
Joined May 2025
- Tweets 80
- Following 51
- Followers 15
- Likes 8
14 Photos and videos








4 Dec 2025
Normal aging and clinical frailty are two completely different trajectories, with very different implications for care.
1
1
21
4 Dec 2025
Frailty is often described as “inevitable.”
But much of it is modifiable when we can actually see the early trends.
Visibility creates opportunity.
1
20
4 Dec 2025
Frailty is a quantifiable risk domain. Something we can track, trend, and respond to, not just react to.
16
2 Dec 2025
Despite common belief, frailty is not an inevitable factor of ageing.
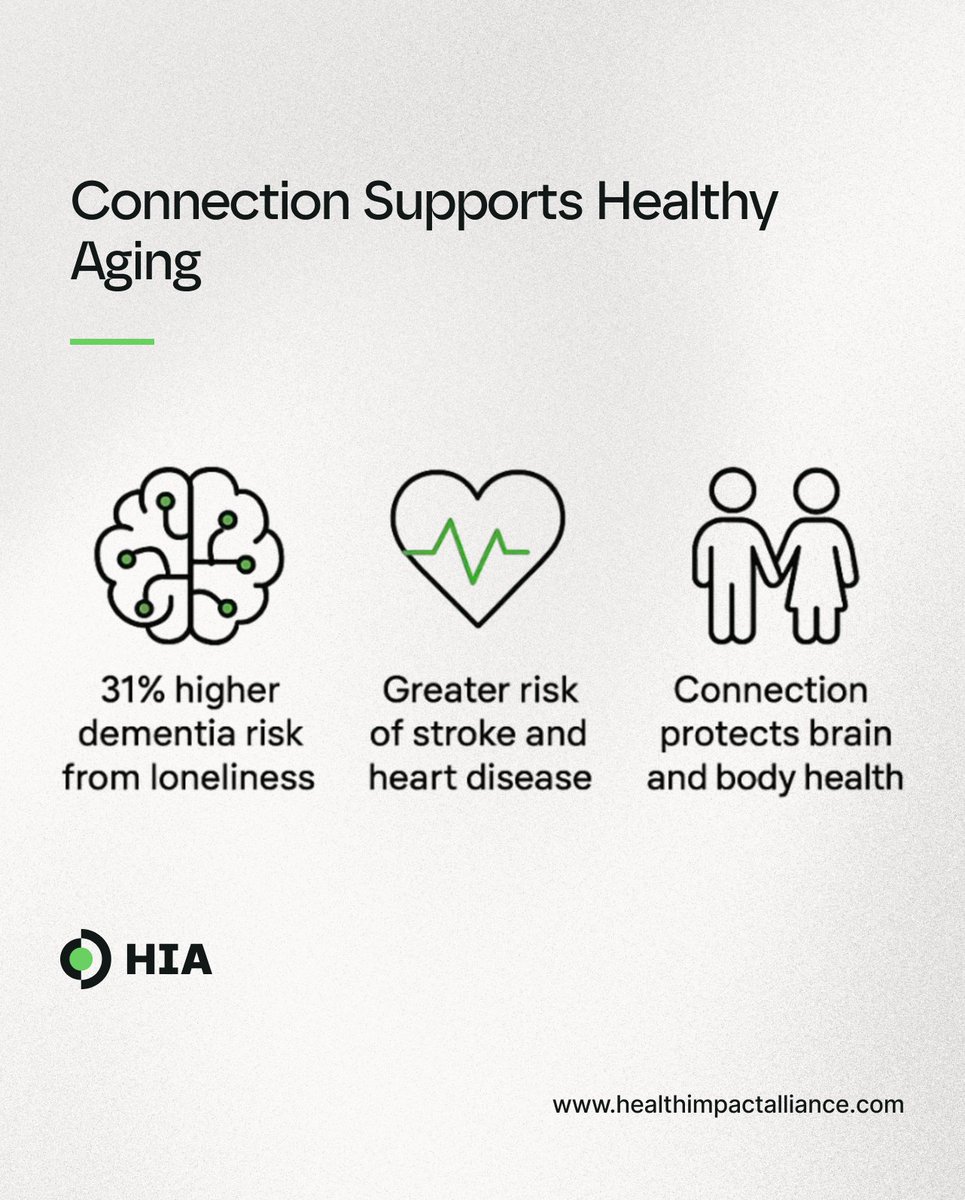
Major risk drivers include low activity, poor nutrition, chronic disease, social isolation, and socioeconomic stress.
