
Cardiologist and echocardiographer at @RespiraINER #Echofirst #POCUS
Joined September 2009
- Tweets 6,319
- Following 1,814
- Followers 1,857
- Likes 11,207
677 Photos and videos







Benigno Valderrábano Salas retweeted

Jun 13
EMCrit 427 - Advancing Concepts in Shock Physiology. As an intro to a 3-part series, I go over two papers discussing new ways to assess and understand shock hemodynamics.
(@emnerd, @thinkingcc, @saracrager)
[#MembersOnly]
emcrit.org/427

1
21
82
10,213
Benigno Valderrábano Salas retweeted

Jun 11
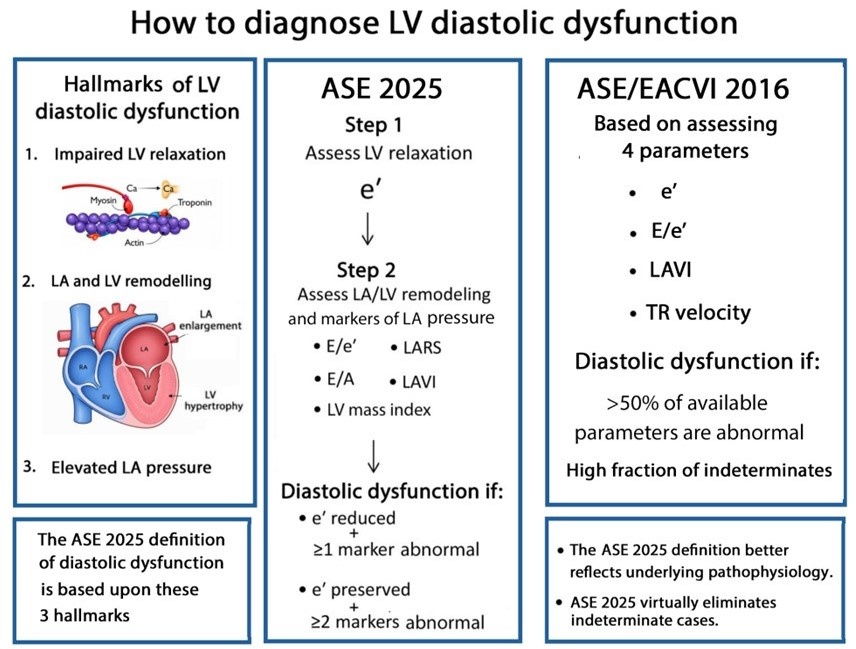
Most echocardiography laboratories have adopted the 2016 diastolic guidelines. With the release of the 2025 update, an important question arises:
What are the key conceptual differences between the 2016 and 2025 approaches to diagnosing diastolic dysfunction?
academic.oup.com/ehjcimaging…
@JGrapsa
12
82
252
16,871
Benigno Valderrábano Salas retweeted

Jun 12
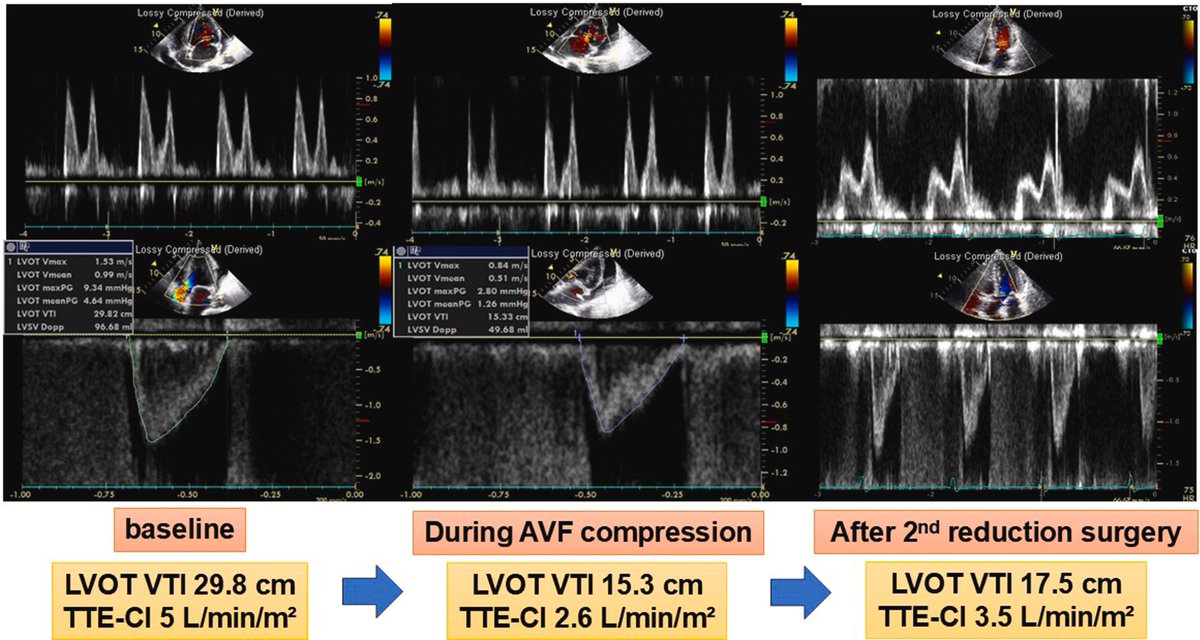
High-output heart failure associated with arteriovenous fistula remains an underrecognized, albeit well-described, clinical entity. This is a nice case with illustrative images - doi: 10.1016/j.jaccas.2026.107193. PMID: 41770183
#POCUS #Nephpearls
2
27
103
5,149
Benigno Valderrábano Salas retweeted

