Lipidologist with over 30 years of clinical experience. Cofounder @PreciseHlthRpt. My passion is creating tools that optimize individual cardiometabolic care.
Joined April 2010
- Tweets 343
- Following 69
- Followers 6,417
- Likes 89
51 Photos and videos




13 Jun 2024
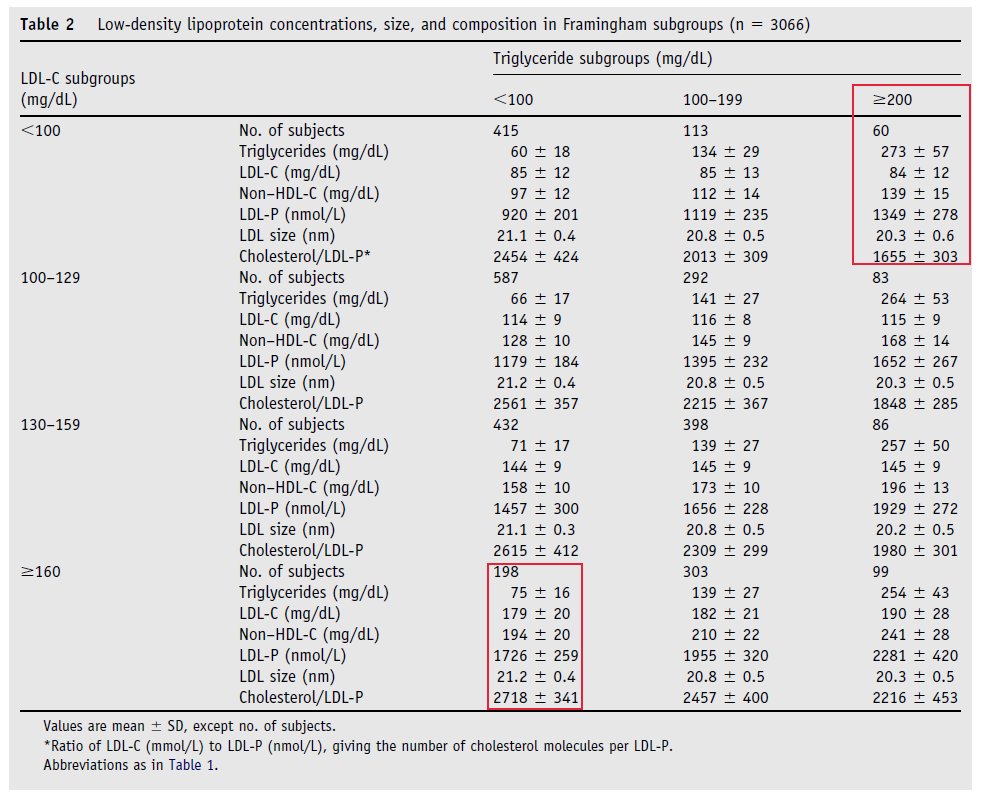
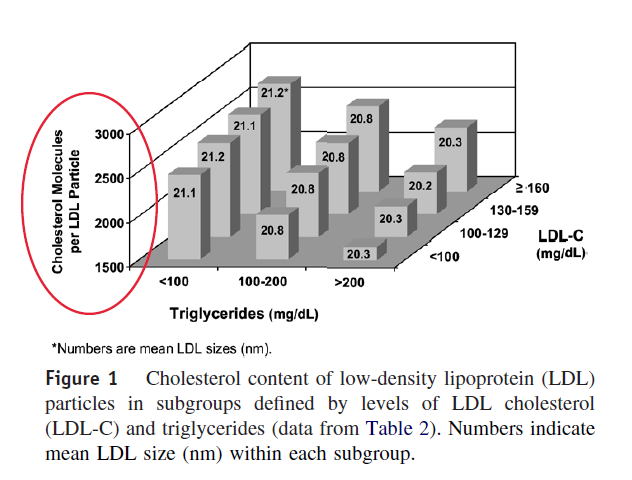
Depending on the data analysis employed, conflicting data have been reported over the past 30 years regarding the relationship of LDL particle size, particle number, and quantities of small LDL or large LDL particles with various ASCVD outcomes.
The interrelationships of particle size, particle number, and particle subclasses confound the strength of each biomarker's association with CVD risk.
Analyses that adjust for the confounding interactions between these measures yield uniquely different insights versus data that do not address this.
