
Diagnostic and Interventional Nephrology, Interest in AKI and extracorporeal support therapies… 🍷,☕️,📚, ✈️ & 🎥. …….🏥🟰🫁🔄🫘
Joined December 2012
- Tweets 801
- Following 452
- Followers 1,398
- Likes 6,020
138 Photos and videos





Mark GN retweeted

Jun 12
Evaluation of Patients With ESRD and Suspected High-Output Heart Failure.
🔗jacc.org/doi/10.1016/j.jacca…

1
10
39
2,344
Mark GN retweeted
Jun 12
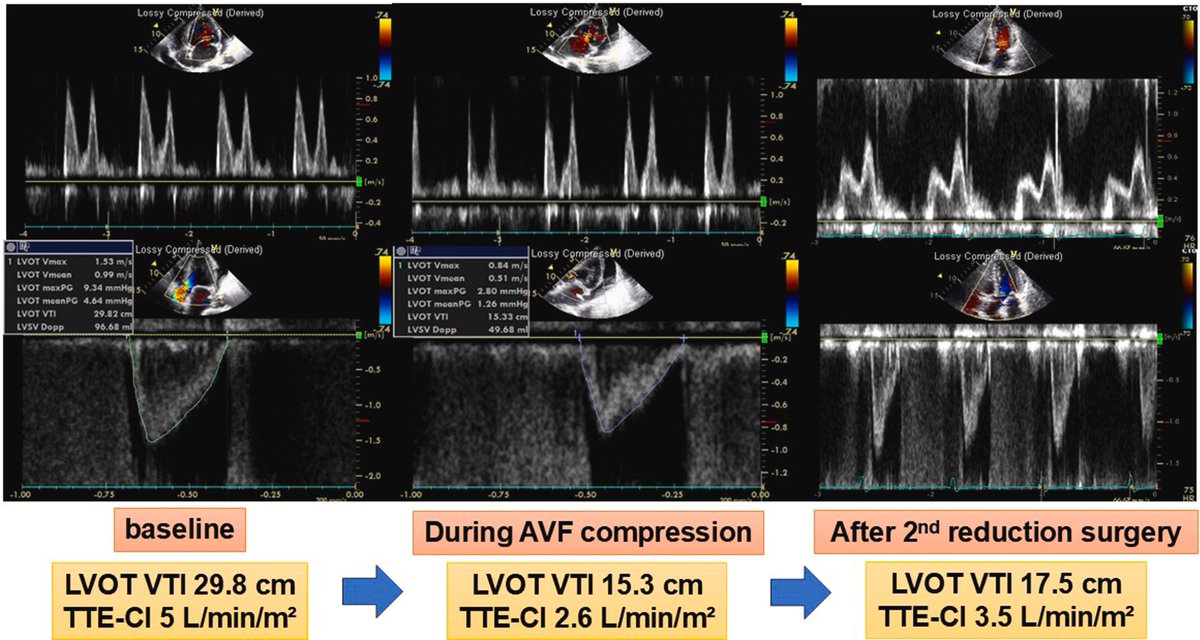
High-output heart failure associated with arteriovenous fistula remains an underrecognized, albeit well-described, clinical entity. This is a nice case with illustrative images - doi: 10.1016/j.jaccas.2026.107193. PMID: 41770183
#POCUS #Nephpearls
2
27
104
5,240
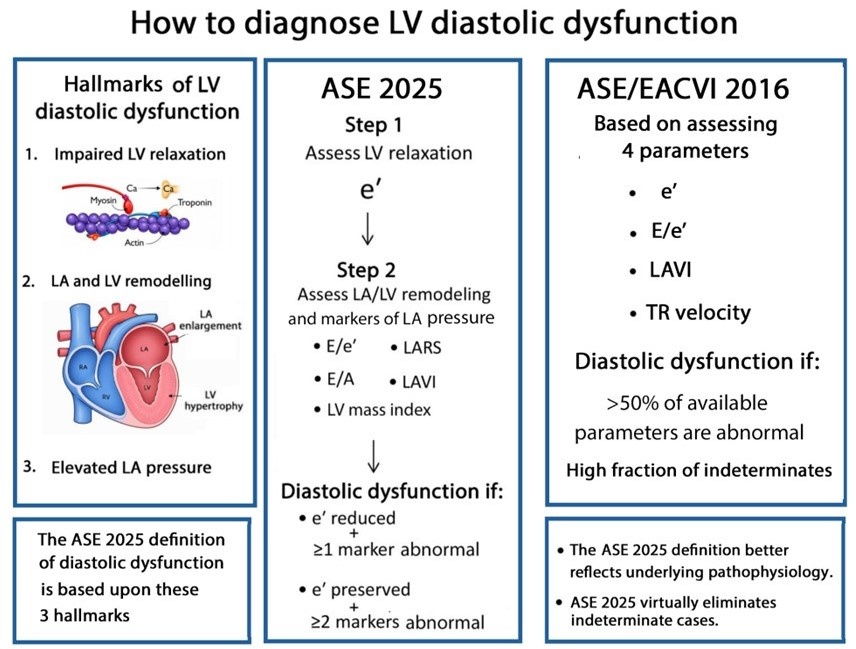
La diastologia que es mi dolor de cabeza🤕 🤯, explicada de forma más sencilla 🤓! Gracias 🤩
Jun 11

Most echocardiography laboratories have adopted the 2016 diastolic guidelines. With the release of the 2025 update, an important question arises:
What are the key conceptual differences between the 2016 and 2025 approaches to diagnosing diastolic dysfunction?