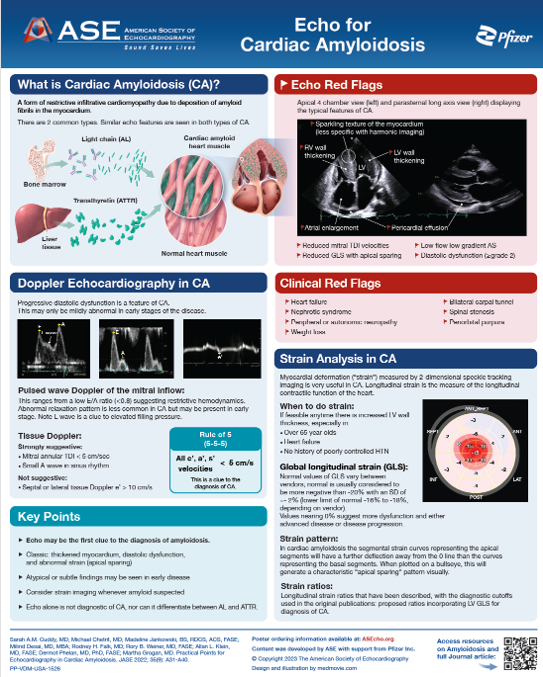
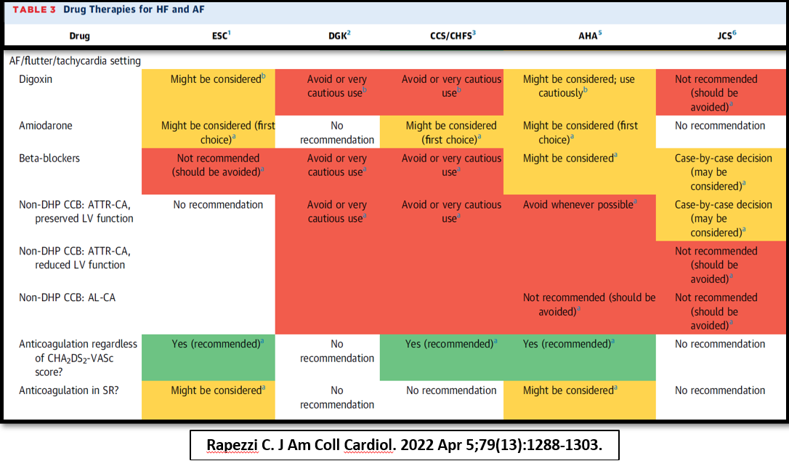
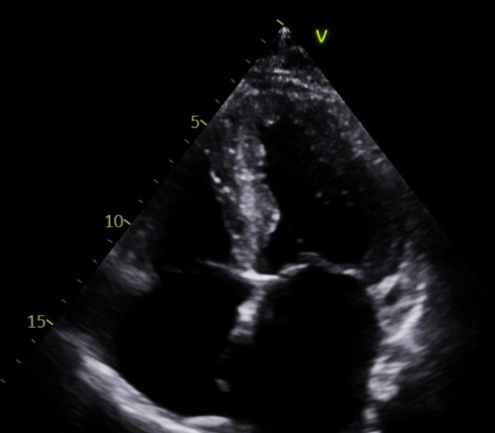
Cardiac amyloidosis 🫀
🚩flags: HFpEF refractory AFib multi-CVAs in older pt
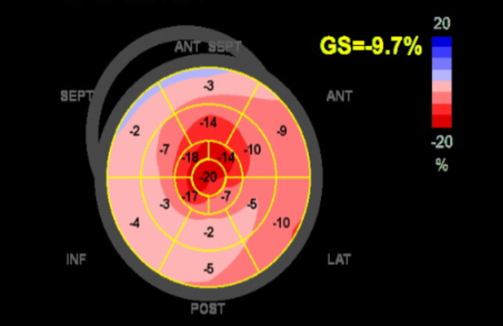
🔍 TTE: ↑ LV wall, ↓ GLS w/ apical sparing 🎯
💎 AFib in amyloid: ↑ thrombus risk → anticoagulant regardless of CHA₂DS₂-VASc; rhythm > rate when tolerated #CardioOnc #CardioTwitter @Abdelcards

🫀 57F w/ HTN, HL, HFpEF, recurrent AFib (refractory to DCCV) & multiple CVAs🧠
Now w/ severe dyspnea & orthopnea 🔍
What's the most likely underlying dx? 👉
Vote below — discussion in 24h
@Abdelcards @ICOSociety @mariellesc1 #CardioOnc #CardioTwitter #EchoFirst
1
29
66
5,894
Benigno Valderrábano Salas retweeted

What is the diagnosis?
39
35
227
68,649
Benigno Valderrábano Salas retweeted
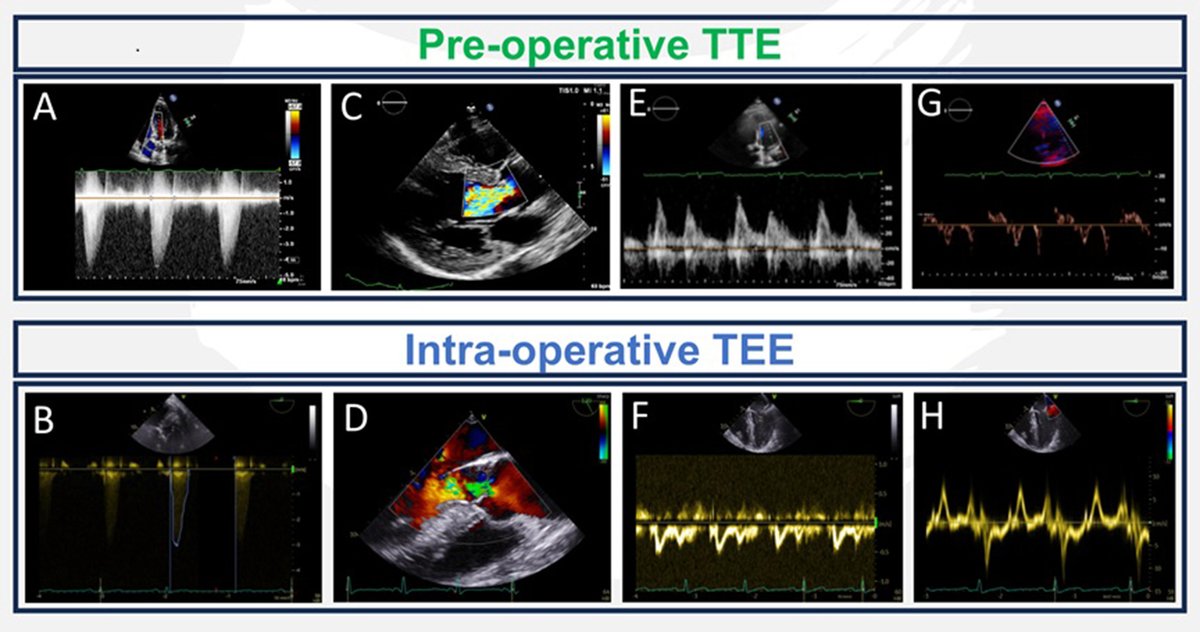
We've released a #new State-of-the-Art Review, "The Effect of General Anesthesia and Mechanical Ventilation on the Echocardiographic Evaluation of Cardiac Function!"
Read it now: bit.ly/4eokgaT
39
88
4,130
Benigno Valderrábano Salas retweeted

