
“No one should ever suffer or die because of failures in healthcare delivery systems or processes of care.”
- Tweets 383
- Following 229
- Followers 134
- Likes 118


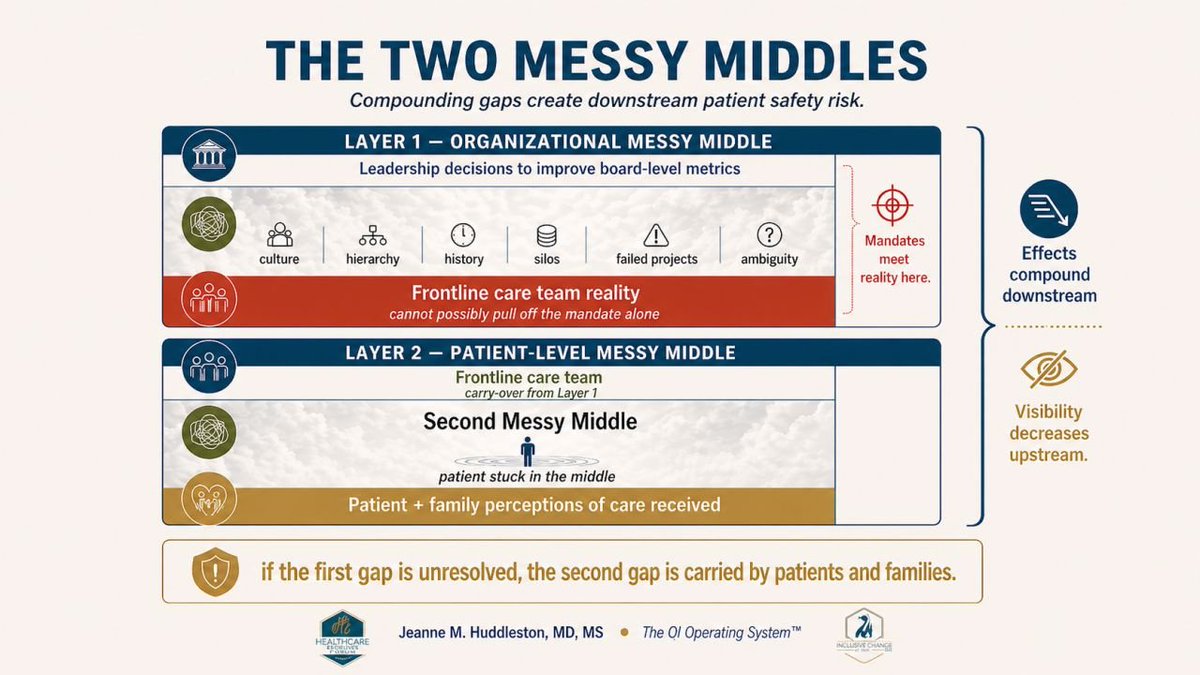

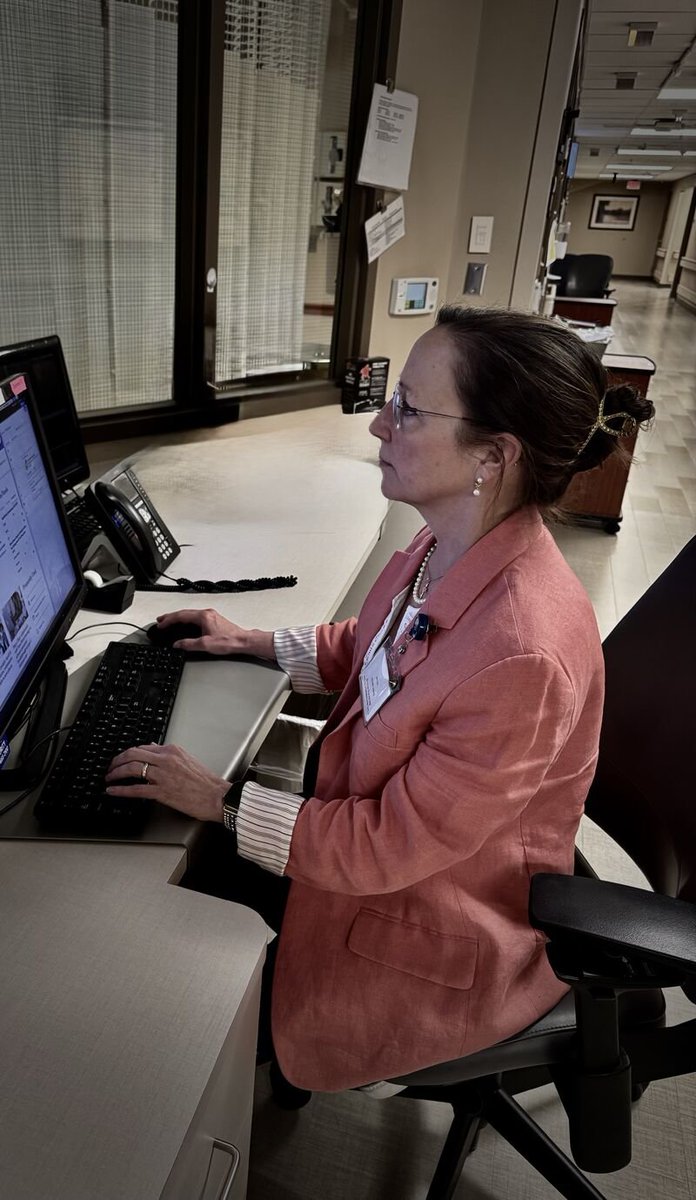


ALT A hospital room scene showing a nurse standing between a patient in a bed and a physician on a laptop screen conducting a tele-admission. The nurse looks concerned and caught in the middle, while the patient appears disengaged. The clinician on the screen is speaking, but the interaction feels disconnected. Overlaid text reads “The Messy Middle,” highlighting the gap between virtual care and real patient needs.
ALT Teal background graphic with the headline “Is Your RCA Process Performative?” followed by “3 Warning Signs” in red text. Three bullet points list: “Action items restate existing policy (not new system changes),” “Same causal factors across RCAs – no pattern-level response,” and “Completion times exceed standard due to deferrals, not complexity.” Red square icons appear next to each bullet point.
