
Interventional Cardiologist at National Cardiovascular Center Harapan Kita 🇮🇩
Joined April 2010
- Tweets 441
- Following 559
- Followers 234
- Likes 288
33 Photos and videos














Nanda Iryuza retweeted

May 10
complete video: details of the clockwise rotation (the burr stretches and pulls the guiding Cath in the coronary)
1
27
116
7,435
Nanda Iryuza retweeted

May 9
Here is my algorithm:
1) Vasodilator therapy (if hemodynamic allow and pull)
2) Pull Rotawire. This works very effectively, 90% of times. It is frequently overlooked. The 0.014 tip works as a great way to bring back the stuck burr. Make sure wire is free with brake off for maximal efficiency. Pulling the driveshaft is less effective, as it is made of 3 coiled wires which gives some elasticity to the driveshaft.
3) If burr is free beyond lesion, can use short dynaglide runs and then pull. Prinicple is that dynamic friction is lower. Don’t overdo this and also with skipping rope technique, there is risk of driveshaft breakage and burr loss due to torsional forces with a fix s immobile burr!
4) Cut driveshaft and remove teflon sheath
5) Deliver GE over driveshaft to the burr and pull.
6) Intimal/subintimal wire and ballooning to dislodge burr and pull.
7) Re-deliver GE over driveshaft and pull.
8) Obtain second access and adding a ping-pong guide. Remember a ping-pong guide is not required in most cases. Once Teflon sheath is removed, a 6F guide can accommodate: Driveshaft coronary wire, Driveshaft Caravel microcatheter, Driveshaft Corsair/Turnpike LP microcatheters, Driveshaft 2.5-4mm balloons
9) Combine subintimal ballooning and GE over driveshaft and pull. Only these maneuvers requires ping-pong guides.
10) Call surgeons.
4
33
107
11,600
Nanda Iryuza retweeted

A backtable illustration of a couple techniques you can use if the #Rotaburr gets stuck,
1-The skipping rope technique.
We have known it for a couple years, and it was recently published
onlinelibrary.wiley.com/doi/…
2-The final resort of cutting the rota driveshaft and advance a guideliner through it to get more leverage to pull.
Of course the first thing you do is to pull hard and maybe try to balloon around it, but those can help with tougher situations.
#CardioX community, please share your additional tips and comments
5
59
267
20,733
Nanda Iryuza retweeted