How common is it?
• 15–17% of older adults are frail
• Prefrailty affects up to two-thirds
• Frailty rises from 11% at age 50–59 to 51% at age 90
Frailty is modifiable. Strength training, adequate protein, chronic-condition management, daily movement, and social connection can slow, stabilise, or even partially reverse decline.
27
21 Nov 2025
For decades, healthcare has moved between two distinct models, Health 1.0 and Health 2.0, but neither has solved the core issues.
1
31
21 Nov 2025
Health 3.0 evolves previous healthcare; it doesn't reject it. It combines what has worked, improves what hasn’t, and uses new tools to support healthier, more independent lives.
1
20
19 Nov 2025
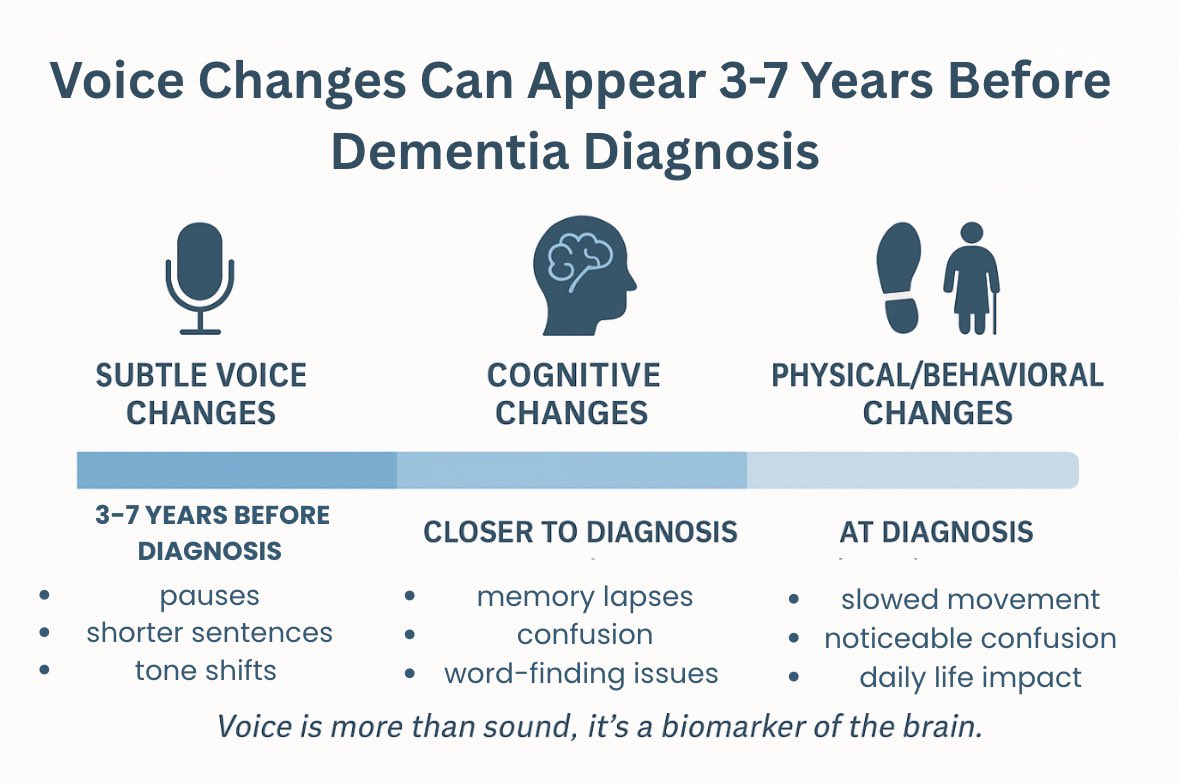
No doubt that medication saves lives, but it shouldn’t be the first time we notice something is wrong.
Most health decline has measurable early signals long before symptoms appear. We should combine proaction and preventative monitoring with clinical care.
17 Nov 2025

Do you think people rely too much on medication instead of prevention?
21
13 Nov 2025
Despite advances in healthcare and technology, fall-related deaths among older adults have reportedly risen by over 70% in the past two decades.
Why haven't we done more about this?
20
11 Nov 2025
A fall is rarely “just a fall”.
It’s usually a signal of something deeper. Mobility decline, vision changes, or early cognitive impairment.
Routine check-ups and proactive screening matter more than reaction after the injury.
1
27