
Neuroradiologist, Mayo Clinic. @UofUNeuro, @IURadiology, @OhioStateMed, @KelleyIndy, @DukeU grad. Opinions are my own.
Joined January 2017
- Tweets 404
- Following 573
- Followers 998
- Likes 1,427
54 Photos and videos















Kalen Riley retweeted
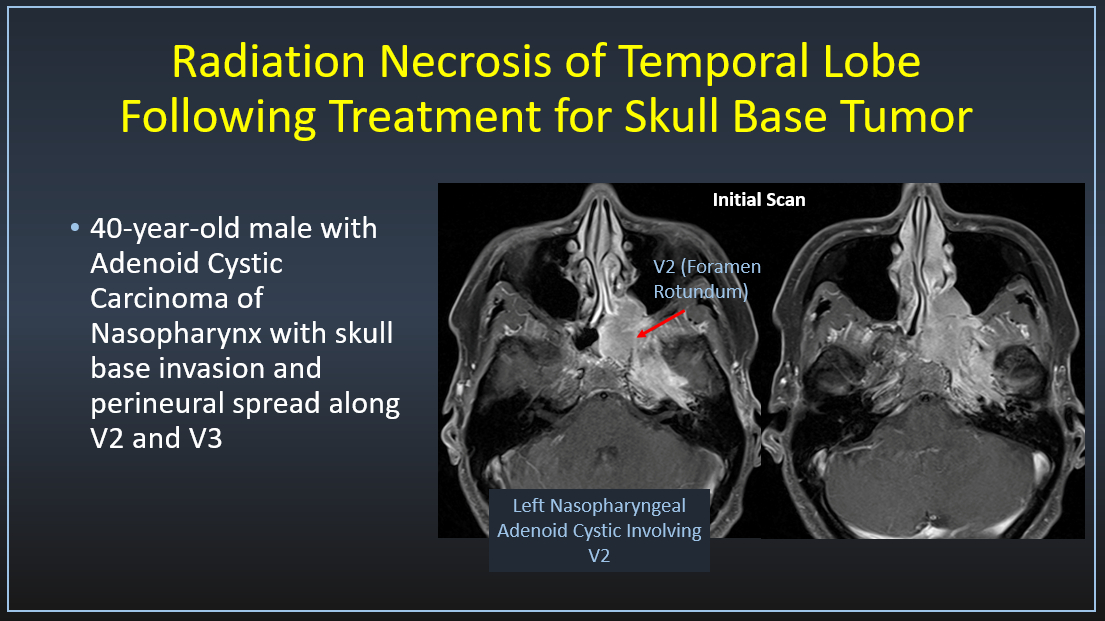
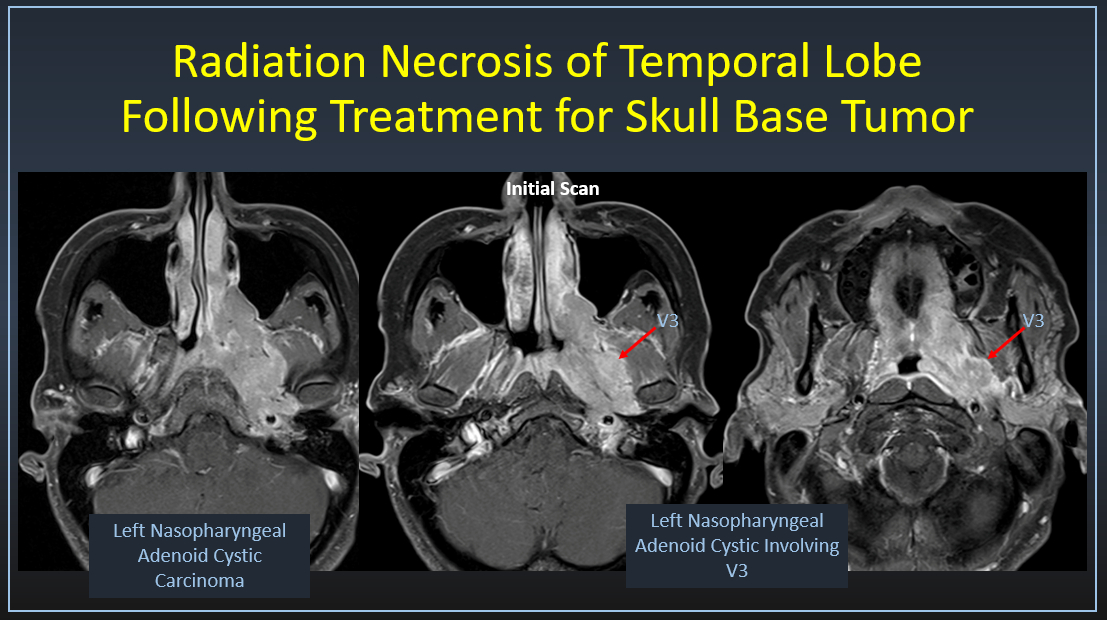
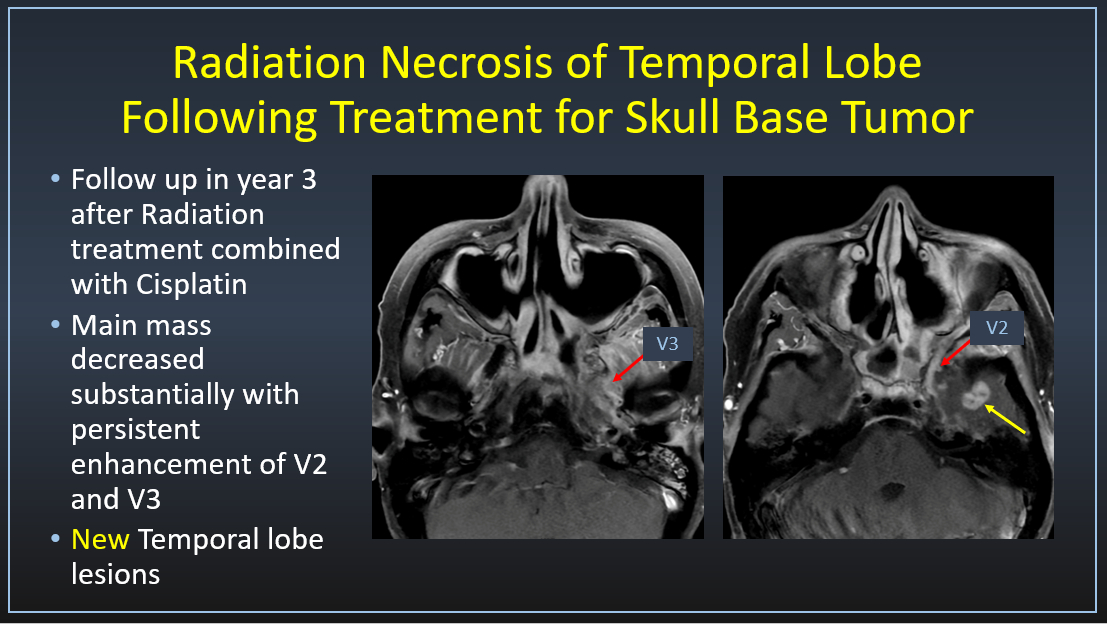
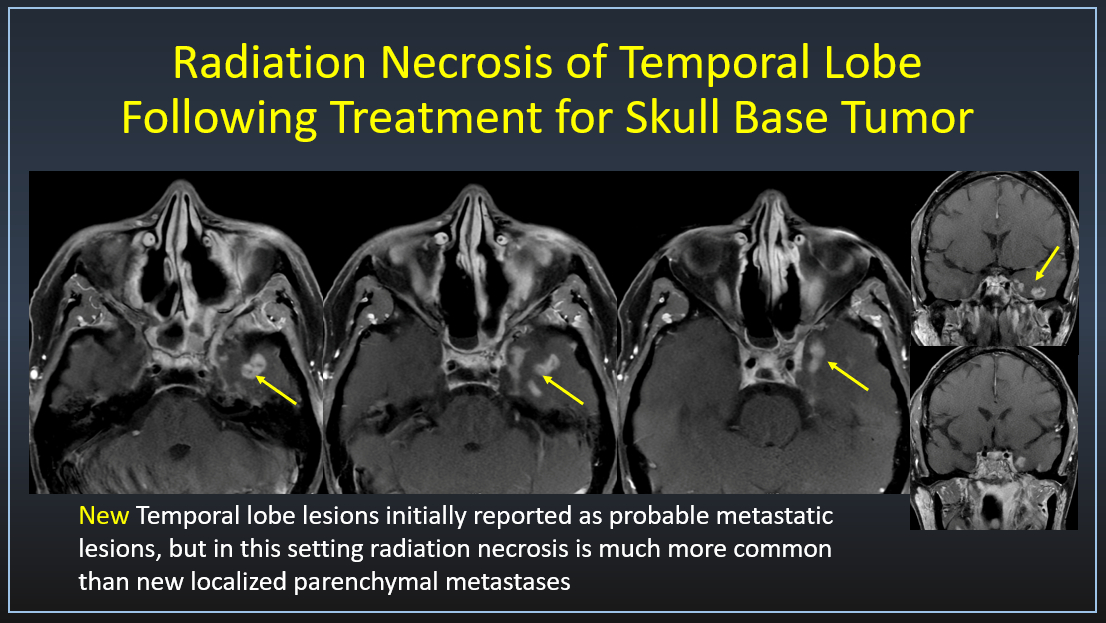
In a patient with prior radiation for nasopharyngeal carcinoma (NPC) or other primary malignant tumor such as adenoid cystic carcinoma, a new intraparenchymal lesion in the anterior temporal lobe is much more likely to represent radiation necrosis than metastatic disease. (Radiation necrosis until proven otherwise)
Imaging clues that favor radiation necrosis:
-Location: anterior/inferior temporal lobe ( and within radiation field)
-Timing: Within first 3 years of radiation
-Enhancement: irregular, ring-like or “soap-bubble”
-Edema: often disproportionate
-Perfusion (DSC MRI): ↓ rCBV
-MR spectroscopy: lipid-lactate peaks, ↓ choline
Metastasis, while rare, becomes more plausible if:
-Lesion is outside radiation field
-Multiple lesions in atypical locations (e.g., cerebellum, cortex elsewhere)
-Markedly elevated perfusion (high rCBV)
-Known systemic metastatic progression
4
38
140
7,213
Kalen Riley retweeted

