
Heart Surgery-MarinHealth, CA. Tips/Techniques to facilitate heart surgery. All my opinions based on personal experience. Yolopactli/ticitl
Joined August 2012
- Tweets 1,491
- Following 263
- Followers 2,302
- Likes 297
307 Photos and videos










50 y.o woman treated for “HTN & chronic headaches” for decades. Thought weak legs after walking was normal. Finally got a CT chest; revealed the real problem. Simple surgical fix: 24Fr Ao‑to‑Ao bypass. She feels like a new person. Reminder to keep differential wide.
2
6
680
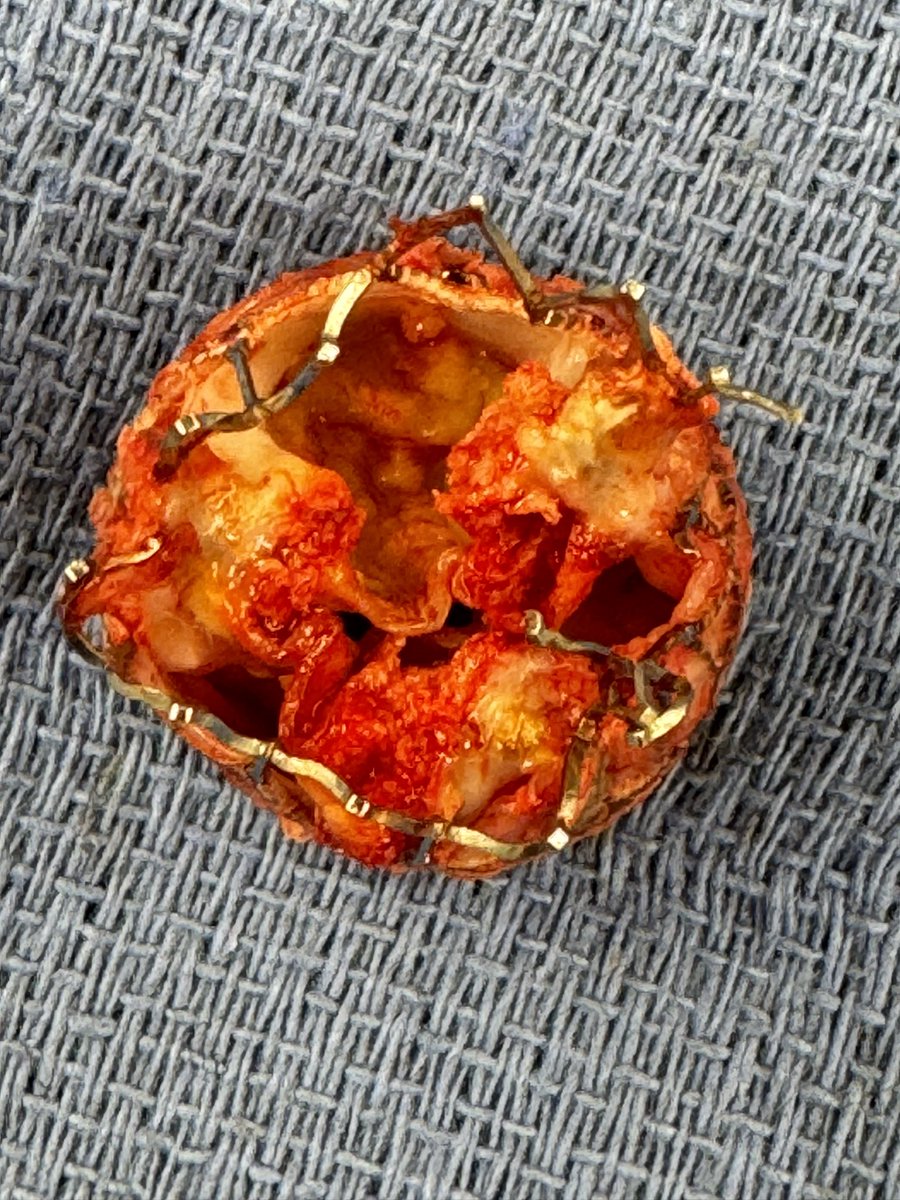
72 yo w h/o bicuspid AS S/P TAVR 5yrs ago, now severe stenosis of implant. Explant revealed massive calcification & dense pannus. Hard to imagine Tavr in Tavr. Standard root enlargement enabled safe implantation of a 29 mm Epic. @DrZeigler1 @JCoselli_MD @Abedeanda @tomcnguyen


3
8
41
4,671
Use of an Intraoperative Head, Neck, and Back Support... : Annals of Surgery journals.lww.com/annalsofsur…
3
789

6 Nov 2025
Not all aortic valves come out clean. This one was heavily calcified... had to be cut out in several pieces. Mean gradient 74mmHg. Conduction system intact, annulus fully debrided, and a 29 mm prosthesis seated smoothly in a super athletic man.
2
1
17
1,799

6 Aug 2025
Excising an aortic valve as a single piece is a skill set developed when learning to properly detach leaflets at the annular insertion. No need to "tear & pluck" at leaflets & calcium. Almost no annular debridement required. SAVR, w 29mm Abbott Epic valve via mini sternotomy.
