
Science & medicine communicator. Exposing the misinformation that harms health—and the evidence that protects you from it.
Joined August 2011
- Tweets 106,249
- Following 6,176
- Followers 9,163
- Likes 99,325
19,298 Photos and videos










IntegralAnswers retweeted

A compilation of moments between animals and humans
58
1,493
11,358
196,091

The two best-selling brain supplements have the weakest evidence on this list. The strongest data belongs to a cheap fish-oil dose and a prescription you already know.
7 nootropics, ranked by how strong the HUMAN trial evidence is, not how loud the marketing is.
1. Omega-3 (DHA and EPA). The only one with moderate-grade trial evidence. Across 24 RCTs and 9,660 people, a real but small gain in executive function, showing up above about 500 mg a day. More isn't better: very high doses bring their own heart-rhythm risk.
Caveat: the famous "30% lower Alzheimer's risk" is from population studies, not trials, and the big prevention trial in healthy elders found nothing. Best of a humble bunch.
2. Modafinil. A prescription-only wakefulness drug, Schedule IV controlled in the US, not something you can buy. The one compound here with a clean pooled positive in rested people, and it's tiny: average effect size 0.12 across 14 trials, mostly on hard executive tasks. It's on the list for evidence strength, not as something to go take. It may even dull creative thinking.
3. Caffeine plus L-theanine. A real, repeatable attention boost, but read the fine print: every trial is a single dose, in young adults, measured for about two hours. A review of 49 trials puts the attention effect at a modest 0.33. Cheap and reliable for the next two hours. Not a proven daily upgrade.
4. Creatine. A small memory signal, mostly in older adults. But Europe's food-safety regulator reviewed it in 2024 and rejected the cognition claim outright, and the largest "win" meta double-counts participants. In young healthy people the effect is zero.
