
Joined May 2021
- Tweets 749
- Following 282
- Followers 455
- Likes 2,068
57 Photos and videos







Jan Biegus retweeted

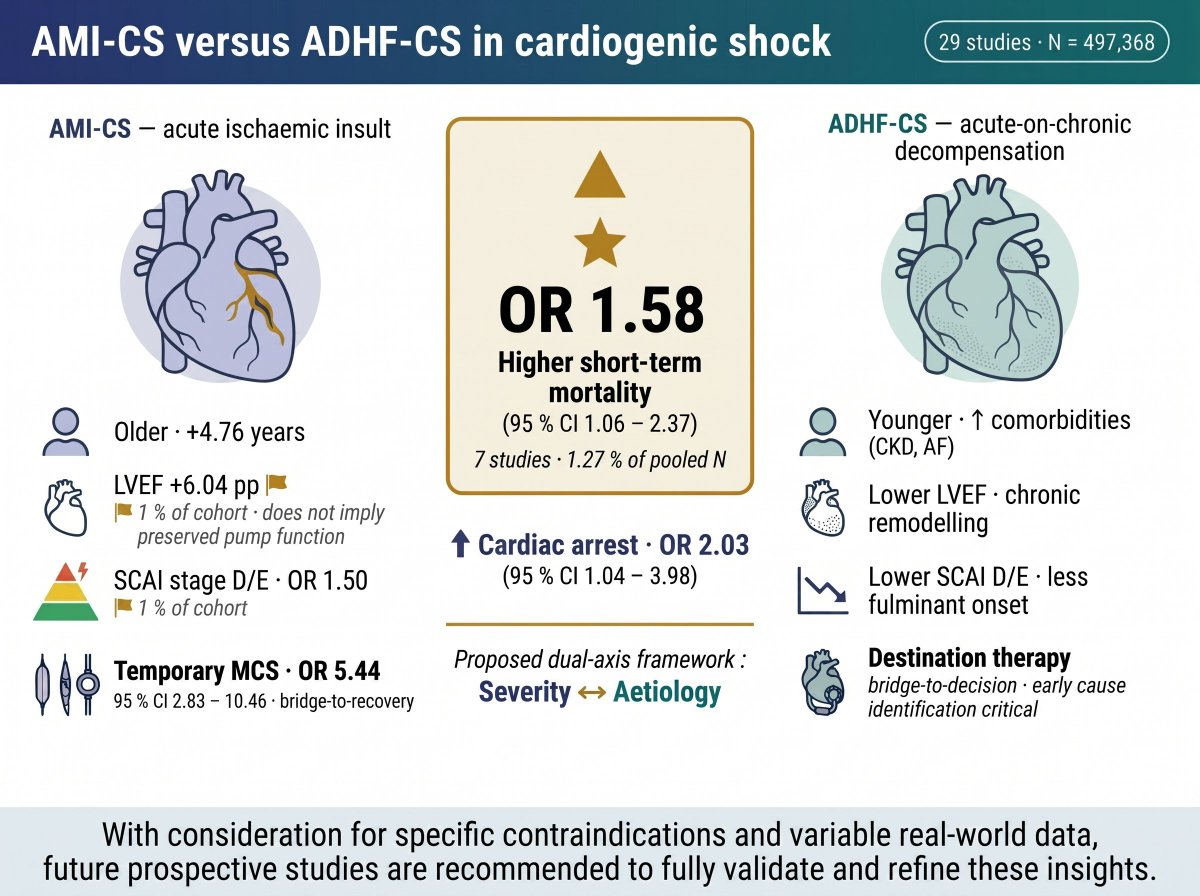
Heart attack or worsening heart failure in cardiogenic shock - does the cause change survival? 🫀
29 studies, ~497k patients: AMI-CS = more fulminant, 5× more mechanical support, higher mortality (OR 1.58).
Time for a severity × aetiology framework.
📄 doi.org/10.1093/ejhf/xuag186
2
3
164
Jan Biegus retweeted