May 1
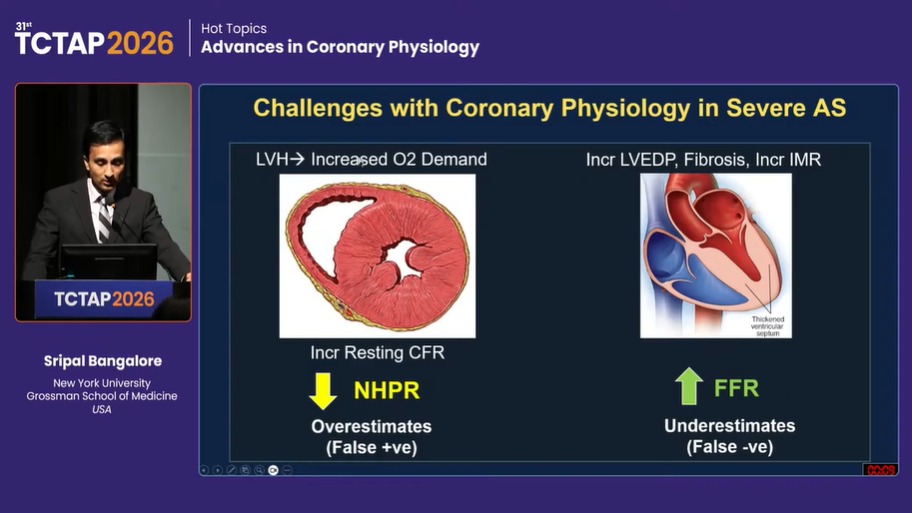
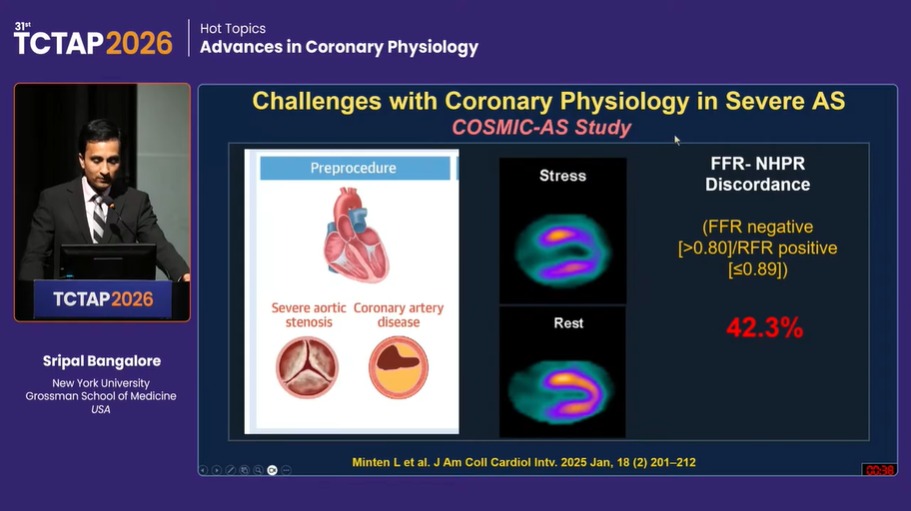
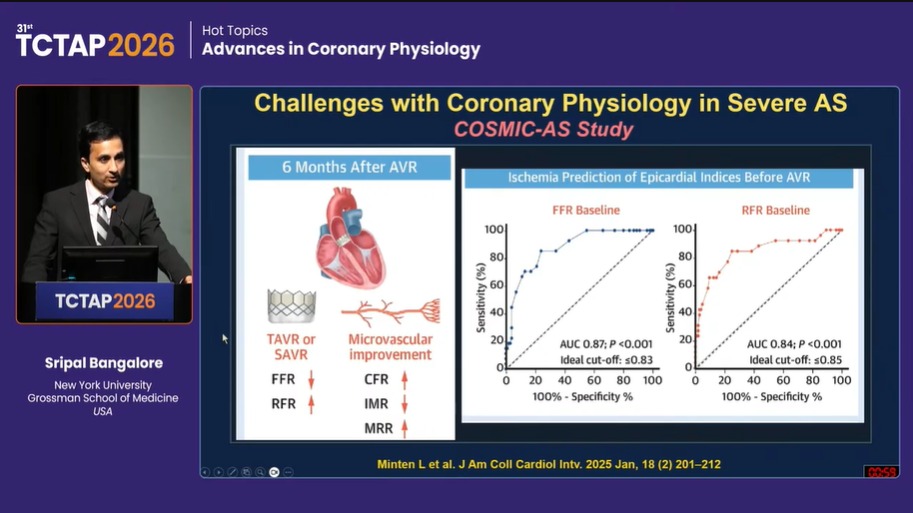
What are the Implications of Severe AS on Coronary Physiology ⁉️
💥Overestimation of NHPR: FALSE ➕️
💥Underestimation of FFR: FALSE ➖️
💥 ⬆️ in Prevalence of FFR-NHPR Discordance ~ upto 42.3 %
💥Defer PCI if iFR >0.85 or FFR >0.83
💥TAVR/SAVR improves physiology indices

May 1

#TCTAP2026
❤️🔥 Get ready to tune into a comprehensive coronary physiology session covering invasive & non-invasive tools—from FFR/NHPR discordance and MV testing to wire-based/wireless strategies, CT-FFR, and landmark trials; refining real-world decision-making in the cath lab.
2
27
72
7,796
Nanda Iryuza retweeted