academic.oup.com/ehjcimaging…
@JGrapsa
3
10
980
Mark GN retweeted

Jun 4
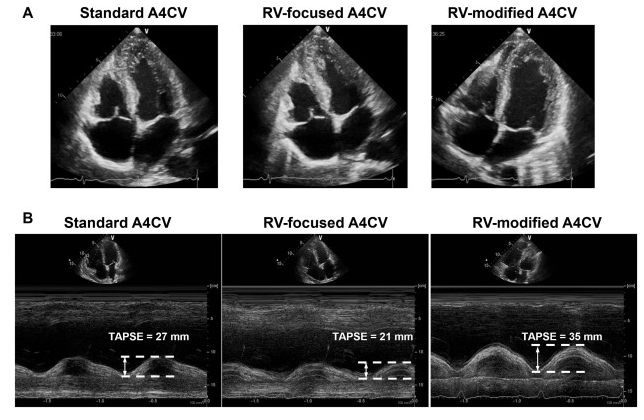
🫀¿Cuál es la vista ecocardiográfica más adecuada para medir el TAPSE?
El plano apical de 4 cámaras modificado.
👉🏼 Presenta una mejor concordancia con el strain del ventrículo derecho
👉🏼 Disminuye los errores relacionados con la angulación del haz de ultrasonido
🔗 DOI: 10.1016/j.echo.2024.12.013
42
145
5,557
Mark GN retweeted

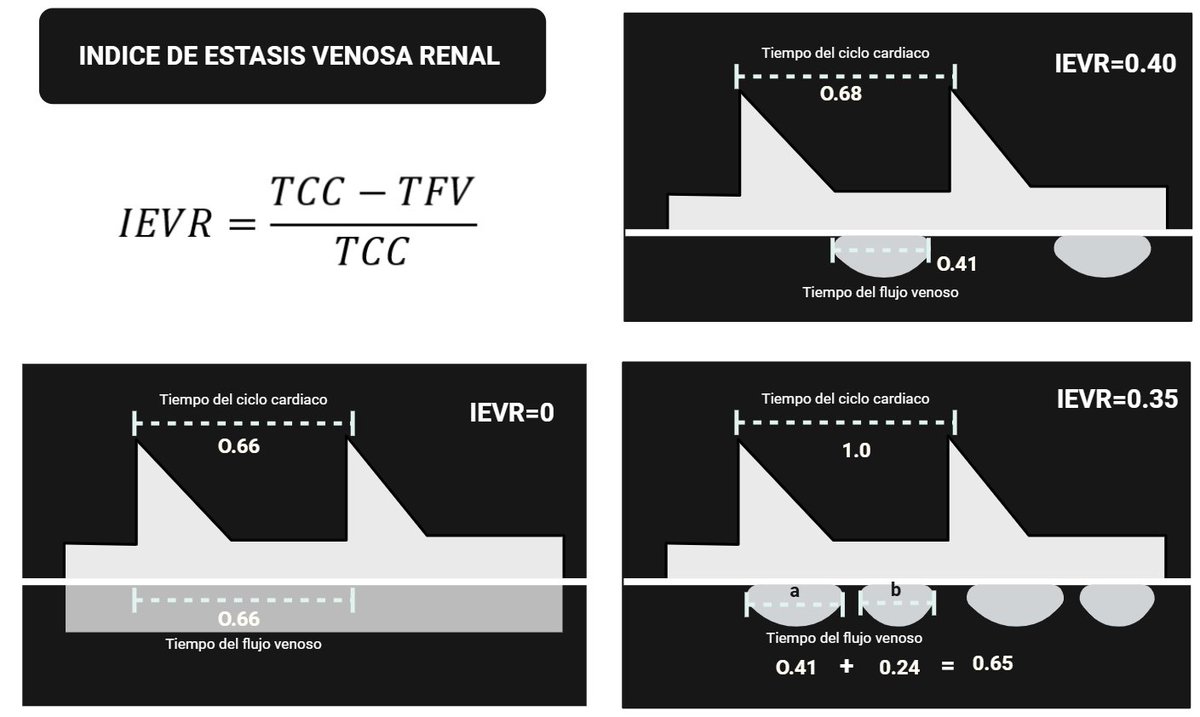
Qué es el índice de estasis venosa renal (IEVR) y para qué sirve medirlo? 🤔
1
3
6
279
Mark GN retweeted
Jun 1
Hepatic vein Doppler waveform components explained.
