
Biomed Scientist in #longevity. Mentor & Investor in Health startups. Past CTO @BioVivaScience ,Researcher @CASMIORG ,Lead @oxfordscisoc @NewsInLongevity ,BGRF
- Tweets 8,450
- Following 2,755
- Followers 10,561
- Likes 6,367















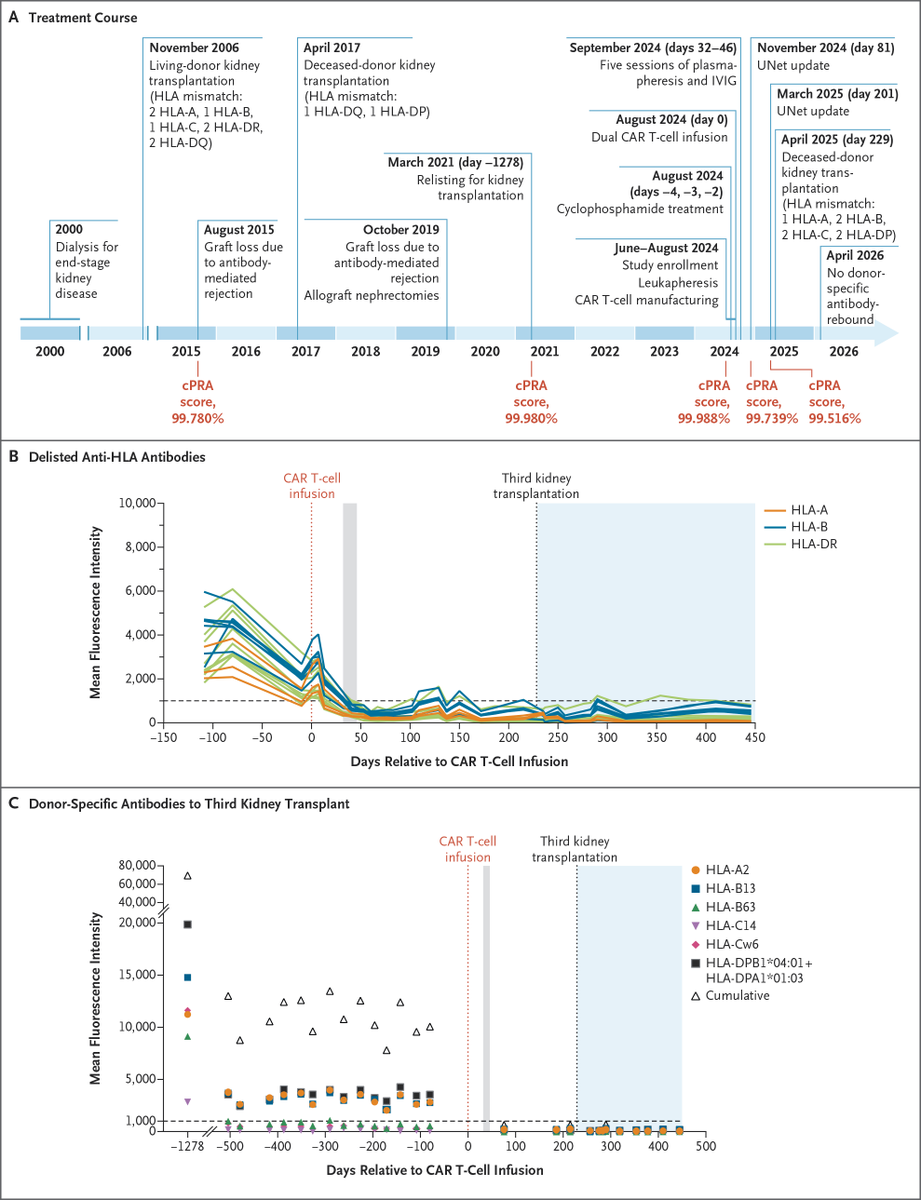
ALT This image presents a detailed timeline and graphs related to treatment course and anti-HLA antibody levels in Patient 1. A) Treatment Course Timeline: Shows the treatment course and calculated panel-reactive antibody (cPRA) scores before and after the infusion of chimeric antigen receptor (CAR) T cells in Patient 1. B) Delisted Anti-HLA Antibodies Graph: Displays levels of antibodies to HLA antigens that were eventually delisted in the patient, before and after the CAR T-cell infusion. C) Donor-Specific Antibodies to Third Kidney Transplant Graph: Shows levels of donor-specific antibodies to the third kidney transplant before and after the CAR T-cell infusion.