Mar 6
7
33
126
89,992
Nanda Iryuza retweeted

🫀📉 Can more intensive LDL-lowering improve CT-FFR in stable chest pain?
This new JACC study evaluates whether intensive lipid-lowering therapy (statin ezetimibe) alters CT-derived fractional flow reserve (FFR-CT) — a noninvasive marker of lesion-specific ischemia — in patients with stable chest pain and coronary atherosclerosis.
🔍 Study essentials
Patients with stable angina and coronary plaque on CT angiography were managed with aggressive lipid-lowering using statins plus ezetimibe, targeting substantial LDL-C reduction. FFR-CT was measured at baseline and on follow-up to assess functional changes in coronary physiology attributable to therapy.
📈 Key message
The core focus — integrating structural and functional imaging — points to a key concept: lipid-lowering can potentially improve lesion physiology, not just plaque burden. By using FFR-CT (a validated surrogate for invasive FFR), the authors are examining whether aggressive LDL-reduction actually shifts physiological indices toward less ischemia.
🧠 Why this matters
Lipid-lowering benefits have traditionally been shown at the event level (MI, death).
Structural plaque regression with statins/ezetimibe is documented in IVUS and CT studies.
But fewer data exist on functional improvement in coronary blood flow with therapy.
Linking lipid therapy to improved FFR-CT suggests that LDL-lowering may not only slow plaque progression but also improve coronary physiology — a potential mechanistic bridge to clinical benefit.
📌 Bottom line:
Intensive lipid-lowering might influence not only plaque morphology but lesion-specific ischemia as assessed noninvasively, expanding our understanding of how therapies translate into physiological improvement.
3
18
59
20,854
Nanda Iryuza retweeted

Feb 9
Wonderful to host @Iryuza our interventional fellow from Indonesia who has been with us for the past year for a PCI / TAVI fellowship . It is his last week with us and has been a joy to have him here. Looking forward to a long collaboration with many more fellows

5
5
99
4,407

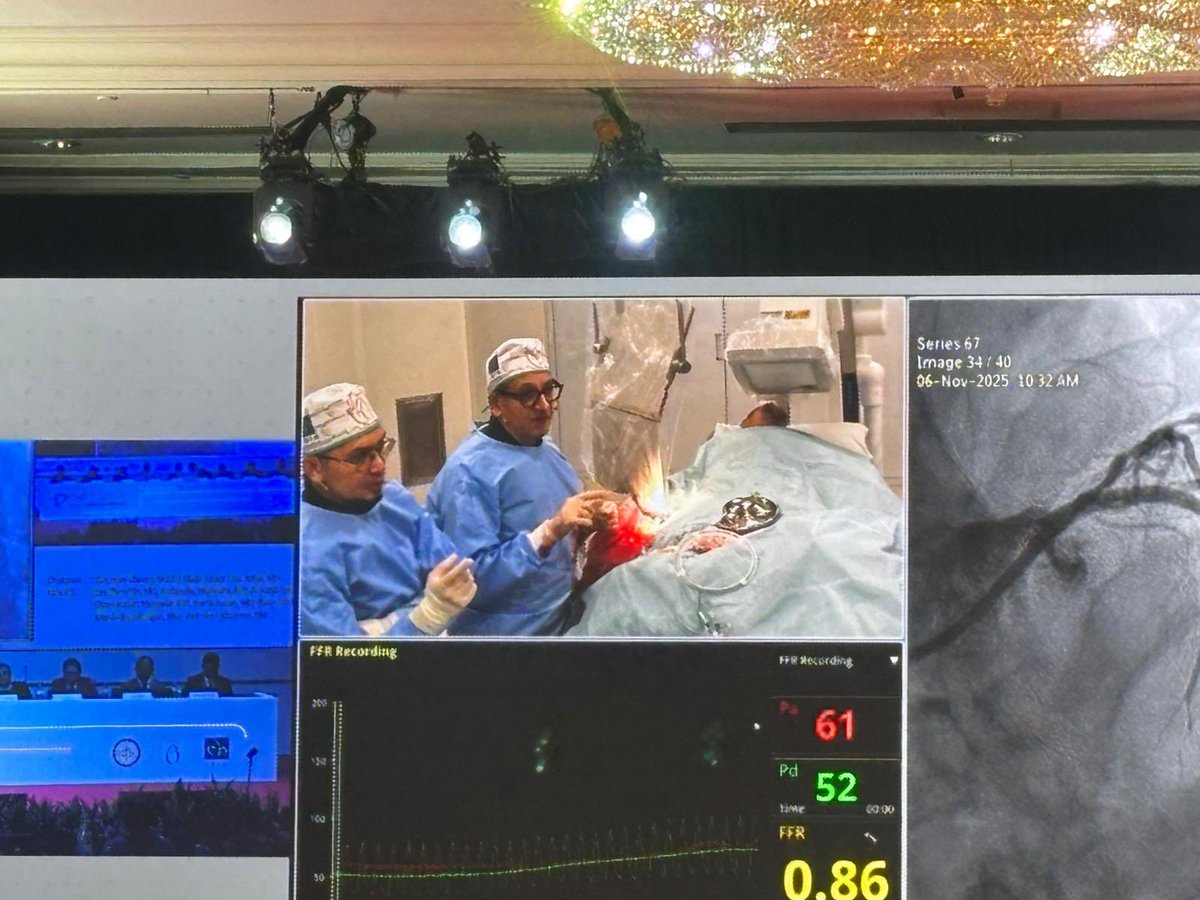
10 Nov 2025
Great honor to have my mentor, Prof. @mmamas1973 in Jakarta for ISICAM! Proud to do a successful live case together at the National Cardiovascular Center Harapan Kita. Educational, inspiring, and memorable. Hope you enjoyed the event!
@ISIC_Official @aninkasaboe