5. Bacopa monnieri. Nine trials, 437 people, twelve weeks minimum. The effect is real but narrow: it speeds up attention, it doesn't boost memory. Expect stomach upset, the main reason people quit.
6. Lion's mane. One small win (30 older adults with mild impairment) that vanished four weeks after they stopped taking it. A 2025 trial in healthy young adults came back mixed and inconclusive, no clear overall benefit. Huge data in mice. Thin, messy data in people.
7. Ginkgo. The most thoroughly disproven supplement on this list. 3,069 people, six years, 120 mg twice a day: 277 got dementia on ginkgo, 246 on placebo. A second trial in 2,854 people agreed. Cochrane, 36 trials, calls the benefit "inconsistent and unreliable." Safe enough if you're not on blood thinners. It just doesn't work.
Fish oil and modafinil have the best data. The two on the front shelf have the worst.

7
4
39
2,511
IntegralAnswers retweeted

35
4
5
782

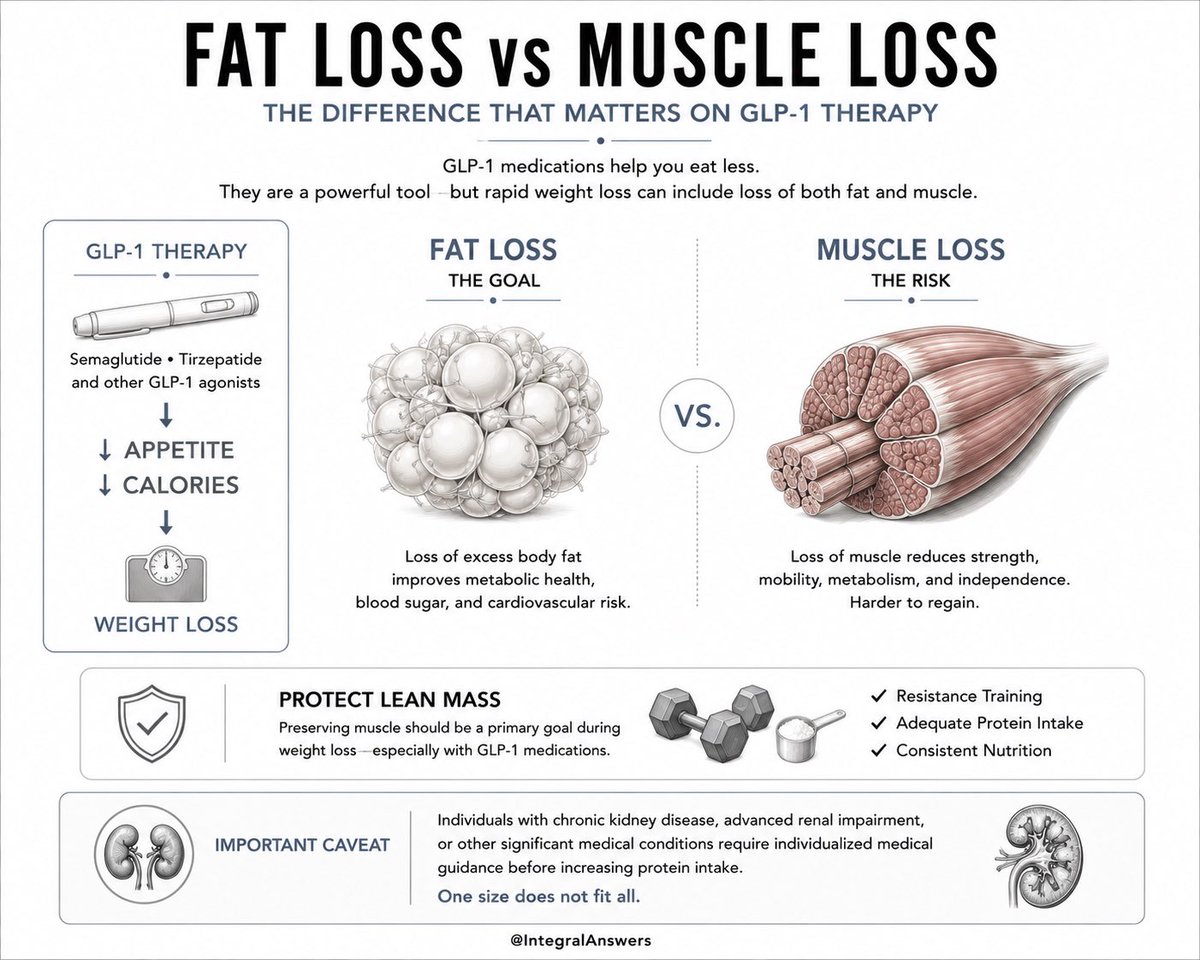
1/ GLP-1 Users Who Are Weight Training
The conversation changes when GLP-1 drugs enter the picture.
Semaglutide.
Tirzepatide.
Retatrutide.
These drugs help people eat less.
That’s the point.
But rapid weight loss can include loss of:
• Fat
• Muscle
Preserving muscle becomes one of the most important goals of treatment.
Protein and resistance training become strategic tools—not optional extras.
2
1
4
337
3/ The real objective of GLP-1 therapy is not merely becoming lighter.
It’s improving body composition.
The ideal outcome:
Less fat.
More preserved muscle.
Better metabolic health.
Resistance training plus adequate protein appears to be the most evidence-supported strategy currently available.
Important caveat:
Patients with chronic kidney disease, advanced renal impairment, or other significant medical conditions require individualized medical guidance before increasing protein intake.
One size does not fit all.