4
3
40
2,236
Luis J Castro MD retweeted

14 Feb 2024
on my 26th birthday, i wrote I Took A Pill in Ibiza…10 years ago. The song became popular several years after i wrote it. Yesterday i celebrated my 36th birthday. i feel proud to look at the song lyrics and know that NONE of them are true anymore. I’ve grown into a completely new man…one that i’m proud of. check this out… 🧵
1,184
20,999
163,652
20,600,829
31 Jul 2025
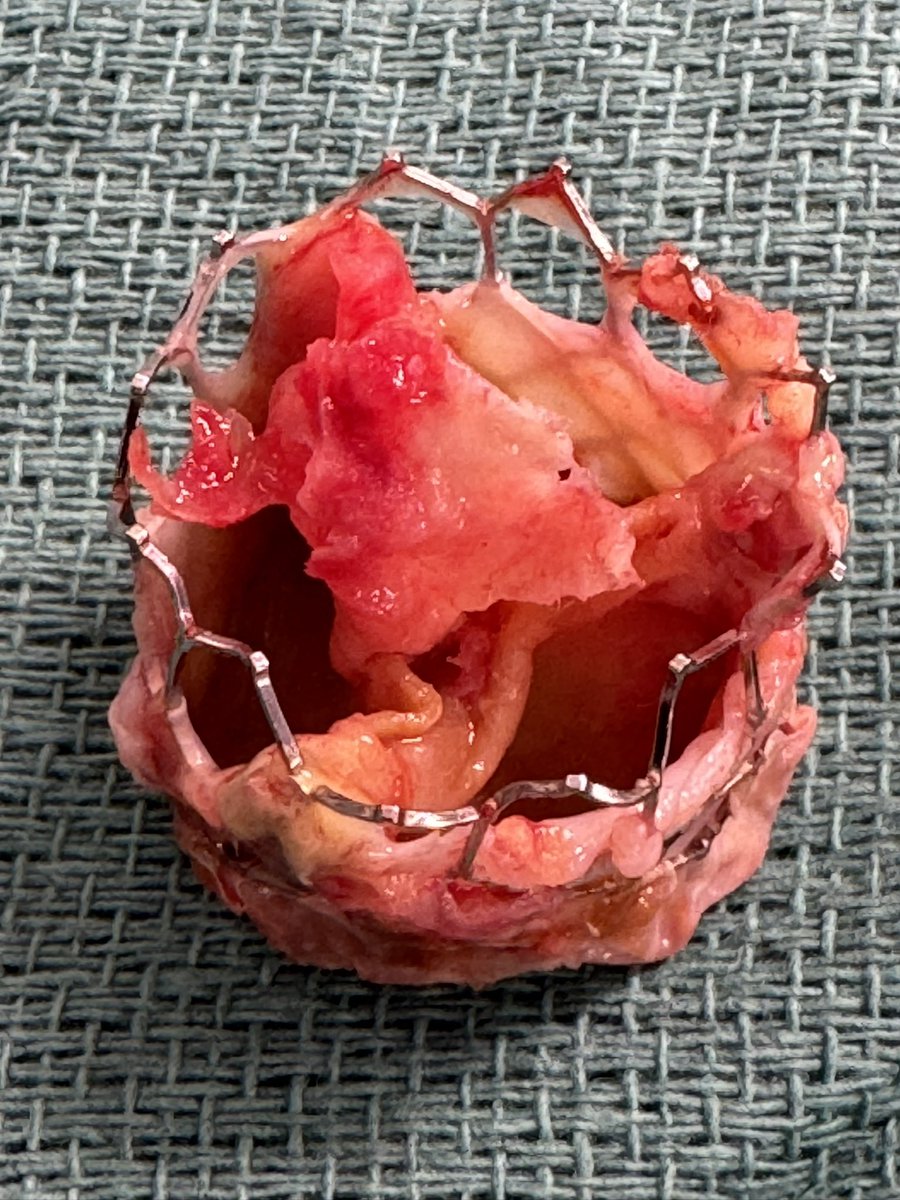
85 yo 👱🏼♂️, TAVR 3 years ago, now with endocarditis. Ugly, calcified root with obstructed prosthesis, required SAVR & partial aortic wall endarterectomy. Challenging to say the least. 25 mm tissue valve implanted via mini sternotomy. Clamp time 45 minutes.

6
2
47
2,389
31 Jul 2025
I use a surgical elevator to intelligently separate native smashed-up aortic leaflets from outer frame with counter-traction by grabbing the top of frame using a grasping tool. Start with the right, non, then left cusp. In 3-5 minutes, it "pops" out. It's not a "sardine can".
1
7
685
31 Jul 2025
Great day! Cardiac surgery is alive & thriving. 3 cases. 1st case, partial anomalous right pulmonary vein into SVC, patch baffled into LA via fossa septostomy. 2nd, AVR/replacement Ascending aorta. 3rd, TAVR explant for endocarditis requiring surgical AVR. All extubated...
