
Joined March 2009
- Tweets 35,148
- Following 4,074
- Followers 12,003
- Likes 71,517
2,870 Photos and videos










Pinned Tweet

26 Sep 2024
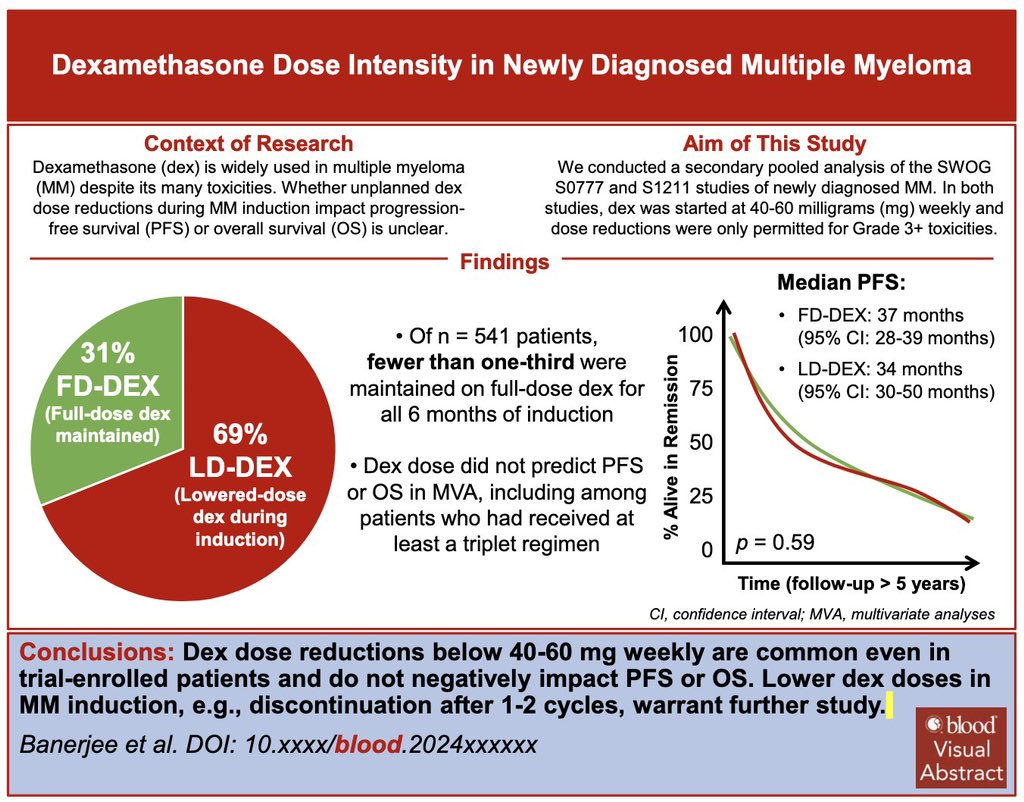
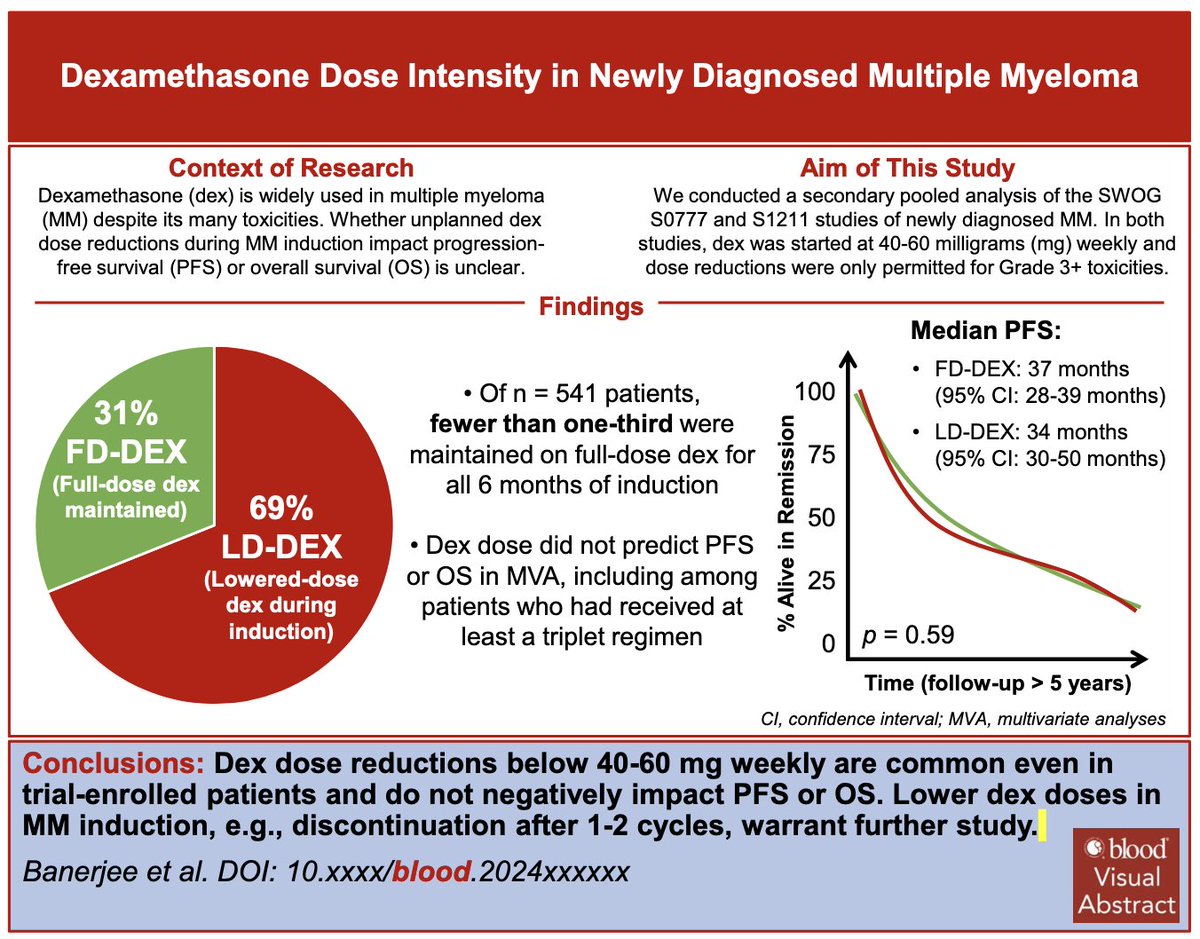
