
Masters in Nutrition Science & Bachelor of Science (Physio). Author and podcast host. Science over hyperbole. Tweets are educational only, not medical advice.
Joined October 2019
- Tweets 18,310
- Following 1,427
- Followers 35,957
- Likes 8,760
1,860 Photos and videos





Pinned Tweet

Mar 26
What happened to the clinical study that Shawn Baker was raising money for? Was that study conducted, or if not, where is the money?
22
15
163
23,739
Simon Hill MSc, BSc retweeted

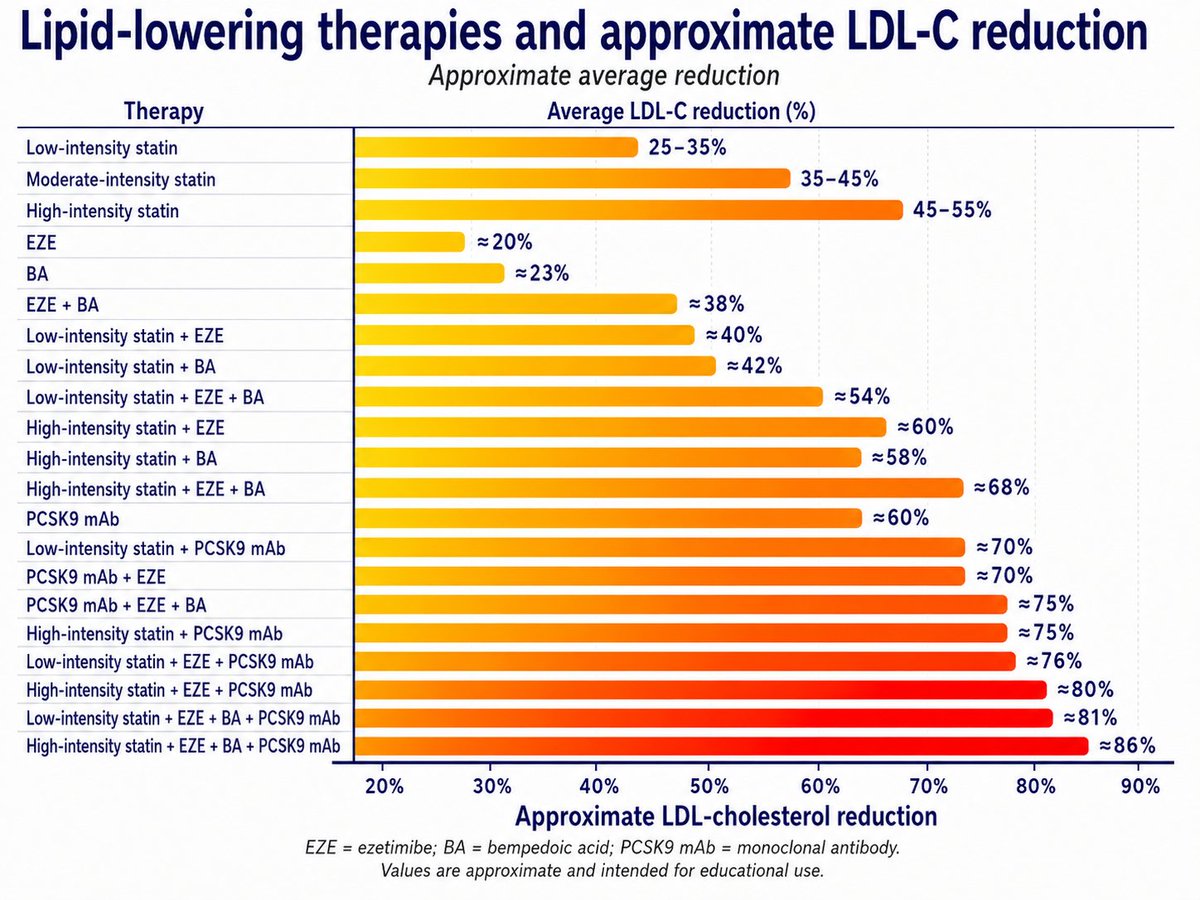
When LDL-C is far from target, don't just double the statin and hope. Combination therapy beats simply pushing one drug to the max, because stacking complementary mechanisms gives larger LDL-C reductions than dose titration.
1. pubmed.ncbi.nlm.nih.gov/4087…
2. pubmed.ncbi.nlm.nih.gov/3913…
1
6
16
856
The Anabolic Window Might Be One of Fitness' Biggest Myths. | EP#406
youtu.be/ZtaKRdV5pi8
2
4
16
5,841
Jun 12
Fair?
Jun 12

So typical of that crowd
2
2
2,948
Simon Hill MSc, BSc retweeted
Jun 12
I am going to try a ketogenic diet a parachute and jump out of a plane.
2
1
21
2,601
Simon Hill MSc, BSc retweeted

Jun 11
Someone asked this account today: "Name one RCT showing keto does not reduce cardiovascular events!"
Sounds reasonable. It is not.
The keto "health influencers" are making an emphatic claim that keto is safe for your heart. Specifically the program or supplements they want you to pay for.