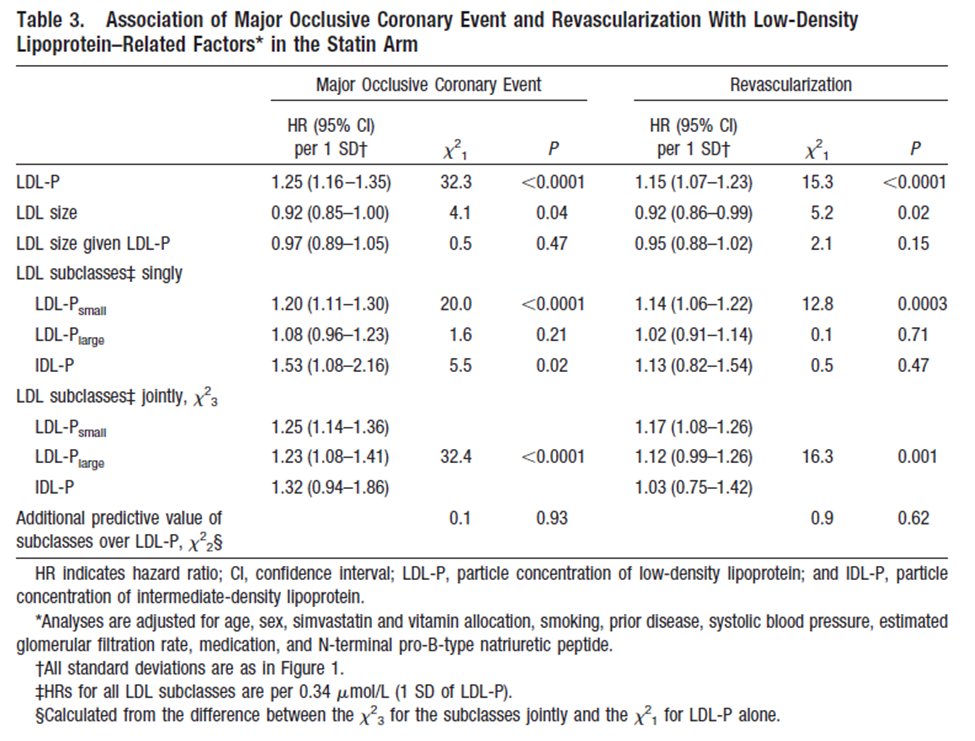
When LDL particle size and LDL particle number are adjusted for one another, only LDL particle number remains significantly predictive of events. (1-6)
Additionally, small LDL particles have a strong inverse relationship with large LDL particles. (6, 7)
In older reports that fail to adjust for this confounder effect, small LDL size appears more strongly related to CV risk than large LDL.
Data that address confounding of small and large LDL size demonstrate both small and large LDLs are significantly associated with CVD risk independent of each other, traditional lipids, and established risk factors, with no association between LDL size and CVD risk after accounting for the concentrations of the two subclasses. (6, 7)
Thus, rather than small dense LDL (sdLDL) being differentially atherogenic, analysis designed to address confounder variable effects demonstrates that small and large LDL particles have a similar strength of association with ASCVD risk.
These relationships underscore expert panel recommendations finding insufficient evidence to advocate measuring LDL size or subclasses to assist ASCVD risk assessment or management.
1. Contois JH, et al. Clin Chem. 2009;55:407-19.
2. Brunzell JD, et al. J Am Coll Cardiol. 2008;51:1512-24.
3. Lamarche B, et al. Circulation. 1997;95:69-75.
4. Mora S, et al. Circulation. 2009;119:931-9.
5. Blake GJ, et al. Circulation. 2002;106:1930-7.
6. Otvos JD, et al. Circulation. 2006;113:1556-63.
7. Mora S, et al. Atherosclerosis. 2007;192:211-7.
27
28
134
42,634
27 May 2024
Like many today, I pause to reflect and honor those who made the ultimate sacrifice so that we can live in freedom.
Thanks to all my brothers and sisters who answered the call. It was an honor to serve. 🇺🇸
1
40
5,672
25 May 2024
This short video illustrates how our thinking regarding various drivers of fatal and non-fatal outcomes has matured.
Having Jim Otvos as my research partner for over 25 years has been an honor. Our team has had the unique opportunity to explore the clinical relevance of analytic improvements in lipoprotein quantification and discover new individual and multi-markers that extend our understanding of disease behavior and clinical management.
As I enter my 36th year in lipidology, we are moving in the right direction regarding understanding complex outcomes and improving individual shared decision-making conversations about cardiometabolic risk assessment and management.