#POCUS #VExUS #Nephpearls
🔗youtu.be/7KII6btTGJ8?si=YsnK…
37
110
14,564
Mark GN retweeted
May 31
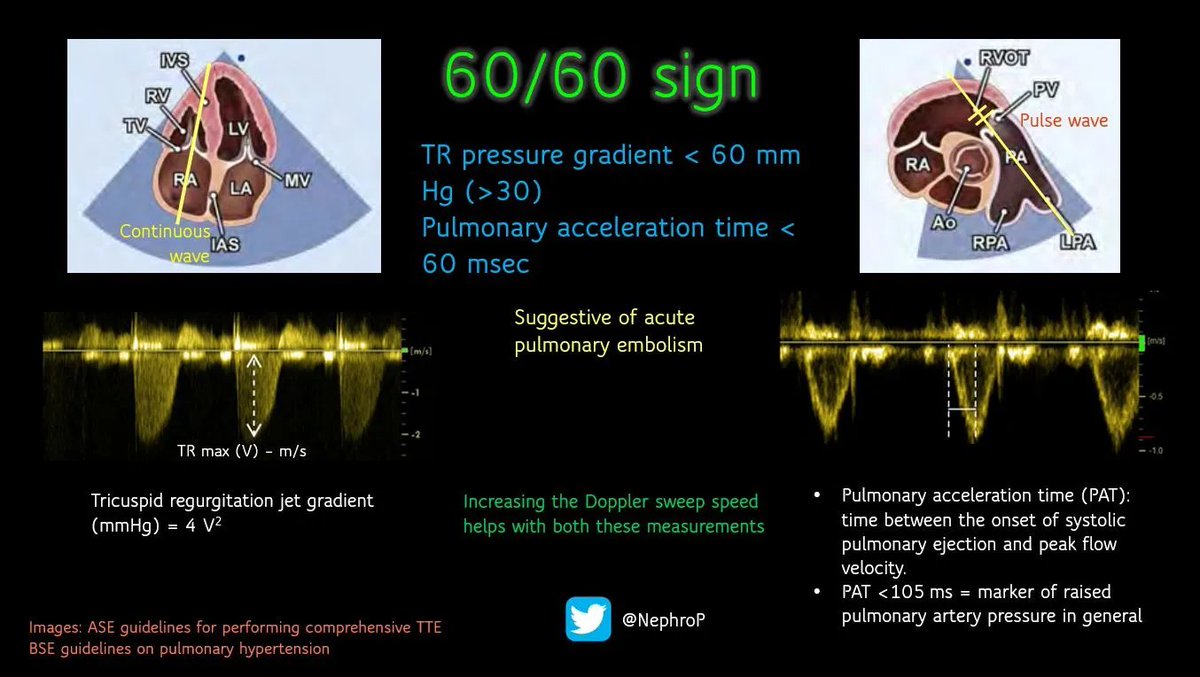
The 60/60 sign is a cardiac #POCUS finding used to support the bedside diagnosis of acute pulmonary embolism. It refers to the simultaneous presence of two measurements, both involving the number 60.
RV outflow tract (RVOT) acceleration time ≤60 ms - This is the time from the onset of blood flow through the pulmonary valve to its peak velocity. In acute PE, the sudden obstruction causes blood to accelerate and decelerate abnormally fast, producing a "truncated" or shortened flow profile.
Pulmonary artery systolic pressure (PASP) ≤60 mmHg (but >30 mmHg) - estimated via the tricuspid regurgitation jet.
In acute PE, the thin-walled right ventricle cannot generate very high pressures because it has not had time to adapt. A PASP above 60 mmHg suggests a chronic process (e.g., chronic pulmonary hypertension) where the RV has hypertrophied over time
2
29
131
5,324
Mark GN retweeted
May 31
#POCUS #echofirst #Nephpearls
RVOT pulse-wave Doppler can provide useful clues about pulmonary vascular resistance.
