
Intensivist I Internal Medicine | ☕️, 🍩, 🥐, 🍫 addict
Joined April 2020
- Tweets 14,443
- Following 755
- Followers 58,446
- Likes 12,154
2,690 Photos and videos






Our reaction to any new study is either “I don’t believe it” or “I knew it”...
A NEJM trial in ICU pts w acute resp failure found that mucolytics (carbocisteine & hypertonic saline) don’t help. My ICU rounds line “mucolytics are useless” may need an update: “and possibly harmful”
9
53
249
20,759
Aggressive chest PT…
Jun 12

Profesör doktorun, küçük bebeğin bronşitini profesyonel şekilde çıkarttığı anda çekilen video.
Community note
Bronşit bronşların iltihabıdır ve fiziksel olarak çıkarılamaz; videodaki işlem balgam temizleme olup bronşiti tedavi etmez. memorial.com.tr/hastaliklar/br… guven.com.tr/saglik-rehberi… mayoclinic.org/diseases-condi…
2
2
26
10,647

IMCrit retweeted

16 Jun 2024
Glottic impersonalisation
“Yes, I am sure the tube went into the trachea…”
@jducanto @cliffreid @DaveOlvera1 @airwayGladiator

12
51
220
66,882
I endorse this message 💯
Jun 5

SOHO trial in NEJM:
🏙️ Multicenter RCT comparing high-flow nasal cannula vs. low-flow oxygen among patients with acute hypoxemic respiratory failure (mostly pneumonia)
🏙️ Inclusion criteria required a respiratory rate >25 and substantial hypoxemia (P/F <200)
🏙️ No difference in the primary endpoint of mortality (not surprising, the mortality endpoint is nearly always neutral in modern RCTs evaluating the nuances of supportive care).
🏙️ HFNC reduced the rate of intubation and increased the number of ventilator-free days.