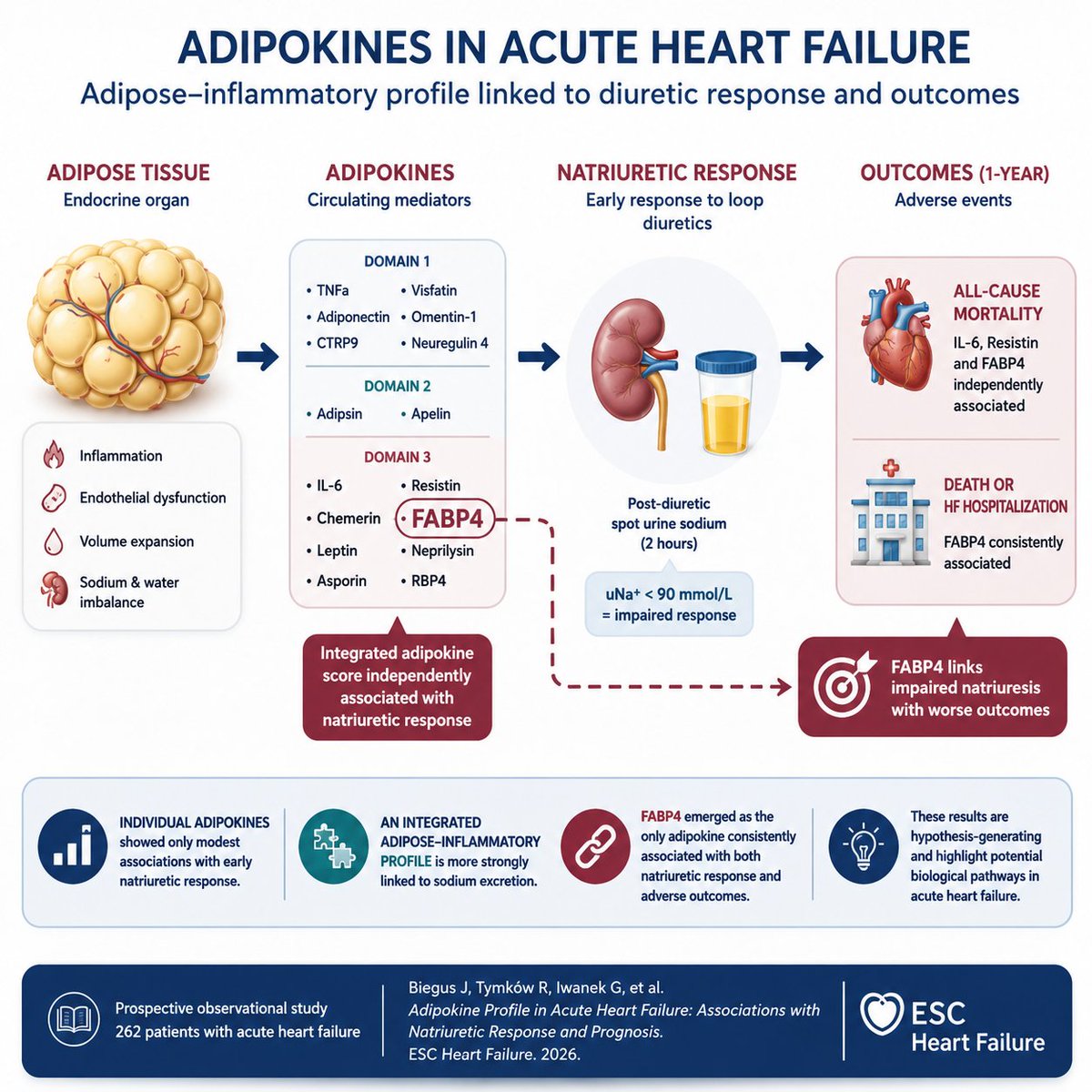
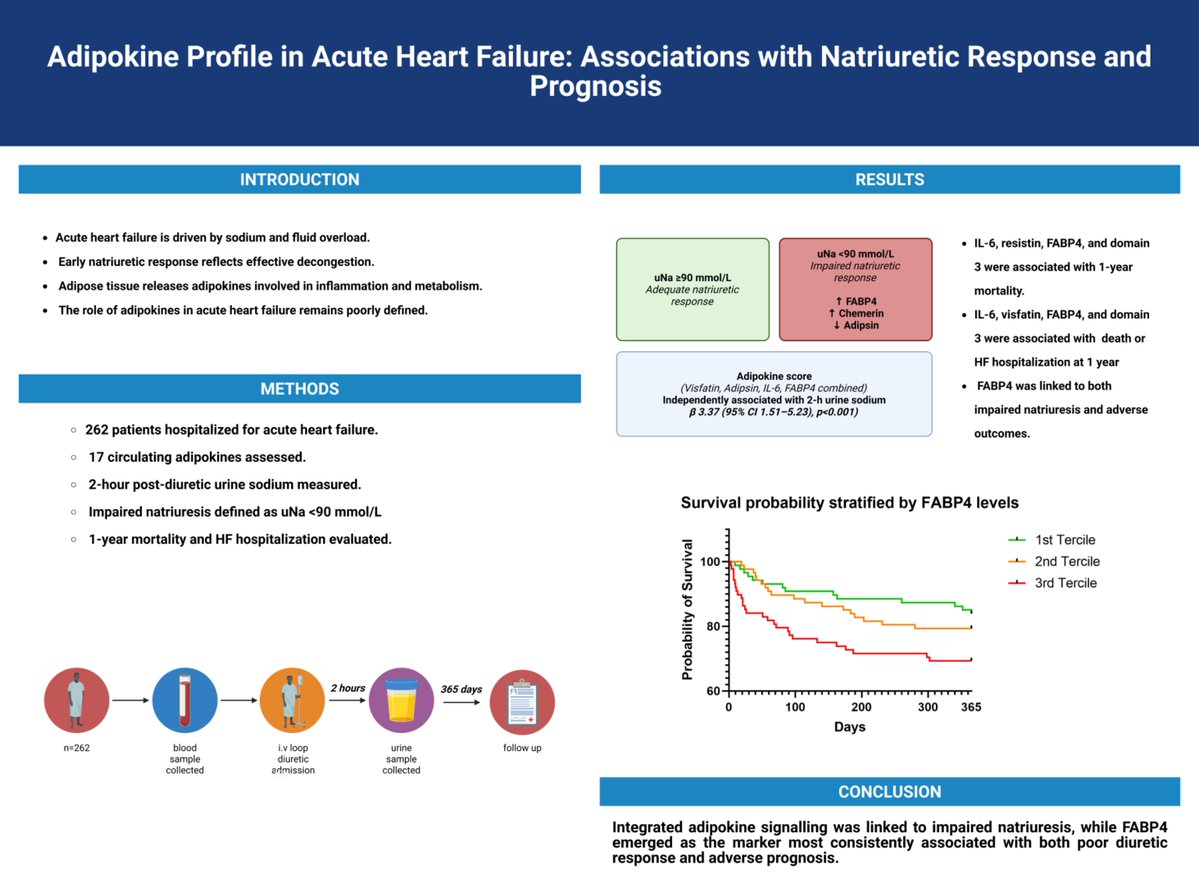
🫀Adipokine Profile in Acute Heart Failure: Associations with Natriuretic Response and Prognosis. see @ESC Heart Failure ow.ly/REjz50Z7SBu
@EJHFEiC @JanBiegus @Ppponikowski #HFA_ESC @hvanspall @ShelleyZieroth @FudimMarat @gcfmd @MarcoMetra @GianluSava #ESCHeartFailure
1
16
46
3,645
Jan Biegus retweeted