29 Nov 2025
It’s time for my annual @RSNA blast to begin!
The Head & Neck programming is always 💯 high yield with the “best of the best” educators and experts. 🗣️👂👃👁️🧠
Head to rsna.org/annual-meeting to build your #RSNA25 agenda! Or just bookmark this:

7
23
65
9,121
Kalen Riley retweeted

27 Sep 2025
Another fun and fabulous ASHNR! Thank you to @PhilipRChapman1 for planning an amazing meeting with world class educational content. Sad to miss the gala tonight but looking forward to next year’s meeting in Pittsburgh @ASHNRSociety @CynXinWu




2
21
1,453
Kalen Riley retweeted

24 Sep 2025
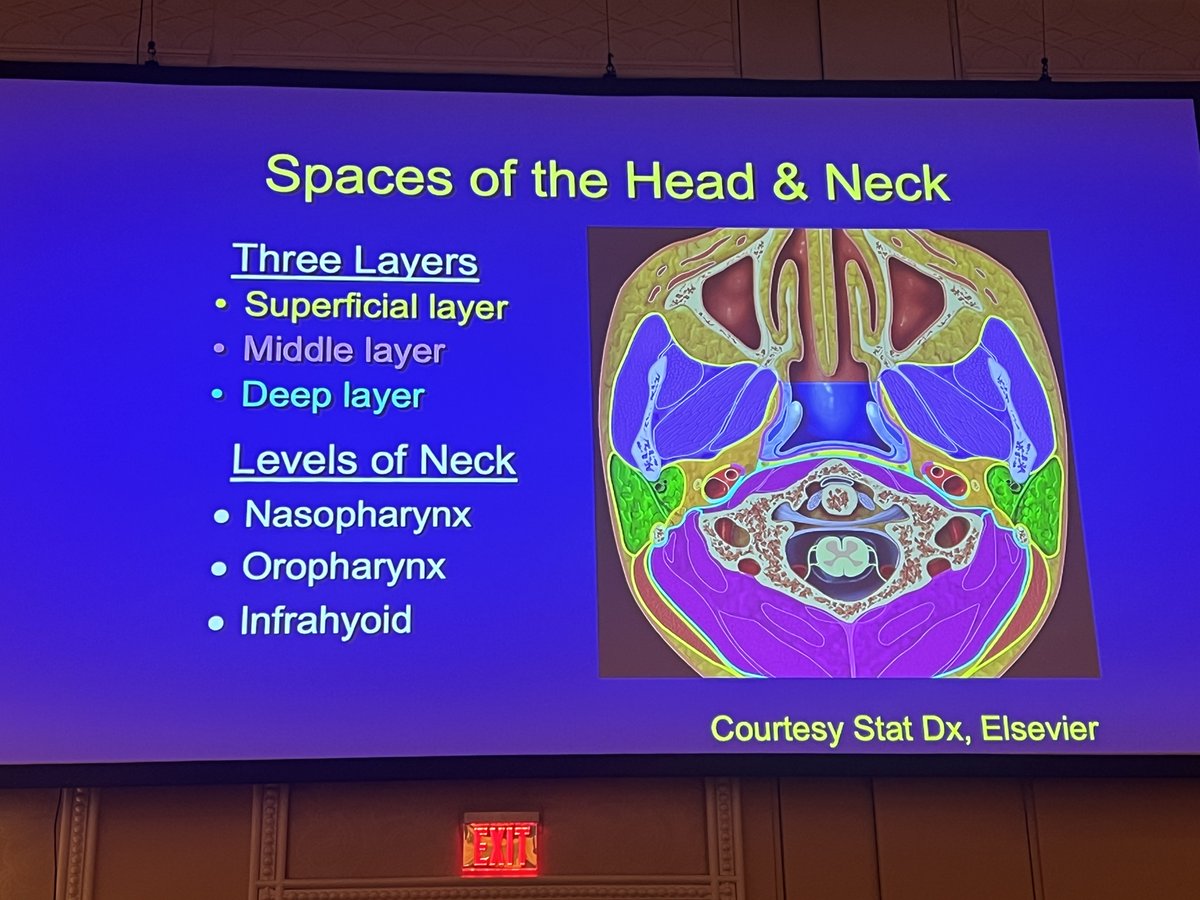
Important to recognize the concept of deep cervical fascia, but memorizing the specific layers is less important! #ASHNR25
2
14
849
Kalen Riley retweeted
24 Sep 2025
Welcome to #ASHNR25 !! Thanks to Dr. Chapman for organizing a fantastic program!


7
16
1,018
Kalen Riley retweeted
28 Jul 2025
#ASHNR25 is less than 2 months away!! Join us in Las Vegas 9/24-28 for the premier head and neck imaging meeting and learn from amazing educators. This year's meeting will feature new interactive parallel sessions and hands-on a ultrasound workshop to round out the fantastic educational program.
Register now at ashnr.edusymp.com/product/de…