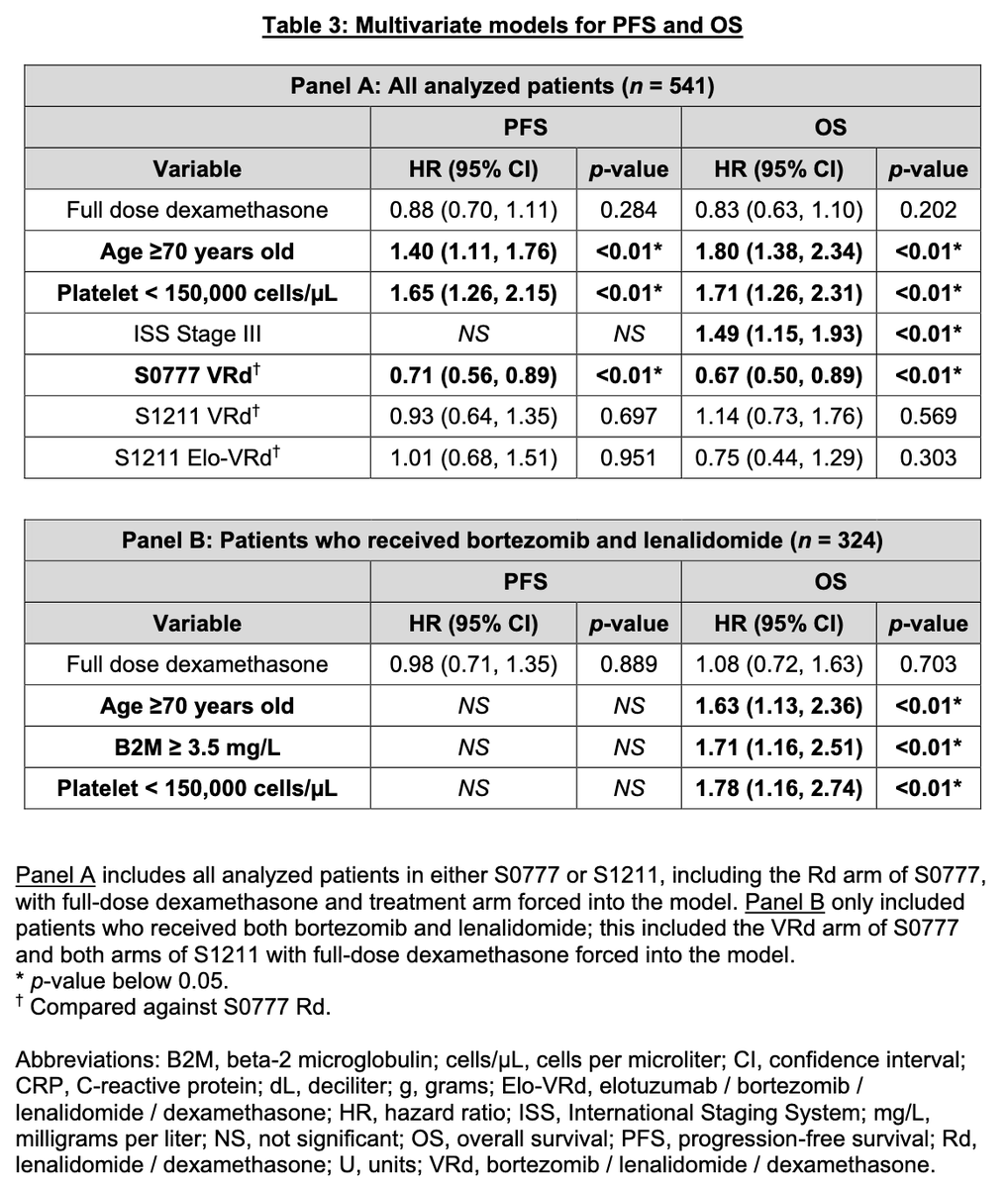
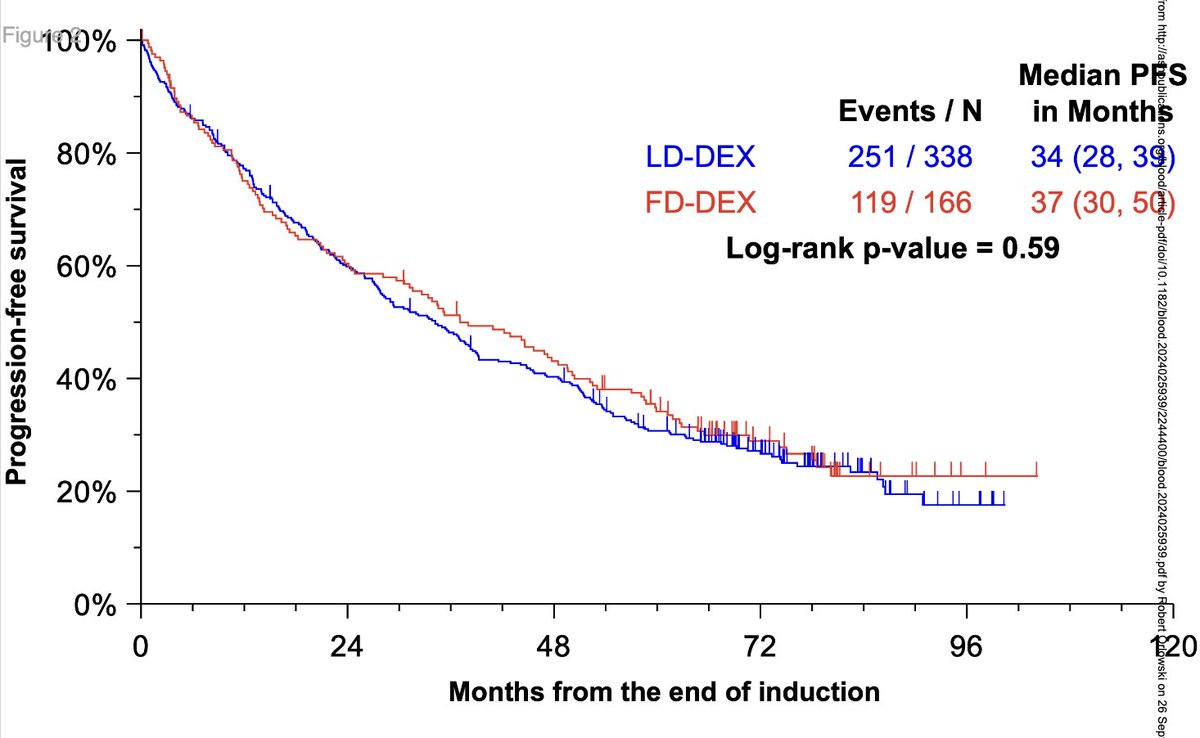
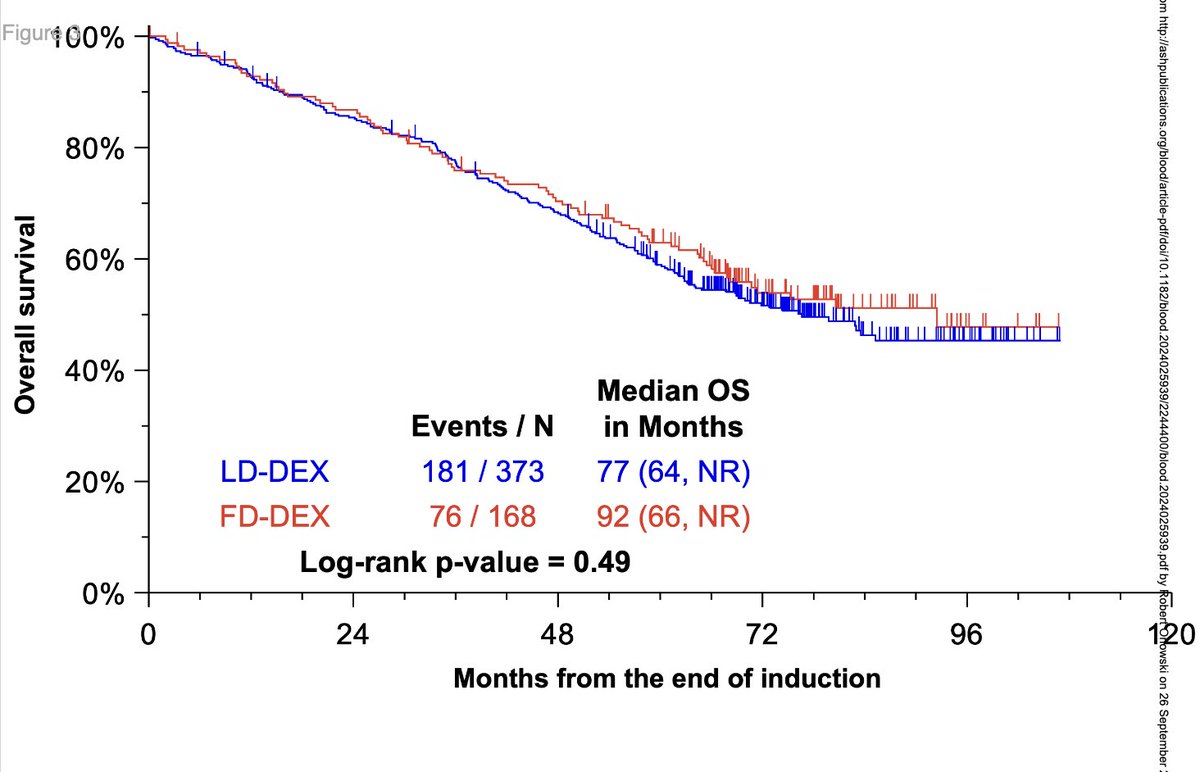
Grateful to @BloodJournal, co-authors, and @SWOG for making this #downwithdex piece possible!
Dex 40mg weekly in #MMsm induction:
1️⃣ Not practical even for trial-enrolled patients
2️⃣ Does not improve PFS vs ⬇️ dex
Twitter 🧵 once I’m back from #IMS24!
ashpublications.org/blood/ar…
26 Sep 2024