🏙️ No significant signals of harm from HFNC.
This is similar to the FLORALI trial (by the same group of investigators). However, FLORALI showed *improvement* in mortality, whereas the current study didn't.
Why do these studies disagree about mortality?
The FLORALI trial found no mortality difference between HFNC versus conventional oxygen among ALL PATIENTS. However, it DID find a mortality difference in the *subgroup* of patients with P/F <200.
So this is a classic tale in critical care - a subgroup analysis from one trial subsequently fails to replicate. (At least, in terms of the mortality benefit.)
But chasing mortality in these trials is a fool's errand. Overall, the SOHO trial still supports the use of HFNC in acute hypoxemic respiratory failure (in terms of reduced intubation and improved ventilator-free days).
Using HFNC for sick pneumonia patients is already standard care, so I don't see this changing practice very much. Keep calm and HFNC on. 🌬️
2
24
10,734
My thoughts are with all those people that spent their day at home today with a potassium of 3.3 (and nothing bad happened to them!)
#foamcc #electrolytes
8
9
135
10,968
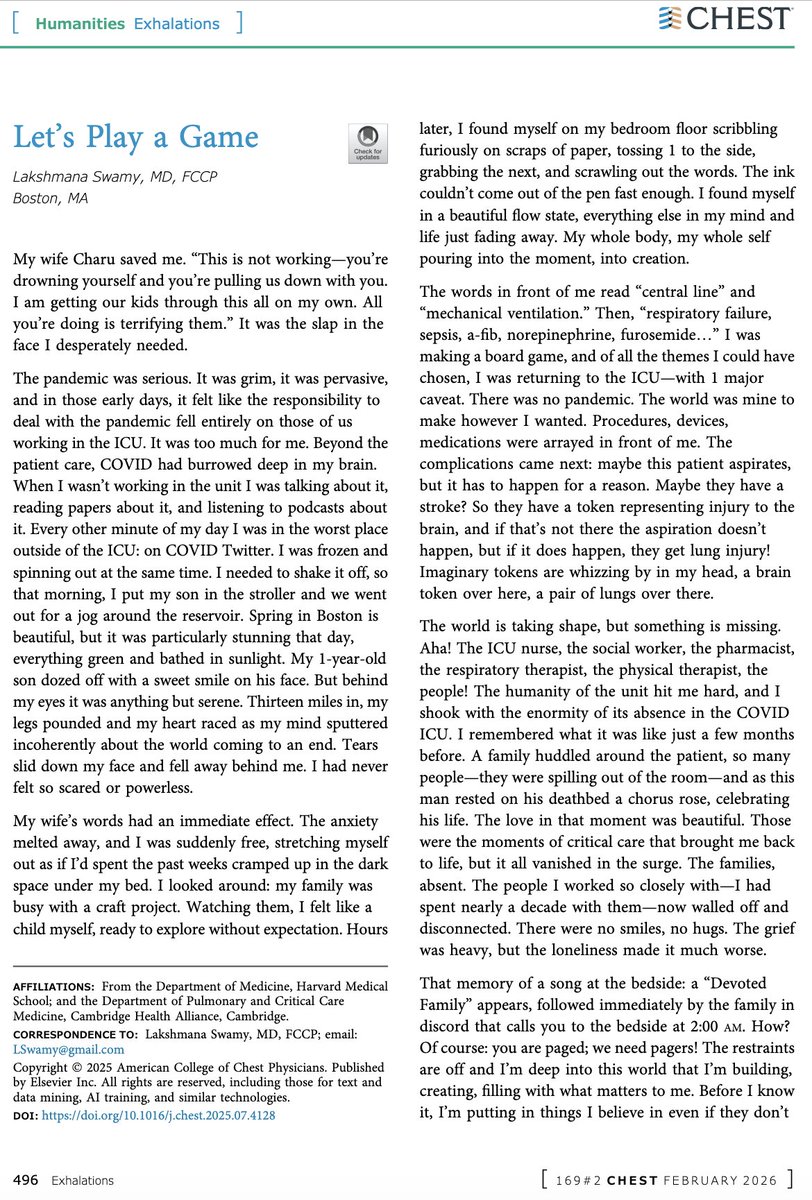
Since @laxswamy is no longer posting here, I’m sharing this 👇 from @journal_CHEST
For some, #COVID was “just a hoax.” But for many of us, it brought connection, learning, and unforgettable people into our lives online
@medtwitter doesn’t feel the same anymore...
1
3
18
3,089
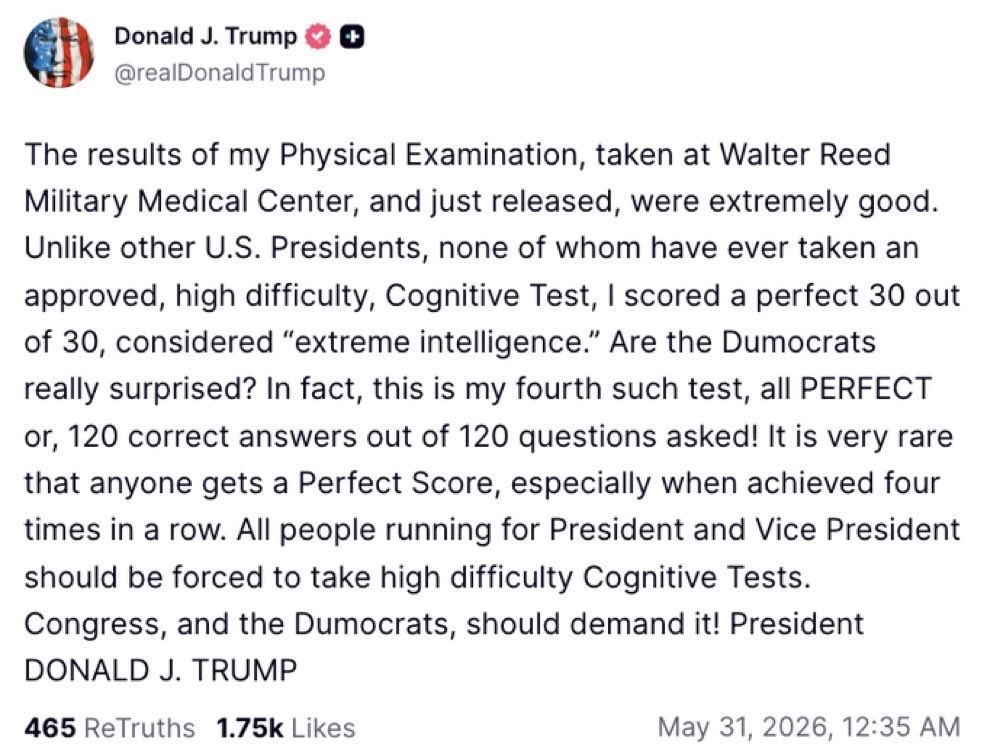
He probably forgot he took it
Jun 1

