
ambulance verpleegkundige, student physician assistant, dad of 3 🧍🏼♀️,alpinism, running, training, ECG‘s ,neurology, fan of FOAM, life long learning,
Joined December 2018
- Tweets 4,292
- Following 1,432
- Followers 538
- Likes 16,215
186 Photos and videos









Pinned Tweet

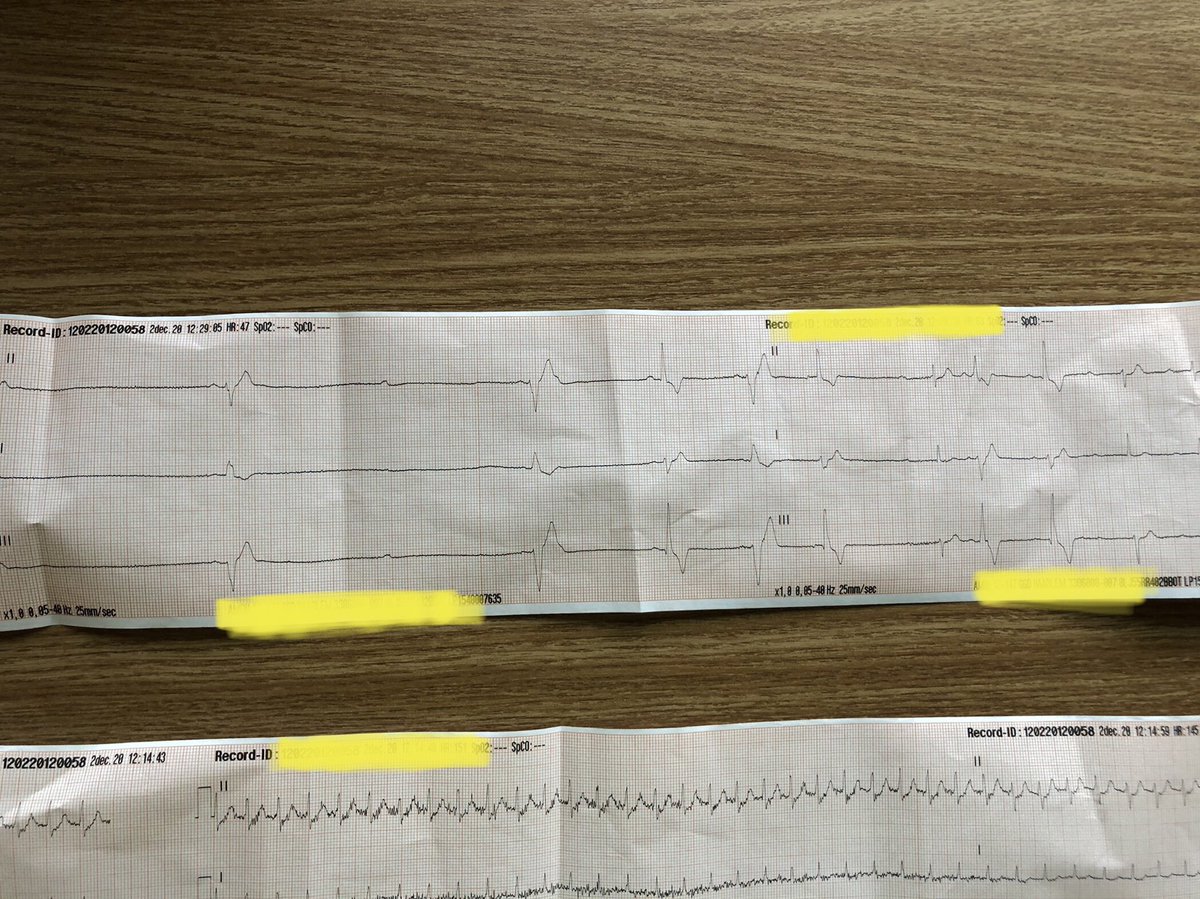
2 Dec 2020
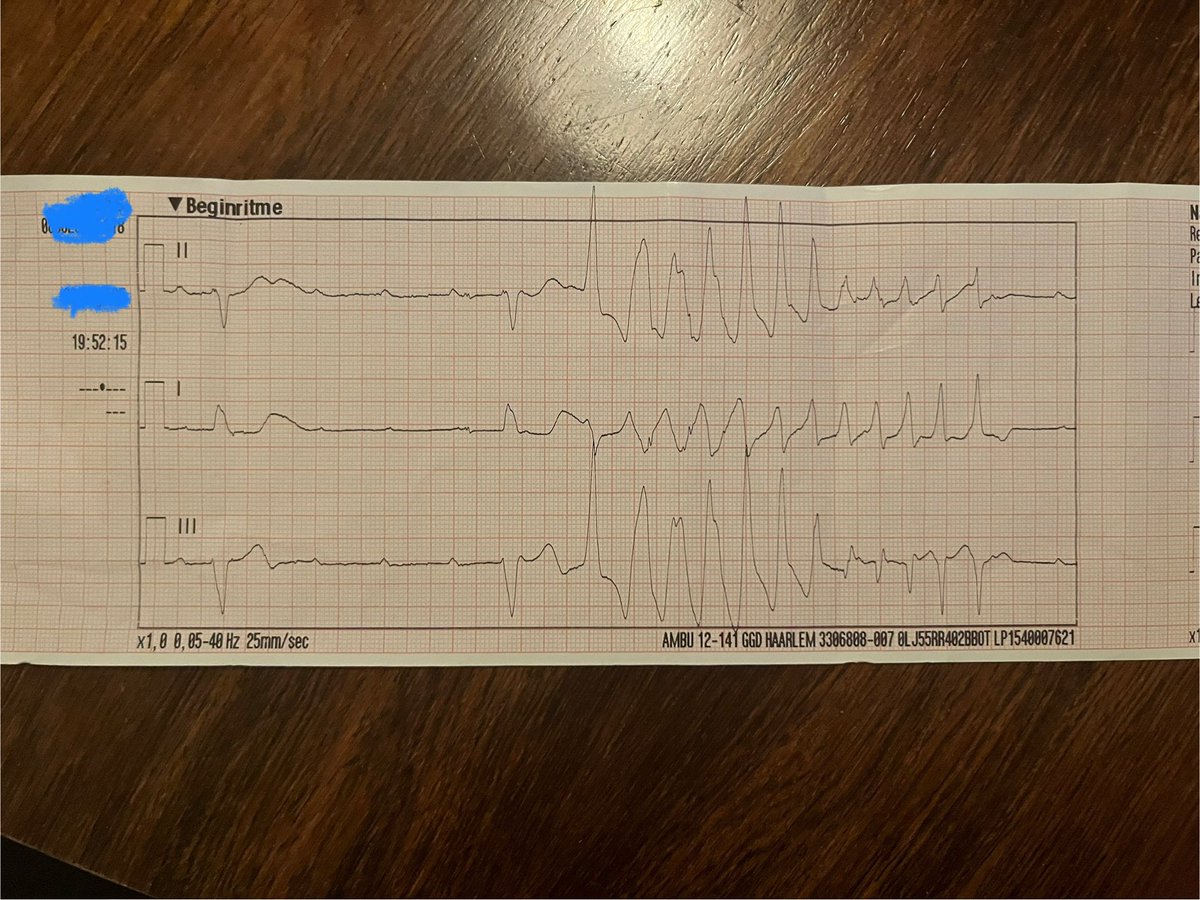
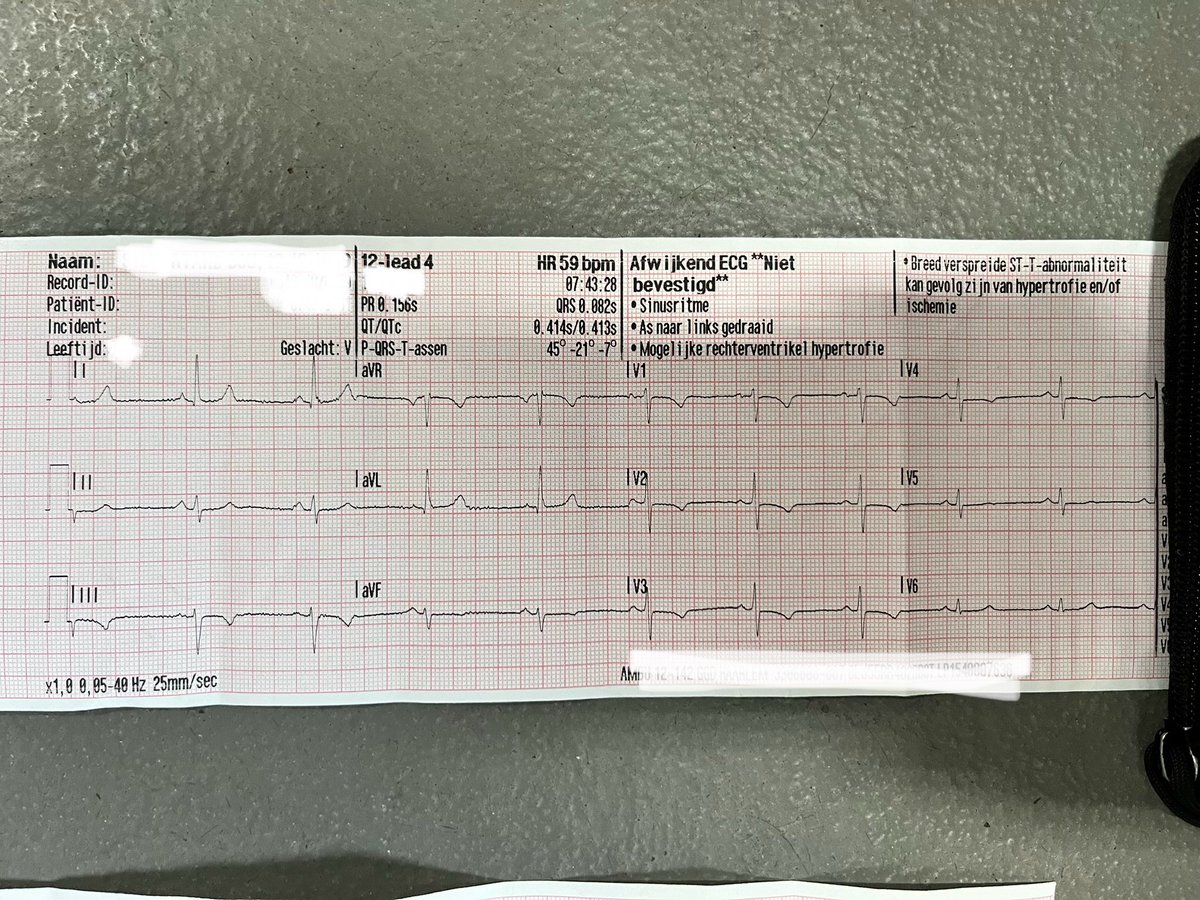
A f 87yo experiences chest thightness during shuffleboard.. first one since the #covid19 outbreak
➡️phx MI, HT
➡️med🤷♂️
➡️ RR 100/60, m #valvalsa👎🏻
➡️ adenosine 6mg👎🏻 12mg😁—-> ST/SR 🤙🏻
➡️🤯... did not appreciated the feeling🤮
#epeeps #ecgtwitter #FOAMed