There has never been a keto cardiovascular outcomes trial. Not one. Which means the keto community has no evidence that keto reduces events.
They have surrogate markers, anecdotes, and a one-year preprint with no control group. That is the entire positive evidence base for a claim about the number one cause of death.
So they invented a better move. Flip the burden. Demand that critics prove the negative. Now the absence of a harm trial becomes a shield.
"You cannot prove it hurts us."
Here is how this works everywhere else. A drug company cannot go to the FDA and say "name one trial showing our drug increases mortality."
They have to prove it works. The burden sits with the claim, not with the skeptic.
The claim is that keto is cardiovascularly safe. Possibly even beneficial. That claim needs a trial. Not a demand that someone else disprove it.
Most people fall for the move. Now you will not.
You have a parachute. Use it.

11
13
57
2,764
Jun 11
Nutrition Scientist Dr. Federica Amati: Why It's So Hard to Lose Weight and Keep It Off
youtu.be/rMznfyxTX7M
2
1
9
1,825
Simon Hill MSc, BSc retweeted

I had a great chat with my amazing Aussie friend, @theproof We talked about aggresive prevention, the dangers of life optimization, the future of GLP1ra, MASLD and a little bit of what i have learned communicating on social media. I hope you enjoy the episode when it comes out.
Jun 10

Had a great conversation yesterday with @DrMauinforma which will be on The Proof channels soon.
We had been talking about this episode for about eight years. Far too long … left the conversation grateful for the value that will be provided to our listeners but also regretting that it had taken so long to make this happen.
We focussed on metabolic health, cvd, and how medicine has changed over the past decade. I learned a lot.
6
20
3,189
Jun 10
Nutrition Scientist Dr. Federica Amati: Why It's So Hard to Lose Weight and Keep It Off
youtu.be/rMznfyxTX7M
1
1
6
1,481
Jun 10
Had a great conversation yesterday with @DrMauinforma which will be on The Proof channels soon.
We had been talking about this episode for about eight years. Far too long … left the conversation grateful for the value that will be provided to our listeners but also regretting that it had taken so long to make this happen.
We focussed on metabolic health, cvd, and how medicine has changed over the past decade. I learned a lot.
3
1
12
5,442
Simon Hill MSc, BSc retweeted

Jun 10
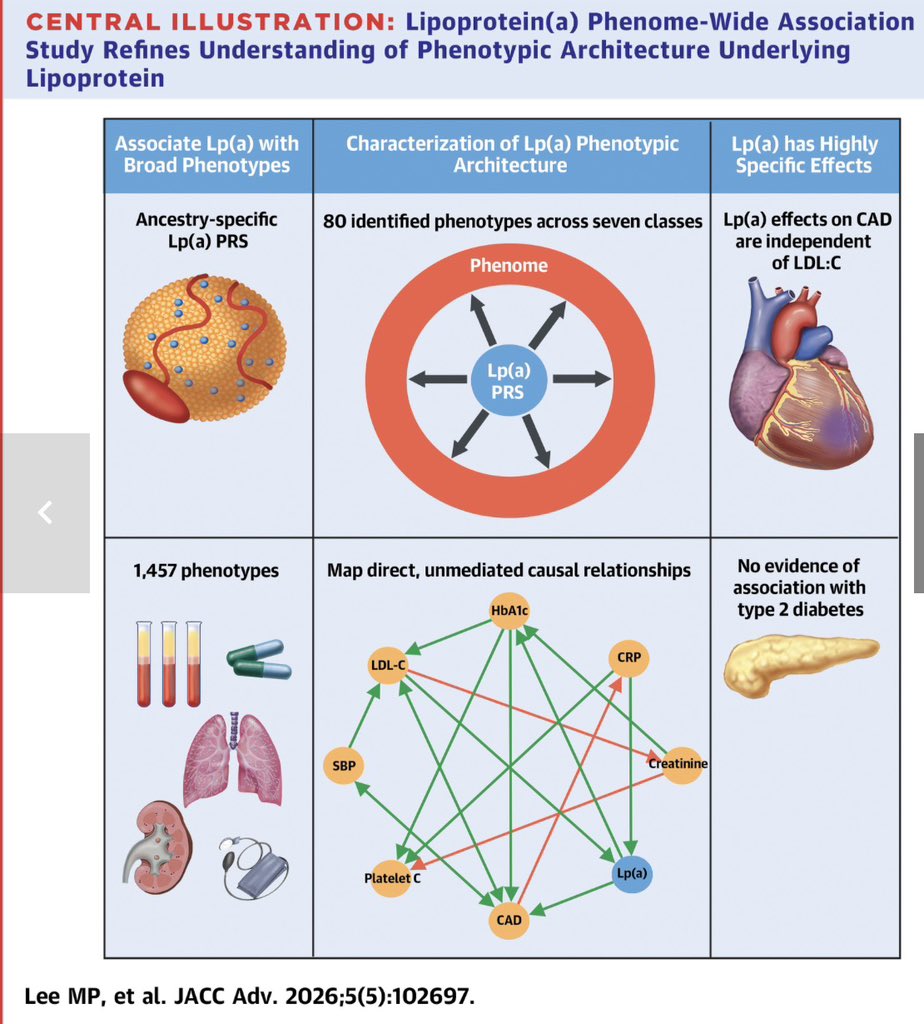
👉This new Mendelian randomization study, including more than 425,000 participants from the UK Biobank, provides important insights into the specific causal effects of Lp(a) and its implications for future Lp(a)-lowering therapies.