1
3
131
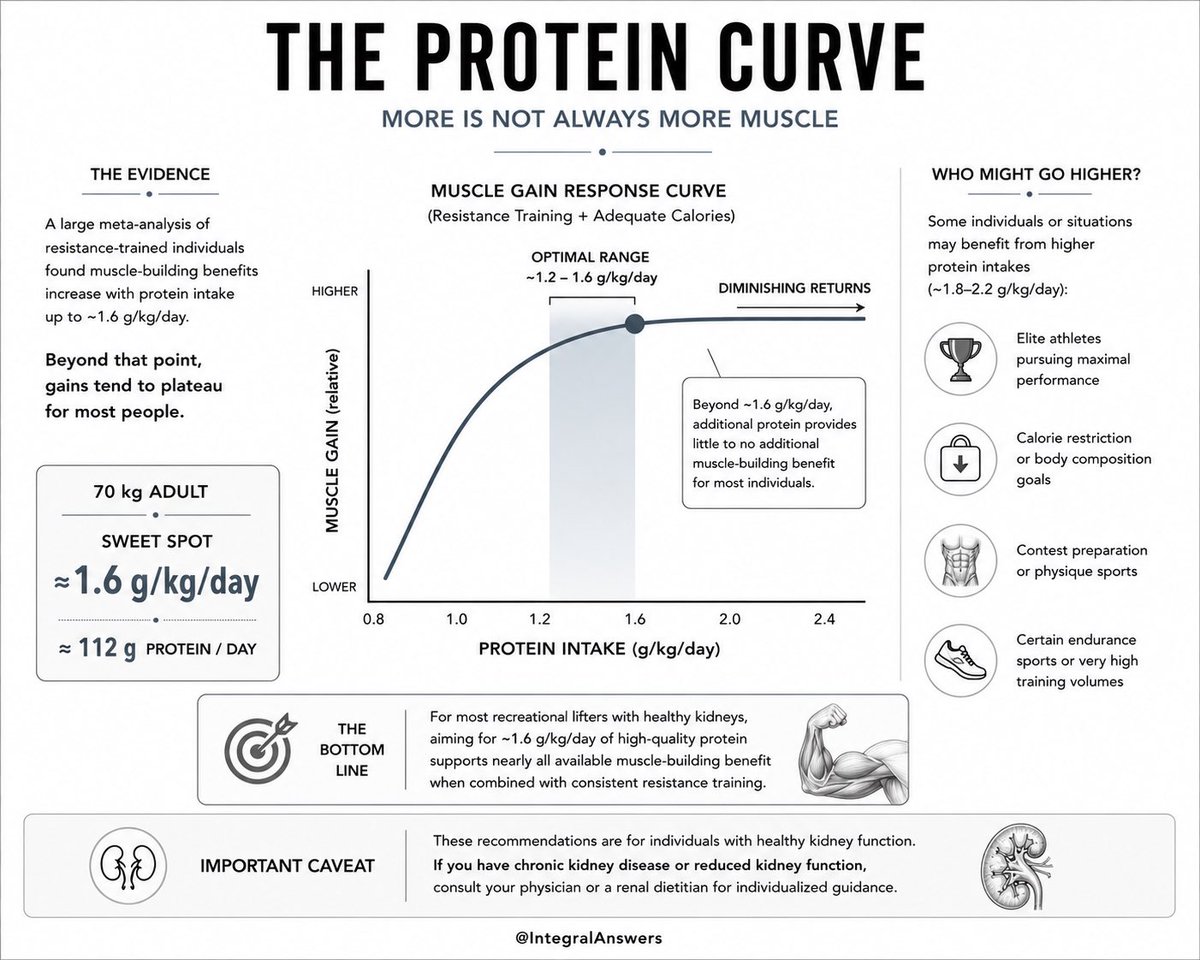
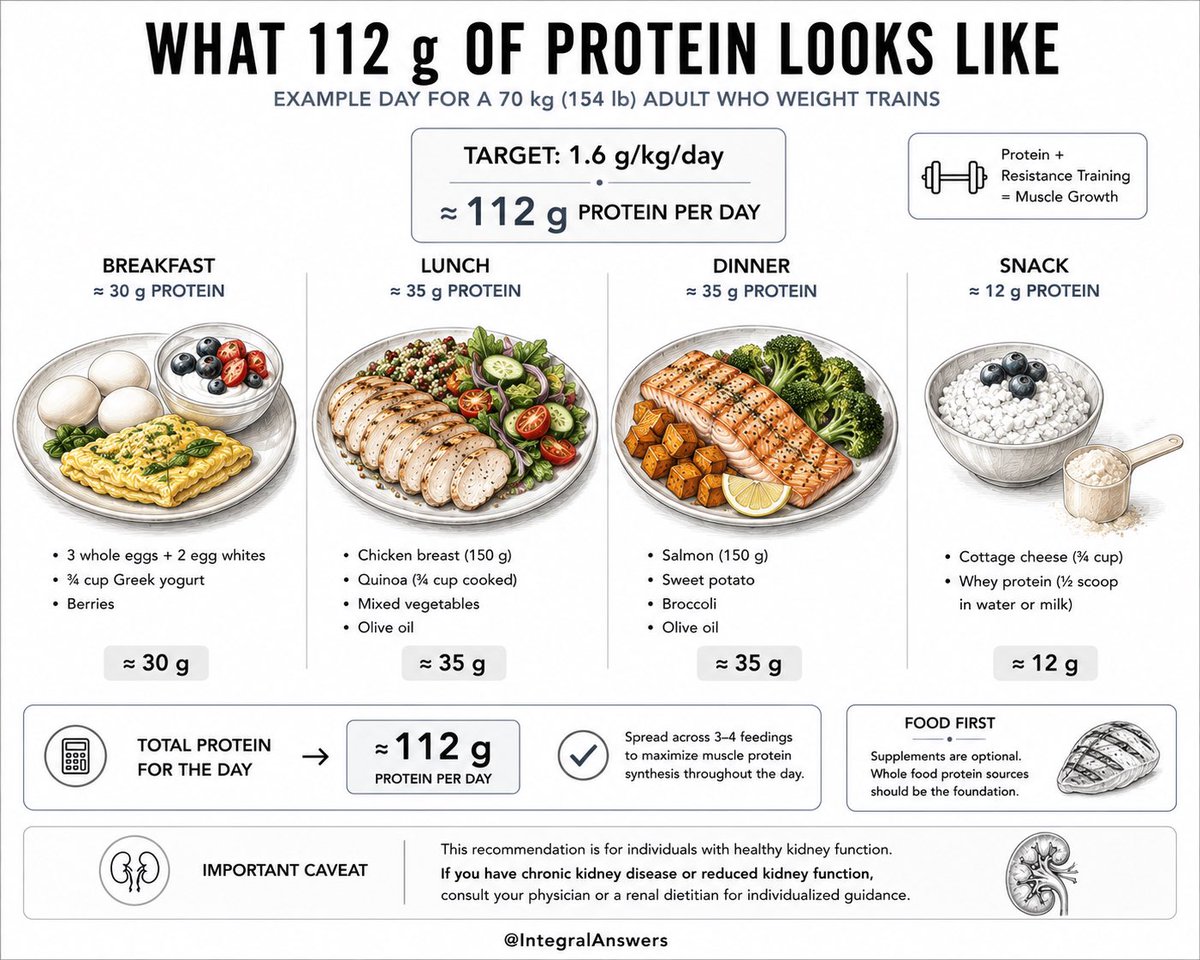
1/ Adults Who Weight Train
Once resistance training enters the picture, protein requirements change.
The best available evidence suggests muscle-building benefits rise with increasing protein intake up to roughly:
1.6 g/kg/day
Beyond that point, gains tend to plateau for most individuals.
More protein is not always more muscle.
This finding comes from one of the most influential meta-analyses in sports nutrition.
The evidence points toward a sweet spot—not an endless upward curve.
2
1
267
3/ Athletes pursuing maximal performance sometimes consume:
1.8–2.2 g/kg/day
But evidence suggests most recreational lifters achieve nearly all available benefit closer to:
1.6 g/kg/day
More isn’t necessarily harmful for healthy kidneys.
It may simply provide diminishing returns.
Exceptions:
• Elite athletes
• Calorie restriction
• Contest preparation
• Certain endurance sports
The goal should be evidence-based adequacy—not social media excess.
