next: consistent IHC panel for MCD?
I used to be a vocal skeptic of Hans and a key GEP fan, some say as an OG for GEP. I used to lament Hans IHC as the only tool available for my patients, when many trials used GEP instead.
But I have been surprised by learning how IHC has dramatically improved over the last decade or so with availability of standardized antibody clones, use of auto strainers, and interpretation consistency.
How was I convinced?
We did a systematic meta-analysis of >2200 patients from 19 studies. We used the PRISMA diagnostic test accuracy framework for comparing Hans to GEP.
library.ehaweb.org/eha/2026/…
Remarkably, this analysis now clearly shows that Hans is consistently non-inferior to GEP across current modern studies at a 10% NI margin for Accuracy, Precision, and Specificity.
This solid performance of Hans IHC is very much in line with current CAP benchmarks for diagnostic tests, and within the margins of NanoString GEP using FFPE vs original frozen GEP as the original elusive gold standard.
Long live Hans as the best currently available SOC for COO across the globe.
3
1,737
May 27
The best quote for DLBCL treatment Ive seen in years!
👏👏👏👏
May 27

An age of abundance and a chaos of choice…
1
3
3,322
May 27
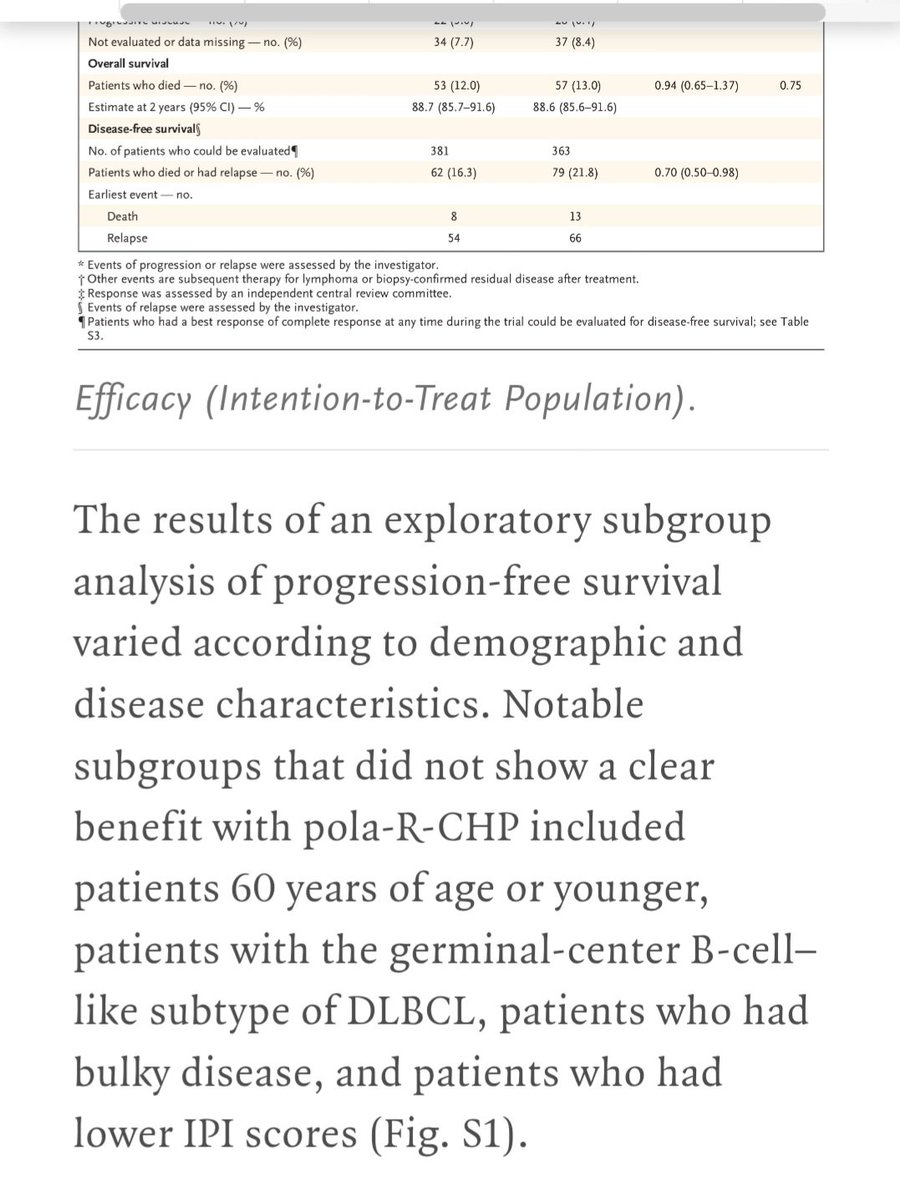
Its time to conclude that Pola is not an agnostic drug in DLBCL. It is rather a precision therapy for non-GCB/ABC/MCD DLBCL.
The fact that Queen Laura brings this up adds extra flavour to the discussion, since she doesnt believe in Precision therapy in DLBCL! 😂😂😂
May 27

POLA-R-ICE vs R-ICE in r/r LBCL
Adding pola to R-ICE missed its 1ary endpoint overall.
Subgroup winners: DLBCL, relapsed, bulky disease & ⬆️ LDH all showed meaningful OS benefit.
1ary refractory disease? Pola won't save it. Perhaps BsAb-chemo combos are the answer there? #EHA2026
5
5
38
13,870
Guilherme Perini, MD retweeted

May 26
If you are interested in lymphoma analysis from EHA2026 do sign up - should be good fun! #lymsm #lymphoma vjhemonc.com/event/post-eha-…

5
47
2,526