☝️Top 5 Take-Home Messages
1️⃣ Lp(a) exerts a direct causal effect on coronary artery disease (CAD), independent of LDL-C. This reinforces that Lp(a) is not simply another LDL particle, but an independent driver of atherosclerosis.
2️⃣ Among 1,456 phenotypes analyzed, only CAD and HbA1c showed direct causal effects of Lp(a). Most other associations appear to be indirect or mediated through other pathways, highlighting the remarkable specificity of Lp(a).
3️⃣ Very low genetically determined Lp(a) levels were not associated with a higher risk of type 2 diabetes. These findings provide reassuring evidence for the long-term safety of profound Lp(a)-lowering therapies currently under development.
4️⃣ The optimal Lp(a) threshold for myocardial infarction risk discrimination was ~86 nmol/L in Europeans and ~93 nmol/L in Africans, suggesting that clinically relevant risk may begin at lower levels than the current 125 nmol/L cutoffs adopted by many guidelines.
5️⃣ The study supports treating LDL-C and Lp(a) as complementary but distinct cardiovascular risk factors. Even with optimal LDL-C control, elevated Lp(a) remains a causal contributor to coronary disease, emphasizing the need for dedicated Lp(a)-lowering strategies.
☝️Bottom line: Lp(a) appears to have a highly specific causal role in coronary atherosclerosis, independent of LDL-C, while concerns about diabetes risk from very low Lp(a) levels are not supported by this large Mendelian randomization analysis.
🔓🔗 jacc.org/doi/10.1016/j.jacad…
@society_eas
@nationallipid
@JACCJournals
8
28
110
7,139
Jun 10
Most of the GLP-1 conversation is still about the drugs, not the biology they operate within. What are three types of hunger? What are the four phases of satiety? And what does "prehab" actually mean before starting medication?
In this episode, I sat down with Dr Federica Amati, Head Nutritionist at ZOE and author of The Appetite Reset, to unpack the science of appetite for everyone, on or off medication.
For the full show notes head to: theproof.com/nutrition-for-s…
3
17
1,904
Jun 9
Nutrition Scientist Dr. Federica Amati: Why It's So Hard to Lose Weight ... youtu.be/rMznfyxTX7M?si=OHMW… via @YouTube
1
6
1,540
Jun 9
What are your thoughts on the increased heart rate observed when on retatutride (compared to Tirzepatide).
4%
Likely good for longevity
61%
Likely bad for longevity
35%
Doesn't matter
122 votes • Final results
16
8
7,413
Simon Hill MSc, BSc retweeted

Treat the Plaque. Not the Risk Factors.
For decades, preventive cardiology has largely operated under a simple assumption:
Measure risk factors.
- Estimate risk.
- Treat risk.
But there is a problem.
Many myocardial infarctions occur in patients who would never have qualified for aggressive prevention based on conventional risk scores alone. Meanwhile, many individuals with multiple risk factors will never experience a cardiovascular event.
Why?
Because risk factors are not the disease.
Atherosclerosis is the disease.
A patient does not suffer an MI because their SCORE2, PCE, LDL, ApoB, hsCRP, or Lp(a) is elevated.
They suffer an MI because they have developed coronary atherosclerosis.
Yet we continue to spend enormous effort measuring surrogates while often ignoring the organ that actually matters: the coronary arteries.
This review argues that coronary CT may allow a shift from population-based prevention toward disease-based prevention. Not by predicting who might develop atherosclerosis, but by directly visualizing who already has it.
Perhaps the most provocative observation is that, in large contemporary cohorts, total plaque burden and non-calcified plaque often outperform stenosis severity itself as predictors of future events.
That should make us pause.
For years we have been obsessed with narrowing.
Meanwhile, the disease was sitting in the vessel wall.
The future of prevention may not be:
👉 Treat the cholesterol.
👉 Treat the inflammation.
👉 Treat the risk score.
The future may be:
- Identify the plaque.
- Quantify the plaque.
- Track the plaque.
- Treat the plaque.
Everything else is a surrogate.
#CardiacCT #CCTA #Atherosclerosis #PreventiveCardiology #TreatThePlaque #CardiovascularImaging #PrecisionMedicine #PhotonCountingCT #PCCT
10
27
55
4,872
Simon Hill MSc, BSc retweeted
Jun 8
This might be the only one shot (excuse the pun) to say Tom...that's wrong!
Sorry I had to. We are due for a call.