1
129
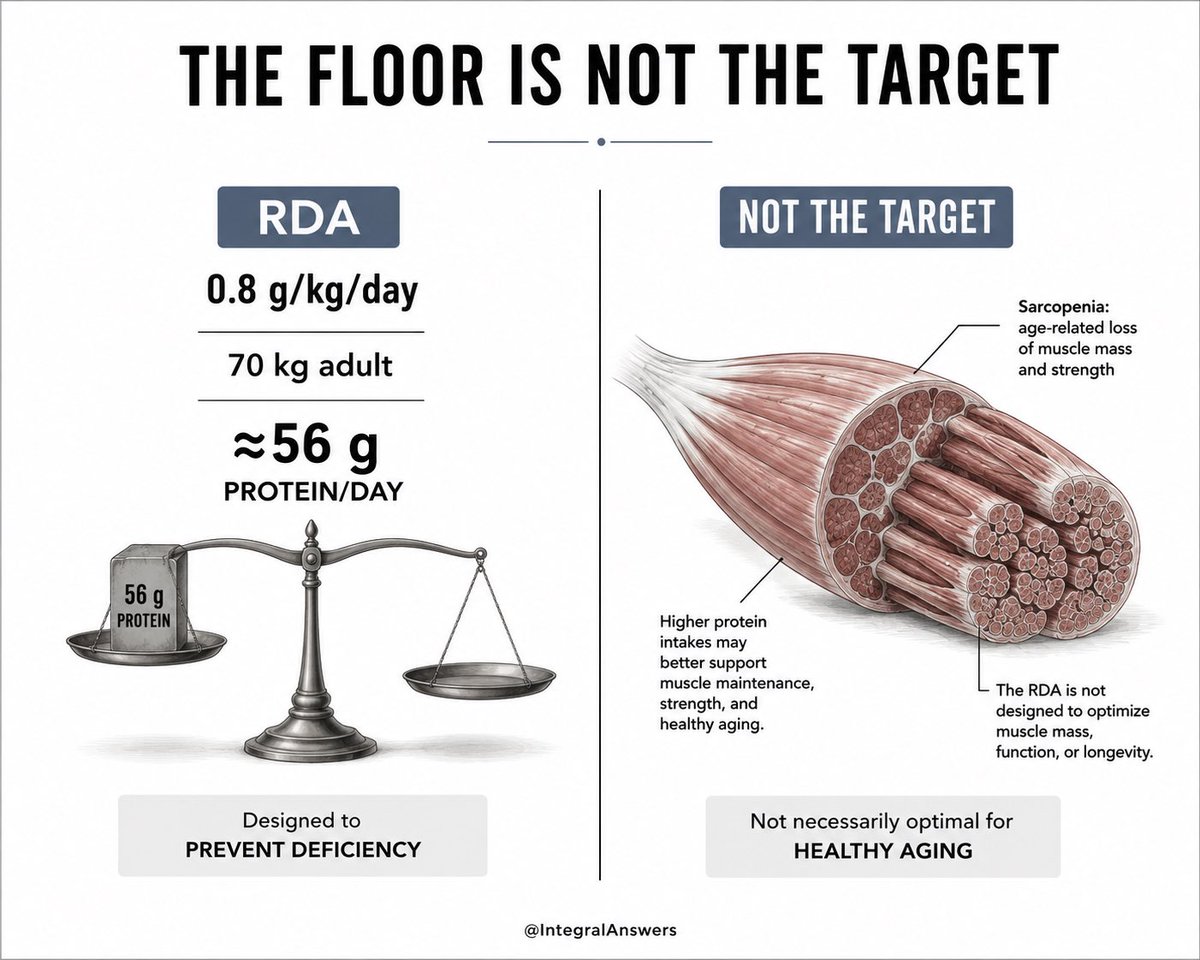
1/ Healthy Adults Seeking Healthy Aging
The protein RDA (0.8 g/kg/day) is one of the most misunderstood numbers in nutrition.
It was designed to prevent deficiency—not optimize health, muscle retention, strength, or healthy aging.