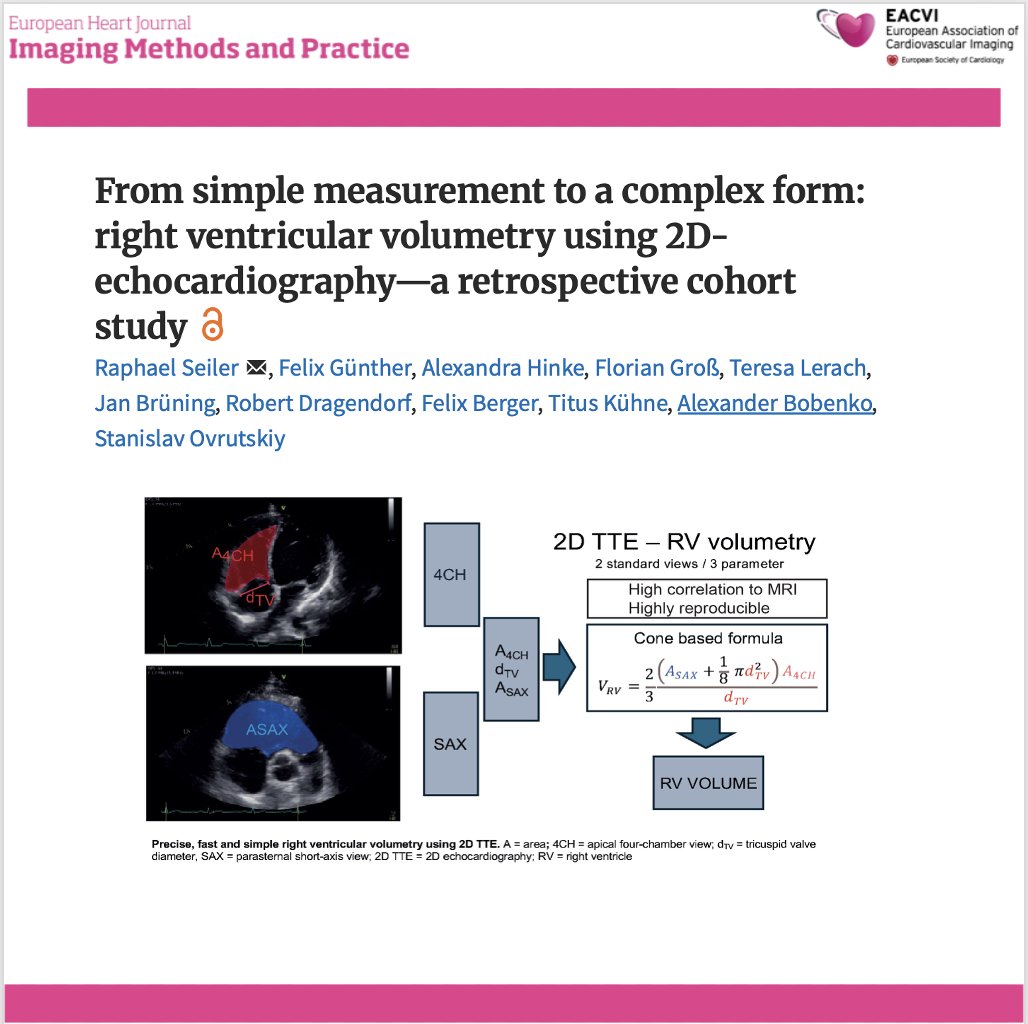
📄 Can we finally measure RV volume accurately with simple echocardiography?
🔗 DOI: doi.org/10.1093/ehjimp/qyaf1…
🫀 The right ventricle (RV) remains one of the most challenging chambers to assess—especially in congenital heart disease (CHD).
👉 Gold standard? Cardiac MRI
❗ But: expensive, time-consuming, and often requires sedation
✨ This study proposes a simple, fast, and accurate 2D echo-based method for RV volumetry—bringing us closer to true bedside quantification.
✨ The key idea:
👉 Model the RV using a cone-based geometric approach
➡️ Using only 2 standard echo views:
Apical 4-chamber (A4CH)
Parasternal short-axis (SAX)
📐 With just a few parameters:
✔ Cross-sectional areas (A4CH, ASAX)
✔ Tricuspid valve diameter
📊 Performance vs MRI:
🔥 Excellent agreement:
Systolic volume → ICC 0.98
Diastolic volume → ICC 0.96
📉 Minimal bias:
Δ systolic volume ≈ 0.1 mL
Δ diastolic volume ≈ 5.2 mL
➡️ Clearly outperforms traditional 2D models
💡 Why this matters clinically:
👉 Enables:
✔ Rapid bedside RV assessment
✔ Reduced need for repeated MRI
✔ Easier follow-up in paediatric & CHD patients
👉 Particularly valuable in:
Post-operative monitoring
Serial evaluations
Resource-limited settings
🚀 Key innovation:
👉 A mathematically robust yet practical model
➡️ Balancing accuracy simplicity
➡️ Adaptable to different RV shapes
🚨 Bottom line:
2D echocardiography—when combined with smart modelling—can approach MRI-level accuracy for RV volumetry.
#Cardiology #Echocardiography #RightVentricle #CongenitalHeartDisease #CardiacImaging #CMR #Innovation #MedTech #PediatricCardiology 🫀📊
39
91
4,750
Benigno Valderrábano Salas retweeted

So proud of incoming Mayo Clinic cardiology fellow, @ayeshasinghmd, on her publication documenting a 40% rate of residual angina in ISCHEMIA patients following complete revascularization as adjudicated by angiographic core lab. ahajournals.org/doi/full/10.…
7
22
84
10,960
Benigno Valderrábano Salas retweeted

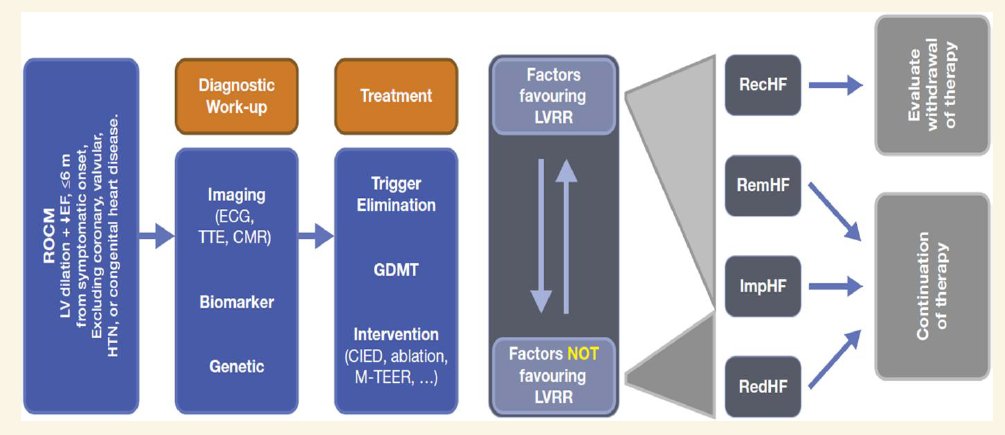
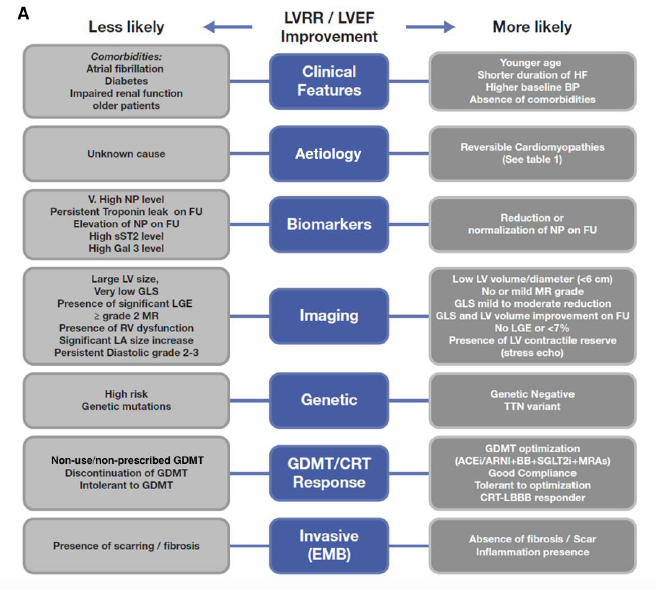
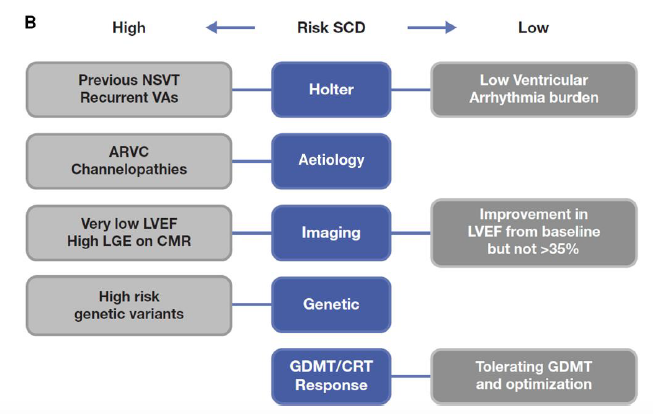
🚨Recent-onset cardiomyopathy?
New HFA-ESC practical guideline of how to evaluate and manage it ❗️
Two prognostic axes: the potential for LV reverse remodeling & risk o SCD
@MarcoMetra @WilfriedMullens @AmrAbdin10 @GMCRosano @GianluSava @ppponikowski
doi.org/10.1093/eschf/xvag11…
3
2
197
Benigno Valderrábano Salas retweeted