2
1
7
3,296
Simon Hill MSc, BSc retweeted

Jun 8
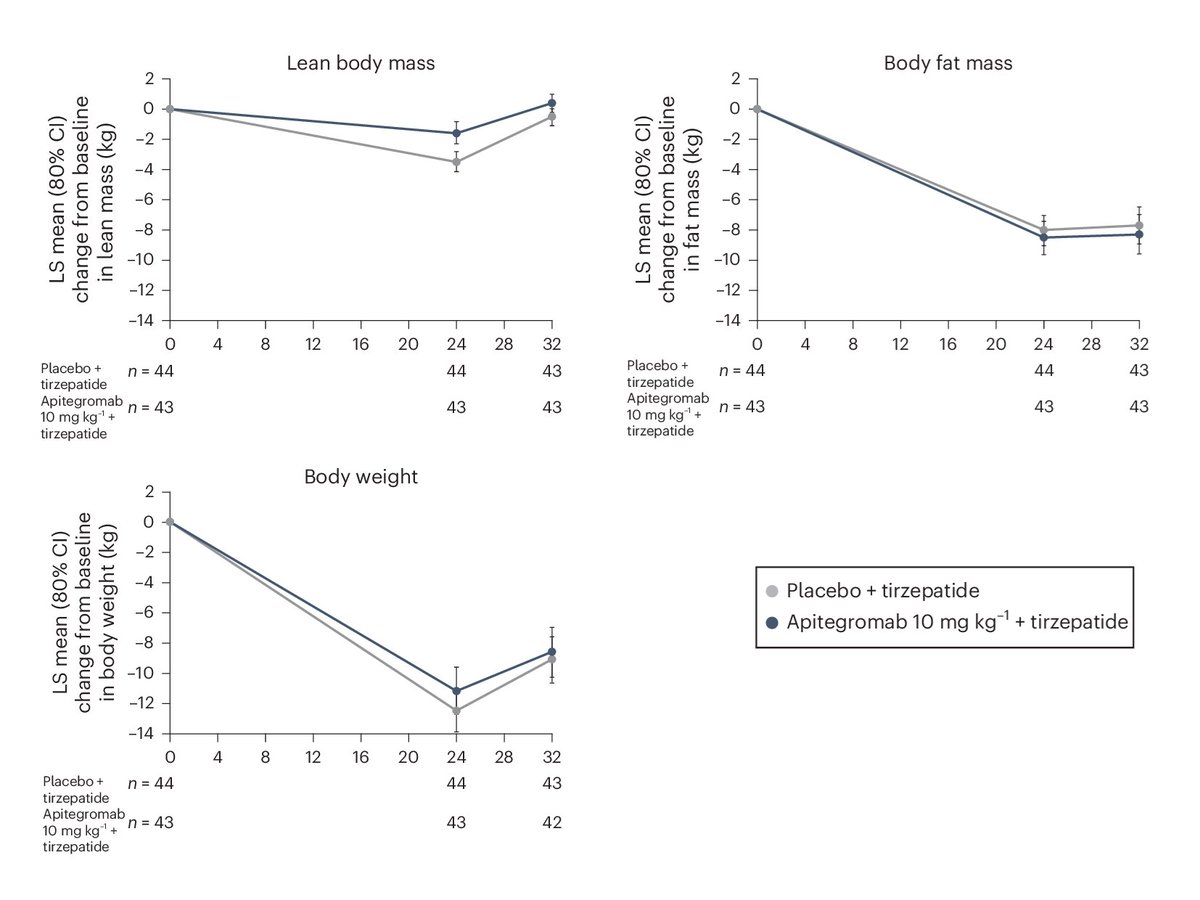
New myostatin inhibitor results!
Over 24 weeks, people on tirzepatide lost ~30% of body weight as lean mass.
People on tirzepatide plus a myostatin inhibitor lost ~15% of body weight as lean mass!
It'll soon be possible to lose weight while barely losing muscle!
42
45
615
57,409
Jun 8
Interesting thoughts shared here by @RonKarlsbergMD on genetics and CAD.
"multiple previously unrecognised causes of CAD"
I assume a major one of these being LP(a). What others should be on that list?