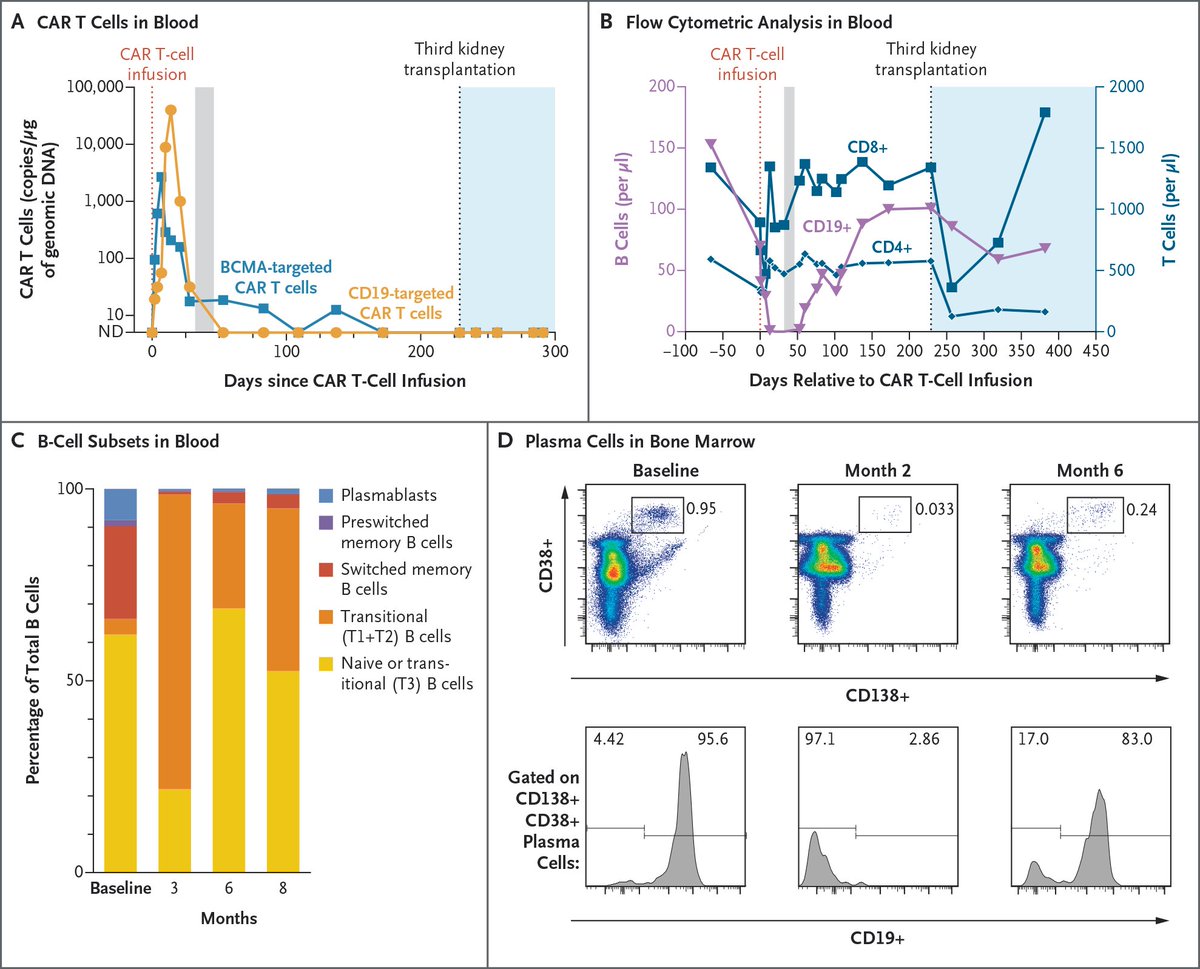
ALT This image consists of four panels showing CAR T-cell pharmacokinetics and pharmacodynamics in Patient 1. Panel A presents a line graph on the levels of CAR T cells in blood after the infusion. Panel B displays the results of flow cytometric analysis in blood before and after the CAR T-cell infusion, including levels of B cells and T cells. Panel C is a graph illustrating the distribution of B-cell subsets before and after the CAR T-cell infusion. In Panel D, the top row shows the percentage of plasma cells in total nucleated cells in bone marrow, and the bottom row shows the percentage of CD138 CD38 plasma cells with CD19 expression, before and after the CAR T-cell infusion.