5
68
5,464
26 Jul 2025
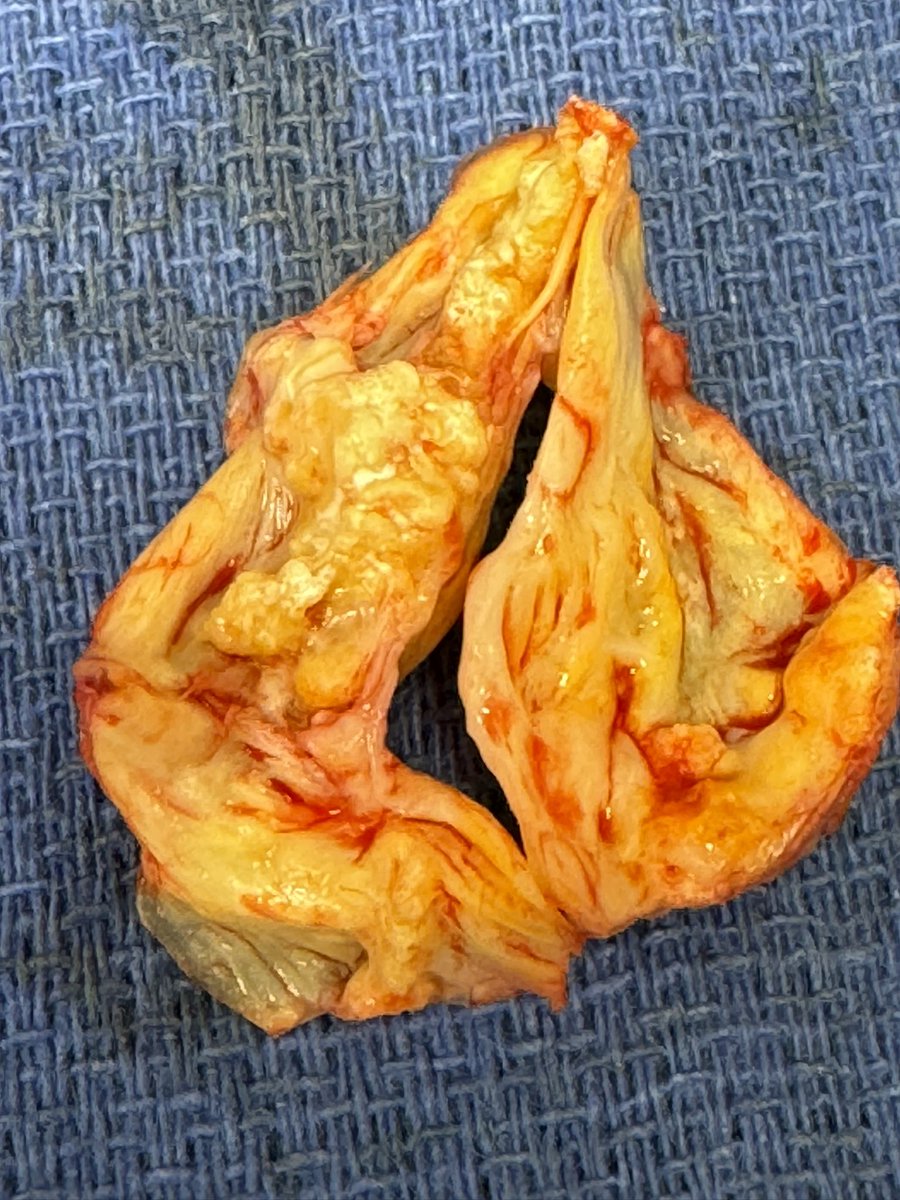
A classic rheumatic" fish-mouthed " aortic valve excised this AM. 50-year-old man with 2 prior mitral valve operations, the last one 20 years ago with a mechanical heart valve. Aortic valve replaced with a 23 St Jude Regent valve.