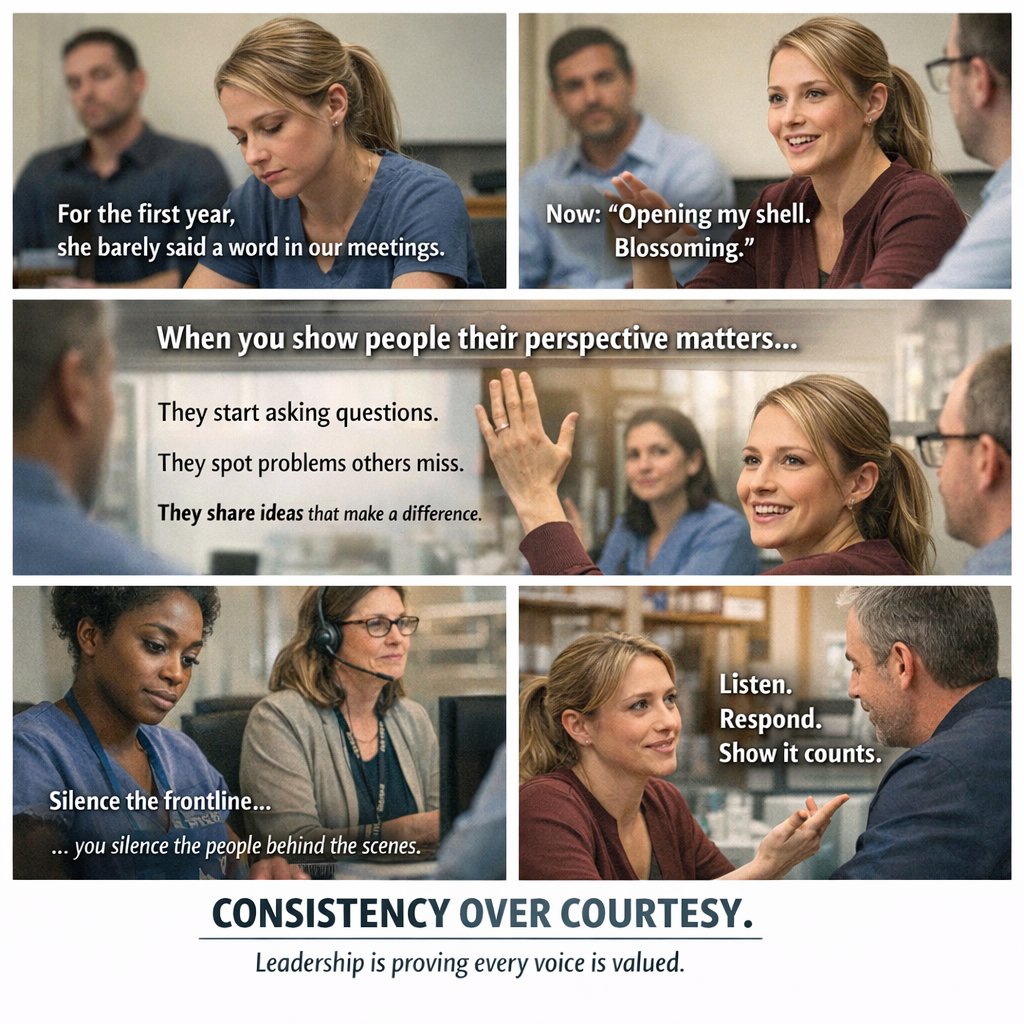
ALT A multi-panel image showing a workplace meeting progression: a team member sitting quietly at a table, later raising a hand during discussion, and leaders actively listening and responding. Text emphasizes that people speak up when they are consistently expected to and when their input leads to visible action.
ALT QI professionals, voice unheard, Quality work in healthcare, nurse, nurse lead, physician, medical
ALT QI professionals, voice unheard, Quality work in healthcare, nurse, nurse lead, physician, medical
ALT QI professionals, voice unheard, Quality work in healthcare, nurse, nurse lead, physician, medical

ALT QI professionals, voice unheard, Quality work in healthcare, nurse, nurse lead, physician, medical

ALT A QI team working on a deteriorating-patient recognition project was stuck for months. Capable professionals. Trained in Lean. Physician, nurse lead, nurse, better care