#Myeloma Paper of the Day: Cool paper from @RahulBanerjeeMD showing analysis of S0777 and S1211 @SWOG trial data that lowering the dose of dex during induction therapy did not have an impact on long-term outcomes like PFS & OS: pubmed.ncbi.nlm.nih.gov/3932…. #mmsm
24
48
216
71,368
Rahul Banerjee, MD, FACP retweeted

CONGRESS | #EHA2026 | PRESENTATION
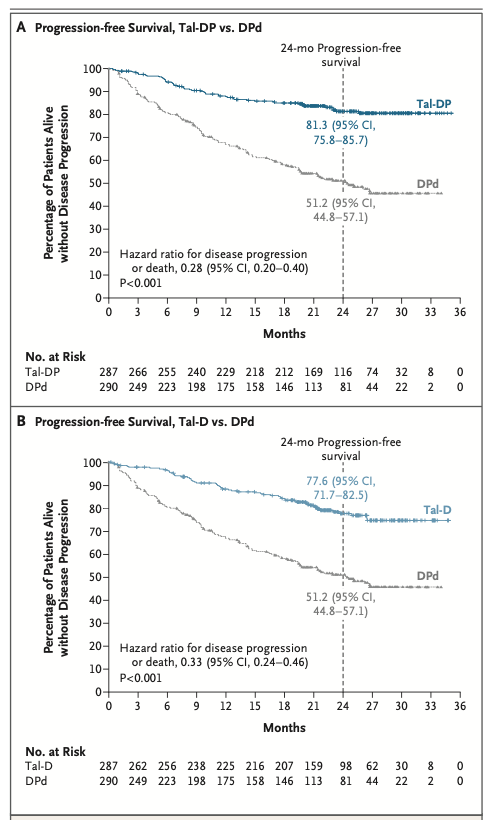
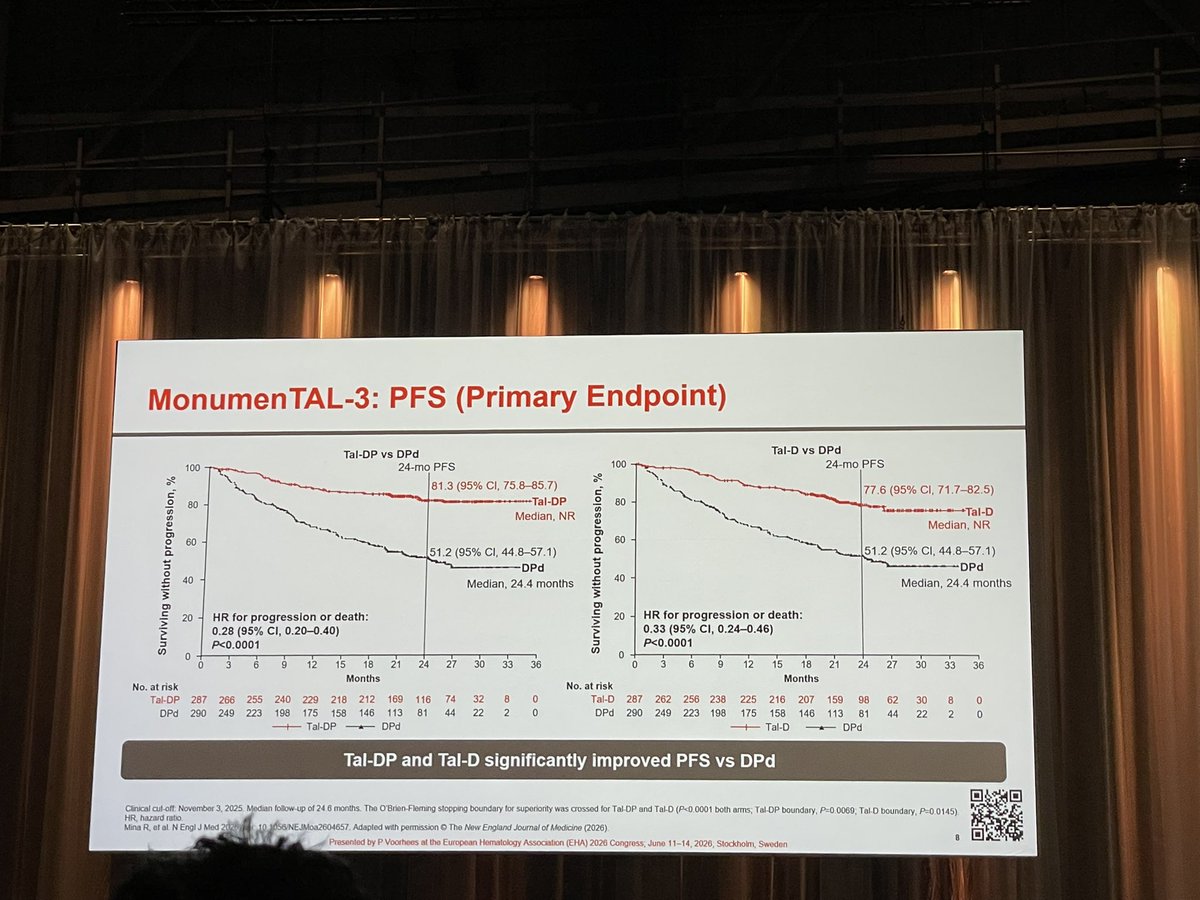
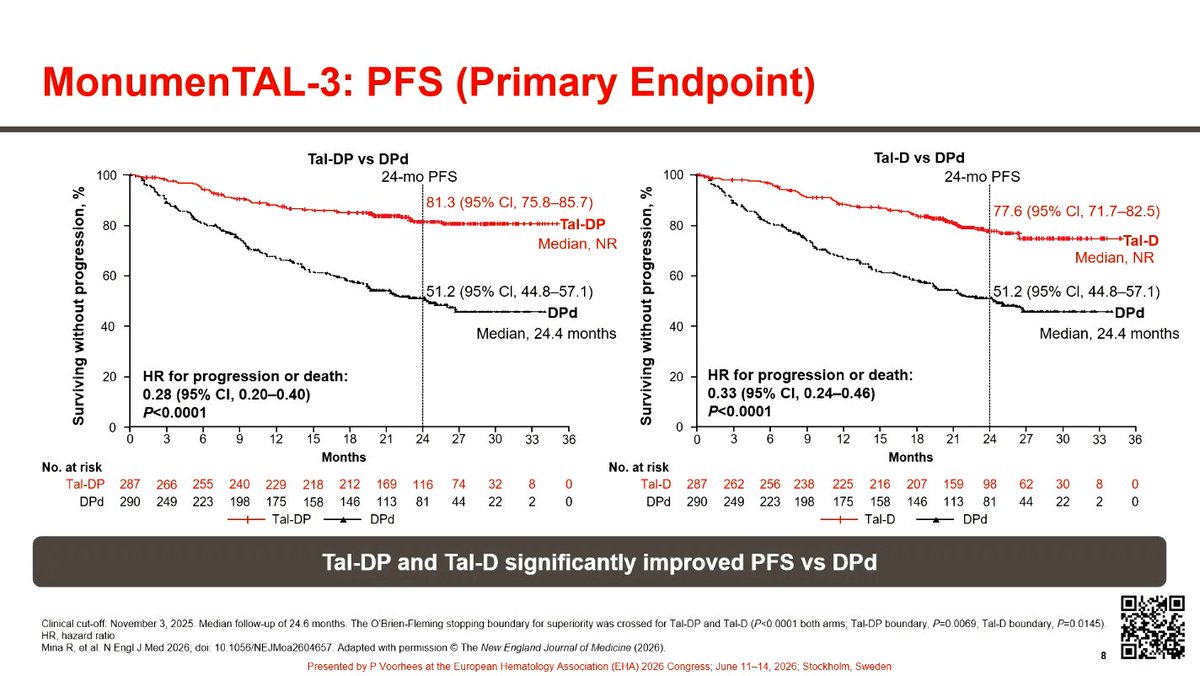
Peter Voorhees presents results from the phase III MonumenTAL-3 study evaluating talquetamab plus daratumumab ± pomalidomide (TalDP; TalD), versus daratumumab plus pomalidomide, and dexamethasone (DPd) for the treatment of RRMM.
TalDP and TalD was associated with improved PFS vs DPd, corresponding to a reduced the risk of progression or death by 72% (HR, 0.28; P < 0.0001) and 67% (HR, 0.33; P < 0.0001), respectively. At 24 months, PFS rates were 81.3% with TalDP, 77.6% with TalD, and 51.2% with DPd. TalDp/TalD were also associated with higher ORR, ≥CR, and MRD-negative CR rates vs DPd. Safety findings were consistent with the known profiles of the individual agents.
Follow our live feed for more updates: loom.ly/CXccZxs
Intended for HCPs only. This congress coverage is independently supported by pharmaceutical companies, who are allowed no influence on the content; a full list of supporters can be found on our website.
#MultipleMyeloma #myeloma #mmsm #MedEd