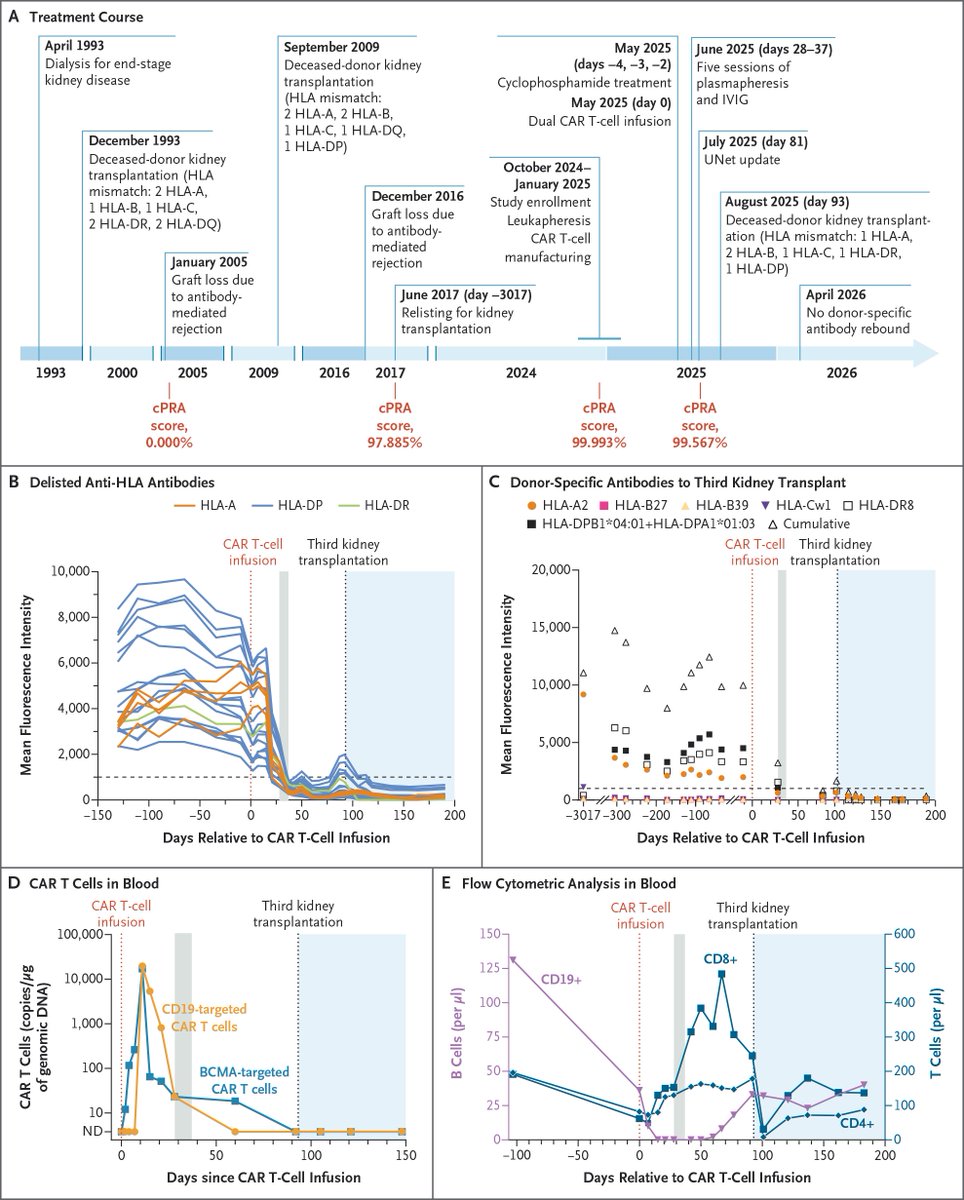
ALT This image features four graphs and a timeline related to treatment course, anti-HLA antibody levels, CAR T-cell levels, and flow cytometric analysis in Patient 2. The timeline in Panel A shows the treatment course and cPRA scores before and after the CAR T-cell infusion in Patient 2. The Panel B graph shows levels of antibodies to HLA antigens that were eventually delisted in the patient, before and after the CAR T-cell infusion. The Panel C graph shows levels of donor-specific antibodies to the third kidney transplant before and after the CAR T-cell infusion. The Panel D graph shows levels of CAR T cells in blood after the infusion. The Panel E graph shows the results of flow cytometric analysis in blood before and after the CAR T-cell infusion, including levels of B cells and T cells.