4
2
23
Jorik Sweenen retweeted

May 23
Tunnelvisie is niet zo makkelijk bij te stellen. Zeker niet wanneer het ook nog geïntegreerd is met identiteit. ewmagazine.nl/kennis/achterg…
2
11
43
2,037
Jorik Sweenen retweeted

Apr 24
Help mee zoeken:L #Retweet
Maxim (14) al dagen vermist; speciaal zoekteam vindt geen enkel spoor
gld.nl/nieuws/8466173/maxim-…
#NieuwsInPerspectief
3
344
166
5,428
Jorik Sweenen retweeted

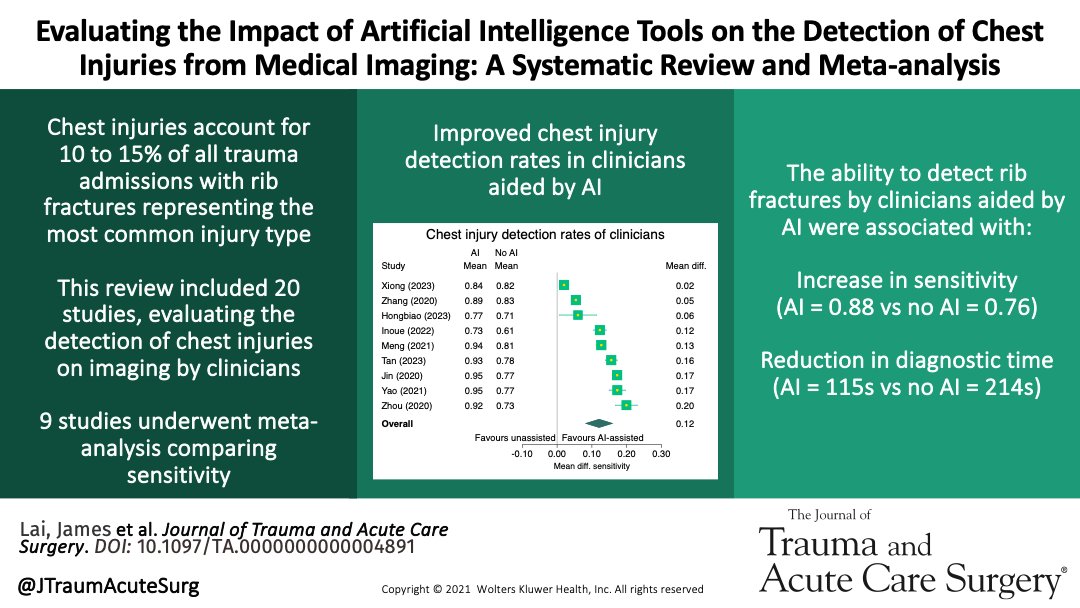
A systematic review of AI and detection of chest injuries: an improvement in sensitivity and reduction in detection time was associated with clinicians assisted with AI to detect chest injuries compared to unassisted clinicians.
#JTACS #ChestTrauma #MedicalArtificialIntelligence
@ImperialCollege
journals.lww.com/jtrauma/ful…
5
12
1,077
Mar 21
Communicatie hulpdiensten valt uit bij lange stroomstoring, oplossing niet in zicht /via @Nieuwsuur. Wat leuk om onze historicus Thiis Gras weer eens te zien… helaas nog wel in oud uniform😉 nos.nl/l/2607176
1
1
145


Mar 15
Hi. Looking for a cardiologist or ECG expert to review a small ECG dataset for my AI-ECG study. Ambulance nurses will assess ECGs with and without PMcardio. The aim is to evaluate time gain and improved sensitivity. DM welcome.@The_Nanashi_O, @smithECGBlog #ecg #cardiology RT🙏
1
1
114
Jorik Sweenen retweeted

Mar 14
It’s Time to Stop Pushing Epi in V-Fib
linkedin.com/pulse/its-time-…

1
14
44
6,700
Jorik Sweenen retweeted

11 Dec 2025
When should you get a CT scan on a STEMI patient to rule out aortic dissection?
drsmithsecgblog.com/when-sho…
5
26
86
13,001
Jorik Sweenen retweeted
2 Dec 2025
Everyone: check out this amazing youtube airway site.
These are the worlds experts in emergency airway. Brian Driver and Matt Prekker have published more on this topic than anyone and here they demonstrate every possible airway technique. Aaron Robinson is an amazing EMS Physician, with tons of ED and prehospital airway experience. @EM_RESUS @HennepinAirway @hcmcEM @hcmcemsed @HennepinHC @hennepinems
youtube.com/@hennepinairway?…
1
35
109
23,549
Jorik Sweenen retweeted

30 Nov 2025
The SGEM Podcast discussing acute-on-chronic abdominal pain in the emergency department is now available. Please consider listening and sharing.
thesgem.com/2025/11/sgem494-… #EBM #FOAMed

5
10
2,214

STEMI mimics ; rule out successfully by @PMcardioApp
Great✅👏
drsmithsecgblog.com/a-man-in…
1
5
17
2,047
Jorik Sweenen retweeted
28 Nov 2025
Does this comprehensive review signal the death of cervical collars, or are the reports of its death an exaggeration?
Find out on this week's episode of the SGEM.
thesgem.com/2025/11/sgem493-…
#EBM #FOAMed @davidcarr333 @emcrit
5
11
39
4,486
Jorik Sweenen retweeted

10 Nov 2025
'Google Maps' voor Romeinse Rijk gelanceerd: 'Wegennet met enorme impact' - nos.nl/l/2589799
5
17
3,519
Jorik Sweenen retweeted