For a 70 kg (154 lb) adult:
• RDA = 56 g/day
That may be enough to avoid deficiency.
It is not necessarily enough to maintain muscle mass over decades.
As we age, skeletal muscle becomes one of our most important metabolic organs—supporting glucose disposal, mobility, balance, independence, and resilience.
The question is not:
“What’s the least protein I can survive on?”
The question is:
“What amount best supports healthy aging?”
Current evidence suggests those are very different numbers.
2
1
5
320
3/ Protein quality matters.
Protein timing probably matters.
Resistance exercise matters.
But for most healthy adults, the biggest mistake is simply under-consuming protein earlier in the day.
A practical approach:
• Protein at breakfast
• Protein at lunch
• Protein at dinner
Rather than consuming nearly everything at night.
Caveat:
Individuals with chronic kidney disease should not automatically increase protein intake without medical supervision.
Healthy kidneys and diseased kidneys are not the same situation.
Personalization matters.

1
2
128



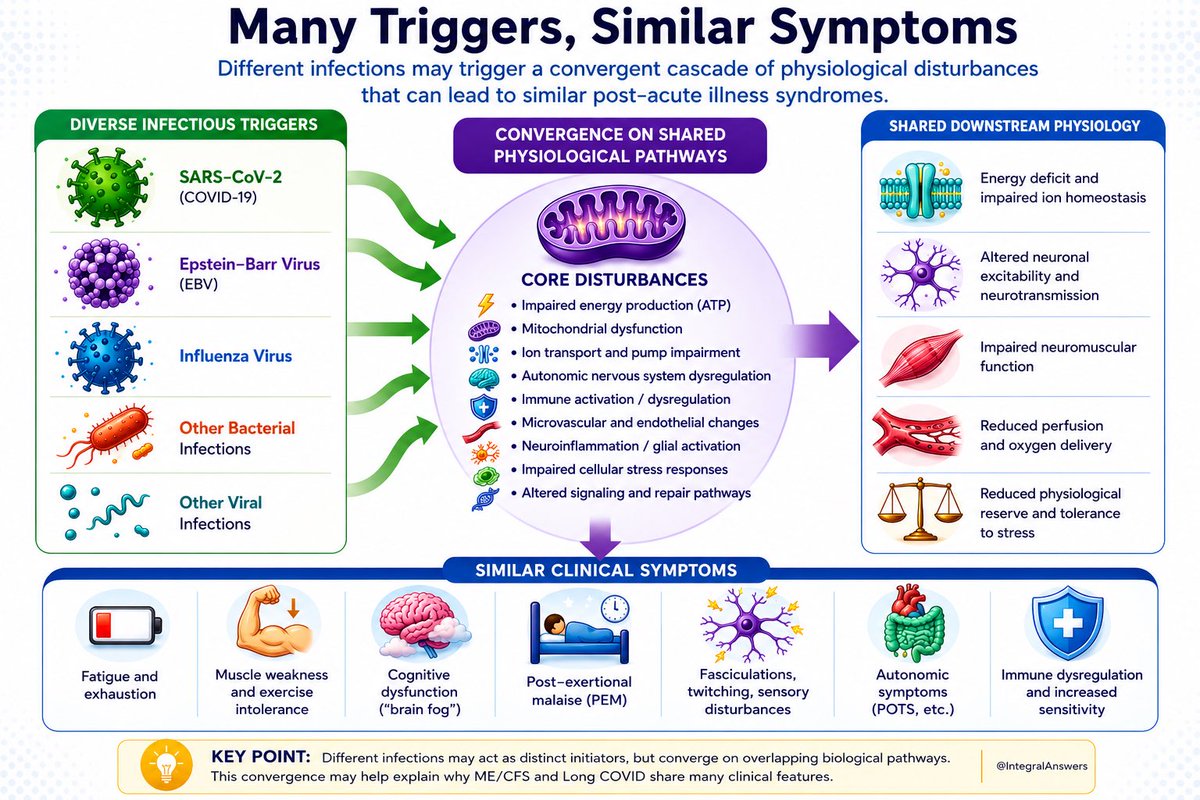
One of the most interesting emerging ideas in post-infectious illness research is that many different infections may trigger similar downstream biological disturbances, producing remarkably similar symptom patterns despite very different initial pathogens.