May 30
Adipokine Profile in Acute Heart Failure: Associations with Natriuretic Response and Prognosis. see@ doi.org/10.1093/eschf/xvag15…
2
2
72
May 29
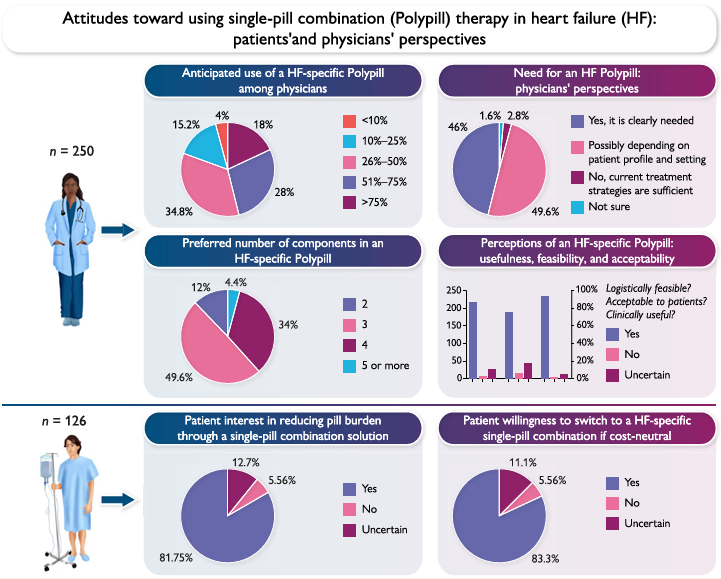
Both patients and physicians are waiting for the heart failure polypill to become a reality.
Our survey shows strong support from both groups for the development of a HF-polypill.
Read more in our ESC Heart Failure doi.org/10.1093/eschf/xvag04…
1
3
108
May 29