2
6
339
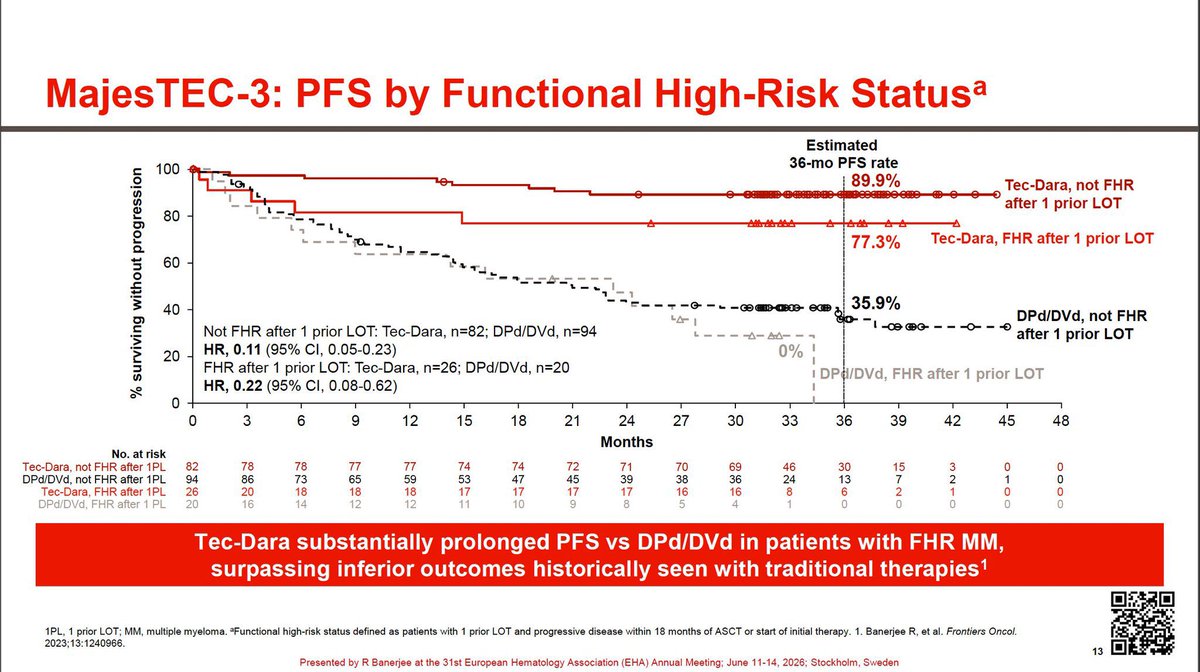
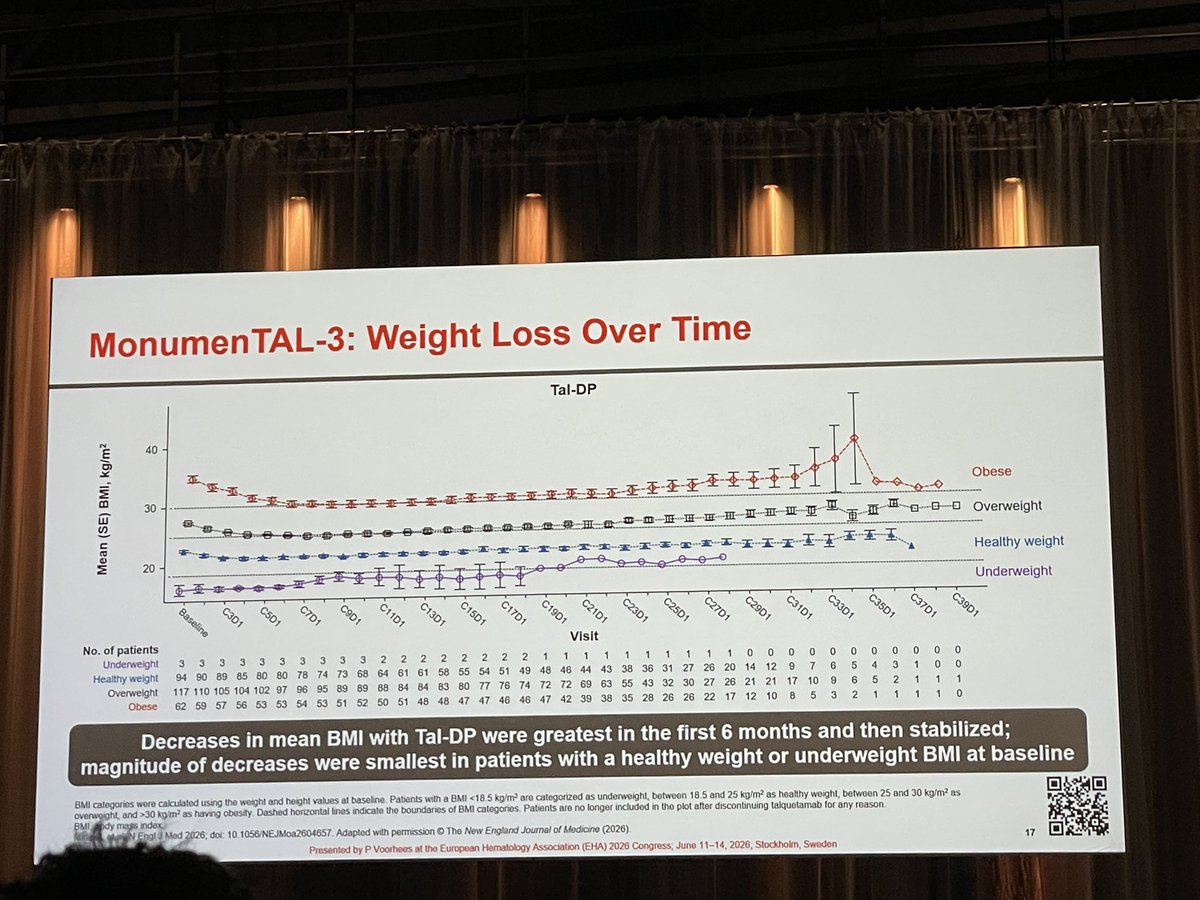
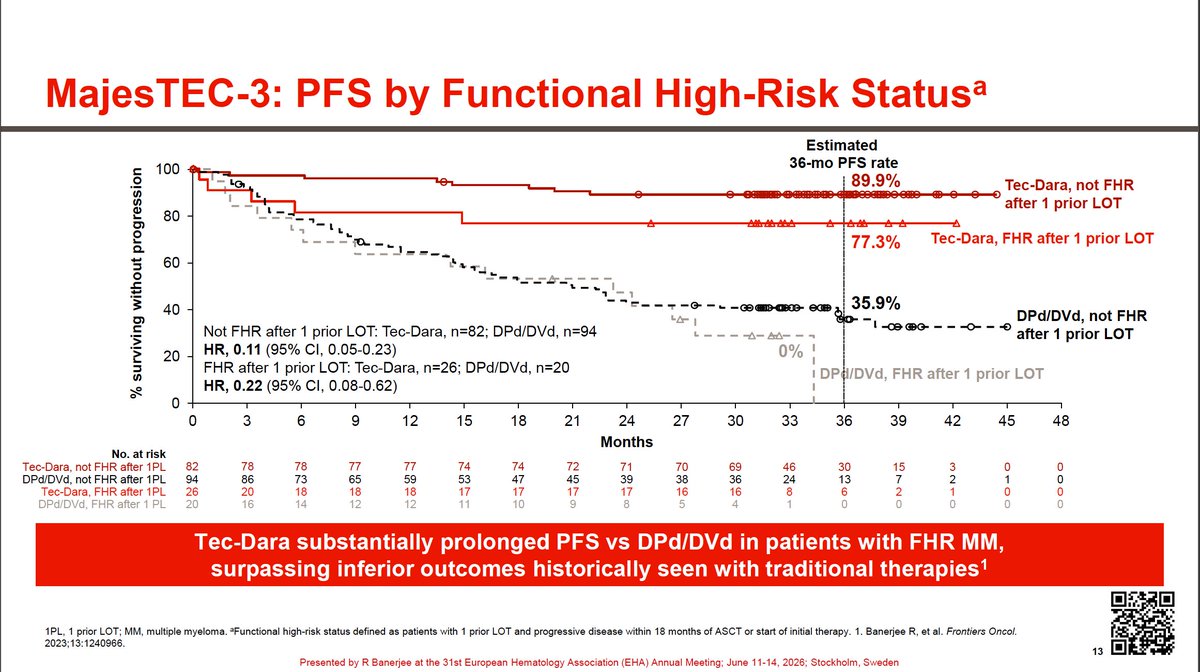
I’ve looked at this #EHA2026 slide 100x but it still always makes me pause.
Unexpected early relapses so scary for patients with myeloma, and historically post-PD OS in FHRMM ≤ 2 years no matter what we do.
Here, off-the-shelf Tx boosted 3-yr PFS from 0% to 77%. Giving these pts a fighting chance for deep & durable remissions 🥹
3
4
16
533
Rahul Banerjee, MD, FACP retweeted