Beyond individual risk factors and risk calculations, optimal care now requires integrating clinical history, nearly 40 risk-enhancing factors, outcome-proven biomarkers, and harmonizing various guidelines to inform a personalized, shared decision-making conversation.
@PeterAttiaMD has been a leading voice in exploring opportunities to transition to this next-level approach in individual care. It would be a pleasure to have a conversation with him to explore these ideas and opportunities for precision cardiometabolic care.
@PeterAttiaMD
24 May 2024

☠️ApoB and All-Cause Mortality☠️
🚨My Most important Tweet (and video) of the Week
WATCH (10m): youtu.be/sAjDjLJUlQQ
High level: There is controversy over the relationship between ApoB and All-Cause Mortality (ACM), with some noting a J-curve whereby at lower levels of ApoB mortality is higher. BUT...
👉We must ask: what are/is the major driver of ACM?
👉Answer: Metabolic Vulnerability
Metabolic Vulnerability can now be quantified with a multi-marker (MVX), which constitutes a metabolic "signature" suggestion a complex of nutritional and inflammatory disfunction. And MVX is GREAT at predicting ACM.
One can conceptualize MVX as the background noise if one is looking at the impact of ApoB on ACM: it's like dropping a pebble into white water rapids... you won't see a ripple because the background is too strong.
BUT, if you "still" the water (account for MVX), the relationship can change... and the J-curve can transform into a straight line!
What are the consequences?
Additional nuances?
You'll have to watch the video to find out!
I review:
👉Signal-to-noise ratio with respect to ACM
👉Drivers of Fatal vs Non-fatal events
👉Metabolic "Signatures"
👉Weighing the costs of intervention
Major ht/ to @Lipoprotein (for references and education) and @theproof (for great 5 hour chat that you should definitely check out when it drops on his podcast... ⚠️WARNING: WILL BE PROVOCATIVE⚠️)
Please engage. Watch the full video, and comment thoughtfully: youtu.be/sAjDjLJUlQQ
5
6
55
15,765
William Cromwell, MD retweeted
12 Jul 2023
Whether statins meaningfully increase Lp(a) has been the topic of spirited discussion.
Last year, de Boer LM et al. published a comprehensive review and meta-analysis of the effect of statins compared to placebo on Lp(a) in the European Journal of Preventive Cardiology.
Their conclusion, “Statin therapy does not lead to clinically important differences in Lp(a) compared to placebo in patients at risk for CVD. Our findings suggest that in these patients, statin therapy will not change Lp(a)-associated CVD risk.”
12
20
102
40,618
22 Jan 2024
Substantial LDL cholesterol elevations are well documented among some lean individuals on a low-carb, ketogenic diet.
This “metabolic demonstration” illustrates how robust and rapid LDL reductions can be in an individual experiencing this phenotype when carbohydrates are added to a chronic low-carb, ketogenic diet.
mdpi.com/2218-1989/14/1/73
22 Jan 2024
🚨#OreoVsStatin - PUBLISHED!🚨
mdpi.com/2218-1989/14/1/73
@Oreo cookies were 💥2X as potent💥 at lowering my LDL cholesterol (LDL-C) compared to high-intensity statin therapy!
What you NEED to know...
👉This was a metabolic demonstration, a 'do not do this at home' experiment that makes no 'health' claims about cookies or cholesterol.
👉The purpose was to BOLDLY test a prediction of the Lipid Energy Model #LEM, i.e. that adding in carbs, including in the from of an Oreo cookies 'addition' (not carb-fat swap) would lower LDL-C in an LMHR on a #keto diet
Why Oreos? ... It's (productively) provocative! 😱
Research on #cholesterol on #keto diets and the #LEM and #LMHR phenotype has so much to teach us about human lipid metabolism! ...
But how do I (we) communicate the scientific 'awe' that we feel to the greatest number of people (as well as force a conversation about #LMHR and #LEM that needs to happen)? ... A dramatic demonstration designed to turn heads might work!
It's not 'just click bait' ... it's 'legit-bait'
I want YOU to feel the 'shock and awe' I feel every day studying this topic. And I want you to engage in the research journey.
What you need to do... or should do... 🙏PRETTY PLEASE 🙏!
👉PLEASE WATCH 👀 VIDEO ABSTRACT here (<8 min): youtu.be/L1mMnnyJrgk
👉 SHARE THIS LINK to the paper itself in a quote RT or original Tweet of your own: mdpi.com/2218-1989/14/1/73 ... doing so helps promote the work and provoke the discussion
... and feel free to tag in your favorite influencers (or least favorite 😉)...