In normal individuals (A), the waveform has a smooth, dome-shaped appearance, with peak velocity occurring in mid-systole, reflecting a compliant, low-resistance pulmonary circulation.
As RV afterload increases, the waveform gradually becomes more triangular. The RVOT acceleration time shortens, and the peak velocity shifts earlier into systole (B).
With further increases in pulmonary vascular impedance and reduced arterial compliance, a characteristic mid-systolic notch may appear (C), creating the classic "W sign."
In advanced pulmonary hypertension with RV failure, the Doppler envelope becomes smaller and more abbreviated, with a very short and steep AccT (D). This reflects rapid equilibration of RVOT and proximal pulmonary artery pressures due to severe afterload elevation.
Like most POCUS findings, RVOT Doppler should be interpreted in the context of the overall echocardiographic picture rather than in isolation.

May 31

#POCUS #Nephpearls #FOAMed
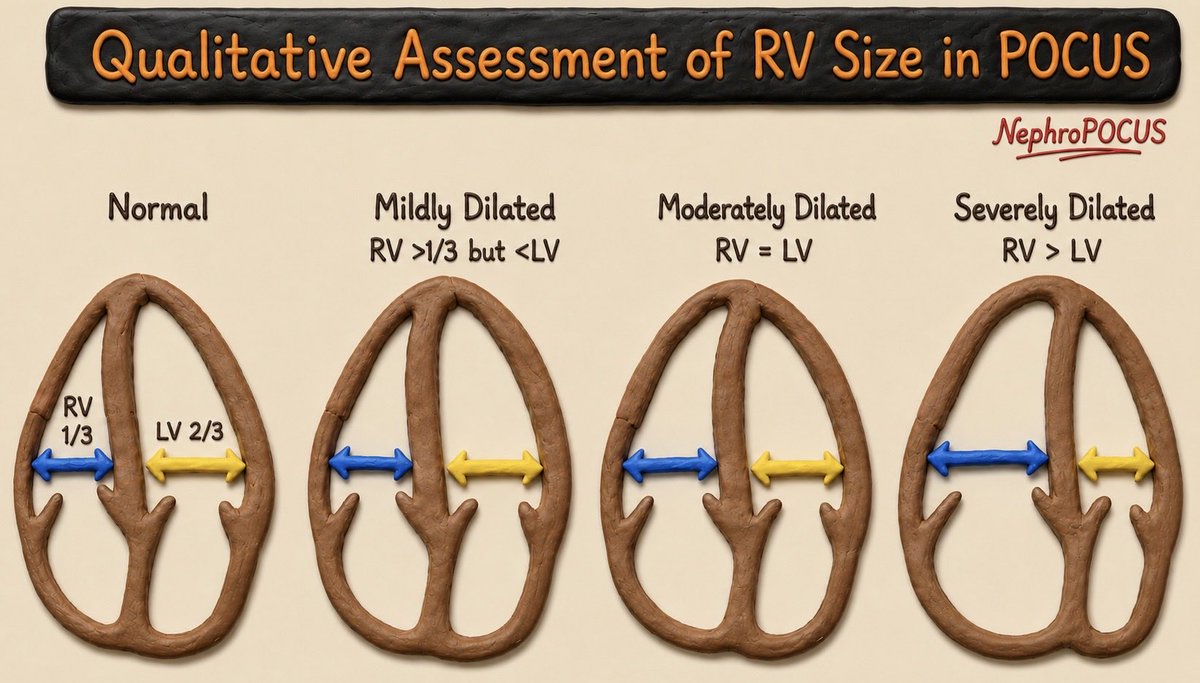
The RV should normally appear smaller than the LV in the apical 4-chamber view and should not exceed about two-thirds of the LV size. If the RV appears equal to or larger than the LV, significant RV dilation should be suspected.
Another helpful visual clue is when the RV becomes the apex-forming ventricle instead of LV. While this finding has not been formally validated with quantitative thresholds, it generally suggests at least moderate RV dilation.
If you remember just one measurement, remember this: the upper limit of normal RV basal diameter is 4.2 cm, measured at end-diastole in an RV-focused apical 4-chamber view.
Also assess RV wall thickness. An RV end-diastolic free wall thickness >5 mm (typically measured in the subcostal view) indicates RV hypertrophy, which often accompanies chronic pressure overload and RV dilation.
Finally, don’t forget to look for interventricular septal flattening on the parasternal short-axis view. Septal flattening (“D-shaped” LV) is another important clue to RV pressure and/or volume overload.