The biology and physiology of Na in HF are far more complex than simple, one-size-fits-all answers suggest. The role of Na in HF is nuanced, and many common assumptions deserve closer scrutiny.
Read our Viewpoint in JAMA Cardiology.jamanetwork.com/journals/jam…
35
May 29
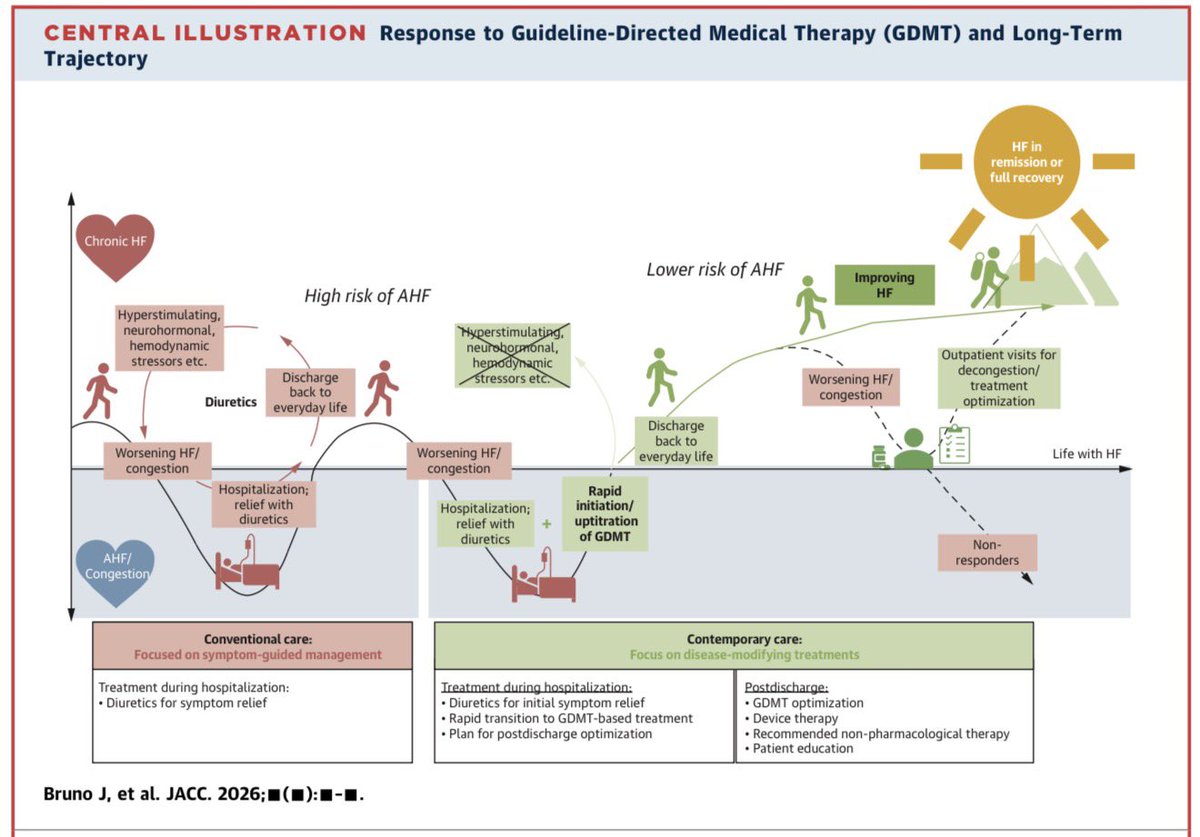
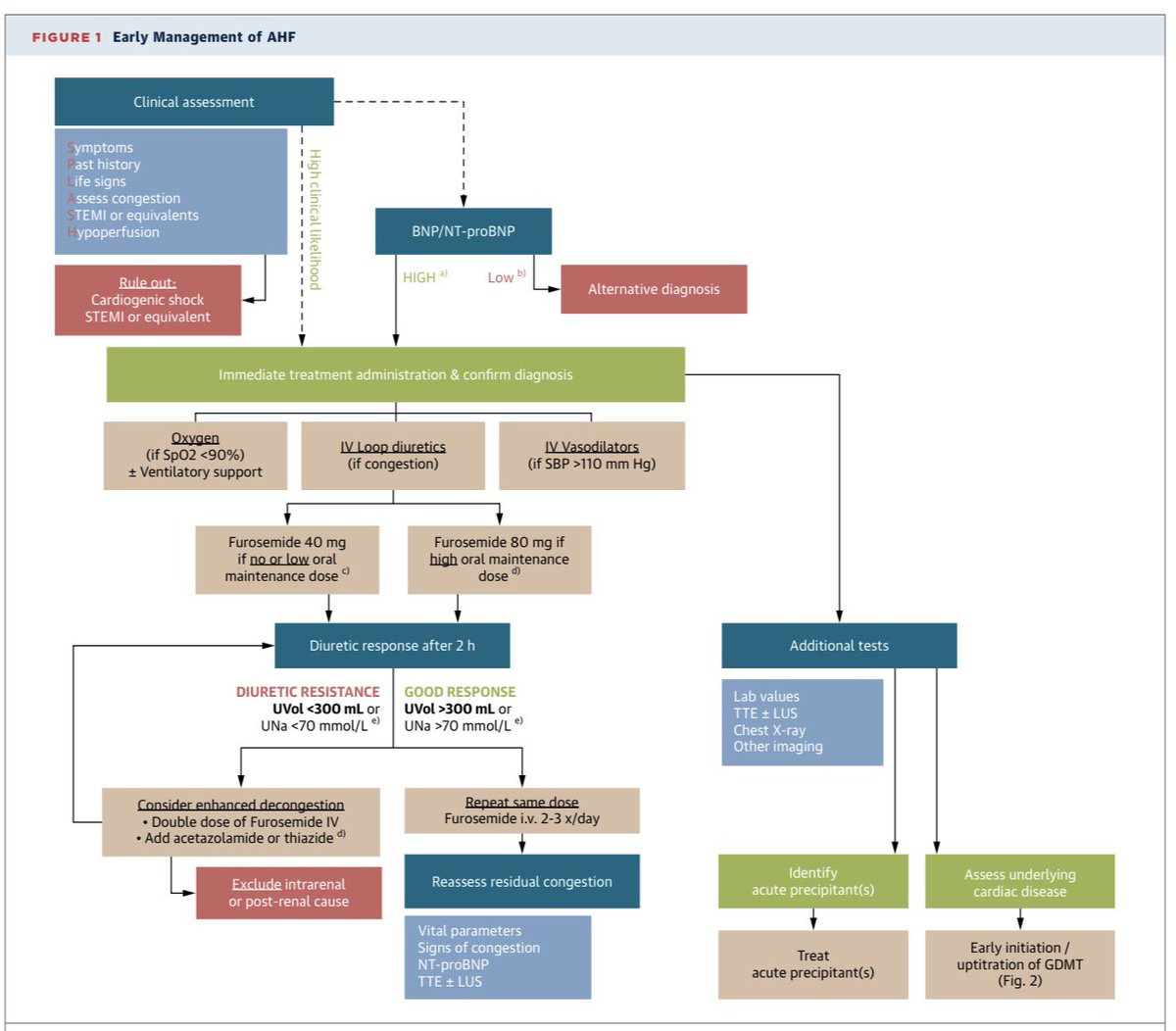
Our State of the Art paper: How to diagnose and handle AHF see in @JACCJournals jacc.org/doi/10.1016/j.jacc.…
May 29