A HUGE thanks to the senior author and expert lipidologist @Lipoprotein for his guiding wisdom, insightful thoughts, and always open and curious mind.
And to @realDaveFeldman, my friend, research wife, and the '#LEM daddy'
Finally... there will be a LOT of coverage of this experiment. Keep in mind, we are not making any health claims, but through a dramatic demonstration, highlighting an uncomfortable tension that arises from a prediction of the Lipid Energy Model, and that is consistent with prior data (7 papers, including 'highest tier' data like our recent meta-analysis of 41 RCTs).
Science is supposed to embrace such uncomfortable questions... so, join us in being curious and advocating for much needed research on #LEM and #LMHR so we can make sense of what observations like this really mean... STAY CURIOUS 🤔
5
32
134
33,182
24 Jul 2023
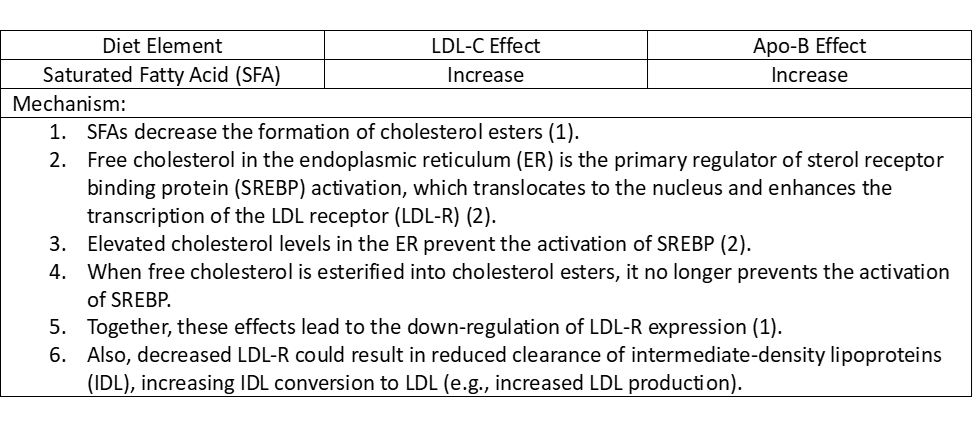
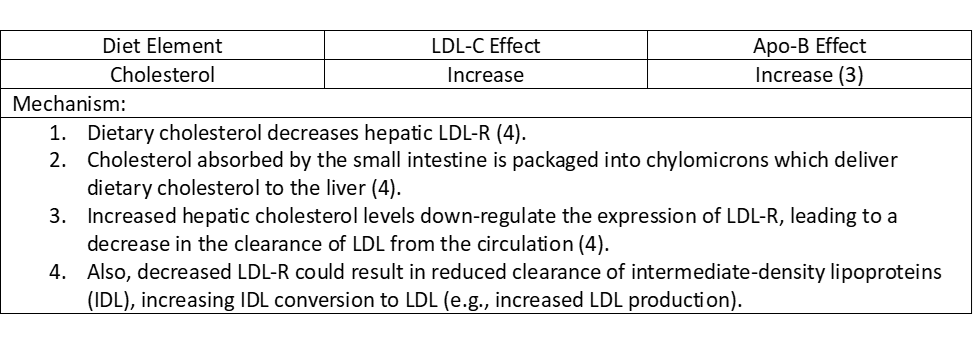
Several recent posts have asked for references elucidating the relationship between increased saturated fatty acids and dietary cholesterol and decreasing LDL receptor (LDL-R) quantity.
I recommend starting with this review:
Feingold KR. The Effect of Diet on Cardiovascular Disease and Lipid and Lipoprotein Levels. [Updated 2021 Apr 16]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: ncbi.nlm.nih.gov/books/NBK57…
Below are tables I constructed from the review that summarize the mechanisms underlying LDL-R down-regulation:
1. Fernandez ML, West KL. J Nutr.2005;135:2075–2078.
2. Dietschy JM. J Nutr. 1998;128:444S–448S.
3. Ginsberg HN, Karmally W, et al. Aterioscler Thromb Vasc Biol. 1995;15:169-178.
4. Grundy SM. Does Dietary Cholesterol Matter? Curr Atheroscler Rep. 2016;18:68.
7
22
106
28,346
William Cromwell, MD retweeted

10 Jul 2023
How easy is getting your Cardiometabolic Risk Assessment completed?