8 Nov 2025
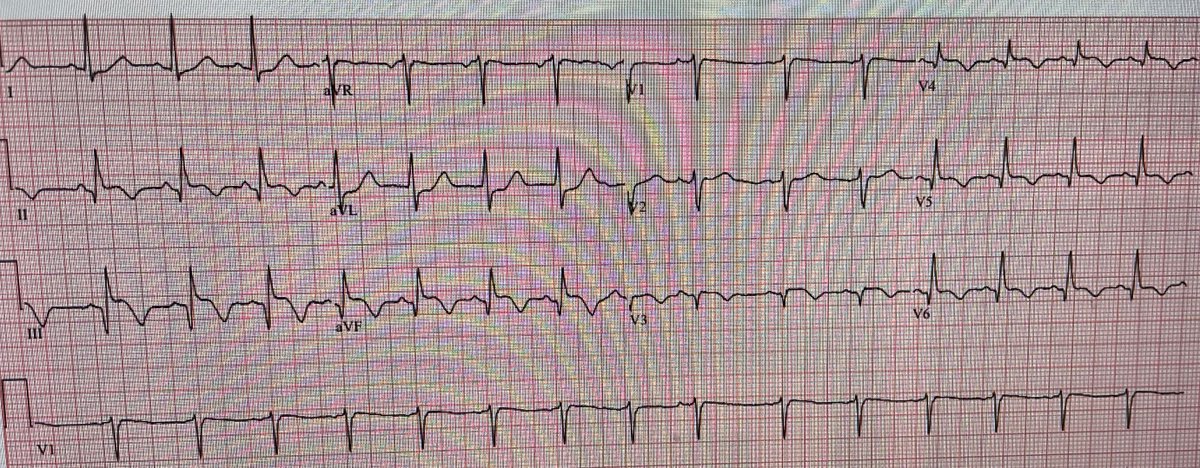
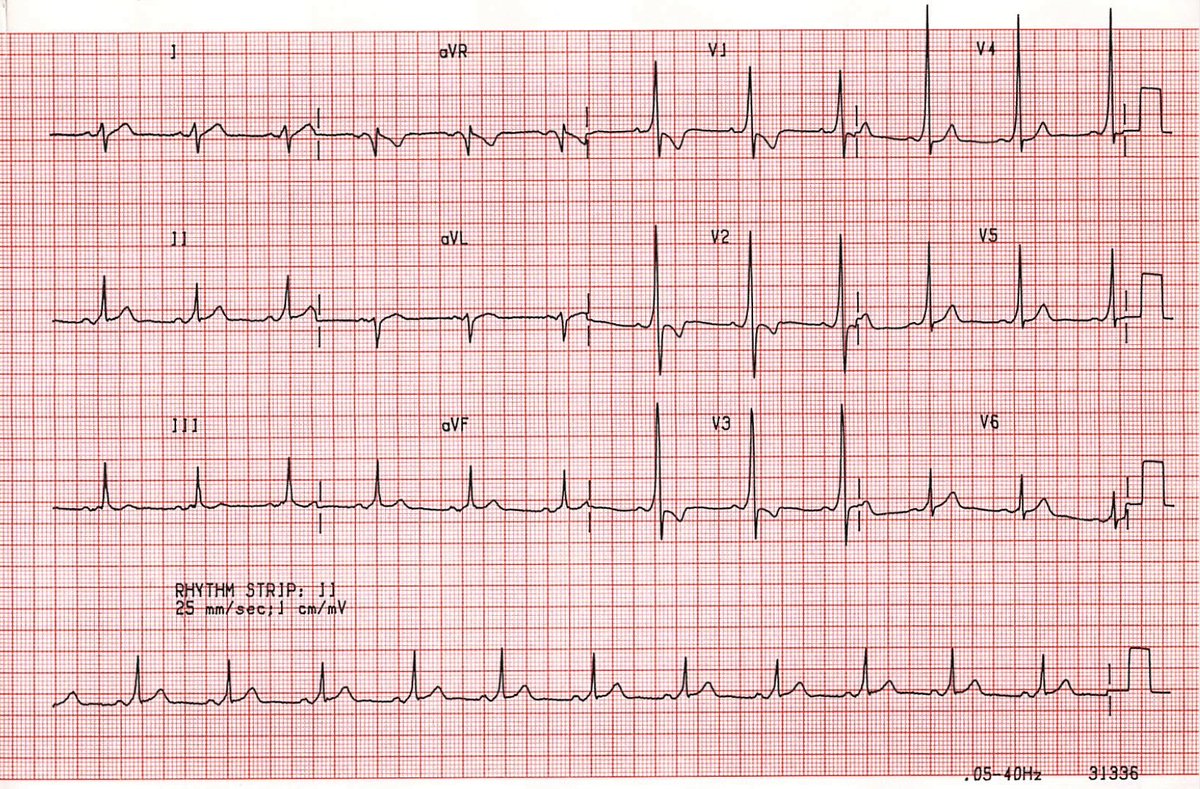
A 20yr ♂️ with complaints of dizziness and fainting spells. Family history of sudden death.
ECG done showed👇.
diagnosis?
Management?
#MedTwitter #MedEd #MedX #CardioTwitter #Cardiology #Cardio #ECG
@IhabFathiSulima @elidyynwa @MEmwanta @TSM_Humanist @mendietaalex1 @AWallflower7
11
9
62
8,772
Jorik Sweenen retweeted