2
5
9
1,718
Nanda Iryuza retweeted
7 Nov 2025
Great evening at #ISICAM gala dinner with dancing, singing 😬 and friends @aninkasaboe @Iryuza @uziyahya46 teguh santoso @Laserrman
What a great meeting, the warmth friendliness and joy of the Indonesian doctors is the best




2
11
48
3,885
Nanda Iryuza retweeted
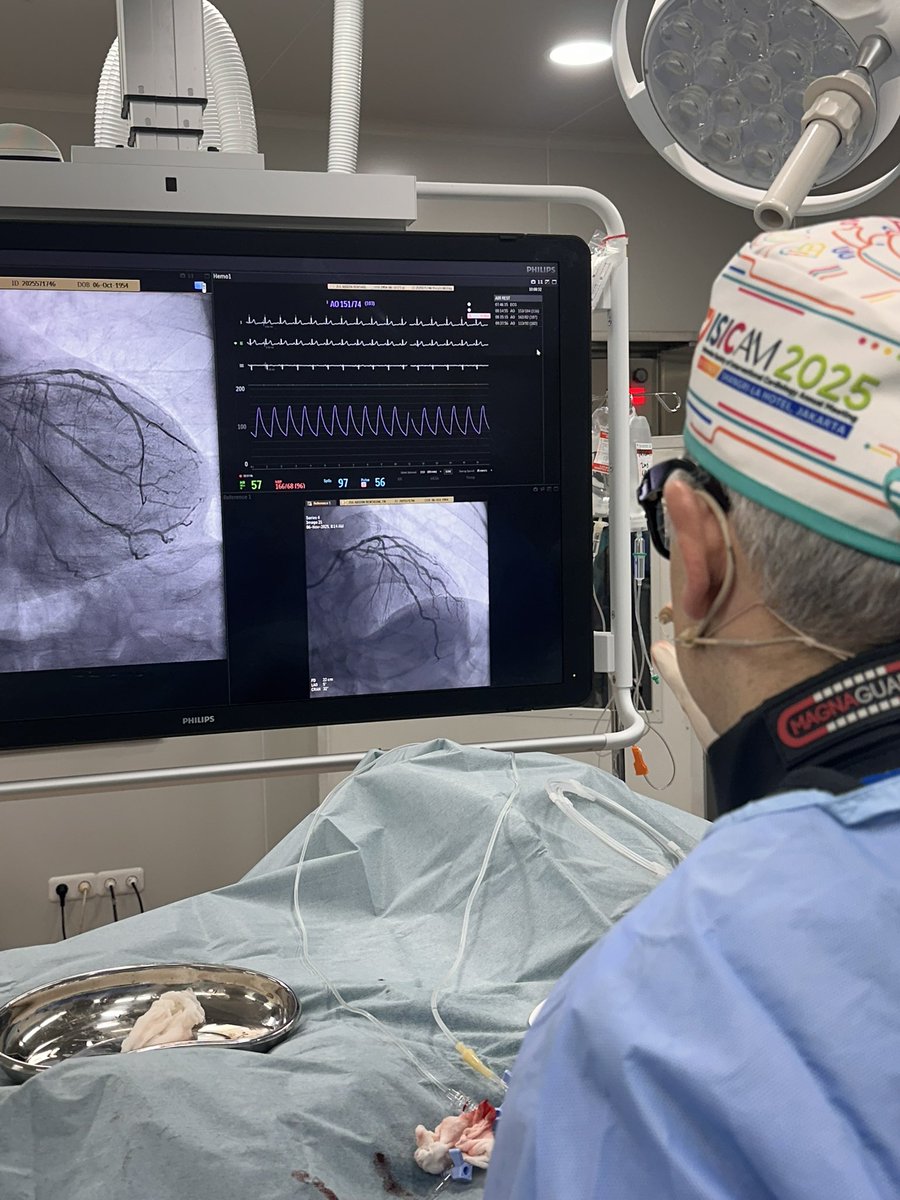
6 Nov 2025
Great to do opening live case at #ISICAM with medina 1.1.1 lms disease and diffuse lad disease.
Oct and physiology guided provisional hybrid approach with prox lad stent into lms, then cutting balloon guided seloution dcb in mid lad with @Iryuza
@aninkasaboe @uziyahya46 @mirvatalasnag


