Mucormycosis is a rapidly progressive, invasive fungal infection that causes severe disease. The latest epidemiologic data, risk factors, diagnostic strategies, and treatment approaches are discussed in a new review. 👉
nej.md/3ZsLZ21
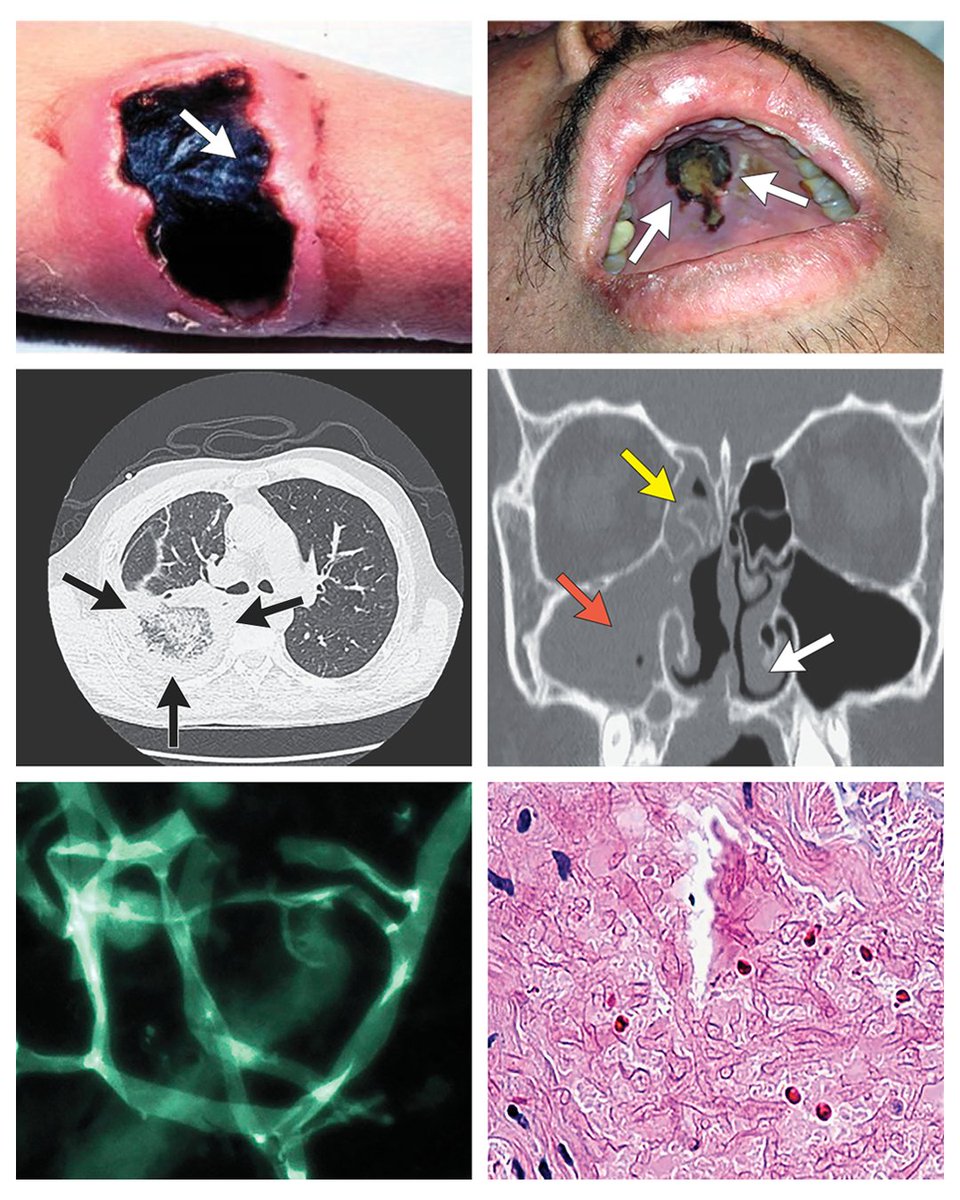
Early diagnosis and initiation of antifungal therapy significantly reduce mortality among patients with mucormycosis and hematologic cancers, from approximately 80% to 40%. Accurate diagnosis of mucormycosis begins at the bedside with evaluation of symptoms and signs in patients at high risk (seen in figure). Although early symptoms and physical findings in patients with mucormycosis are often nonspecific, they carry important diagnostic significance in patient populations with high risk. Periorbital cellulitis, diplopia, focal palatal necrosis, and necrotic wounds in patients at high risk should cause serious concern for mucormycosis and lead to prompt assessment. Maintaining a high index of suspicion for mucormycosis in such patients can be the impetus for obtaining fluids and tissues for diagnostic analysis, ordering imaging procedures, initiating antifungal therapy, requesting surgical assessment, reversing immunodeficiencies, and correcting metabolic abnormalities.
Learn more in the Review Article “Mucormycosis” by Dimitrios P. Kontoyiannis, MD, ScD, and Thomas J. Walsh, MD, from the University of Texas M.D. Anderson Cancer Center (
@MDAndersonNews), Center for Innovative Therapeutics and Diagnostics, and University of Maryland School of Medicine (
@UMmedschool):
nej.md/3ZsLZ21

ALT Top left: Cutaneous mucormycosis characterized by blackened, raised eschars.
Top right: Lesions due to palatal mucormycosis.
Middle left: In pulmonary mucormycosis, a large reversed halo sign in the right lower lobe characterized by a pulmonary infiltrate with a central ground-glass opacity that is circumscribed by denser air-space opacities.
Middle right: Examples of imaging results in mucormycosis of the right maxillary sinus, right ethmoid sinus, and left nasal turbinates.
Bottom left: Direct examination of sinus aspirate under fluorescence microscopy with calcofluor staining showing broad, ribbonlike hyphae with nondichotomous right-angled branching typical of rhizopus.
Bottom right: Histopathological analysis of infected tissue with periodic acid–Schiff staining showing broad, ribbonlike hyphae with nondichotomous right-angled branching.