Ischemic cardiomyopathy remains a leading cause of HF and CV death. This review highlights the evolving role of imaging, viability, and revascularization, while reinforcing GDMT and device therapy as the foundation (link.springer.com/article/10…). #HREV @GianluSava @NicolasGirerd
2
31
65
7,131
Benigno Valderrábano Salas retweeted

Uno de los mejores artículos del año! Que piensan? Cuál es el valor se FFR que se asocia con síntomas? 💪
ahajournals.org/doi/epdf/10.…

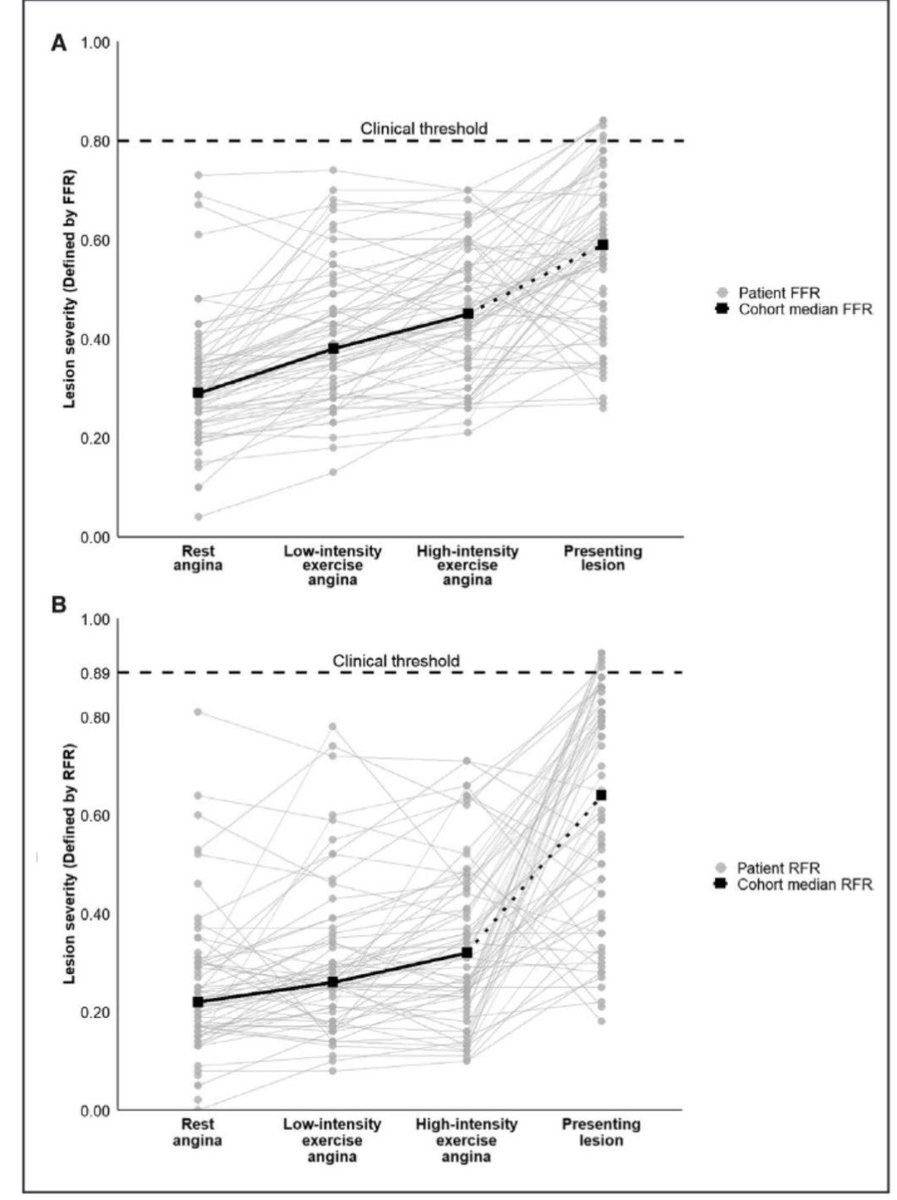
8
33
2,816
Benigno Valderrábano Salas retweeted