3
10
67
10,313
Nanda Iryuza retweeted

26 Oct 2025
💡 See Beyond the Vessel — Master Coronary Physiology!
Join our hands-on Workshop on Physiology and learn how to guide treatment & optimize outcomes through evidence-based physiology and imaging integration.
🗓 Wed, 5 Nov 2025 | 🕐 13.00–17.00 WIB
📍 Jawa Room, Shangri-La Jakarta
🔗 Register now at isicam.id
#ISICAM2025 #StayOnTrack
@uziyahya46 @Iryuza

1
1
468
Nanda Iryuza retweeted
26 Oct 2025
🔥 Hidden Dangers, Visible Impact!
High-risk plaques may stay silent — until it’s too late.
Discover how advanced imaging transforms early detection into life-saving action.
📅 Fri, 7 Nov 2025 | 🕚 11.00–12.00 WIB
📍 Ballroom A, Shangri-La Jakarta
🚀 Don’t miss your next breakthrough — register now at isicam.id
#ISICAM2025 #StayOnTrack
@uziyahya46 @mmamas1973 @RoccoVergallo @IndahSP_MD et al.

5
5
1,034
Nanda Iryuza retweeted

17 Sep 2025
Pinned: Cardiovascular Physiology Hub
Discovering physiology together: untangling the concepts most often misunderstood at the bedside.
Foundations
– Starling’s law as servo-control x.com/icmteaching/status/194…
– Cardiac output & Anderson’s model x.com/icmteaching/status/193…
– Preload x.com/icmteaching/status/194…
– Making sense of acid–base x.com/icmteaching/status/195…
– Afterload & systemic vascular resistance x.com/icmteaching/status/196…
Concepts in flow & pressure
– Critical closing pressure & waterfalls (series)
• Part 1 x.com/icmteaching/status/195…
• Part 2 x.com/icmteaching/status/195…
– High-output heart failure x.com/icmteaching/status/196…
– Why is CVP in the MAP equation? x.com/icmteaching/status/195…
– Tissue perfusion x.com/icmteaching/status/194…
Frameworks & applied physiology
– Shock: pump vs pipes framework x.com/icmteaching/status/195…
– Interface model of shock x.com/icmteaching/status/194…
– Cardiac output monitors x.com/icmteaching/status/194…
– Sepsis does not cause hypovolaemia x.com/icmteaching/status/193…
Why RCTs fail (3-part series)
– Part 1: Consensus, thresholds & physiology x.com/icmteaching/status/196…
– Part 2: Heterogeneity vs colliders x.com/icmteaching/status/196…
– Part 3: Beyond colliders x.com/icmteaching/status/196…
I’ll keep adding here as new threads drop.
27 Jun 2025

1/
Most people think the heart drives circulation.
But what if that’s backwards?
Anderson’s model flips the whole idea of cardiac output on its head — and it changes how you think about fluid, flow, and failure.
🧵👇
#physiology #FOAMed #MedTwitter #criticalCare #cardiacOutput
3
60
179
40,064
Nanda Iryuza retweeted

13 Sep 2025
Planning a PBMV? Don’t start without this!
Dr. Walsh shares a concise, practical prep guide easy to bookmark and refer back to.
#CardioTwitter #CardioX #CathLab
2
18
93
9,219
Nanda Iryuza retweeted

