🩺UK based Rheumatologist & Internal Medicine | Education | Arsenal Fan 35 Years -🏆🔴⚪️ | Just living the Dream ☔️| طب الروماتيزم | 🎬 🏋️♂️♟️🎱
- Tweets 2,203
- Following 476
- Followers 4,436
- Likes 799











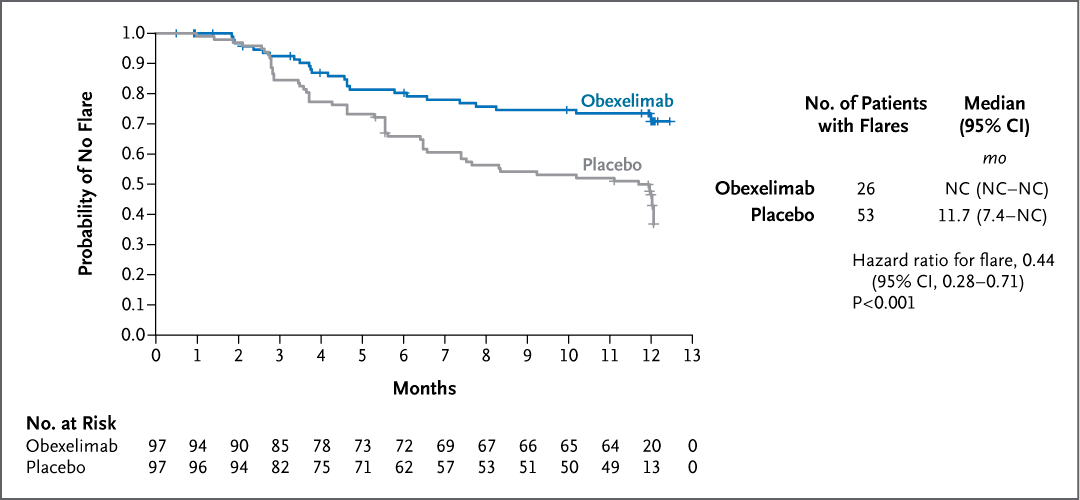
ALT Graph showing estimates over time of the probability of a first flare of IgG4-related disease for which rescue therapy was required. The y-axis represents the probability of no flare, ranging from 0 to 1, and the x-axis shows time in months. The blue line indicates obexelimab while gray line indicates placebo. Notable statistics detail patients at risk, number of patients with flares, and median times. The hazard ratio is 0.44 with a p-value of <0.001.
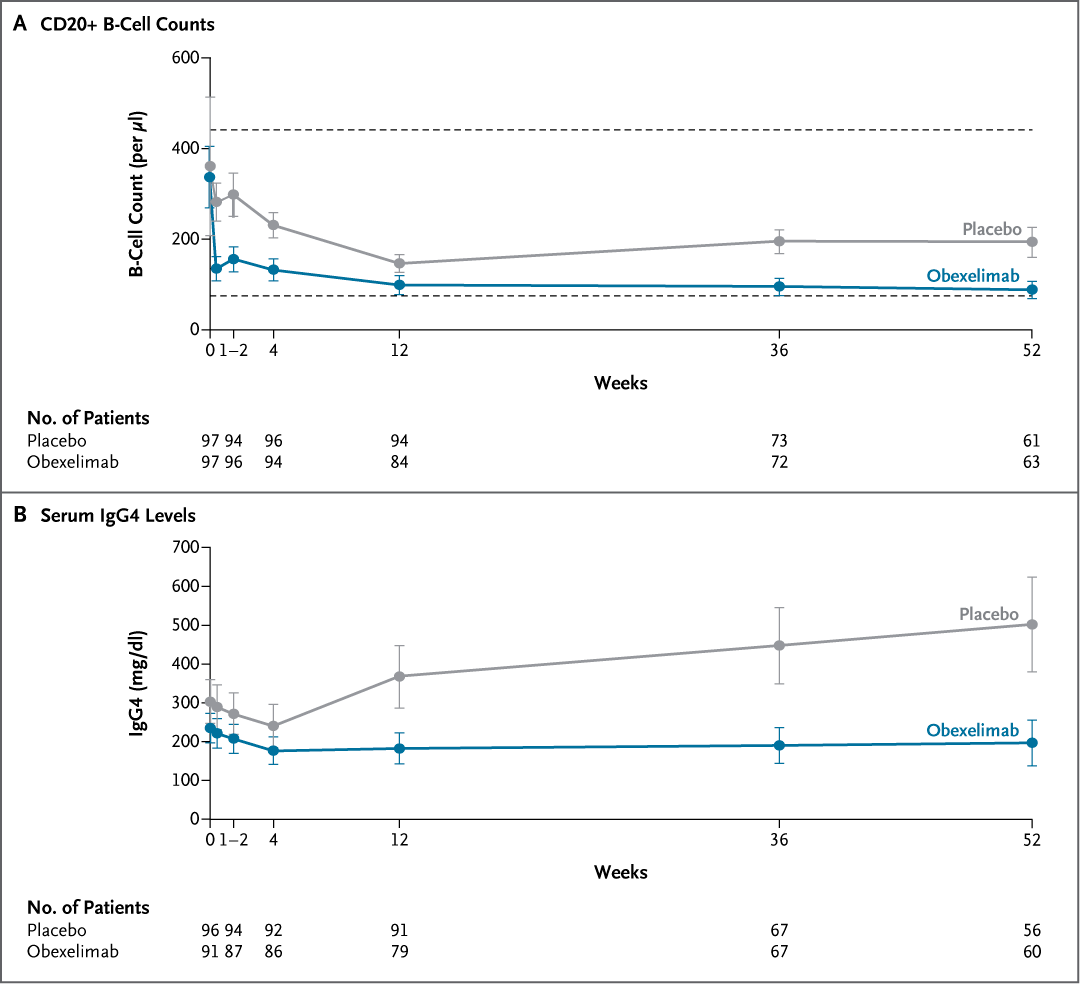
ALT The image displays two line graphs. The top graph shows CD20 B-cell counts over time in weeks, comparing placebo and obexelimab treatments. The bottom graph presents serum IgG4 levels. Both graphs include patient numbers at different stages.