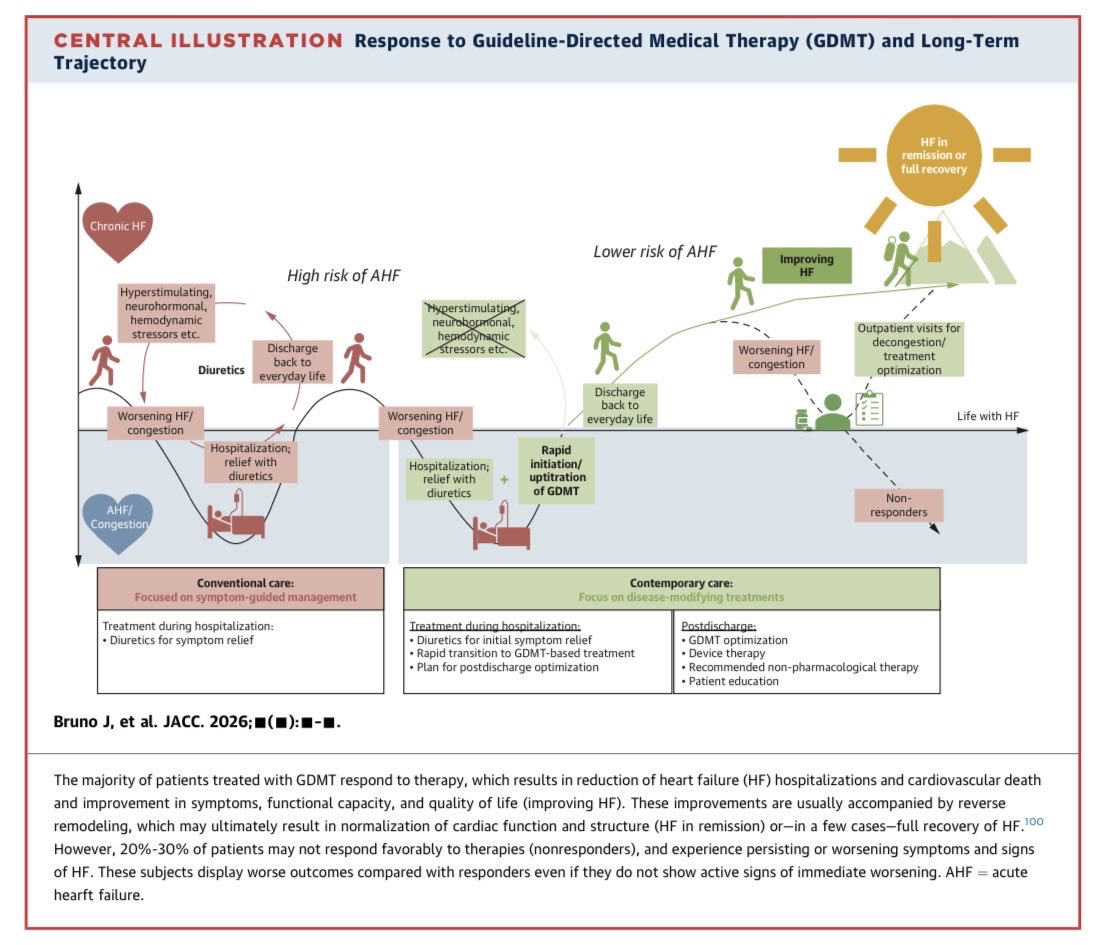
🚨 Managment of AHF is advancing!
Glad to share our review, aimed at:
🔄 Bring together management algorithms across different healthcare settings and resources
🏥 Translate contemporary evidence into practical bedside management
#HeartFailure #AcuteHeartFailure #JACC
3
51
127
10,019
Benigno Valderrábano Salas retweeted