27 Jun 2025
Nonculprit Vulnerable Plaques and Prognosis in Myocardial Infarction With Versus Without ST-Segment Elevation: A PROSPECT II Substudy: @CircAHA
🥸 Rx of nonculprit lesions in STEMI or NSTEMI: @GreggWStone
😱 Summary
👇👇👇

2
34
126
13,583
Nanda Iryuza retweeted

25 May 2025
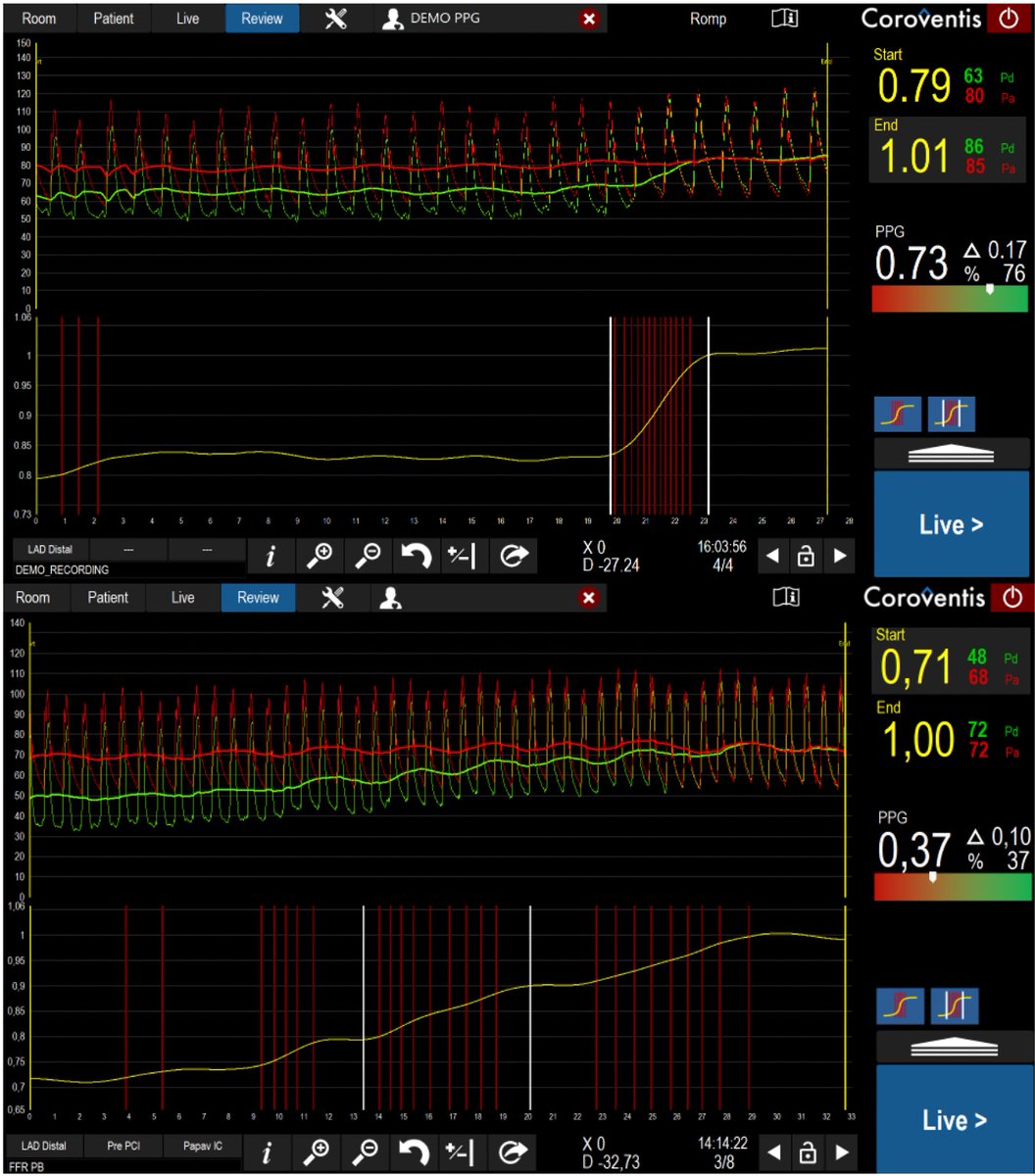
This is the new #PPG Pullback Pressure Gradient - a new physiology-based paradigm in coronary decision-making
High PPG = focal CAD / Low PPG = diffuse CAD
We hope PPG helps us become better interventional cardiologists🙏
@PCRonline @AbbottCardio @coroventis @TCTMD @CoreAalst
5
37
108
6,996
Nanda Iryuza retweeted