4
8
368
Rahul Banerjee, MD, FACP retweeted

#mmsm #EHA26
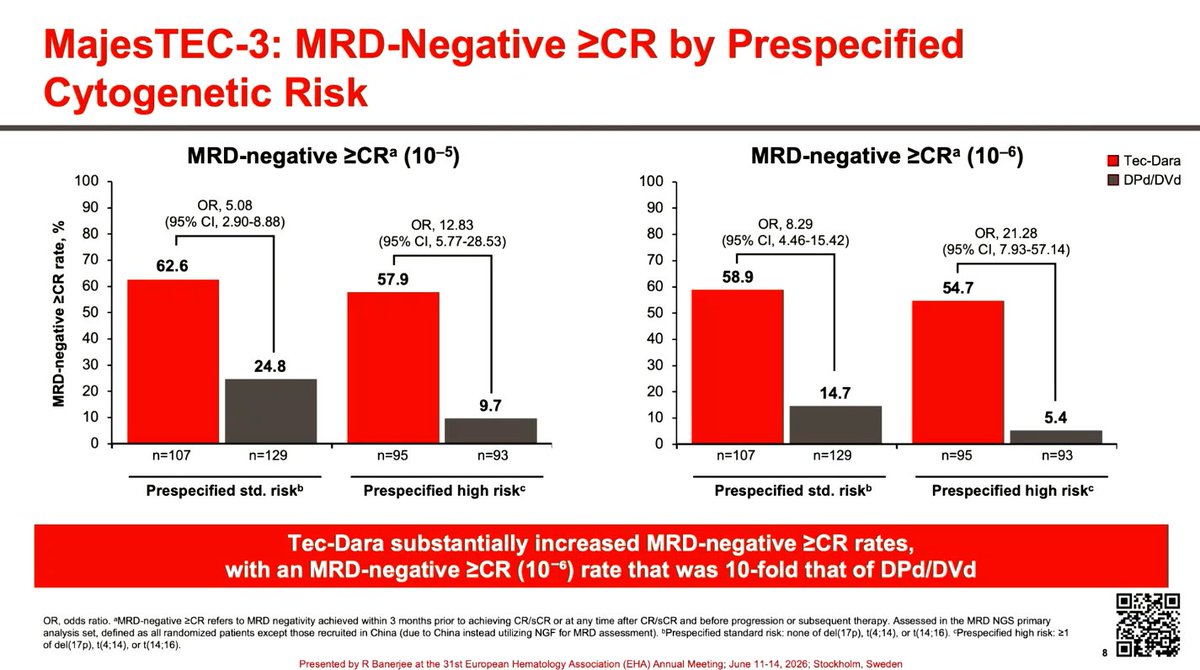
MajesTEC-3 high risk post hoc analysis @RahulBanerjeeMD
Tec-Dara worked well in patients with 2HRCA or more as well as functionally high risk
Really good results in hard to treat patients