This is still a hypothesis—not a settled fact—but the evidence supporting biological convergence continues to grow.
SARS-CoV-2. Epstein-Barr virus. Influenza. Q Fever. West Nile Virus. Ross River Virus. Various bacterial infections.
Different pathogens. Different tissues. Different immune responses.
Yet many patients develop a strikingly similar syndrome characterized by:
• Fatigue
• Post-exertional malaise (PEM)
• Cognitive dysfunction (“brain fog”)
• Dysautonomia/POTS
• Exercise intolerance
• Sleep disturbances
• Sensory symptoms
What if the pathogen is not the whole story?
Several recent reviews suggest that diverse infectious triggers may converge upon a limited number of vulnerable physiological systems.
Among the repeatedly identified candidates:
🔹 Mitochondrial dysfunction and impaired ATP production
🔹 Endothelial and microvascular dysfunction
🔹 Autonomic nervous system dysregulation
🔹 Neuroinflammation and glial activation
🔹 Persistent immune activation
🔹 Altered cellular stress-response pathways
Komaroff and colleagues have argued that Long COVID, ME/CFS, and other post-acute infection syndromes share many of these abnormalities, including mitochondrial dysfunction, endothelial dysfunction, immune dysregulation, and autonomic disturbances. (PubMed)
The mitochondrial story is particularly intriguing.
Independent reviews in both Long COVID and ME/CFS describe evidence for impaired oxidative phosphorylation, reduced ATP generation, altered metabolic flexibility, oxidative stress, and abnormalities in cellular energy production. (PMC)
This matters because virtually every symptom reported by patients—fatigue, exercise intolerance, cognitive dysfunction, autonomic instability—depends heavily on adequate energy availability at the cellular level.
The autonomic nervous system may represent another point of convergence.
Multiple studies have documented orthostatic intolerance, POTS-like syndromes, altered sympathetic/parasympathetic balance, and broader autonomic dysfunction in both Long COVID and ME/CFS. (Taylor & Francis Online)
Then there is post-exertional malaise (PEM)—arguably the most distinctive symptom shared by many patients.
Rather than simple deconditioning, emerging evidence suggests PEM may involve a complex interaction among mitochondrial dysfunction, immune activation, neuroinflammation, autonomic dysregulation, vascular abnormalities, and skeletal muscle pathology. (PMC)
This convergence model helps explain an observation clinicians have made for decades:
Patients often arrive through different doors—but end up in remarkably similar rooms.
An EBV-triggered illness may not be biologically identical to Long COVID.
An influenza-triggered syndrome may not be identical to ME/CFS.
But they may share enough downstream physiological disturbances that the resulting symptom patterns overlap substantially.
Importantly, none of this means we have found a single cause.
The current evidence points toward a network of interacting mechanisms rather than one master explanation.
Different patients may arrive at similar symptoms through different combinations of mitochondrial dysfunction, endothelial injury, immune dysregulation, autonomic dysfunction, neuroinflammation, and metabolic abnormalities.
The future of research may therefore be less about identifying “the pathogen” and more about understanding why different insults appear capable of converging on the same vulnerable biological systems.
If that hypothesis proves correct, it could reshape how we classify—and eventually treat—Long COVID, ME/CFS, and other post-infectious syndromes.
2
9
29
1,004
References:
• Komaroff et al., Frontiers (2023)
• Komaroff et al., Cell Reports Medicine (2025)
• Molnar et al., Mitochondrial Dysfunction in Long COVID (2024)
• Syed et al., Mitochondrial Dysfunction in ME/CFS (2025)
• Davis et al., Nature Reviews Microbiology (2023)
1
5
168