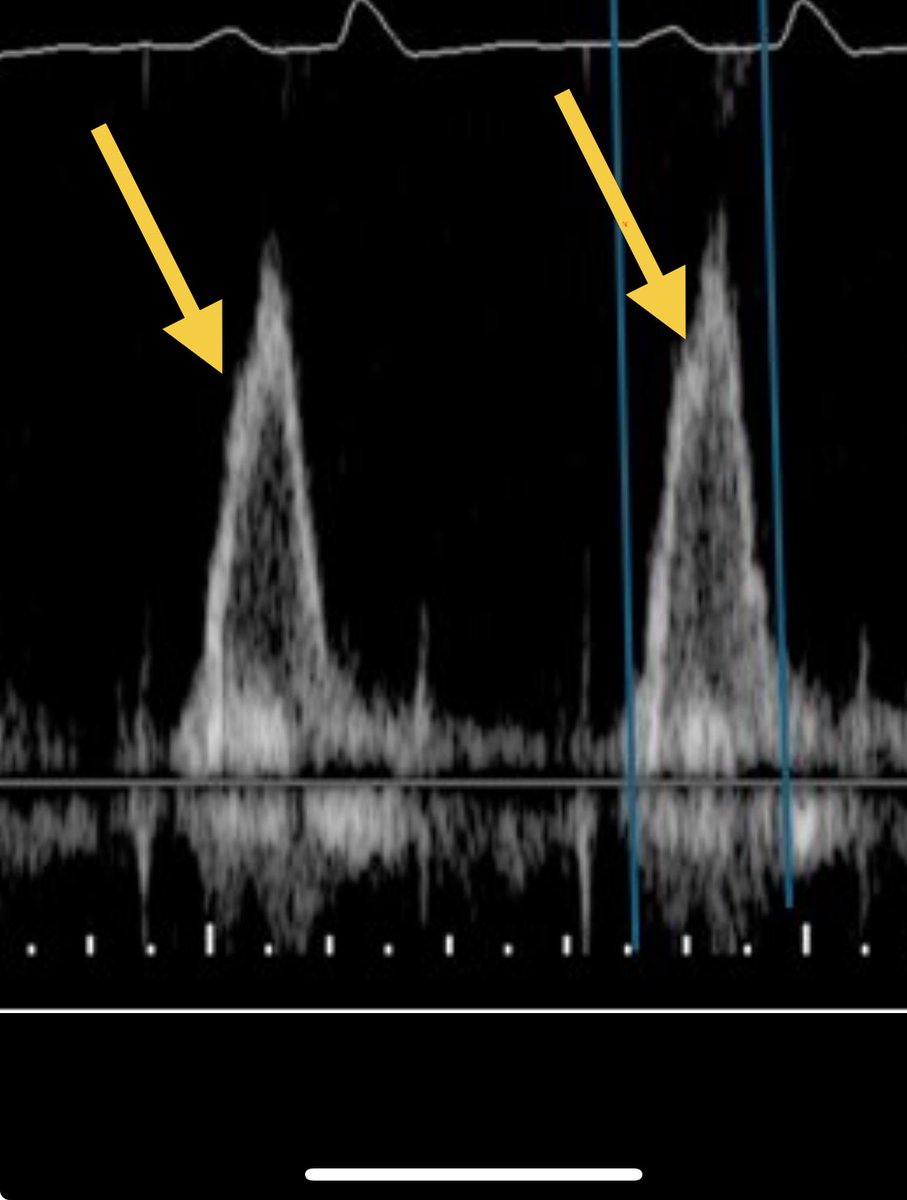
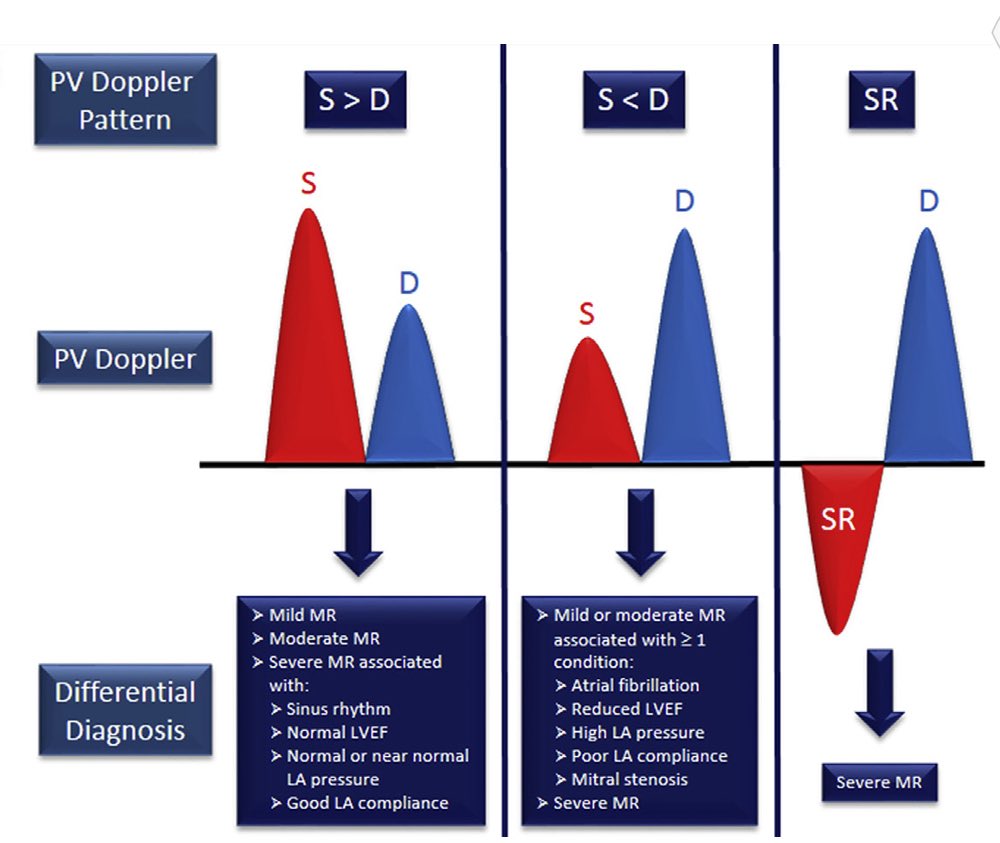
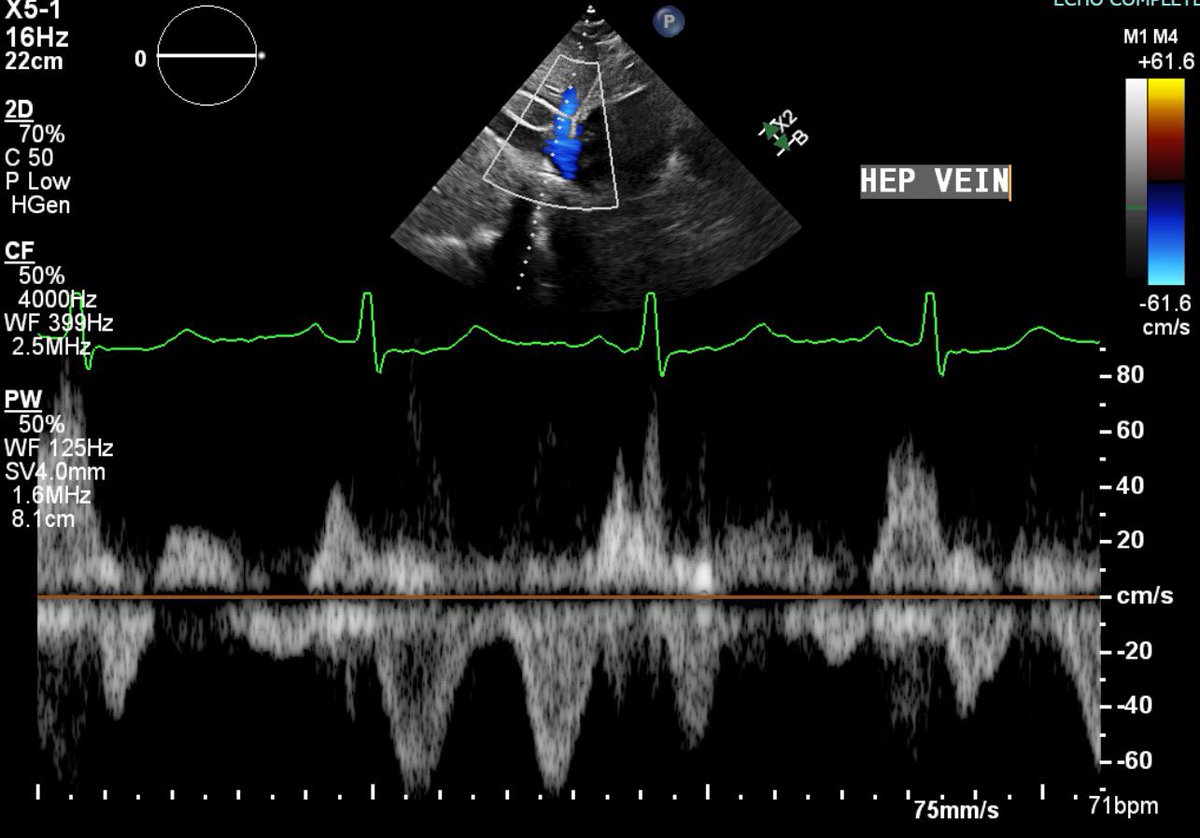
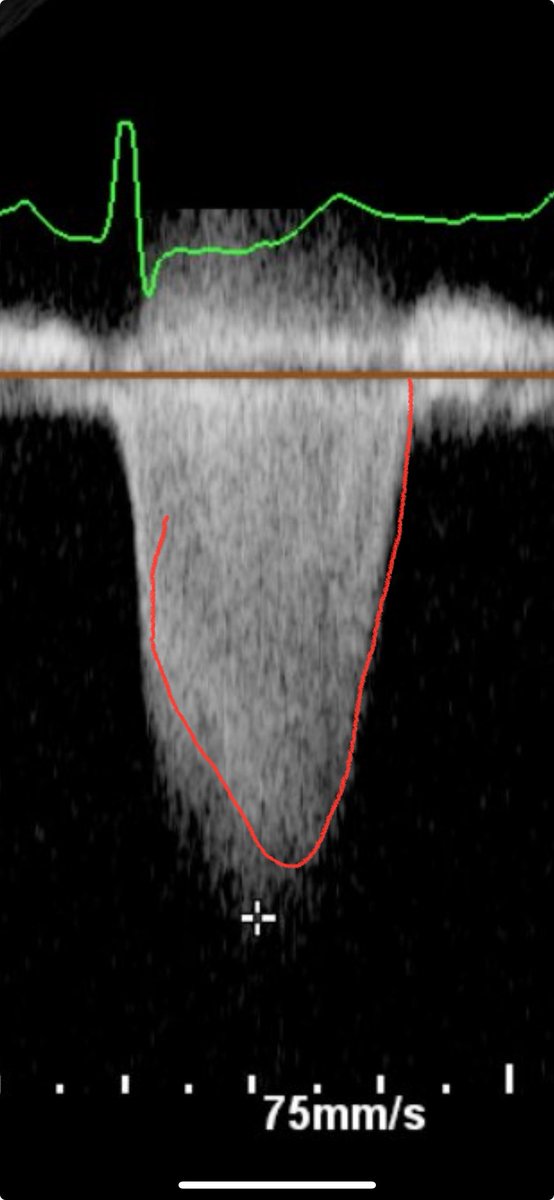
Fellows, what does this layer of jets in the 4C view tell you? @ASE360 @escardio #echofirst @ACCinTouch #ACCEarlyCareer