3
11
25
3,889
Rahul Banerjee, MD, FACP retweeted

Congratulations! Great result and another new landmark SOC at relapse
1
1
136
Rahul Banerjee, MD, FACP retweeted
CONGRESS | #EHA2026 | PRESENTATION
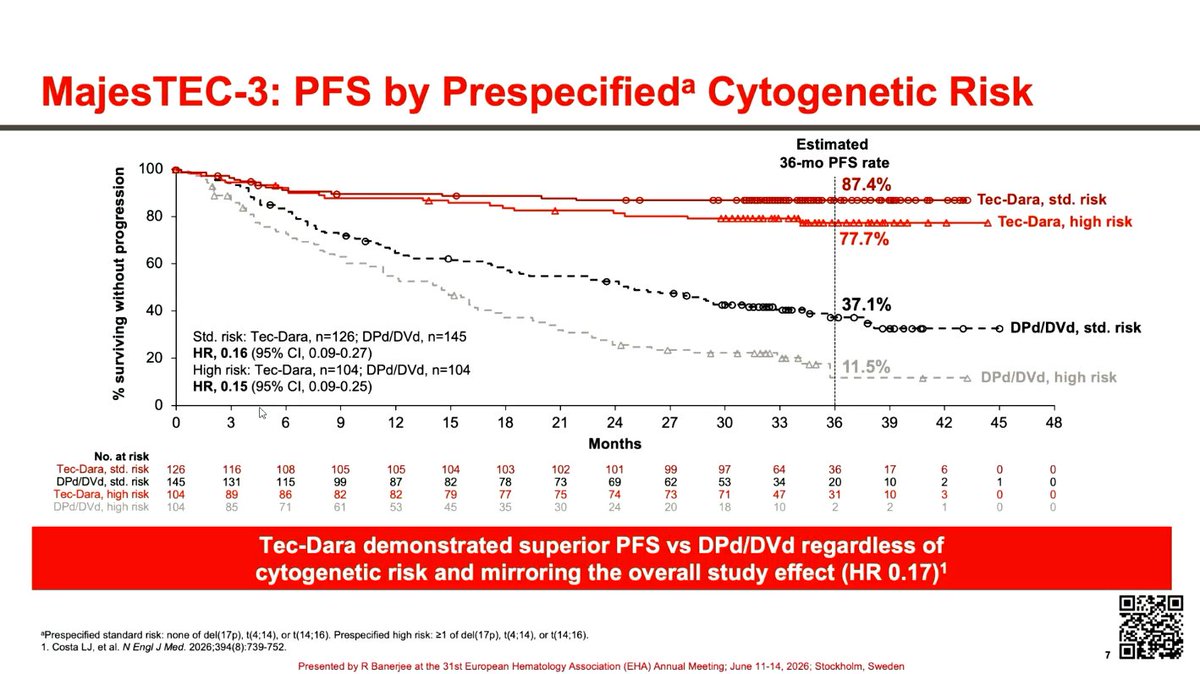
Rahul Banerjee presents results from an analysis of the phase III MajesTEC-3 study evaluating teclistamab plus daratumumab (Tec-Dara) in patients with RRMM, stratified by cytogenetic and functional risk.
Tec-Dara improved PFS versus DPd/DVd across all cytogenetic and functional risk groups. In patients with prespecified HR cytogenetics, median PFS was not reached with Tec-Dara versus 14.4 months with DPd/DVd (HR, 0.15), while estimated 36-month PFS rates were 77.7% versus 11.5%, respectively. Tec-Dara also increased MRD-negative ≥CR rates across risk groups, including among patients with functional high-risk disease (42.9% vs 5.6% at 10⁻⁵sensitivity; OR, 12.75).
Follow our live feed for more updates: loom.ly/CXccZxs
Intended for HCPs only. This congress coverage is independently supported by pharmaceutical companies, who are allowed no influence on the content; a full list of supporters can be found on our website.
#MultipleMyeloma #myeloma #mmsm #MedEd @RahulBanerjeeMD


1
4
13
552
Rahul Banerjee, MD, FACP retweeted

High risk nearly eliminated or redefined
1
5
9
371
Rahul Banerjee, MD, FACP retweeted

Phenomenal presentation by @RahulBanerjeeMD here at @EHA_Hematology #EHA2026! Drop the 🎤 moment with the high risk data! @End_myeloma and @mvmateos broke the MajesTEC-3 data at #ASH25 and these data provide important information for 2L high risk patients. #MyCompany

2
7
18
620
Rahul Banerjee, MD, FACP retweeted

GLP1 is likely going to change landscape of many disease ; I think in a positive way over the next many decades
usmedicine.com/clinical-topi….
1
2
157
Rahul Banerjee, MD, FACP retweeted

Not a plateau in whole cohort, but do the authors have info about MRD -ve VS. ve? Probably there we can see a plateau. @RahulBanerjeeMD