2 Apr 2025
TIMI Flow: A Key Indicator of Coronary Perfusion
TIMI (Thrombolysis in Myocardial Infarction) flow grading is a crucial angiographic tool to assess blood flow in coronary arteries, particularly after an intervention like PCI.
🔹 TIMI 0 (No Flow) – Complete occlusion; no antegrade flow beyond the blockage.
🔹 TIMI 1 (Penetration without Perfusion) – Minimal flow beyond the occlusion but without adequate distal vessel opacification.
🔹 TIMI 2 (Partial Flow) – Delayed but complete filling of the distal vessel; flow is slower than normal.
🔹 TIMI 3 (Normal Flow) – Full, brisk perfusion with normal distal vessel filling, comparable to a non-diseased artery.
TIMI 3 flow is the gold standard for successful reperfusion in PCI, improving outcomes in STEMI and other coronary syndromes.
#Cardiology #TIMIFlow #CathLab
94
330
18,462
Nanda Iryuza retweeted

1 Apr 2025
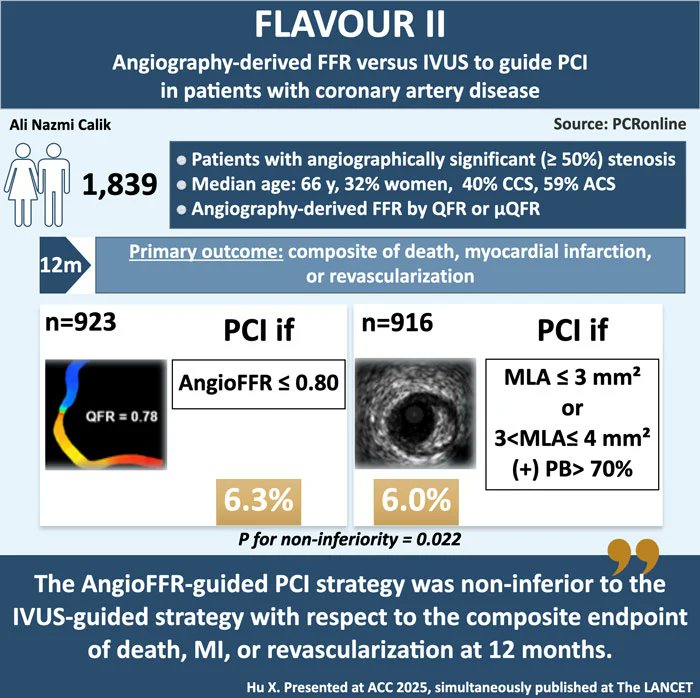
🔥#ACC25 Late-Breaking Trials 🔥: FLAVOUR II
🔗pcronline.com/News/Whats-new…
@ANazmiCalik provides his take ✍️ on this trial of angiography-derived #FFR versus intravascular ultrasound to guide PCI in patients with coronary artery disease
#interventionalcardiology #Clinicaltrial #cardiotwitter
26
45
8,878

Bifurcation Cases With OCT and Coronary CT-OCTOBER and P4 Trials x.com/i/broadcasts/1MYxNwewB…
15
47
7,630
Nanda Iryuza retweeted

8 Dec 2024
🚨Dr. Bernard De Bruyne’s @BernardBruyne Physiology Masterclass episode is now live! 🚨
Learn how coronary physiology is helping us understand plaque rupture. 🫀💥
What stood out to you in this episode? Let us know in the comments!👇
Want to watch the previous Physiology Masterclasses? Find them all here: coreaalstplatform.com/coreaa…
@EmanueleBarba13 @ColletCarlos @SimoneBiscaglia @jeroen_sonck @CardioAalst @OLVZaalst
#Cardiology #PhysiologyMasterclass #FocalDisease #DiffuseDisease
1
12
28
2,200