Literally 3 quick steps.
precisionhealthreports.com/o…
4
7
4,322
29 Jun 2023
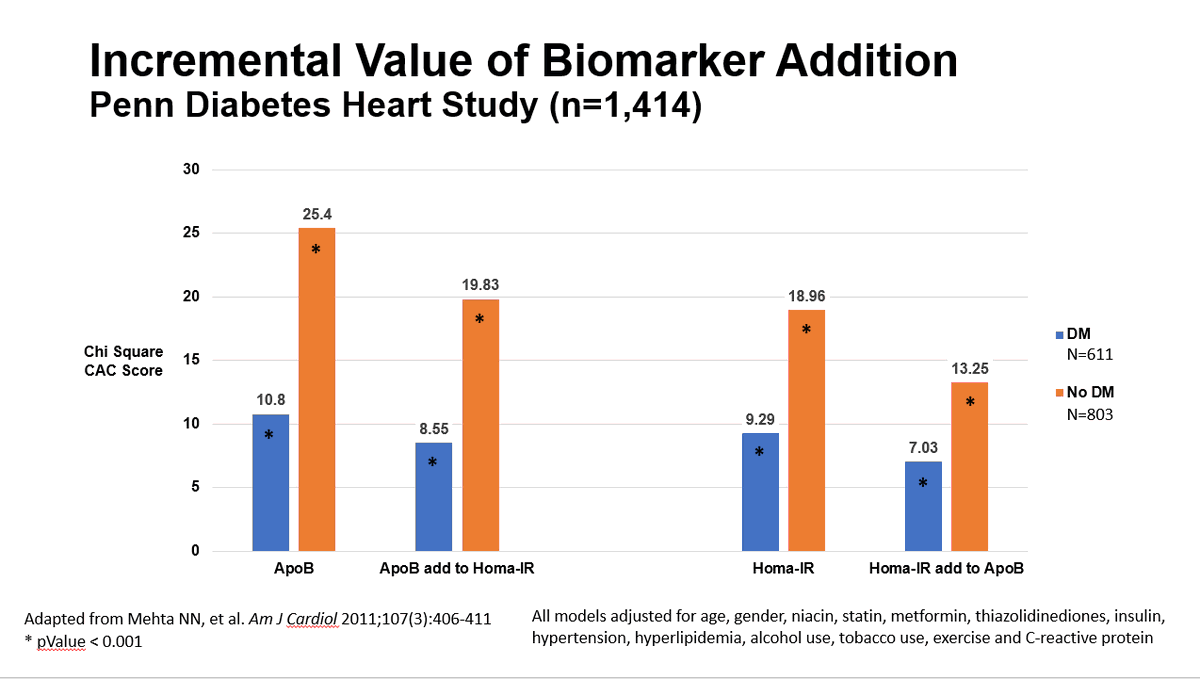
Both insulin resistance (IR) and ApoB are significantly associated with ASCVD risk. Whether one factor adds significant incremental risk information to the other has been the subject of brisk debate.
To address this issue, two fundamental questions must be asked:
1. Are IR and ApoB each significantly predictive of ASCVD risk in a series of models that progressively adjust for base cofactors (BC), BC metabolic syndrome (MS), and BC MS the other variable (IR or ApoB)?
If each continues to have significant predictive value despite these progressive adjustments, then each variable significantly contributes to ASCVD risk.
2. What is the impact of adding one factor (IR or ApoB) to the other in a model adjusted for cofactors?
A Chi-Square analysis of adding IR to ApoB, or ApoB to IR, in models adjusted for cofactors gives insight into the incremental value of the added variable. The higher the Chi-Square, the greater the incremental value of the added variable.
The Penn Diabetes Heart Study assessed the predictive value of HOMA-IR and ApoB for coronary artery calcium (CAC) score in a cohort of 611 diabetic and 803 non-diabetic adults. This study showed:
1. HOMA-IR and ApoB were EACH significantly predictive of CAC in models adjusted for BC MS the other variable (HOMA-IR or ApoB).
2. The addition of ApoB to HOMA-IR, as well as the addition of HOMA-IR to ApoB, added significant incremental risk prediction versus the model with HOMA-IR or ApoB alone (see figure below).
These data support that BOTH IR AND ApoB are significant, independent predictors of ASCVD risk and that EACH adds important incremental risk prediction to the other.
15
31
155
65,976