#EHA2026 not a plateau, but what amazing results all the same!
@szusmani presenting updated CEPHEUS data.
6 years out for some patients, median OS *still* not reached with D-VRd despite no transplant.
Great to see long-term quad data emerging!
2
3
6
441
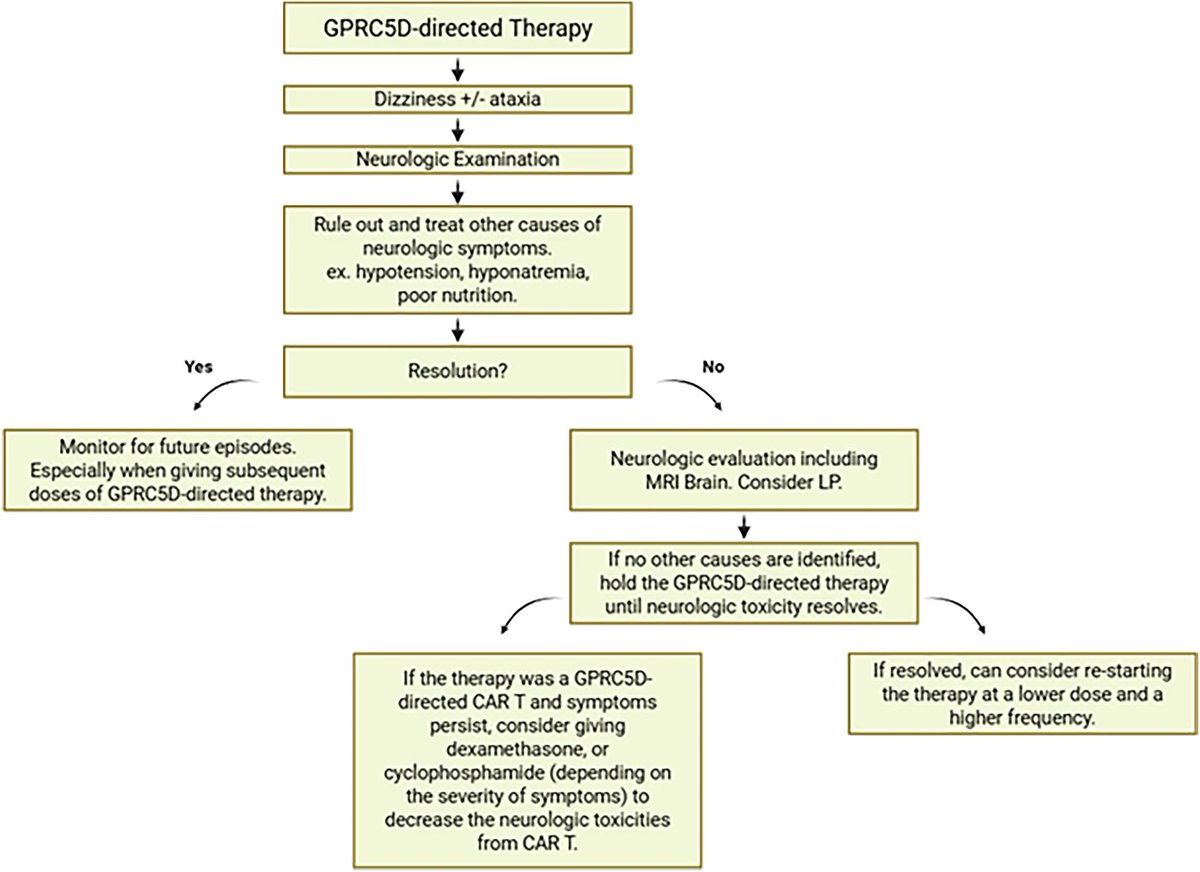
Excellent #EHA2026 🧵- Something we continue to learn about as we use GPRC5D more in myeloma.
We’ll overestimate incidence at first (e.g., dizziness from orthostatic hypotension from wt loss, 1st noted by @AjaiChari ) … but more research & unified AE term will go a long way!

With Tal-Dara published and concerns about ataxia/ balance disorders lets take a deep dive on GPRC5D ataxia syndrome
-> The first report of a cerebellar syndrome from GPRC5D came from MCARH019 reported by Mailankody et al
-2/17 (12%) Grd 3 cerebellar syndrome
-6.5 and 8.4 mo's after infusion
-was a DLT at 450*10^6
1
3
340
Rahul Banerjee, MD, FACP retweeted

3. Uncover the pathophysiology through translational science
4. Incorporate this in prospective clinical trials
5. Develop guidance for clinicians on early identification and prevention, rechallenge
6.GPRC5D is an important therapeutic target
2
2
6
265
Rahul Banerjee, MD, FACP retweeted
2. Understand the syndrome, its variations, risk factors. In the IMWG we are undertaking a co-ordinated effort to collect the clinical course of these patients. Specifically- onset, CNS signs/symptoms, resolution, imaging.
This is a syndrome and should not be considered symptom in isolation. If talq is continued the whole syndrome will develop.
Also imperative to stress is reversibility which we have seen in the real world experience
1
1
4
257
Rahul Banerjee, MD, FACP retweeted
What should we do in the field
1. Common terminology- we can't call it ataxia/balance disorder, other selected neurotoxicity (CART) , cerebellar syndrome. We need to name it as GPRC5D related ataxia/balance disorder across trials and RWE
-This is important so that non specific symptoms like dizziness or balance disorders which has other causes are not attributed wrongly
1
2
3
290
Rahul Banerjee, MD, FACP retweeted
Lets consolidate
-ataxia/balance disorder, dizziness early symptom
-occurs with GPRC5D CART and Bispecific
-increasing incidence over time, hence needs vigilance
What's not known
-why the wide variance
-pathophysiology [seperate tweet]
-syndrome
-who is at risk, reversibility
-prevention/treatment
1
1
3
227
Rahul Banerjee, MD, FACP retweeted
Now lets look at MONUMENTAL-3- Table S19
-captured ataxia and balance disorders
-12.4 &14.5%, 2.9 & 2.2% Grade 3
-8% dose delays/skips
-time to onset- 73 wks -81 wks
-earliest is 3 and 24 days
-quite different/delayed to what we are seeing in RWE
-10-16% resolution, 68-88% no resolution
-low in cycle 1 (0.4% ), increased during cycles 2-6 (4.7%, 2.6%), and highest from cycle 7 (10.9%. 10.2% ).
1
1
5
284
Rahul Banerjee, MD, FACP retweeted
Second report from @Phhersh in real-world
They put together a series of 6 patients and named it vestibular syndrome
Wide variation in onset but notice improvement and reversibility

1
1
3
194
Rahul Banerjee, MD, FACP retweeted
What happens in real world.
I noticed this in some of my patients treated with talq and put together a case series with our group
Notice the relatively early onset and reversibility
Named this as dizziness-ataxia syndrome

1
3
6
224
Rahul Banerjee, MD, FACP retweeted
With Tal-Dara published and concerns about ataxia/ balance disorders lets take a deep dive on GPRC5D ataxia syndrome
-> The first report of a cerebellar syndrome from GPRC5D came from MCARH019 reported by Mailankody et al
-2/17 (12%) Grd 3 cerebellar syndrome
-6.5 and 8.4 mo's after infusion
-was a DLT at 450*10^6
2
6
18
1,512
Rahul Banerjee, MD, FACP retweeted
Thx for reading this on GPRC5D ataxia, more to come. @HiraSMian @VincentRK @myelomaMD @TomMartinMD @DoctorAKrishnan @RobertoMinaMD @HadidiSamer @Mohty_EBMT @TheIACH @AjaiChari @NBahlis @RahulBanerjeeMD @NikhilMunshiMD @NoopurRajeMD Sham Mailakondy @YiLinMDPhD Vania Hungria Peter Voorheese @End_myeloma Torsten Steinbaumm Hermann Einsele
1
6
238