That is the correct observation, and by doing so we can now tackle the multiple previously unrecognized causes of CAD, including the 50% of the disease attributable to genetics and heredity that are not necessarily related to the LDL pathway. This is then the path to plaque-directed therapy and the mitigation and eradication of the disease. #plaquedirectedtherapy
5
8
4,514
Simon Hill MSc, BSc retweeted

That is the correct observation, and by doing so we can now tackle the multiple previously unrecognized causes of CAD, including the 50% of the disease attributable to genetics and heredity that are not necessarily related to the LDL pathway. This is then the path to plaque-directed therapy and the mitigation and eradication of the disease. #plaquedirectedtherapy
1
1
9
5,633
Jun 8
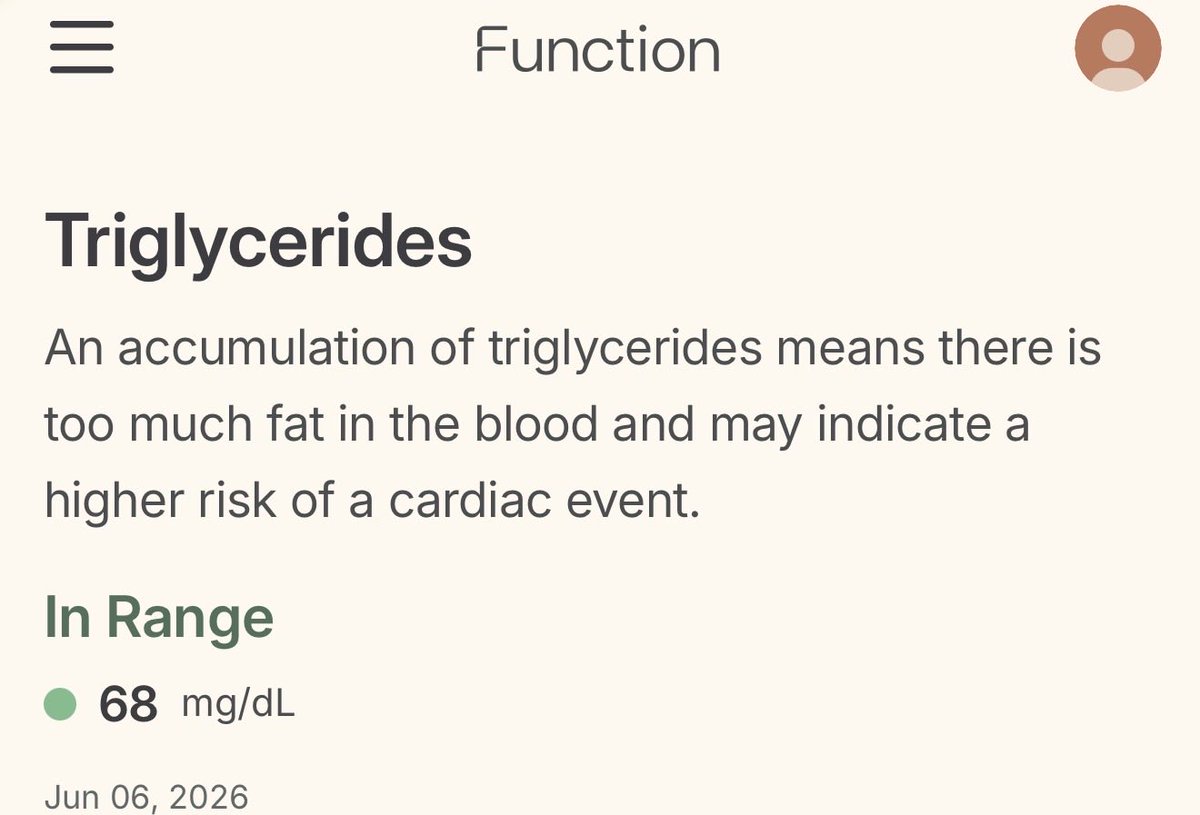
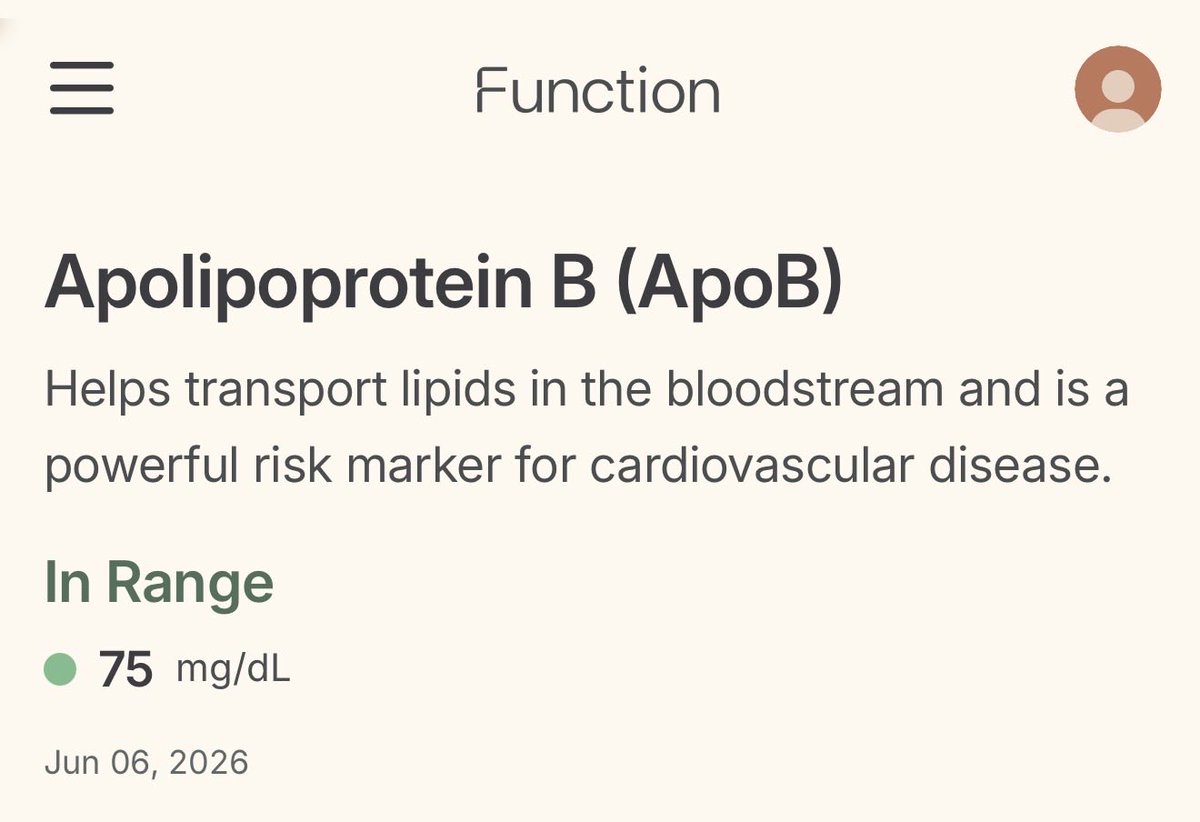
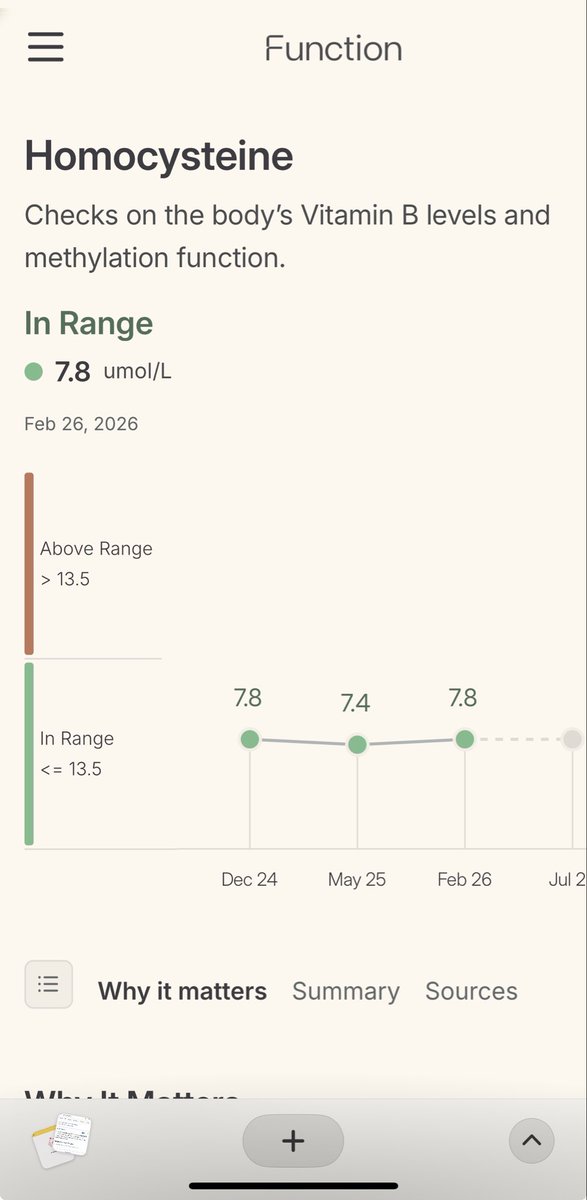
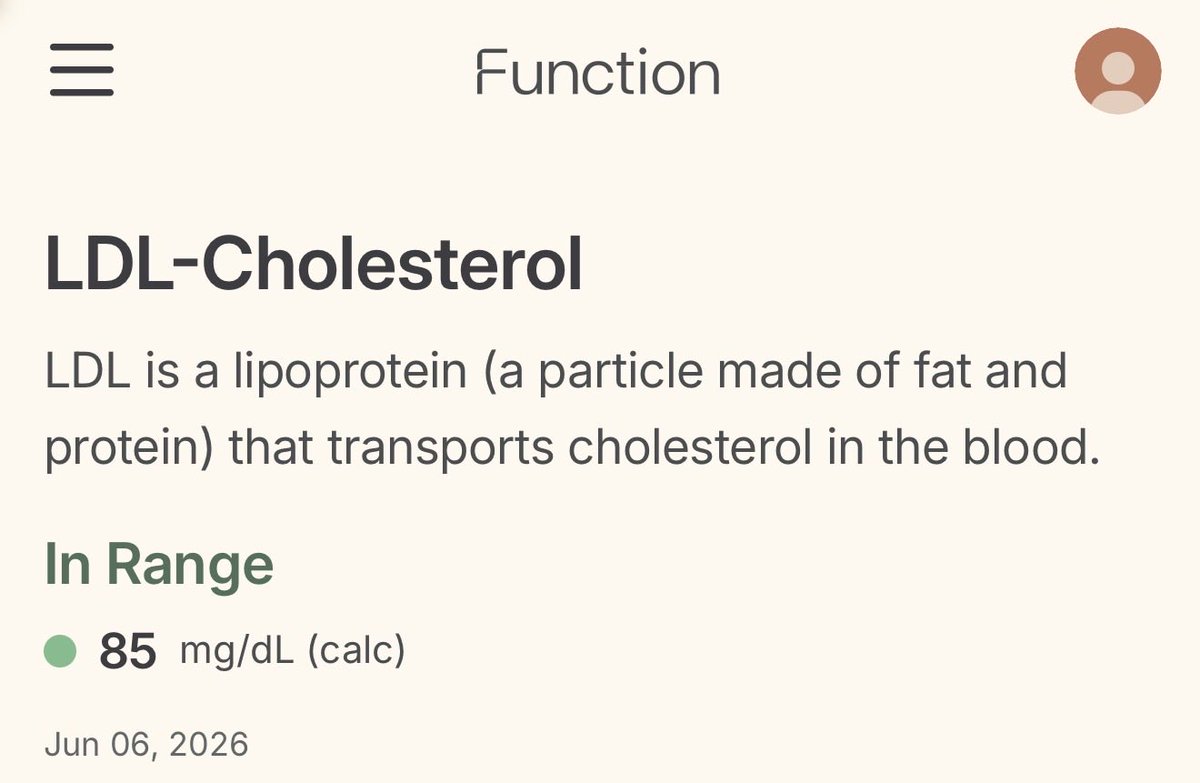