7
15
1,295
Kalen Riley retweeted
29 May 2025
🚨🚨🚨The #ASHNR25 abstract deadline has been extended!! Submit your original research and/or engaging educational projects by 11:59 PM June 4, 2025!! We look forward to seeing all of your fantastic work in Las Vegas!
@amyfjuliano @bpoliceni @PhilipRChapman1 @CMGlastonbury
6
11
1,291
Kalen Riley retweeted
29 May 2025
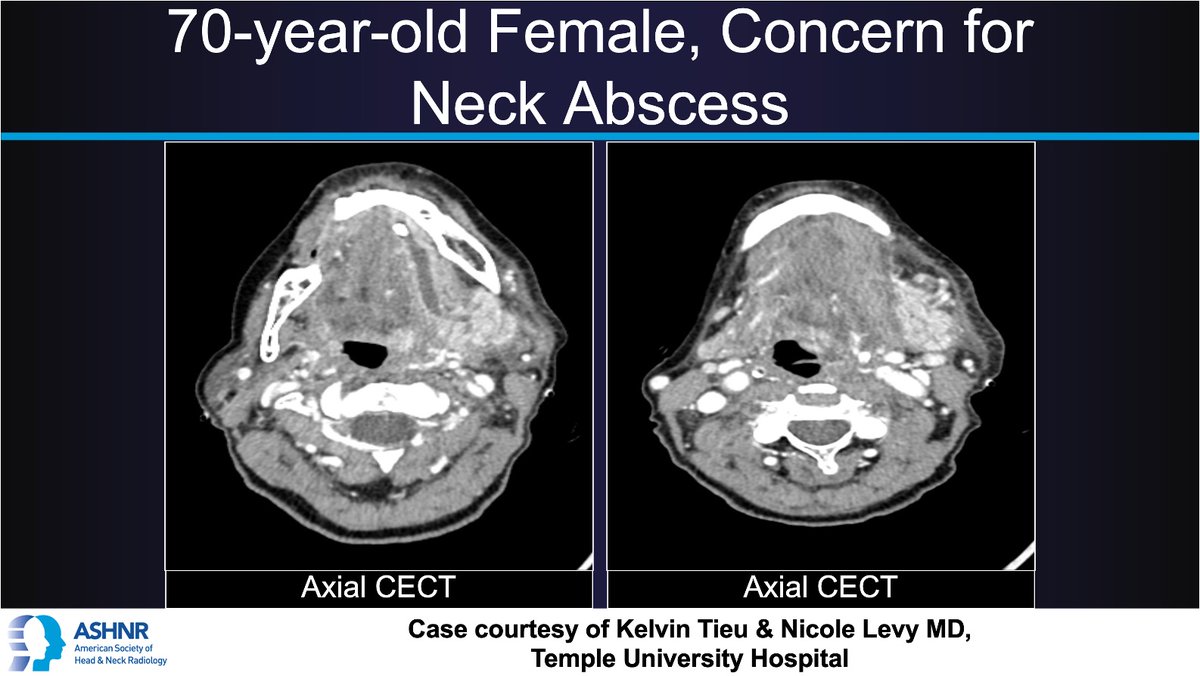
#ASHNRCOTW #299: Neck abscess. Thx
Kelvin Tieu and Dr. Levy 4 case! #ASHNR25
Answer w/ appropriate GIF only -- stay professional & don't spoil it!
@callyrobs @DShatzkes @CDP_Rad @rhwiggins
@nakoontz @KRileyMD @CMGlastonbury @tabby_kennedy @PhilipRChapman1 @cmtomblinson
@amyfjuliano @bpoliceni @MohitTCCNeuro
@AshokSrini15 @KatieTraylorDO @CynXinWu
4
7
31
2,582

24 May 2025
Check out this fantastic article just published by my wife and her group! mdpi.com/2072-6643/17/11/176…
2
4
98
Kalen Riley retweeted