Just published in JACC @JACCJournals!🫀
Acute HF care is evolving:
📍Rapid diagnosis
📍Early decongestion
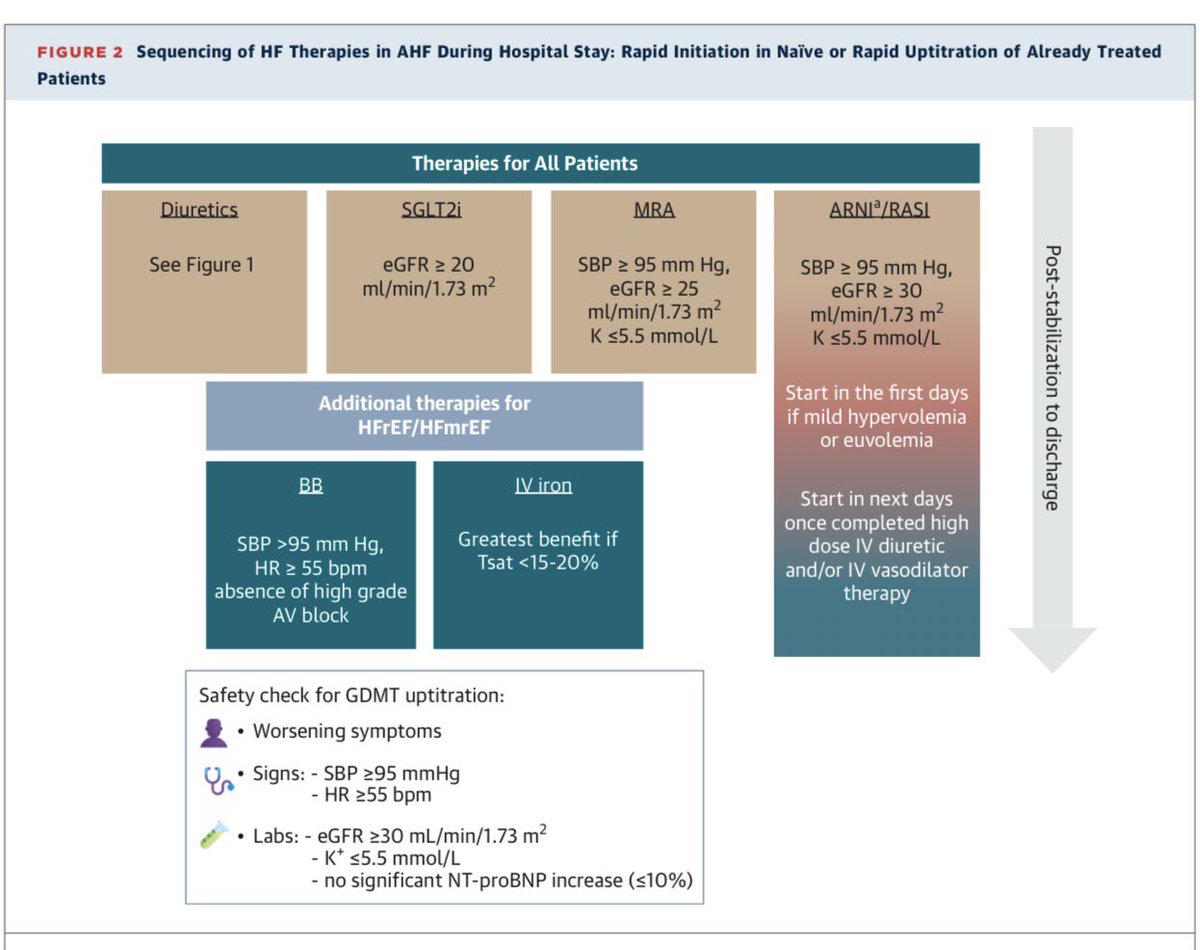
📍Timely GDMT initiation
📍Structured follow-up
📍Focus on long-term outcomes, not just symptom relief
Grateful to have contributed to this international collaboration & learned so much from the exceptional experts involved in this work. Congratulations to @Jolie_Bruno_ and @AlexMebazaa for the leadership & to all co-authors on this important publication🫀
Read the full paper🔗: doi.org/10.1016/j.jacc.2026.…
#HeartFailure #AcuteHeartFailure #JACC @jozinetm @BiykemB @GianluSava @pmyhre
44
May 29
AHF who to diagnose and treat it?
May 29
Just published in JACC @JACCJournals!🫀
Acute HF care is evolving:
📍Rapid diagnosis
📍Early decongestion
📍Timely GDMT initiation
📍Structured follow-up
📍Focus on long-term outcomes, not just symptom relief
Grateful to have contributed to this international collaboration & learned so much from the exceptional experts involved in this work. Congratulations to @Jolie_Bruno_ and @AlexMebazaa for the leadership & to all co-authors on this important publication🫀
#HeartFailure #AcuteHeartFailure #JACC @jozinetm @BiykemB @GianluSava @pmyhre
43
May 29
RT @slumberbell: Just published in JACC @JACCJournals!🫀
Acute HF care is evolving:
📍Rapid diagnosis
📍Early decongestion
📍Timely GDMT initi…
3
11
Jan Biegus retweeted