6
30
152
21,253
Benigno Valderrábano Salas retweeted

May 22
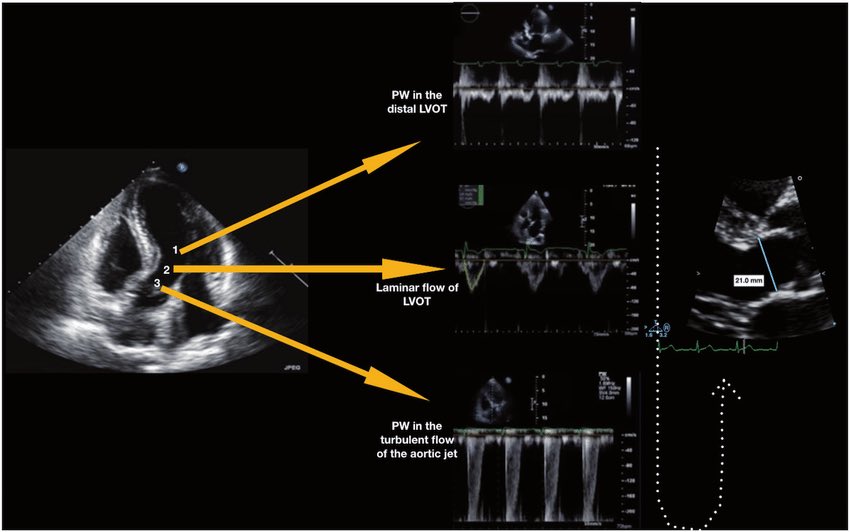
Continuous-wave Doppler interrogation in valvular heart disease: pearls and pitfalls | European Heart Journal - Imaging Methods and Practice | Oxford Academic academic.oup.com/ehjimp/adva…
3
26
67
16,714
Benigno Valderrábano Salas retweeted

May 22
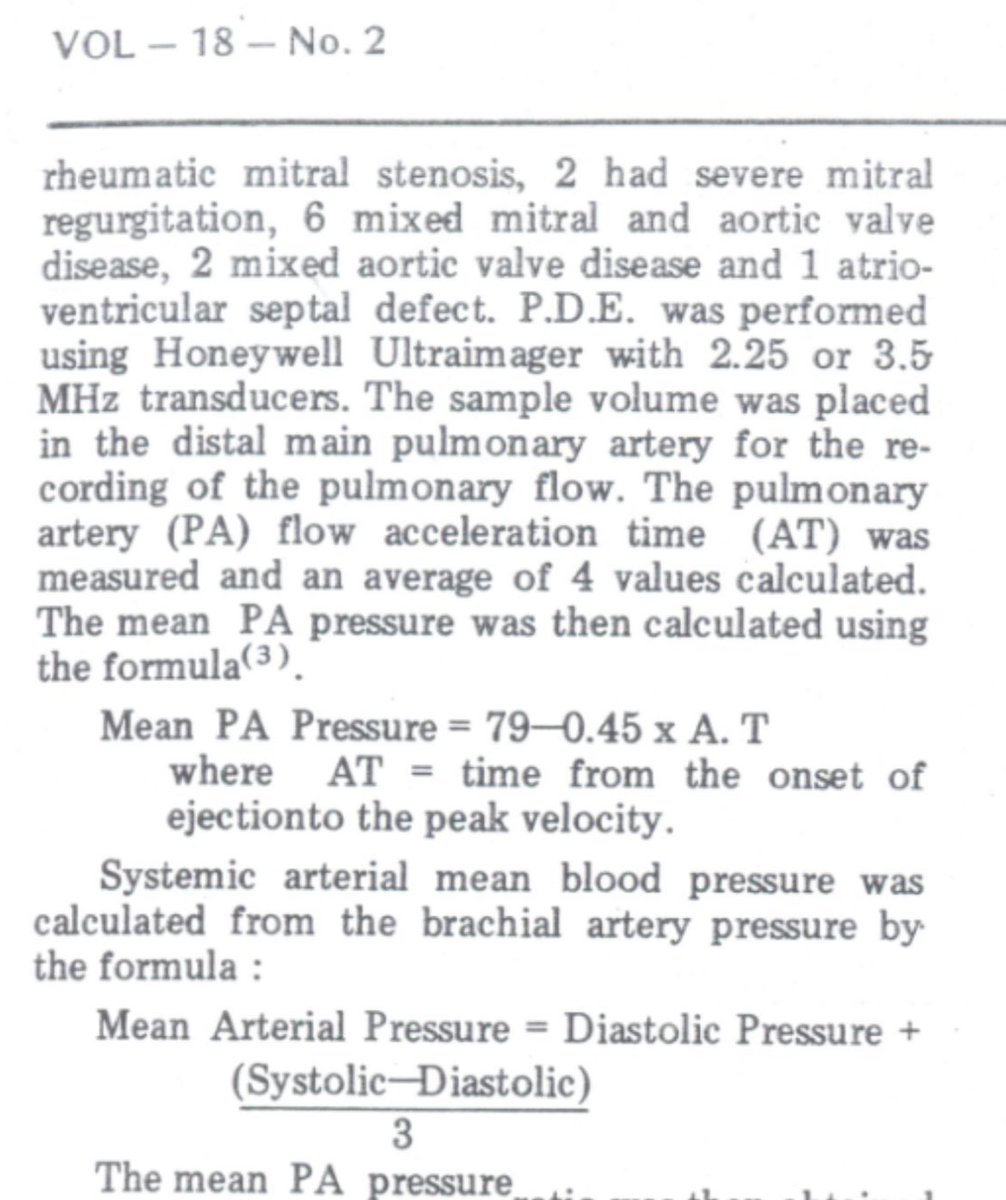
What is best formula to estimate mPAP on #echofirst?
📝 finds minimal end-diastolic PR pressure best correlation (R = 0.92) & diagnostic accuracy AUC 0.96 bit.ly/4nQrzvm in almost 600 pts referred for RHC for PH dx, integrates both PR & TR signals
At 24.5 mm Hg cutoff, mPAPDPmin 89% sensitivity, 94% specificity
At 20 mm Hg, mPAPDPmin sensitivity⬆️99% w/ net reclassification driven by more accurate downgrading of pts w/o PH