7 Mar 2025
🌟#ASHNR25 abstracts OPEN & we are EXCITED to announce FOUR member-in-training $2k travel awards to attend this year's meeting in Las Vegas! 🌟@ASHNRSociety
16
35
4,498
Kalen Riley retweeted
5 Feb 2025
We are thrilled to announce a fantastic new benefit of ASHNR membership!! The ASHNR Head and Neck Radiology Curriculum (HNRC) is a curated collection of 82 superb lectures covering a breadth of H&N imaging topics from past annual meetings. Designed for radiologists at all levels, it allows for a customizable, structured approach to learning H&N imaging. Visit ashnr.org/hnrc today and use your member login to access this wonderful new resource! If you haven't renewed your membership for 2025, now is the perfect time!!
@cmtomblinson
1
20
48
3,981
Kalen Riley retweeted
29 Jan 2025
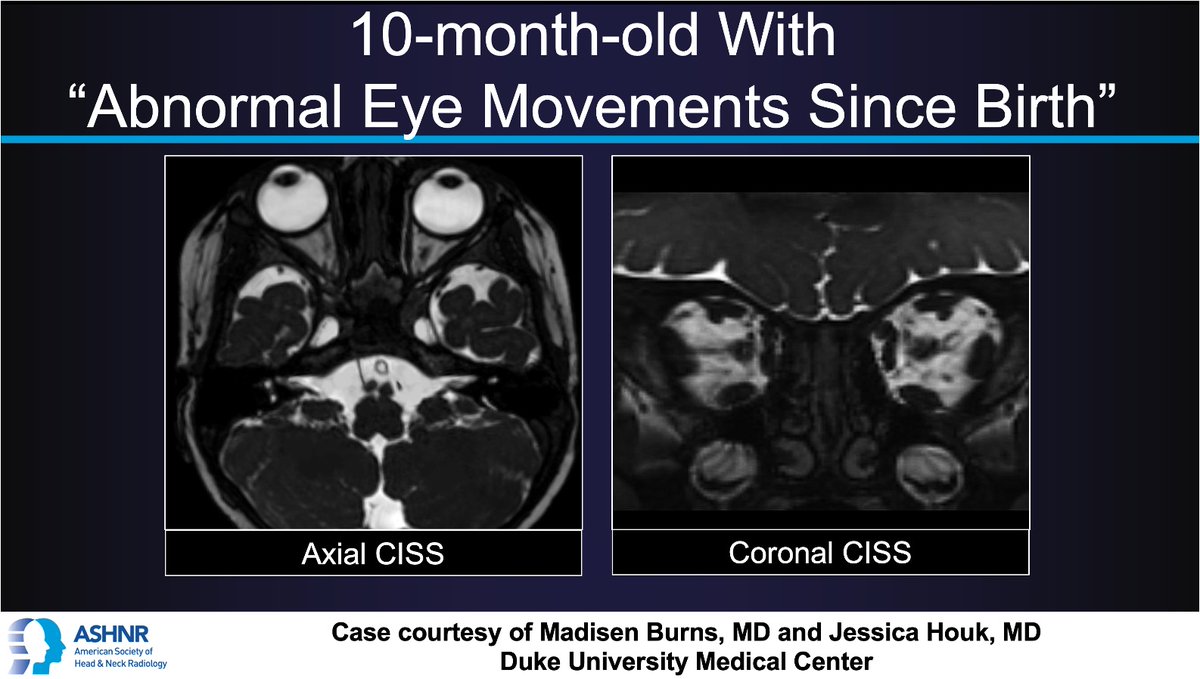
#ASHNRCOTW #283: Abnl eye movements. Thx
@madisenburns1 @jhoukMD 4 case! #ASHNR25
Answer w/ appropriate GIF only -- stay professional & don't spoil it!