📢Growing evidence of the usefulness/safety of a natriuresis/guided diuretic therapy in acute HF.
Let´s use it!!
@ICardiacaSEC @IcyfaSemi

Delighted to share the publication of the #EDICA study in @JCardFail
doi.org/10.1016/j.cardfail.2…
In patients 🏥 with acute HF, a natriuresis/diuresis-guided decongestion strategy (@escardio guidelines) vs a weight-guided one showed:
✅ Greater 5-day NT-proBNP reduction
🟰 5-day clinical decongestion
🟰 Length of stay & 30-day outcomes (🏥/☠️)
🟰 Safety & feasibility
🔎 Trend toward not sustained ⬆️ 24–48 h diuresis, weight loss, & loop-diuretic dose
Some conclussions:
1️⃣ Time matters: earlier identification of diuretic resistance improves biomarker decongestion
2️⃣ Yet this did not translate into better short-term clinical outcomes
🎯Still need to close the gap between decongestion and clinical outcomes:
Timing of assessment? Faster titration? Earlier combination diuretic therapy?
Thanks to the great collab of Cardiology - Internal Medicine - Emergency Dep
@MartaCoboMarcos @JanBiegus @esthermonteroh @fernidom @DeCastro9 @dr_pavia @segoviajavierve @ICardiacaSEC @secardiologia @CardioRenalSEC @HospiPtaHierro @Sociedad_SEMI @IcyfaSemi @SEMES_
11
35
4,776
Jan Biegus retweeted
Glucagon-Like Peptide-1 Receptor Agonists in Patients with Heart Failure with Reduced Ejection Fraction see at ow.ly/bCcN50Z2YaH
@EJHFEiC @JanBiegus @Ppponikowski #HFA_ESC @hvanspall @ShelleyZieroth @FudimMarat @gcfmd @MarcoMetra @GianluSava #ESCHeartFailure

22
49
4,575
Jan Biegus retweeted

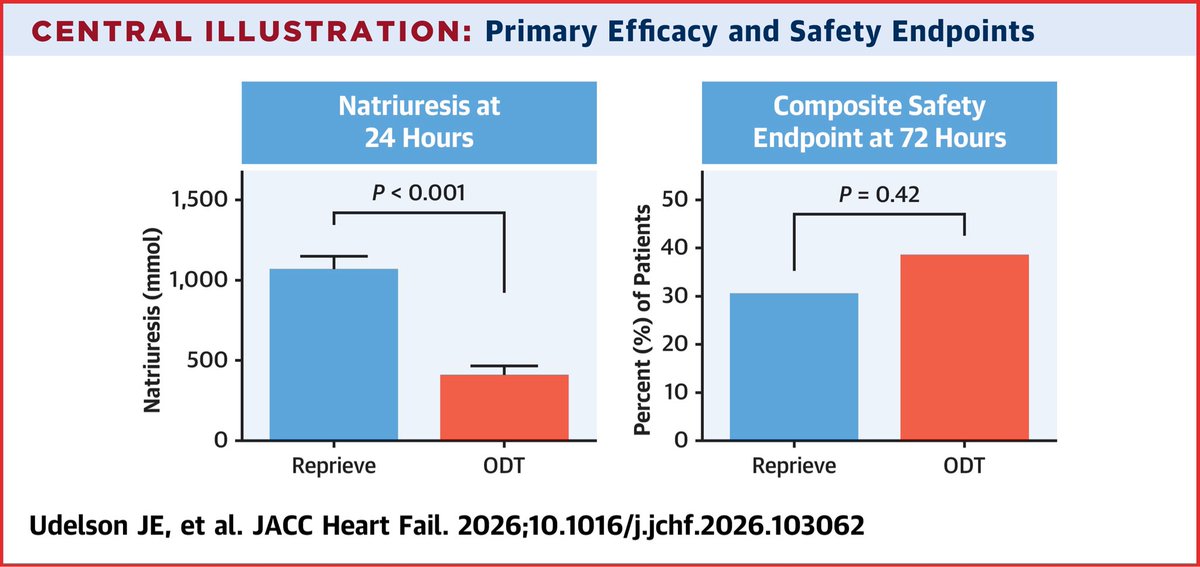
Fluid Management of Acute Heart Failure With the Reprieve System: The Randomized Controlled FASTR Trial
In this pilot trial, the Reprieve System safely produced significantly faster decongestion compared with ODT. Confirmation of these findings in the ongoing pivotal trial is required.
@JACCJournals @ACCinTouch @gcfmd @SJGreene_md @ShelleyZieroth
jacc.org/doi/10.1016/j.jchf.…
16
46
3,537
Jan Biegus retweeted