1
54
162
8,331
Benigno Valderrábano Salas retweeted
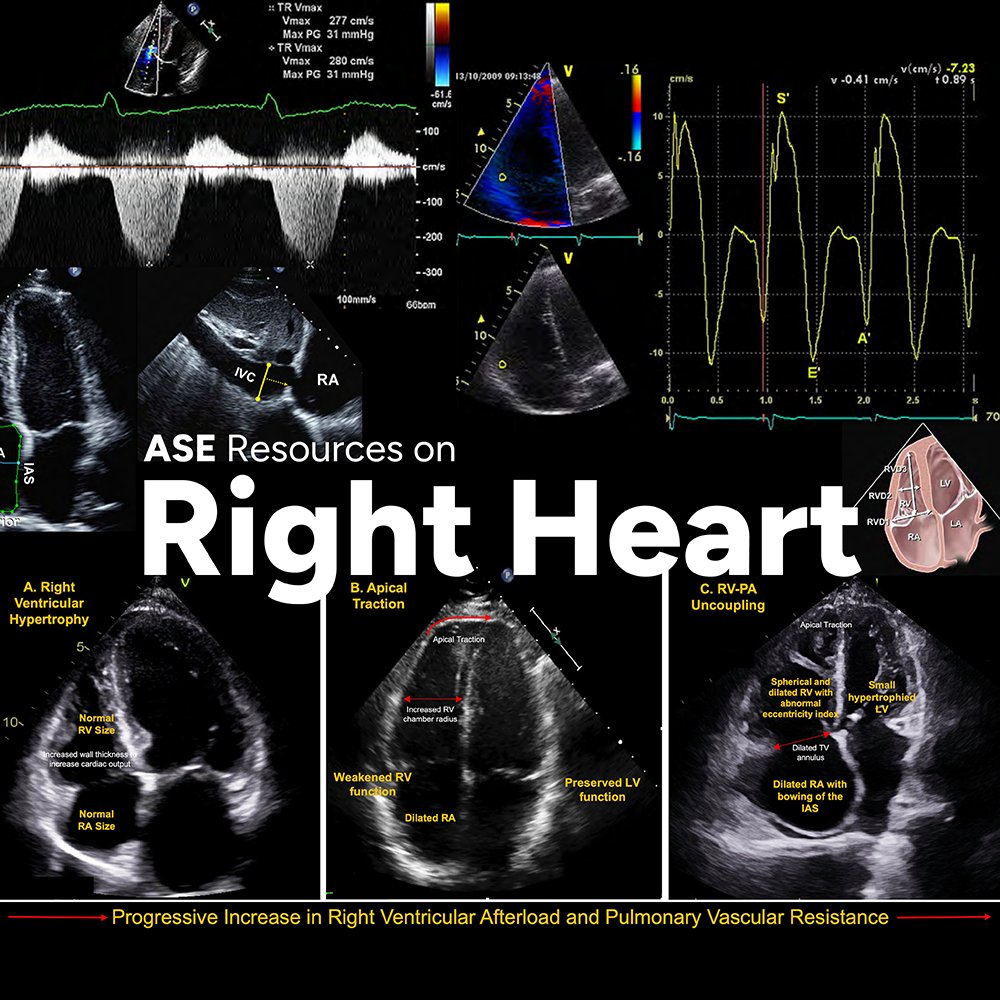
ASE and the @accpchest recently partnered on a project to develop two educational webinars to improve the understanding of cardiovascular ultrasound's application in pulmonary hypertension.
You can find them on our #new Right Heart Resources web page! bit.ly/4nQ5E7p
29
63
3,935
Benigno Valderrábano Salas retweeted
May 20
Very interesting image of IVC!
Any guesses on what the red flow is? (clue: congenital anomaly) - See thread for source/full case.
#POCUS #echofirst #FOAMed
10
24
121
19,417

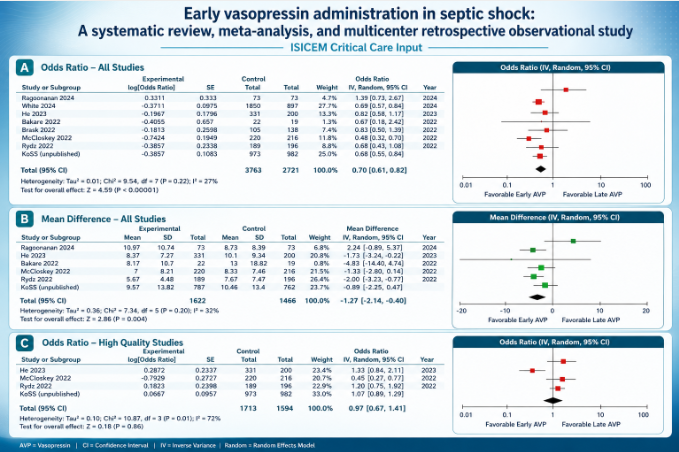
@ISICEM Critical Care Input
Early vasopressin administration in septic shock: A systematic review, meta-analysis, and multicenter retrospective observational study
sciencedirect.com/science/ar…
#ISICEMelearning #Meded @Sciencedirect
4
7
922
Benigno Valderrábano Salas retweeted

#JADEL
I hope you enjoy reading my CASE editorial: Blow Hard!
cvcasejournal.com/article/S2…
I discuss Antonio Maria Valsalva, the complex physiology of the Valsalva maneuver, & include a link to learn about goal-directed methods: youtu.be/MAbId_9dUgU?list=PL…
@CASEfromASE @ASE360


6
10
1,379
Benigno Valderrábano Salas retweeted

🫀In cardiogenic shock, we still focus heavily on MACROcirculation:
📉 blood pressure
📉 cardiac output
📉 LVEF
📉 vasopressor dose
But what if the real battle is happening deeper?
🩸 At the microcirculatory level.
This excellent ATS viewpoint highlights one of the most important evolving concepts in shock physiology:
⚠️ normalization of macrocirculation does not necessarily mean restoration of tissue perfusion.
Despite advances in cardiogenic shock management, mortality remains >40%.
Even more striking, up to 45% of deaths occur in patients with normalized cardiac index.
That disconnect may be explained by persistent:
🩸 microvascular dysfunction
🩸 impaired capillary perfusion
🩸 endothelial dysfunction
🩸 tissue hypoxia despite “acceptable” hemodynamics
The review reinforces that: Microcirculation is not a passive bystander.
It may be a central driver of:
• organ dysfunction
• lactate persistence
• shock progression
• mortality
Particularly interesting is the emphasis on simple bedside tools.
We often think microcirculation requires advanced devices, yet:
📌 capillary refill time (CRT)
📌 mottling
📌 ΔPCO₂
📌 lactate trends
still carry strong prognostic value.
A CRT >3 seconds at ICU admission was associated with worse outcomes, and combining CRT with the CardShock score achieved an impressive AUC of 0.93 for outcome prediction.
The article also reviews modern technologies:
🔬 handheld vital microscopy
🔬 sublingual microcirculation imaging
🔬 NIRS
🔬 laser Doppler assessment
bringing “real time” bedside microcirculatory monitoring closer to clinical practice.
One of the strongest physiological messages:
⚠️ Shock is not only about flow. It is about effective tissue level oxygen delivery.
The review beautifully summarizes the four major mechanisms of microvascular dysfunction:
• heterogeneity
• hemodilution
• congestion
• edema
Particularly relevant for intensivists:
📌 venous congestion itself may worsen microvascular flow
📌 elevated filling pressures impair driving pressure
📌 edema increases oxygen diffusion distance
This is highly relevant in:
• advanced heart failure
• VA ECMO
• mixed shock states
• fluid overloaded patients
Another important takeaway: Persistent microcirculatory dysfunction after VA ECMO initiation was associated with increased mortality, even when macrocirculation improved.
Perhaps the key message of this paper is:
🩸 Microcirculation should no longer be considered a secondary endpoint in cardiogenic shock.
It may become one of the most important physiological targets of the next decade.
📖 Merdji H, American Journal of Respiratory and Critical Care Medicine. 2026, 212(3), 410–413 doi.org/10.1093/ajrccm/aamaf….

ALT
1
60
185
8,492