@callyrobs @DShatzkes @CDP_Rad @rhwiggins
@nakoont @KRileyMD @CMGlastonbury
@tabby_kennedy @PhilipRChapman1 @cmtomblinson @amyfjuliano @bpoliceni @MohitTCCNeuro @AshokSrini15 @KatieTraylorDO @CynXinWu
4
13
41
3,879
Kalen Riley retweeted
12 Dec 2024
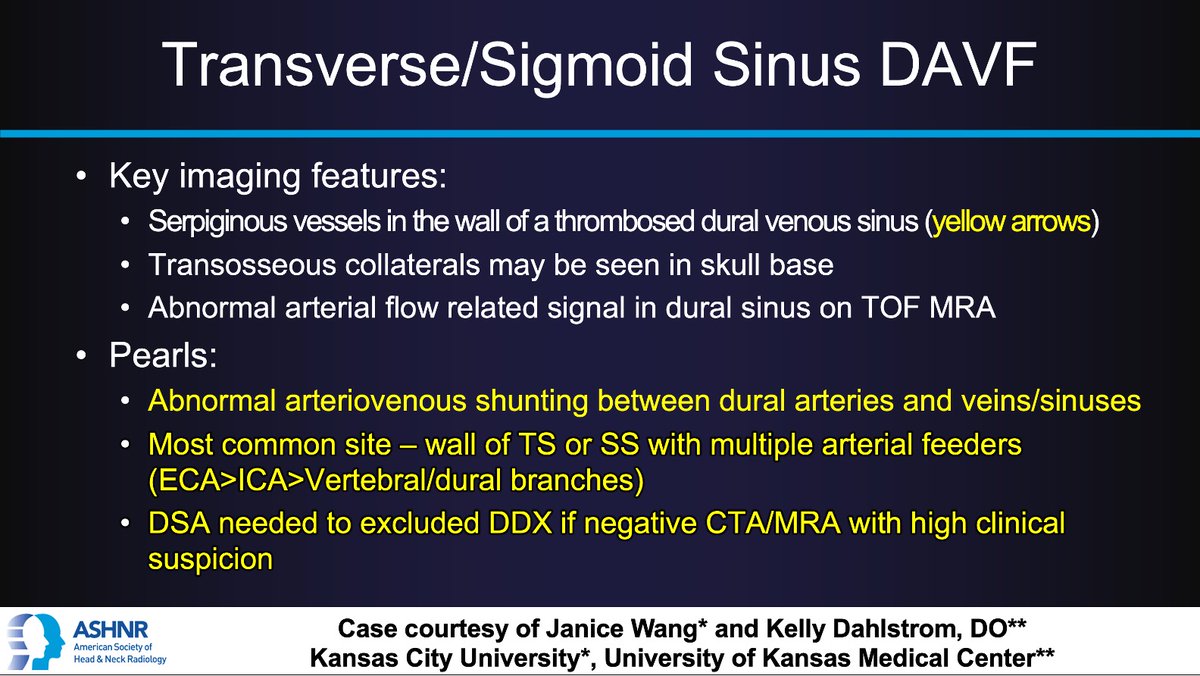
#ASHNRCOTW #278: ANSWER. Thx @janice_a_wang
@kelly_dahlstrom 4 case! #ASHNR25
@callyrobs @DShatzkes @CDP_Rad @rhwiggins
@nakoontz @KRileyMD @CMGlastonbury @tabby_kennedy @PhilipRChapman1 @MohitTCCNeuro @AshokSrini15 @amyfjuliano @CynXinWu @bpoliceni @KatieTraylorDO
20
71
6,551
Kalen Riley retweeted
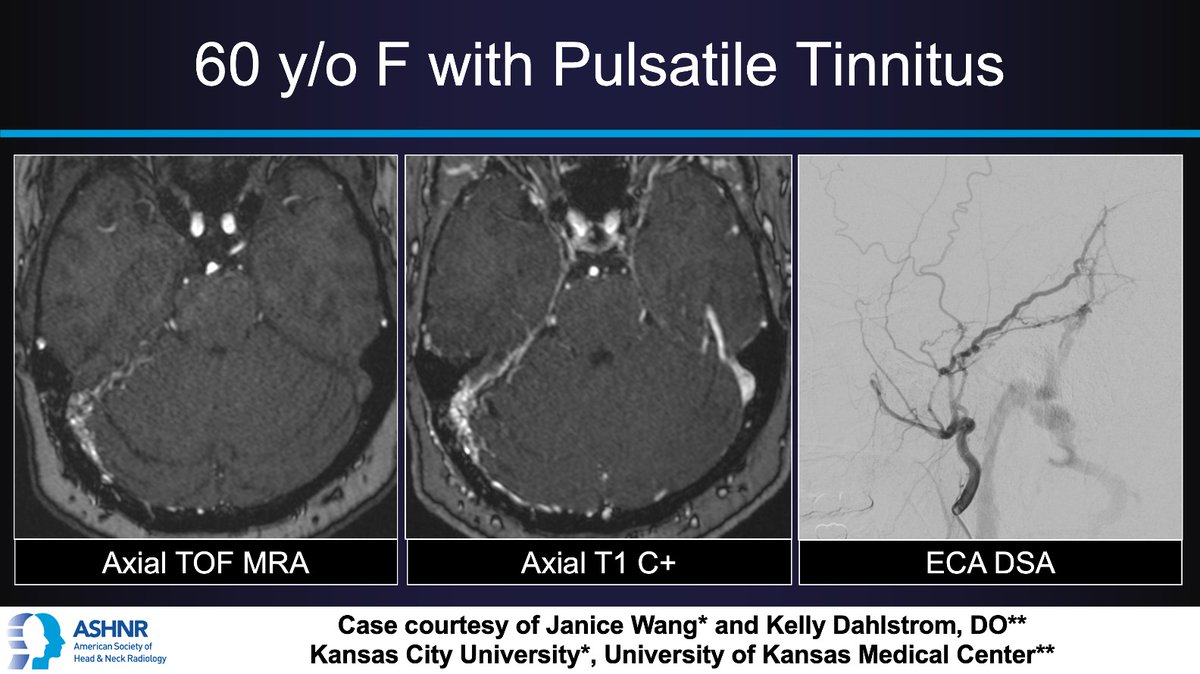
11 Dec 2024
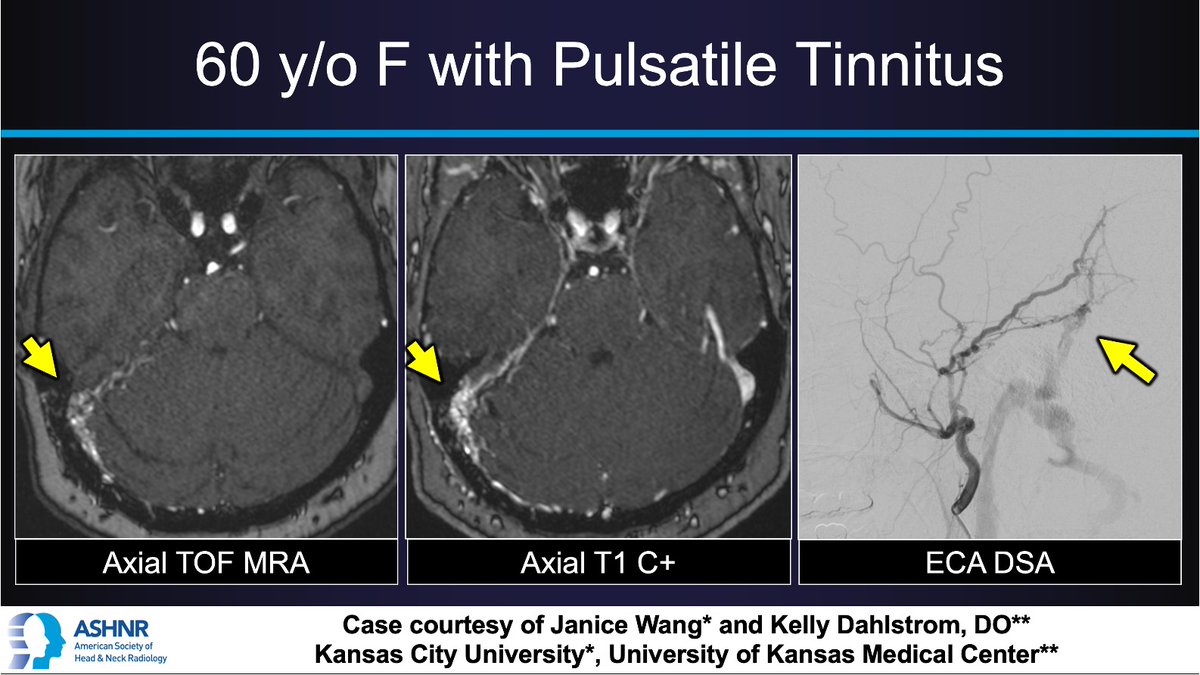
#ASHNRCOTW #278: Pulsatile Tinnitus. Thx
Janice Wang @kelly_dahlstrom 4 case! #ASHNR25
Answer w/ appropriate GIF only -- stay professional & don't spoil it!
@callyrobs @DShatzkes @CDP_Rad @rhwiggins
@nakoontz @KRileyMD @CMGlastonbury
@tabby_kennedy @PhilipRChapman1
5
14
56
5,824
Kalen Riley retweeted