2
5
39
2,639
23 Jul 2025
This device that I wear every day has been a game changer for my practice. After a two or three case day, I leave the OR knowing that the NekSpine device is going to extend my career. Happy to chat with anybody about this.
4
1,143
22 Jul 2025
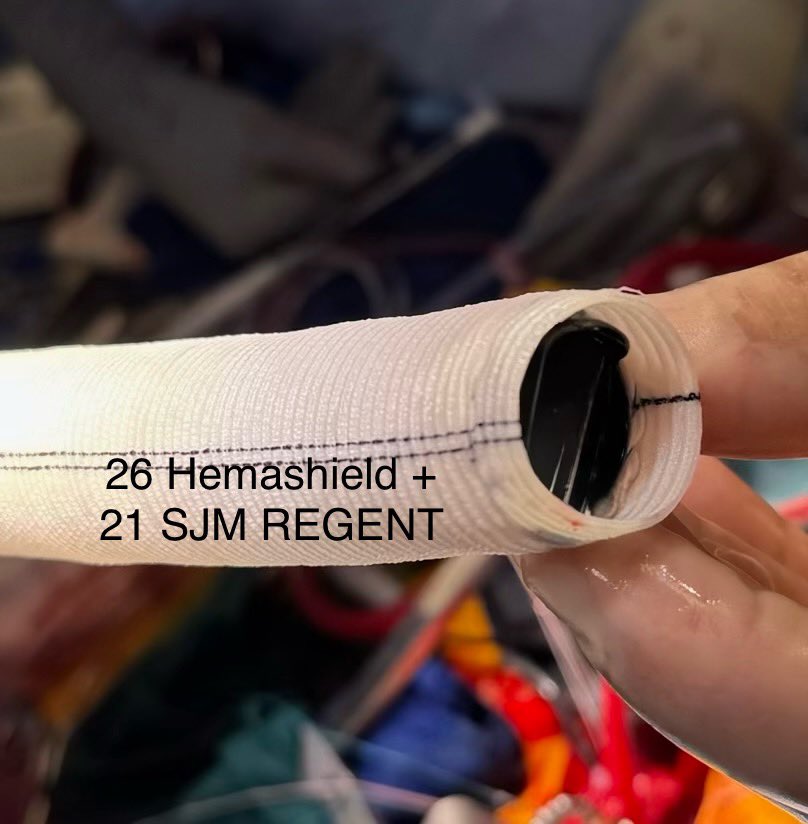
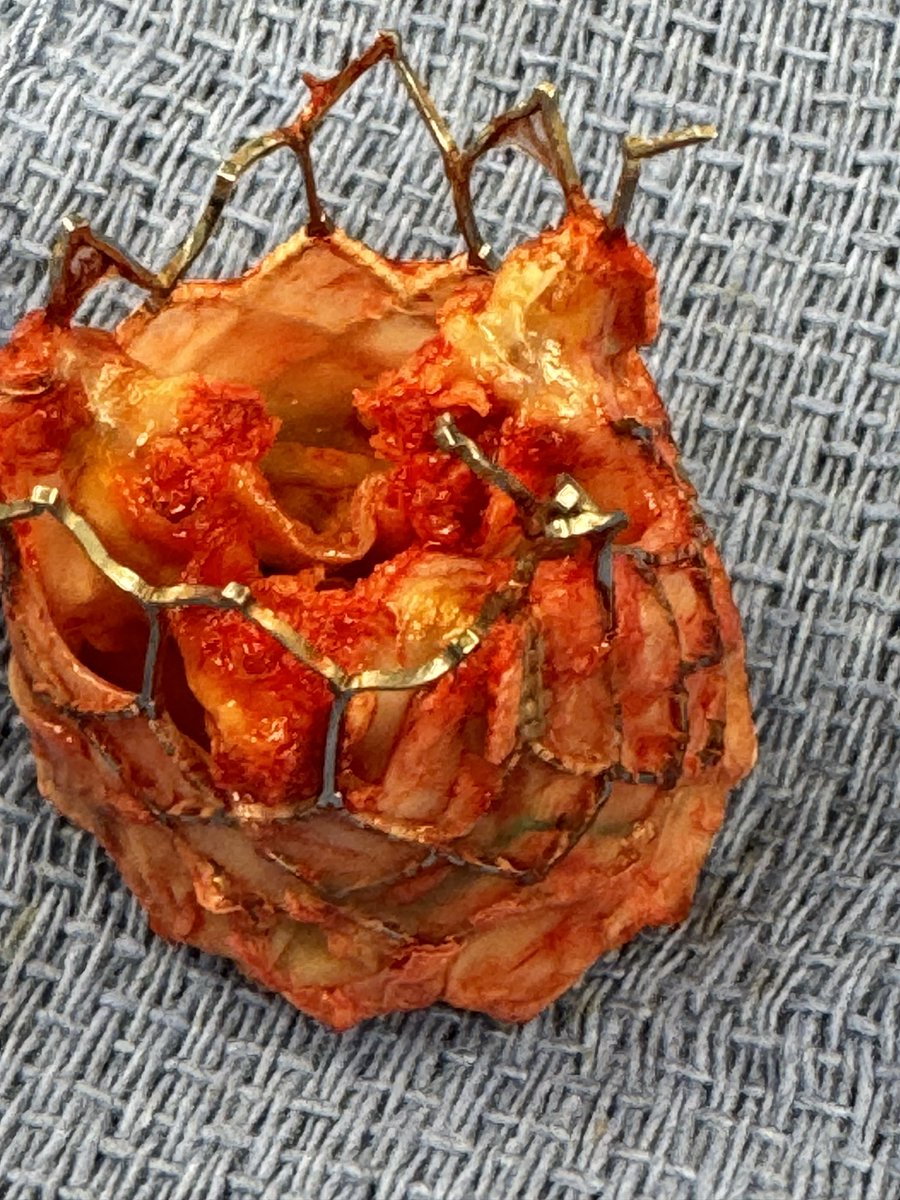
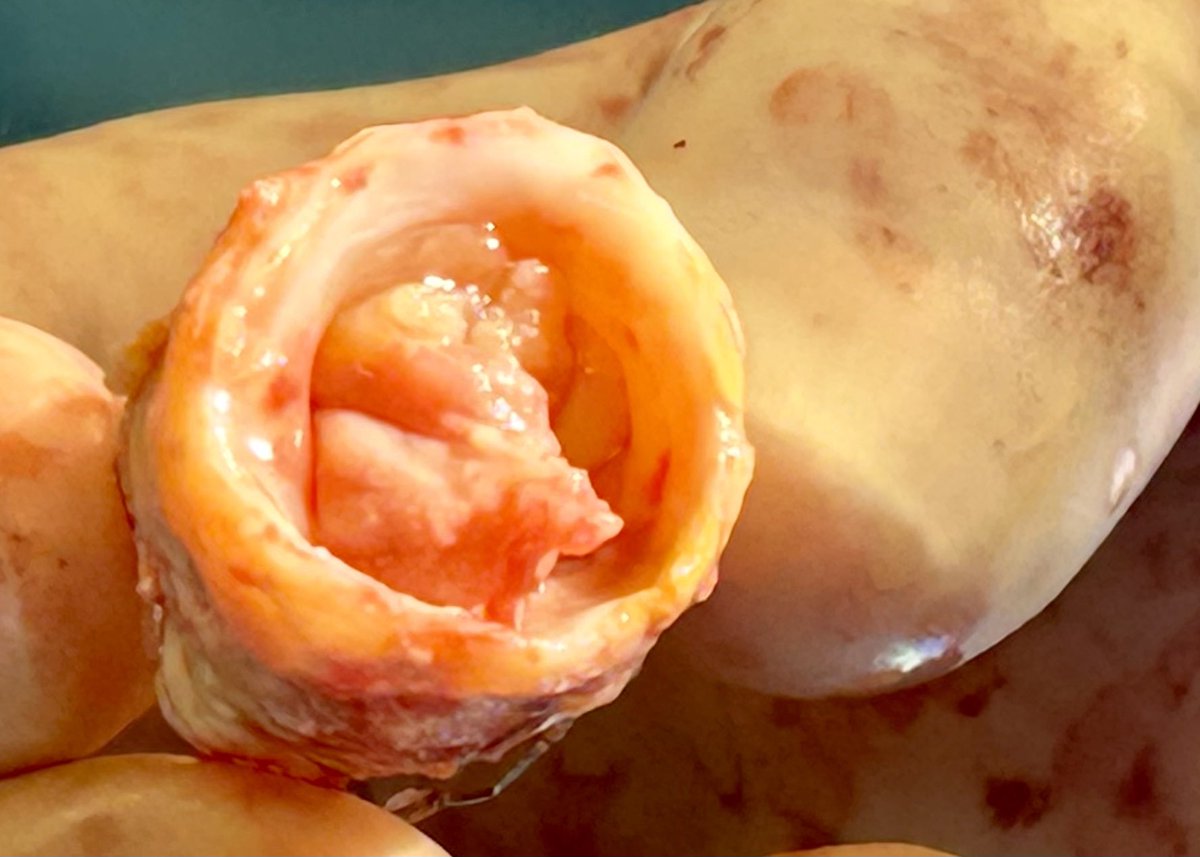
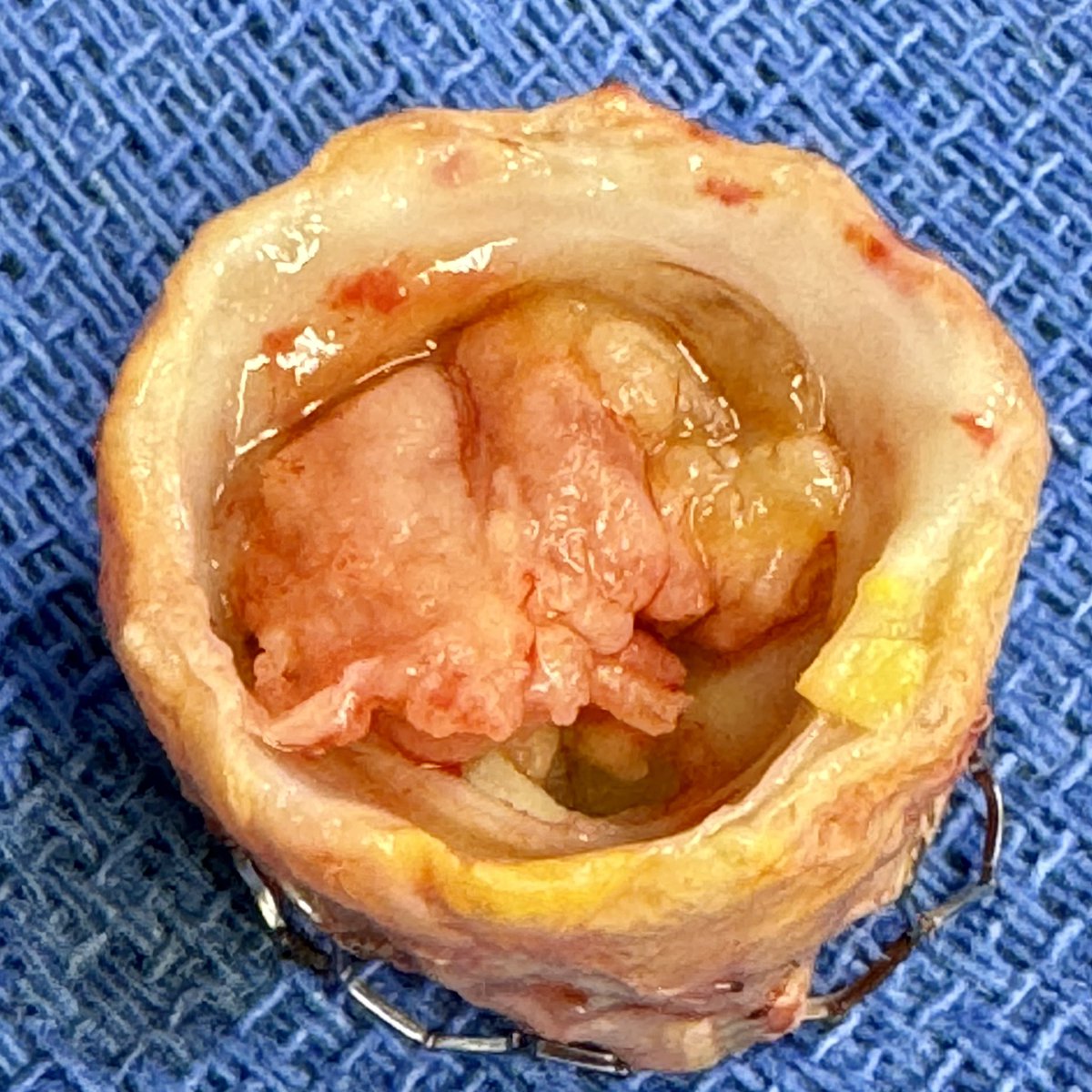
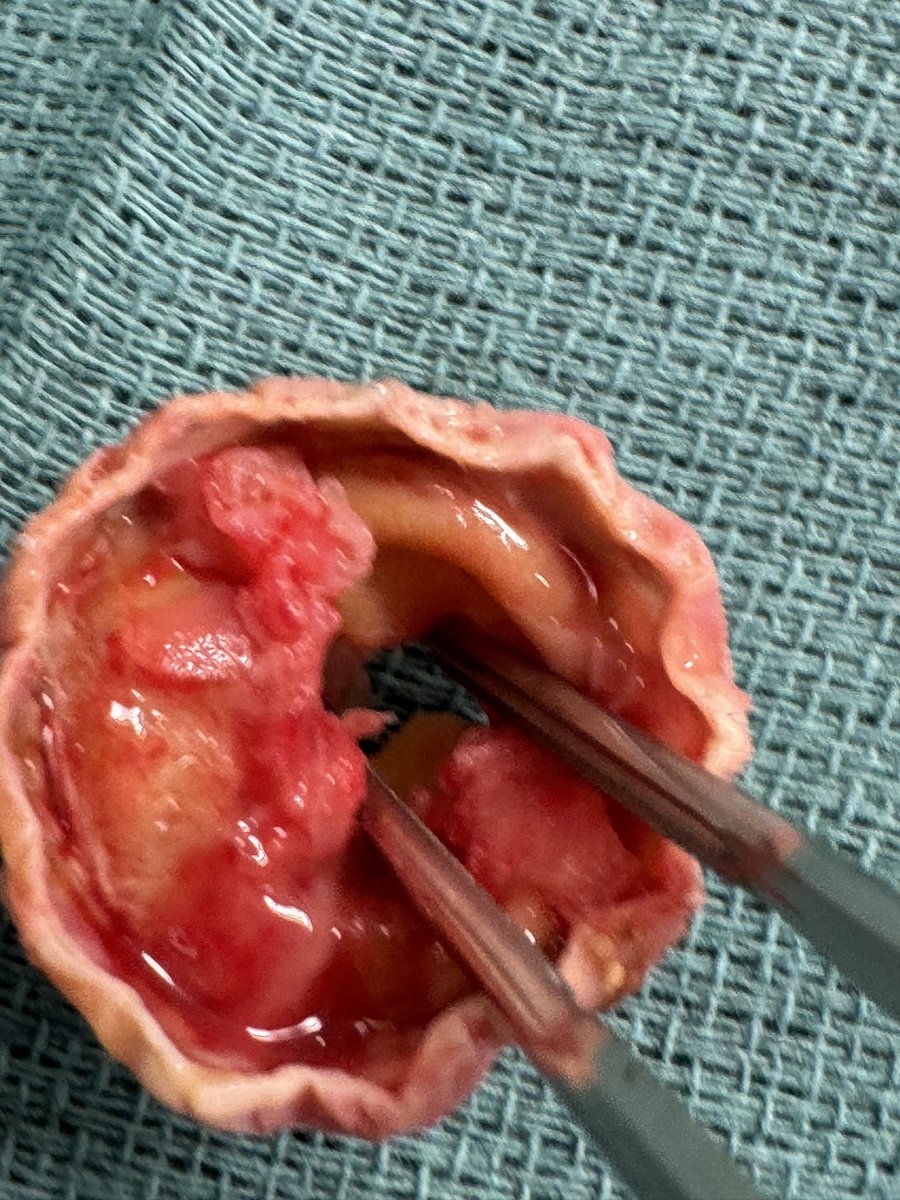
Tough case today. Young 👩🏻, 2 prior heart valve operations, last op w 25 OnX mitral & 19 OnX aortic root 7 yrs ago, now with severe double valve stenoses. Required 3rd time operation, w Commando Root and MVR to safely negotiate disaster. Pictures are worth 1000 words... haha!