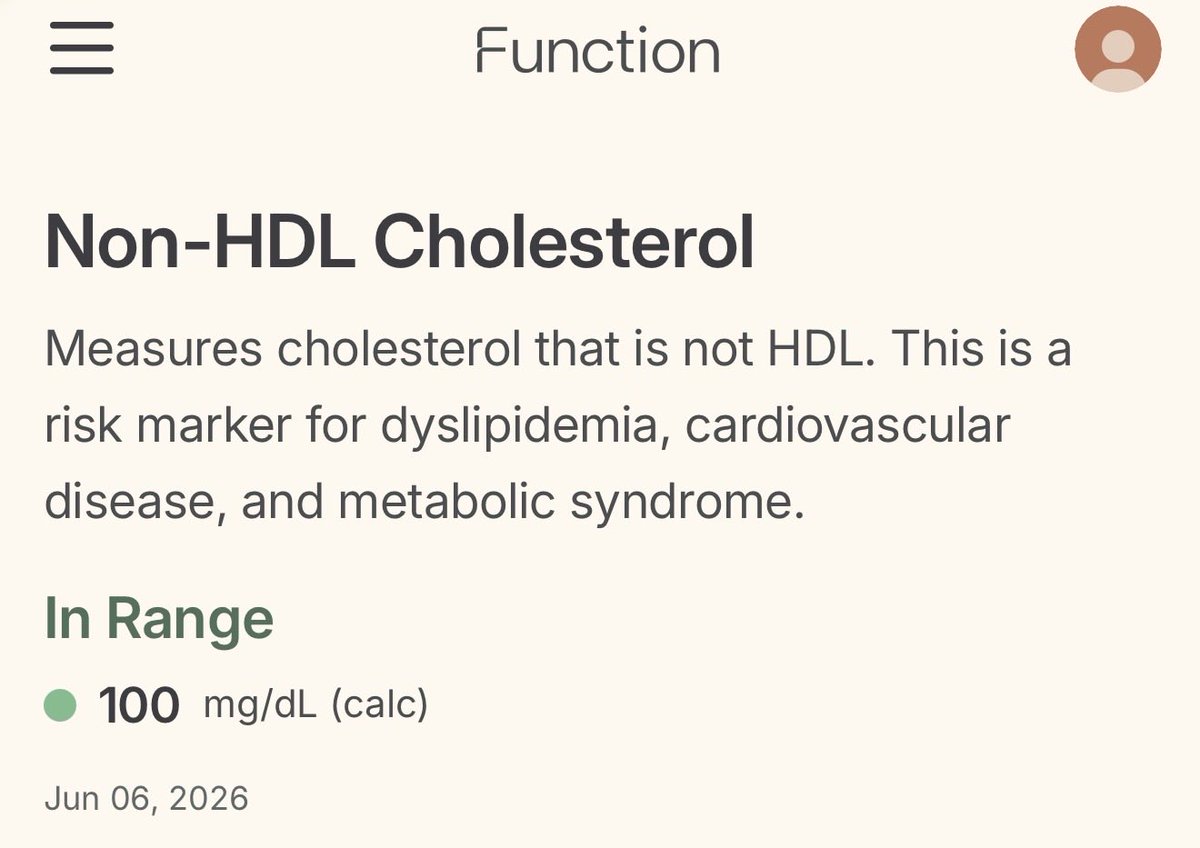
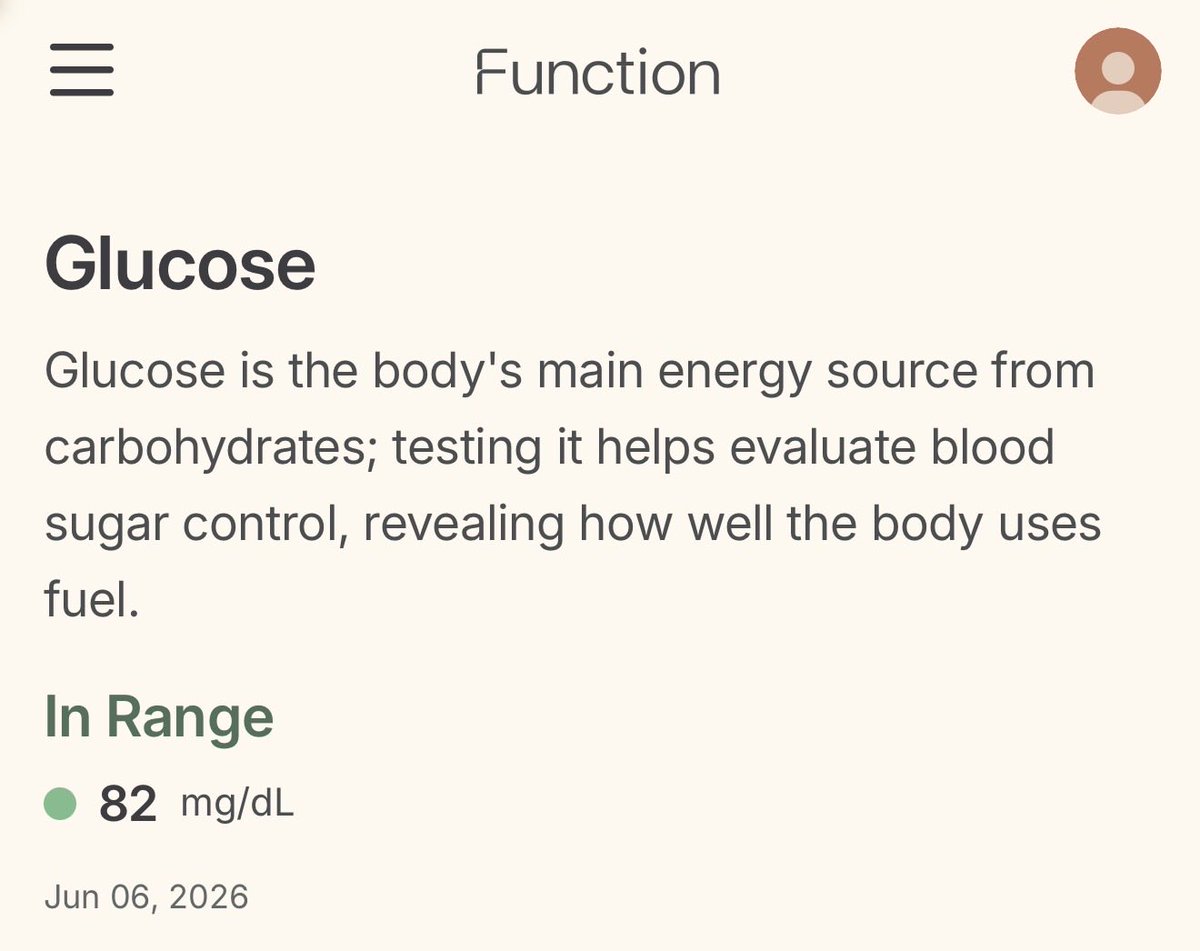
Some of my latest labs with @function
Note these lab tests are before commencing lipid lowering therapy (my baseline). Point being my goal is to get ApoB down from 75 mg/dl (where I sit with diet/lifestyle alone) to under 50 mg/dl.
Why? Details to come on YouTube
youtube.com/@theproofwithsim…
20
5
41
6,597
Jun 8
For more details ⬇️
Jun 8
Feeling extremely lucky to live in 2026 and have access to such incredible medicine and clinical research.
On the eve of my 40th I had my first dose (monthly injection) of a new treatment that I’m hopeful will prevent me from ever having a heart attack or stroke.
This drug will shift my physiology towards those who won the genetic lottery when it comes to atherosclerosis. I won’t get the benefit from birth but I’ll have it from here on out.
Why take this drug?
Well, full details to come in a series of YouTube which will also include my very own serial CTA angiogram results from the Lundquist Institute.