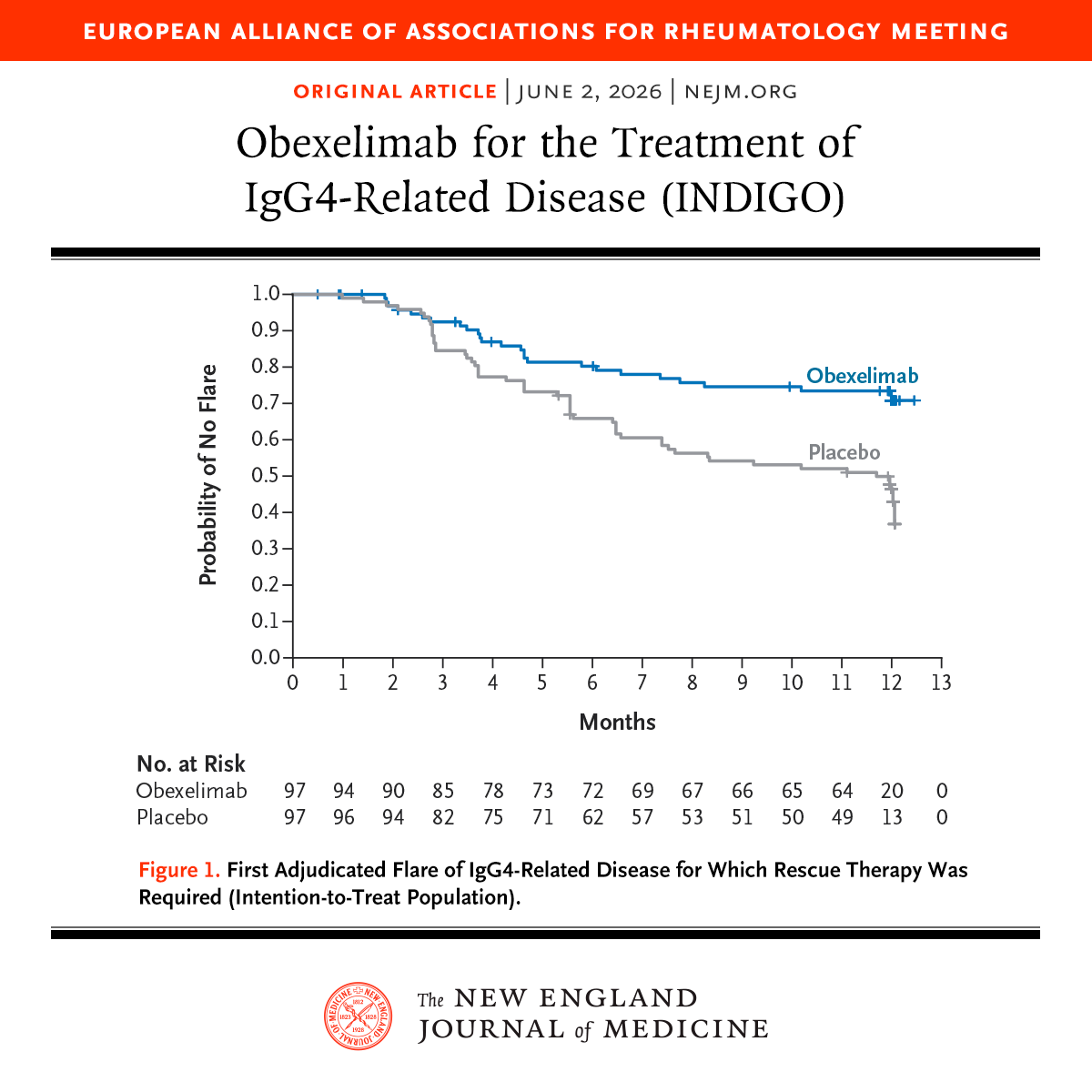
ALT A line graph from an article titled "Obexelimab for the Treatment of IgG4-Related Disease," which shows estimates over time of the probability of a first flare of IgG4-related disease for which rescue therapy was required. Below the graph is a footnote detail and the logo for the New England Journal of Medicine.