3 Nov 2025
Could a short fat central line make a difference in exsanguinating trauma patients?
Listen to the latest @TheResusRoom papers of the Month
Link to the podcast: open.spotify.com/episode/636…
Link to the paper: associationofanaesthetists-p…
#Trauma #Resus #MassiveTransfusion
1
6
22
2,399
Jorik Sweenen retweeted

25 Oct 2025
The new ERC 2025 recommendations for advanced airway management during CPR
Airway and ventilation
📌During CPR, start with basic airway techniques and progress stepwise according to the skills of the rescuer until effective ventilation is achieved.
📌Give the highest feasible inspired oxygen during CPR.
Start effective ventilation breaths as soon as possible ensuring the rate and tidal volume are appropriate to prevent both inadequate ventilation (hypoventilation) and excessive ventilation (hyperventilation).
📌Deliver effective bag-mask ventilation breaths by optimising mask seal and airway patency and if necessary, use a two-person technique for bag-mask ventilation.
📌Give each inspiratory breath over 1s to achieve a visible chest movement.
📌When using a supraglottic airway (SGA), an i-gel is preferred to a laryngeal tube.
📌Tracheal intubation should only be attempted by rescuers with a high success rate and with the use of continuous waveform capnography. The expert consensus is that a high tracheal intubation success rate is over 95 % within two attempts at intubation.
📌Aim for less than a 5-second interruption in chest compression for tracheal intubation.
📌Use direct or video laryngoscopy for tracheal intubation according to local protocols and rescuer experience. In settings where video laryngoscopy is immediately available, it is preferable to use video laryngoscopy instead of direct laryngoscopy.
📌A sustained ETCO trace on waveform capnography must be used to exclude oesophageal placement of the tracheal tube.
📌Once a tracheal tube or a SGA has been inserted, ventilate the lungs at a rate of 10 min-' and continue chest compressions without pausing during ventilations. With a SGA, if gas leakage results in inadequate ventilation, pause compressions for ventilation using a compression-ventilation ratio of 30:2.
📌If using mechanical ventilation, use a volume-controlled mode during chest compressions set the ventilator to a tidal volume of 6-8 mL kg-' (predicted body weight), or to achieve a visible chest movement, the maximum inspired oxygen, a respiratory rate of 10 min-', an inspiratory time of 1-2 s, a positive end expiratory pressure (PEEP) 0-5 cm H2O, the peak pressure alarm at :0-70 cm H20, and the flow trigger off. Ensure mechanical ventilation is effective and if not, use manual ventilation.
📌If standard airway management strategies (oropharyngeal airway and bag-mask/supraglottic airway/ tracheal tube) fail during cardiac arrest, appropriately trained rescuers should attempt surgical cricothyroidotomy to enable oxygenation and ventilation.

6
47
134
18,860
Jorik Sweenen retweeted
17 Oct 2025
@PMcardioApp Medtech Innovator (MTI) and Nasdaq recognized Powerful Medical for winning the Best Science Startup and Overall Winner awards at the American Heart Association (AHA) Health Tech Competition. They did this by featuring them on the NASDAQ Tower in Times Square
1
5
14
2,386