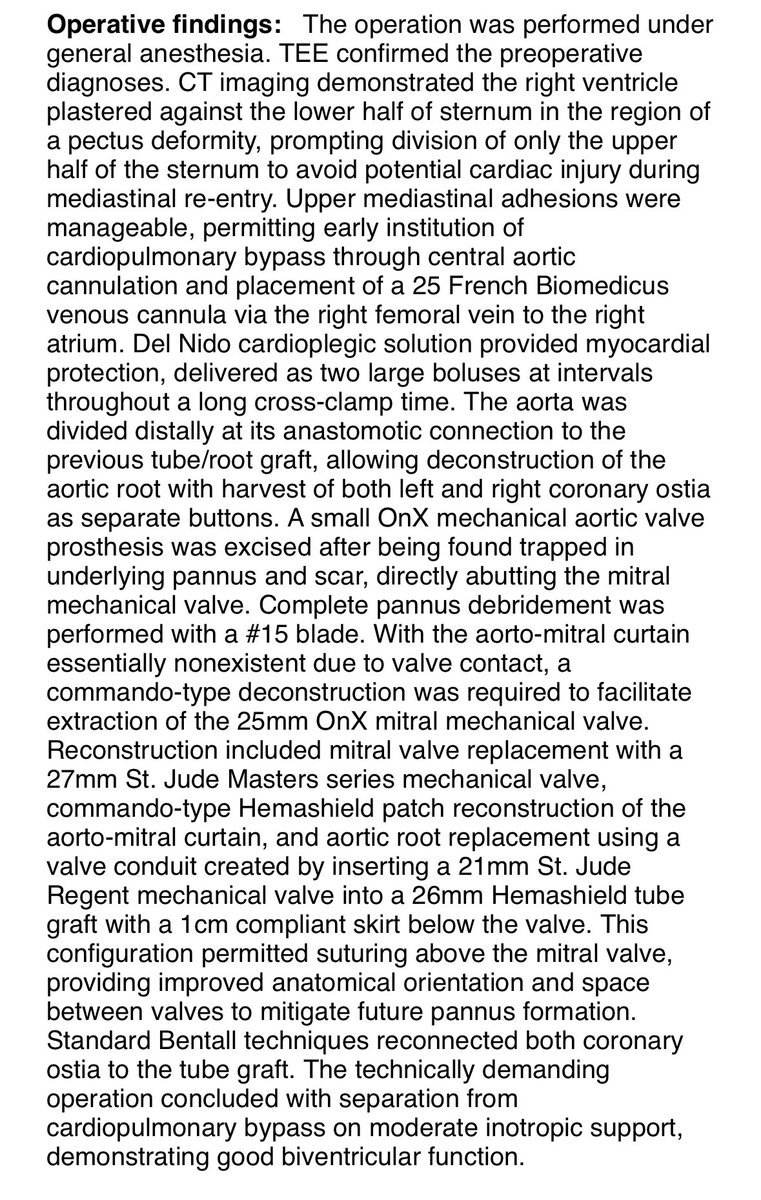
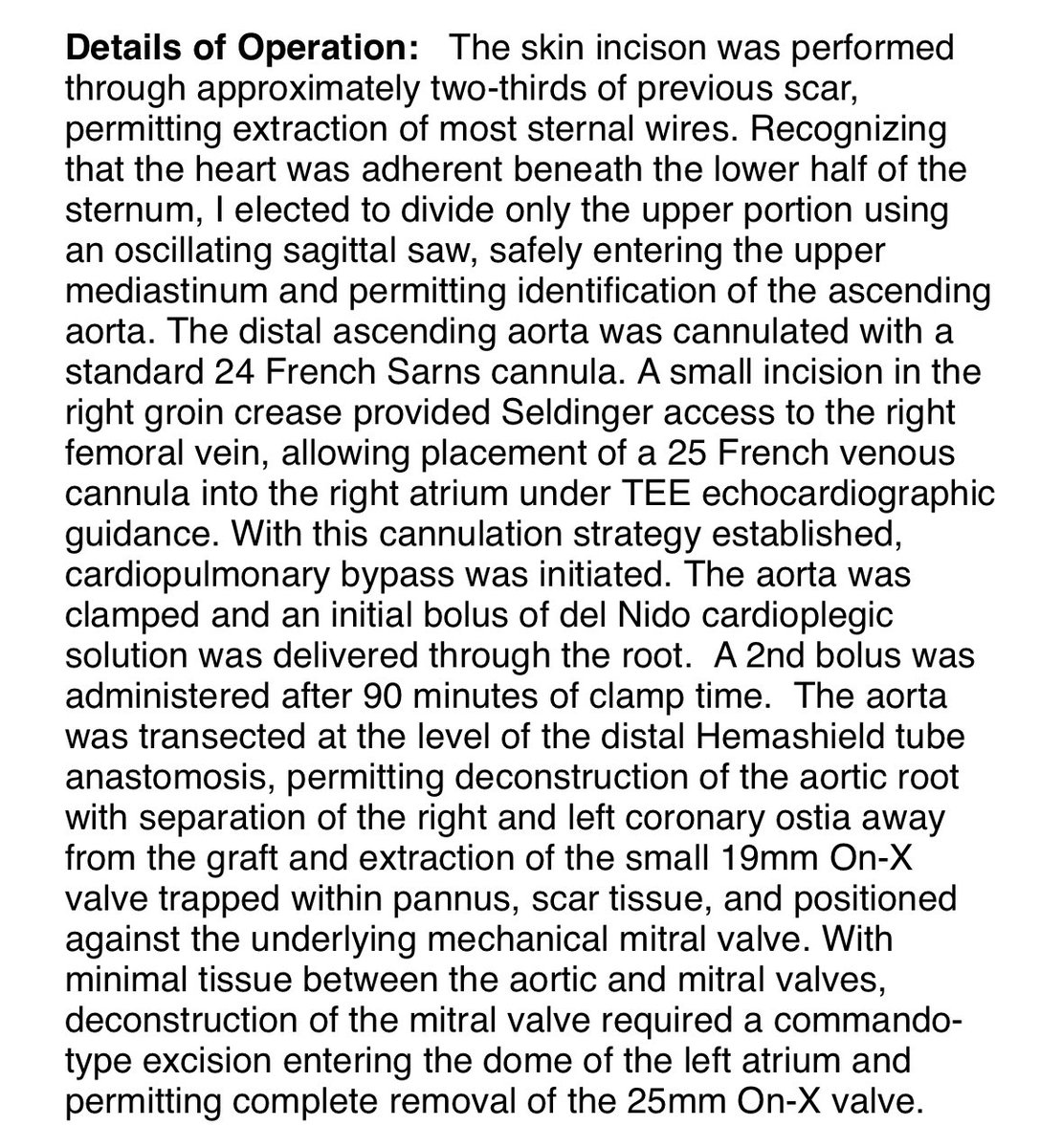
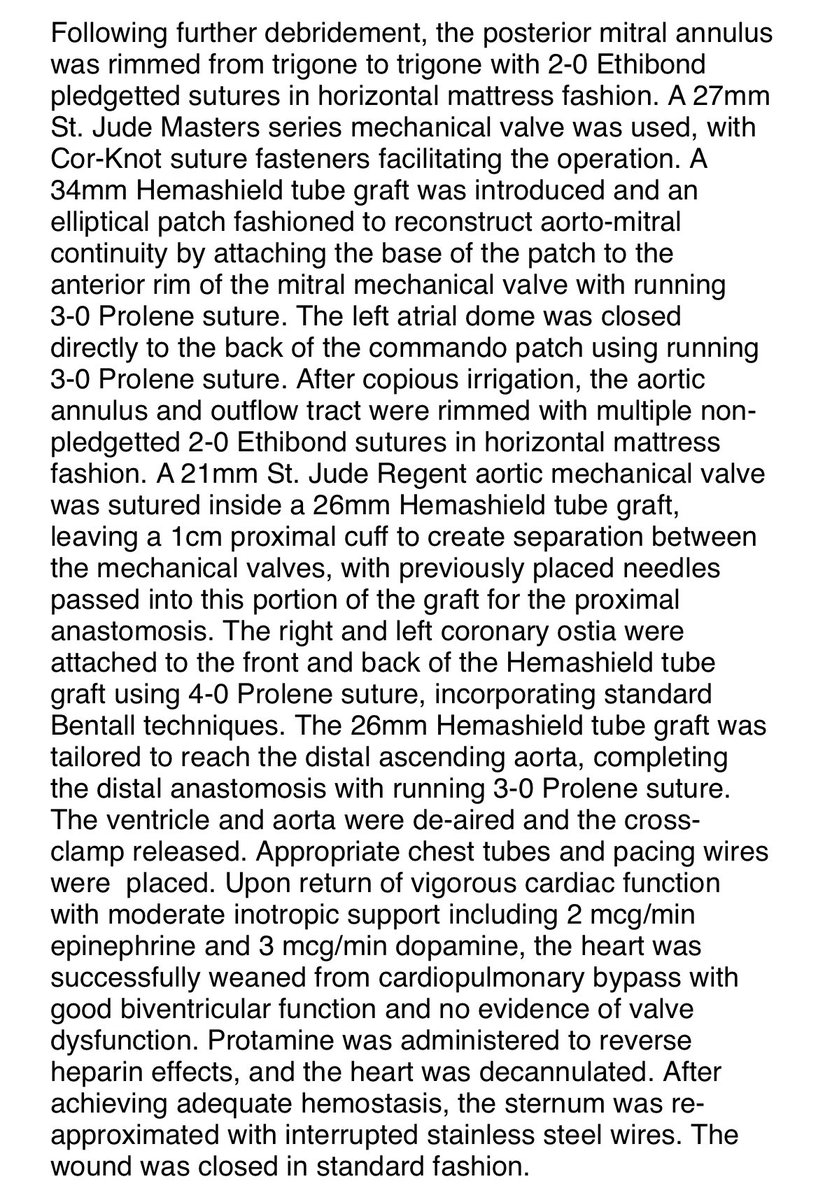
5
4
26
2,492
22 Jul 2025
Constructed St Jude Regent valve with Hemashield tube conduit to create a 1 cm proximal cuff, creating space above underlying St Jude mechanical heart valve... read previous post. 3rd time reoperation today ...@StephenSpindel @DrZeigler1 @tomcnguyen @AspiringCTS @stanfordctsurg
4
4
31
2,791
21 Jun 2025
Tough redo, previous AVR, Left and Right coronaries 2mm above prosthetic annulus. Endocarditis & Severe MR with massive posterior annular calcification. Near impossible exposure. Without understanding Commando "de-" and "re-"construction, cases like these are inoperable.
4
4
40
3,133
27 Jun 2025
Mastering root enlargement is essential, it's the foundation. Leverage the dome of the LA; it's a vital ally for exposure & orientation. Success in LVOT surgery hinges on a deep understanding of anatomic relationships. Commando isn’t just advanced, it’s root enlargement 2.0
1
6
513