1
39
113
12,933
Mark GN retweeted
May 31
#POCUS #Nephpearls #FOAMed
The RV should normally appear smaller than the LV in the apical 4-chamber view and should not exceed about two-thirds of the LV size. If the RV appears equal to or larger than the LV, significant RV dilation should be suspected.
Another helpful visual clue is when the RV becomes the apex-forming ventricle instead of LV. While this finding has not been formally validated with quantitative thresholds, it generally suggests at least moderate RV dilation.
If you remember just one measurement, remember this: the upper limit of normal RV basal diameter is 4.2 cm, measured at end-diastole in an RV-focused apical 4-chamber view.
Also assess RV wall thickness. An RV end-diastolic free wall thickness >5 mm (typically measured in the subcostal view) indicates RV hypertrophy, which often accompanies chronic pressure overload and RV dilation.
Finally, don’t forget to look for interventricular septal flattening on the parasternal short-axis view. Septal flattening (“D-shaped” LV) is another important clue to RV pressure and/or volume overload.
2
35
134
14,855
12/
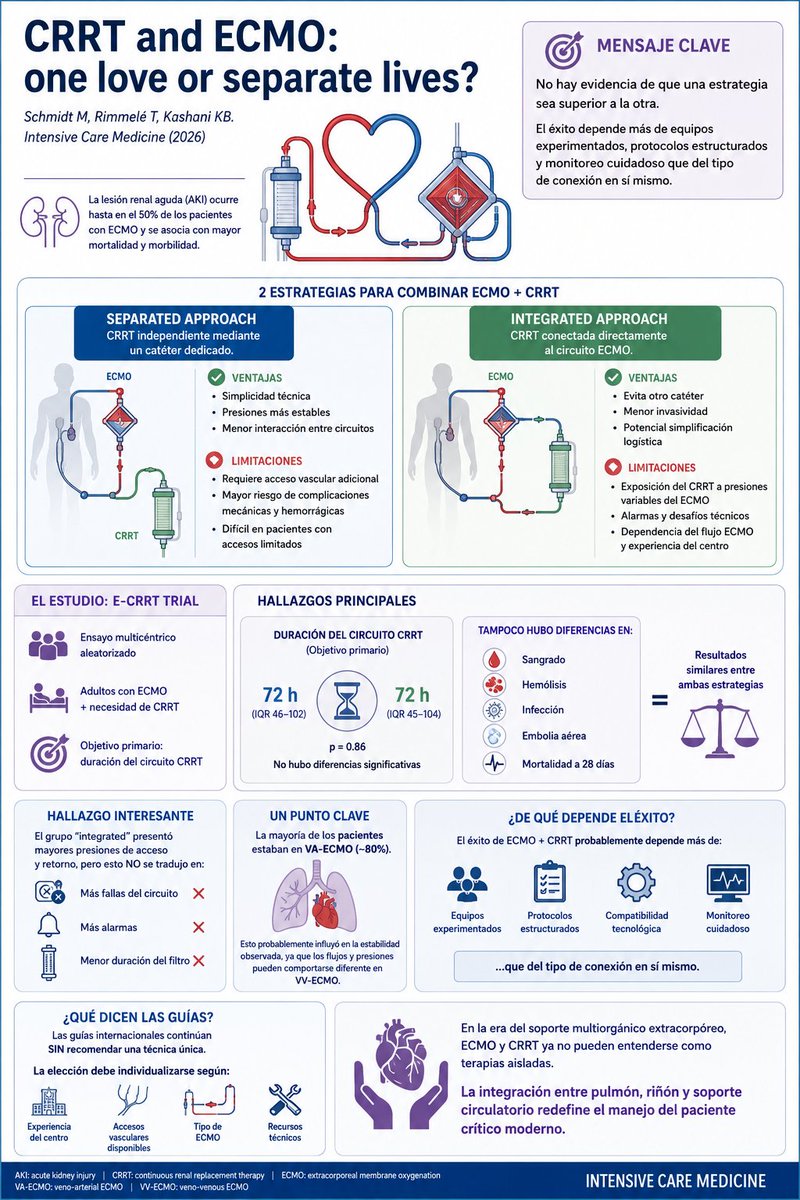
📚 Editorial:
“CRRT and ECMO: one love or separate lives?”
Schmidt M, Rimmelé T, Kashani KB.
Intensive Care Medicine (2026)
#ECMO #CRRT #AKI #CriticalCare #Nephrology #IntensiveCare #ExtracorporealSupport #NephrologyTwitter #FOAMed #ECMOlife
70