At the risk of stating the obvious, taking a dementia test 4 times isn’t a good thing.
29
6,390
IMCrit retweeted

Cheers, chills, and a standing ovation when RASolute 302 showed unprecedented survival on daraxonrasib for patients with progressive pancreatic cancer
Seldom do you sense you’re witnessing a historic moment in cancer care but this feels like ras targeting has arrived
#ASCO26
92
1,273
6,505
1,148,599
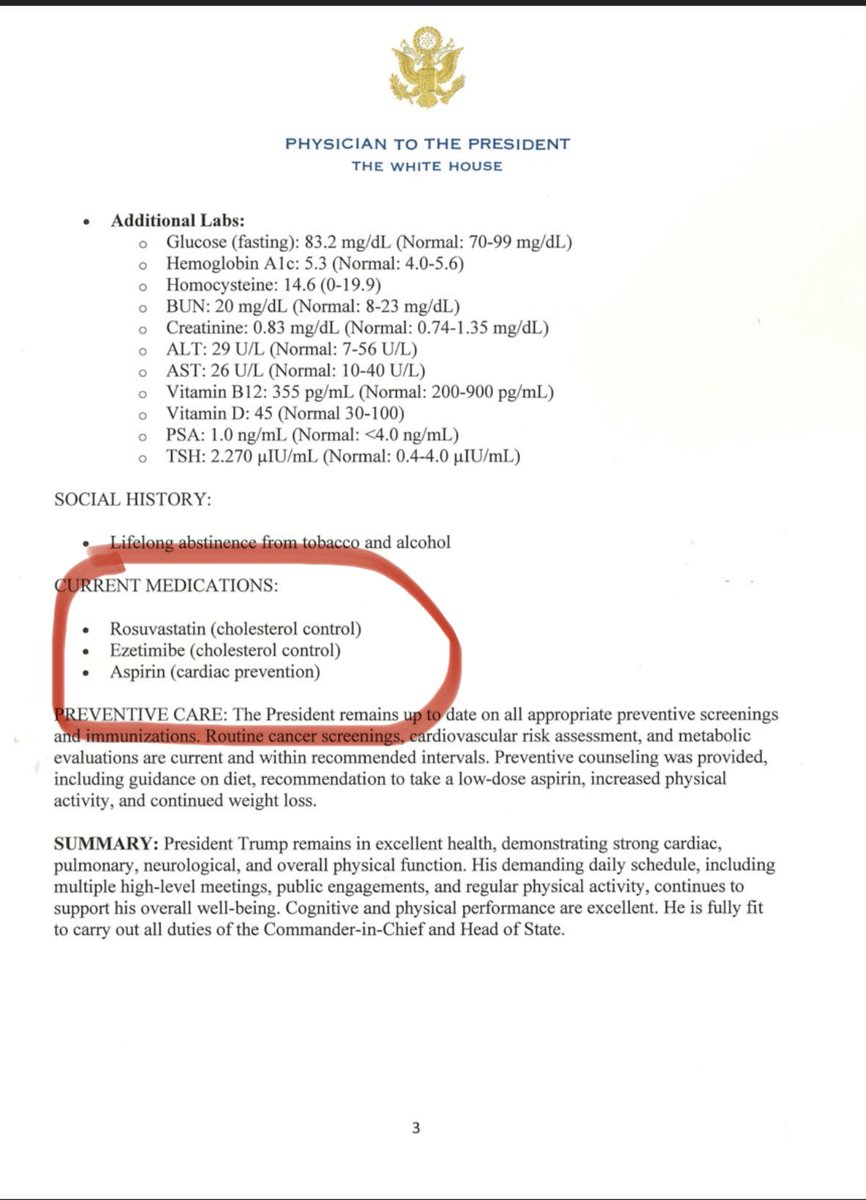
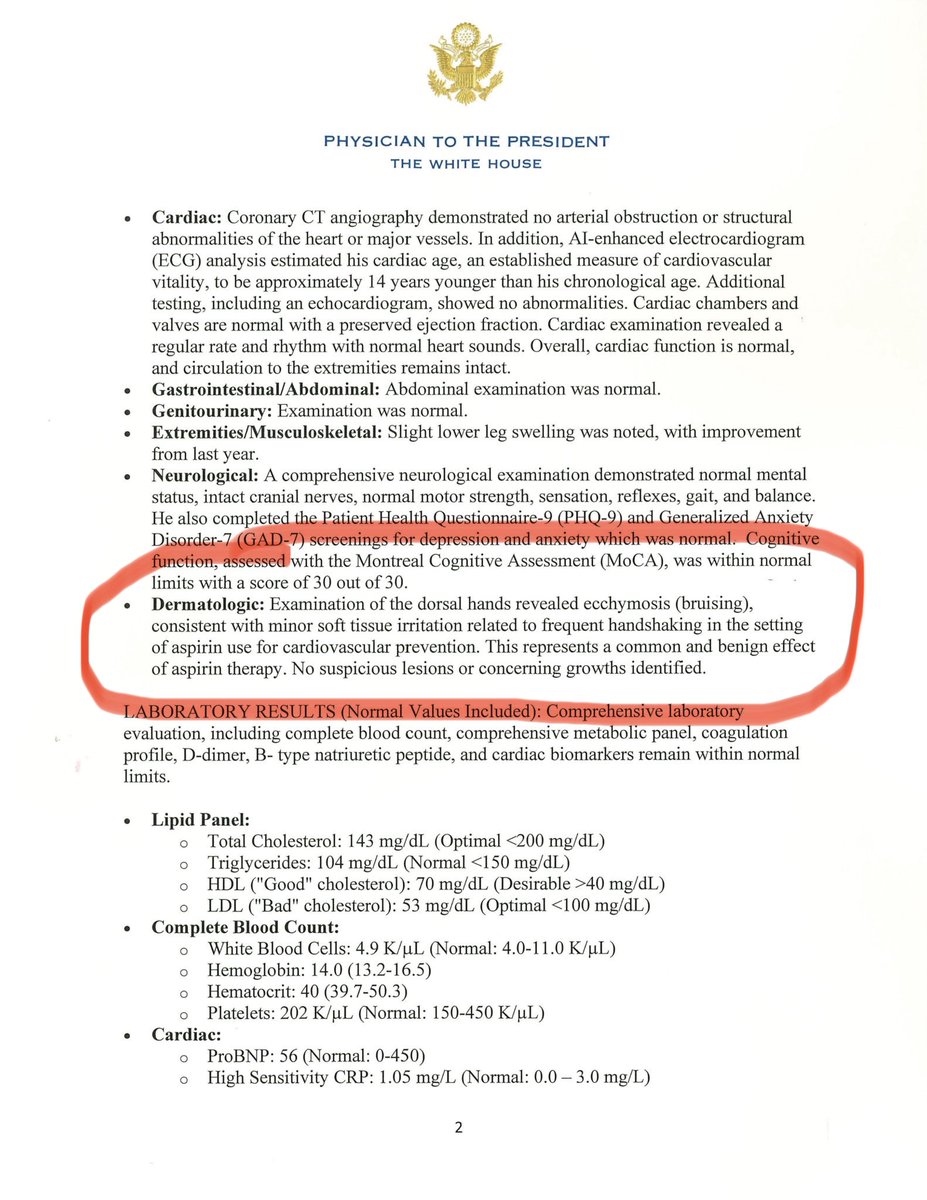
I thought that routine daily aspirin is no longer recommended for the primary prevention of heart attacks and strokes
Please advise @American_Heart #USPSTF
63
23
440
185,966