Can’t wait for its publication in JCF. Thanks to all investigators, and especially to my mentor. @MartaCoboMarcos
@JanBiegus @HospiPtaHierro @fernidom @ICardiacaSEC @CardioRenalSEC
2
4
249
Jan Biegus retweeted
Contemporary heart failure evidence in 2025: a joint summary of key trials from the European Journal of Heart Failure and ESC Heart Failure Journal
Despite an expanding therapeutic armamentarium, delayed diagnosis, underuse of evidence-based therapies, and organizational barriers continue to limit clinical impact. Bridging this implementation gap through earlier prevention, precision phenotyping, and integrated multidisciplinary care is essential to improving outcomes for HF patients
@JanBiegus @K_smala @PMarkwirth @HFA_President @hfcollaboratory @GianluSava @GMCRosano @AmrAbdin10 @HSkouri
academic.oup.com/eurjhf/adva…

5
16
1,045
Jan Biegus retweeted

Interesting perspective @JAMA_current on sodium and decompensated 🫀failure.
🧂 Can Na supplementation facilitate decongestion in HF?
No clear answer yet—but it’s a hypothesis worth challenging
Take a few minutes to question your assumptions 💡
🔗 jamanetwork.com/journals/jam…

3
8
308
Jan Biegus retweeted
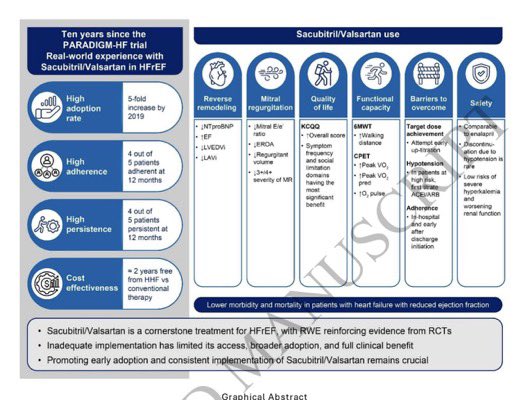
💊 10 years post-PARADIGM-HF: Real-world data on Sacubitril/Valsartan in HFrEF tells a promising — but incomplete — story.
✅ 5-fold adoption increase by 2019
✅ 4/5 patients adherent & persistent at 12 months
✅ ~2 years free from hospitalization vs conventional therapy
Yet inadequate implementation is still limiting its full clinical benefit.
Benefits are clear across the board:
↓ Reverse remodeling (NT-proBNP, EF, LVEDVI)
↓ Mitral regurgitation
↑ Quality of life & functional capacity
⚠️ Barriers remain: target dosing, hypotension, hyperkalemia
Early adoption consistent implementation = lives saved.
#HFrEF #HeartFailure #Cardiology #Sacubitril #Valsartan #RealWorldEvidence
9
20
1,085
Jan Biegus retweeted

Apr 27
🗞️ Ten Years Real-World Experience With Sacubitril/Valsartan in Patients With Heart
2 Failure With Reduced Ejection Fraction
@ESC_Journals @GiuseppeGalati_
@AmrAbdin10 @HanCardiomd
bit.ly/4mTPLMB
2
9
29
3,173
Apr 16
MRI in heart failure and beyond!
Apr 16