1 Nov 2024
Save the Date! San Diego was huge hit this year. Never too early to start planning for next year's ASHNR Annual Meeting Sept 24-28, 2025 at the Encore in Las Vegas @ASHNRSociety

2
20
49
6,022
Kalen Riley retweeted

18 Oct 2024
Registration for the November symposium is now open! Join @nakoontz and expert radiologists on November 14 to deepen your understanding of head and neck anatomy. Use the link in our bio to register now.
8
17
1,800
Kalen Riley retweeted
3 Oct 2024
#HNmonograph ✨October issue @RadioGraphics is ALL HEAD & NECK! Fantastic papers from around the globe [!] with gorgeous images graphics! @DShatzkes @drjengillespie @drSurjthVattoth @pbunchmd @drsuyash @tabby_kennedy @ashasarm @alexandra_foust @AmitAgarwalMD @GillianPotter7
2 Oct 2024

The latest issue of @RadioGraphics is now available! Check out the October issue here. bit.ly/NewRadG #RGphx #RadCME #RadRes @RadG_Editor
24
68
7,556
Kalen Riley retweeted

8 Sep 2024
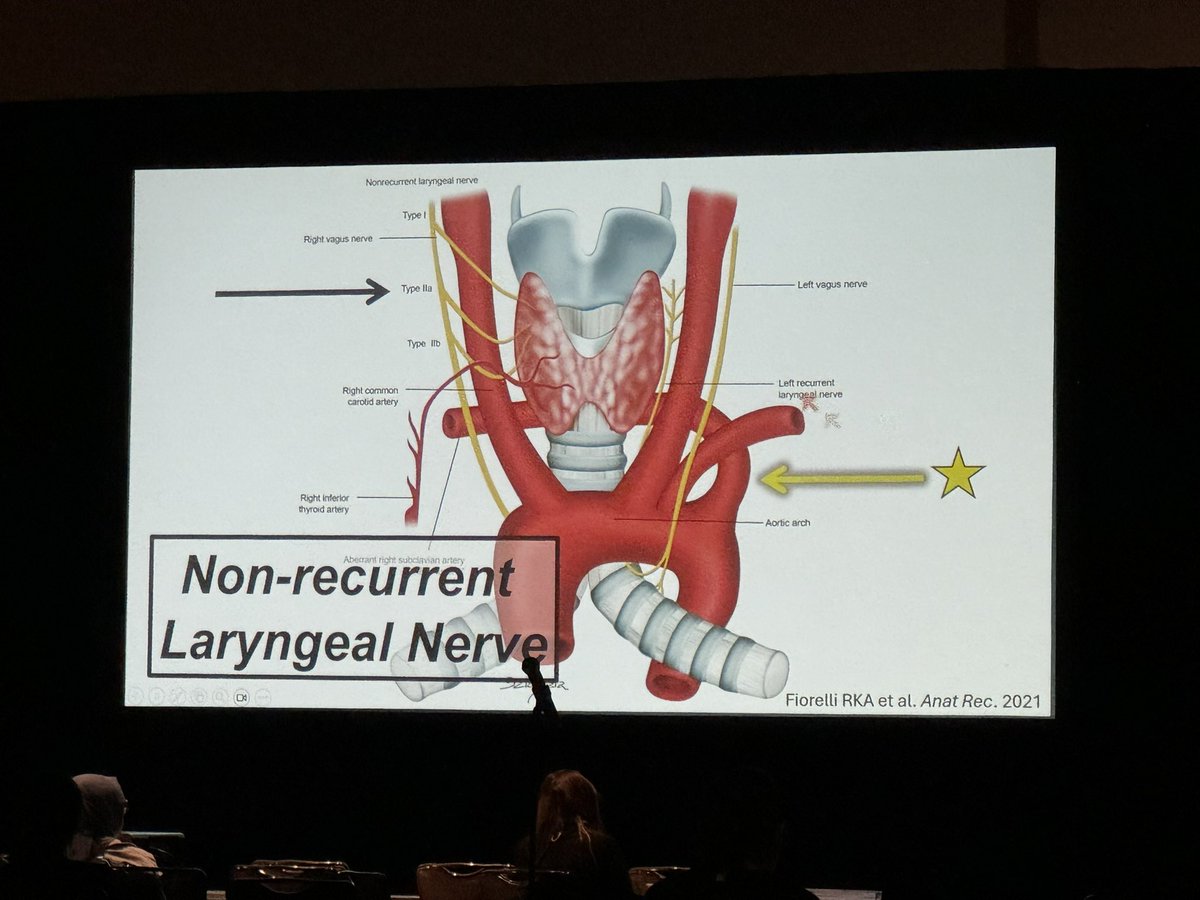
The non-recurrent right laryngeal nerve is a rare but important variant to be aware of to help prevent injury during surgery. Seen in the setting of an aberrant right subclavian artery.
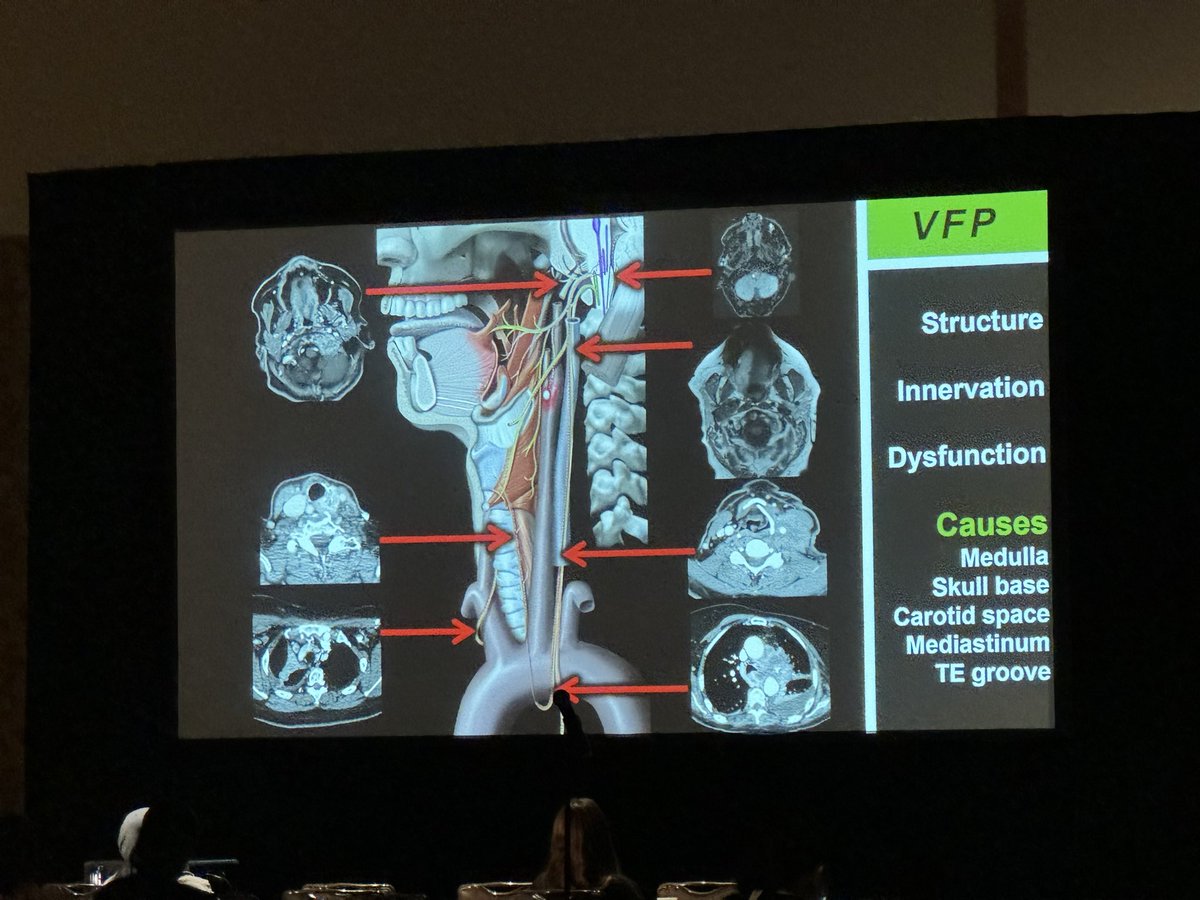
@LNLedbetter vocal cord paralysis talk at #ASHNR24
1
14
47
9,011
Kalen Riley retweeted
5 Sep 2024
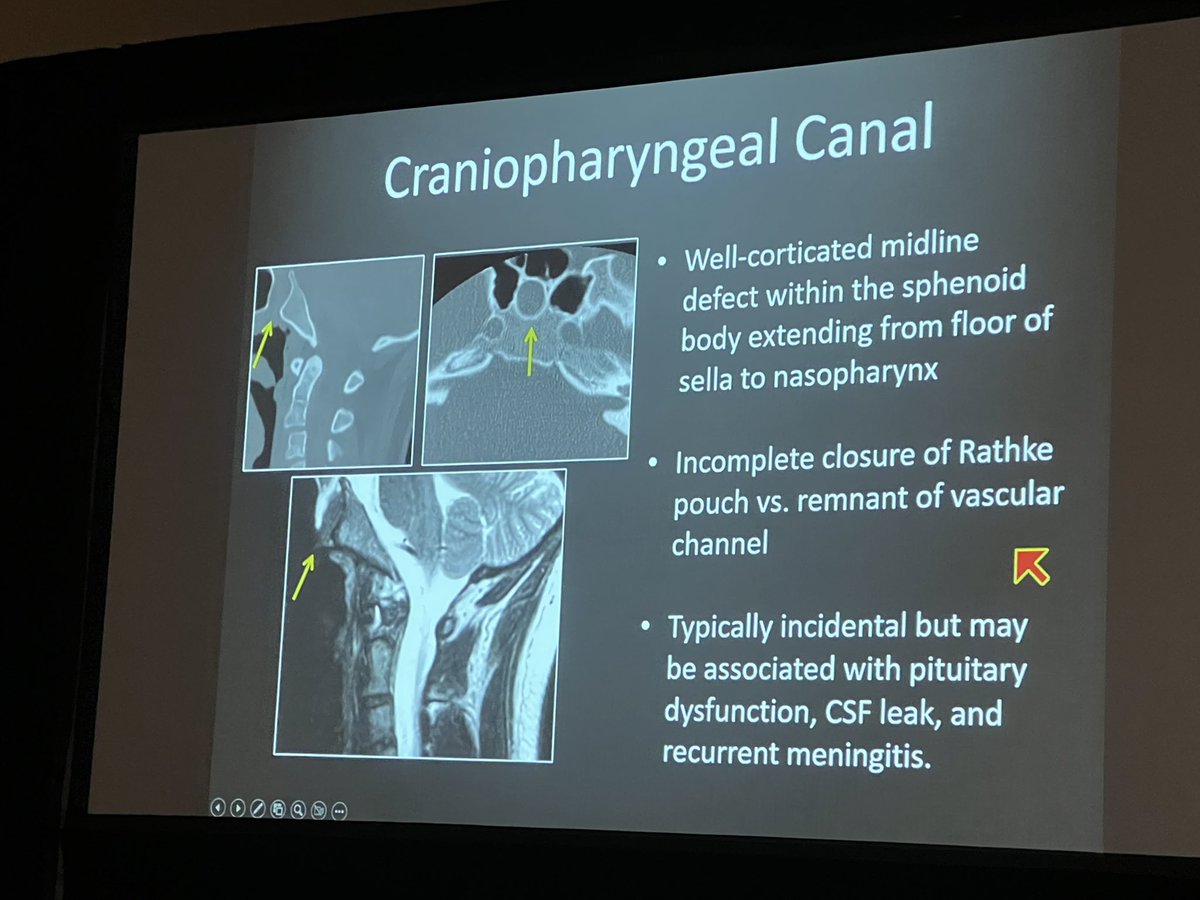
A couple of these important central skull base variants beautifully illustrated by @DrNikyFarid #ASHNR24

14
92
8,584
Kalen Riley retweeted
30 Aug 2024
#ASHNR24 Less than a week to opening session of @ASHNRSociety with excerpta session presented by TRAINEES! CANT WAIT to see this team of 10 share their amazing cases with you! @ashasarm @MohitAgNeurorad @thecortexclub @RamVaidhyanath @ESHNRSociety @TheASNR #CaliforniaDreamin
9
21
2,442