For now here’s some background information:
I had two scans done so I could see my baseline level of plaque and annualised plaque progression.
These scans were done under the supervision of @BudoffMd using the same machines/tech (Qangio and Heartflow analysis) as done in the latest Keto-CTA study (led by @realDaveFeldman) allowing for a reasonable comparison group (metabolically healthy individuals without a prior cvd event not on lipid lowering therapy). Yes I’m an n=1 and comparing myself to the mean has limitations but it’s helpful for me as an individual.
The main difference being that at age 29 I changed to a high fibre low saturated fat diet which lowered my LDL-C and ApoB to 70-90 mg/dl over the last decade.
In KETO-CTA 21% had a PAV annual change of 1% or higher by QAngio. That’s considered rapid progression. And total plaque grew by 18.7 mm3 per year on average (mean 18.7 mm3/median 6.6mm3).
I can also compare my results to Nature-CT - a great new study performed by @RonKarlsbergMD with annualised plaque progression for untreated (not on lipid lowering therapy) adults with average LDL-C of 111mg/dl. Over 5 years the group median non-calcified plaque nearly doubled. Total plaque grew by 6.7 mm3 per year (much less than KETO-CTA) despite 54% having a CAC of 0. Showing plaque progression in untreated adults with ‘normal’ cholesterol levels.
Episodes with CT imaging experts and clinicians will be found on my YouTube channel and made freely available so you can understand the science and decision making process here - and perhaps apply it to yourself with your own doctor.
Any guesses of what drug this is?
Hint: it’s thought to act peripherally - doesn’t cross the blood brain barrier. And it acts in circulation but its desired effect plays out at the liver (hepatocyte).
youtube.com/@theproofwithsim…
1
1
7
1,918