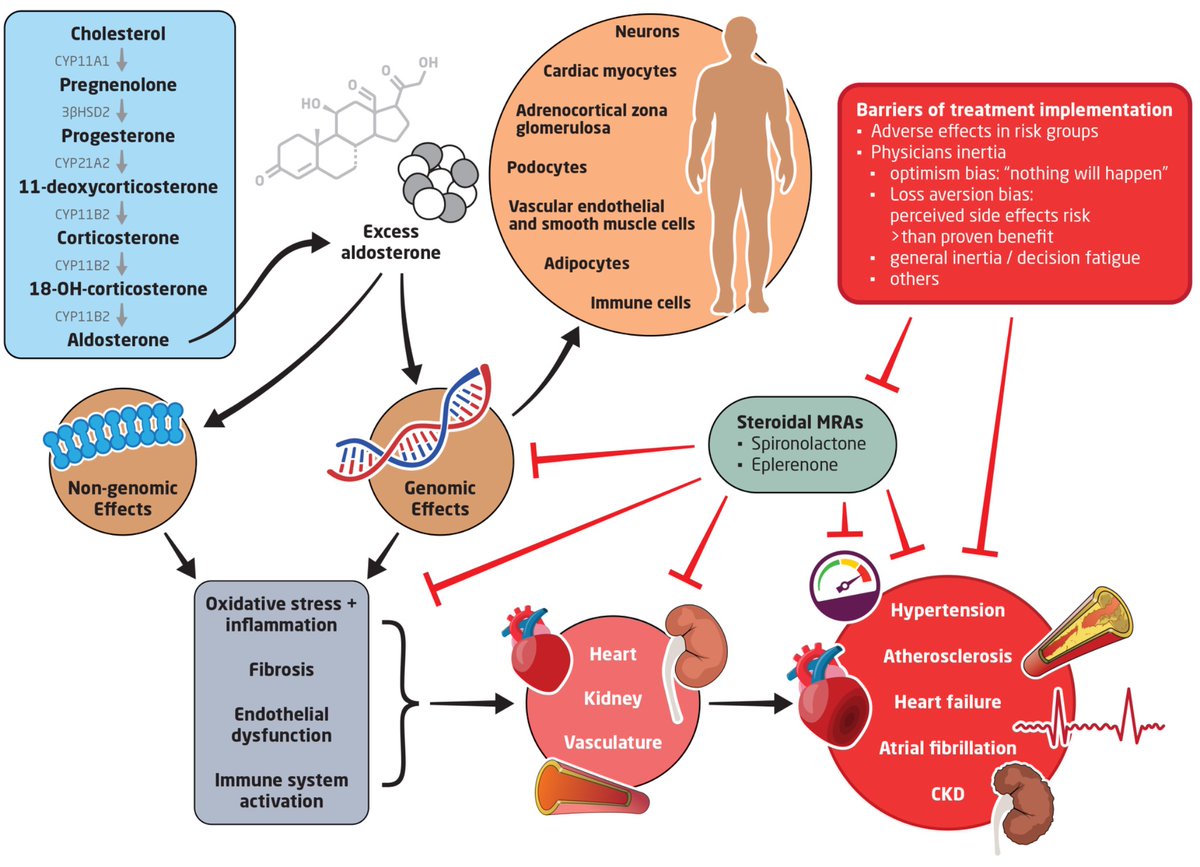
European Journal of Heart Failure International Expert Position Paper Utilisation, Optimisation, and Clinical Benefits of Steroidal #MRA in Heart Failure with a Reduced Ejection Fraction
academic.oup.com/eurjhf/adva…
#EJHF @ESC_Journals
@HanCardiomd @GiuseppeGalati_ @AmrAbdin10
1
3
189
Jan Biegus retweeted
Apr 16
European Journal of Heart Failure International Expert Position Paper Utilisation, Optimisation, and Clinical Benefits of Steroidal #MRA in Heart Failure with a Reduced Ejection Fraction
academic.oup.com/eurjhf/adva…
#EJHF @ESC_Journals
@HanCardiomd @GiuseppeGalati_ @AmrAbdin10
1
36
64
4,091
Jan Biegus retweeted

Heart failure with mildly reduced and preserved ejection fraction remains one of the biggest areas of unmet need in cardiovascular medicine.
In our recently published review (co-authored by @jozinetm and @GianluSava) in ESC Heart Failure, we examine the established and emerging pharmacologic options for HFmrEF and HFpEF,
The larger message is clear: the therapeutic landscape is finally becoming more actionable, but treatment still needs to be more deliberate, phenotype-aware, and evidence-driven.
A few key takeaways:
SGLT2 inhibitors now have the strongest and most consistent evidence base across EF ≥40%.
Finerenone has added important momentum as a promising option for HFmrEF/HFpEF, especially as we think more seriously about cardio-kidney-metabolic biology.
Phenotype-specific treatment matters. Obesity, CKD, diabetes, atrial fibrillation, and other comorbidities are not side notes in HFpEF. They are central to the disease.
The obesity-HFpEF space is evolving quickly, with incretins like semaglutide and tirzepatide helping push the field toward more targeted therapeutic strategies.
And importantly, there is still substantial room for progress. Ongoing studies of newer approaches, including selective MR modulation and aldosterone synthase inhibition, may help address some of the major gaps that remain.
HFpEF and HFmrEF are not therapeutic dead ends like they used to feel like just 5 years ago. But they do require us to think beyond a one-size-fits-all model.
doi.org/10.1093/eschf/xvag05…
3
40
125
6,530