
Joined January 2013
- Tweets 2,290
- Following 3,351
- Followers 2,531
- Likes 7,970
210 Photos and videos










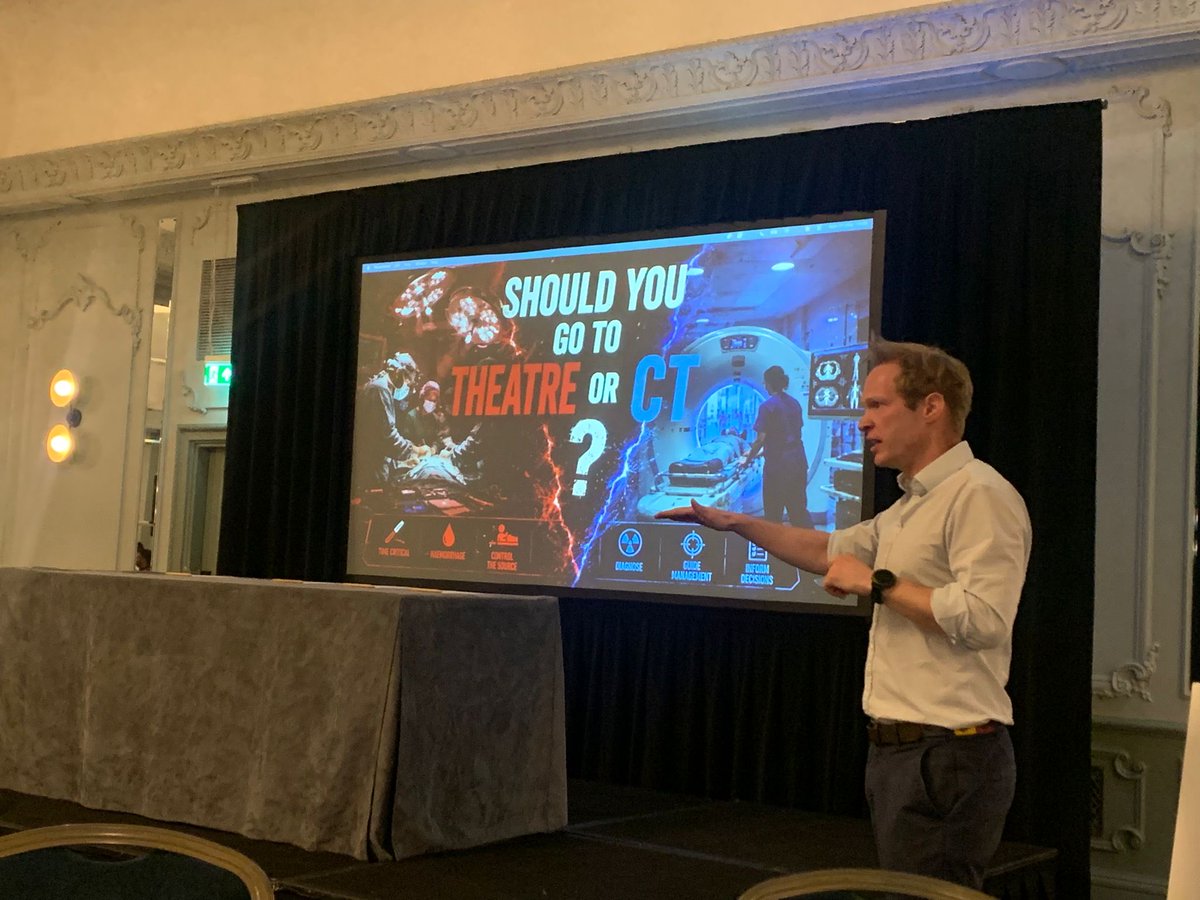
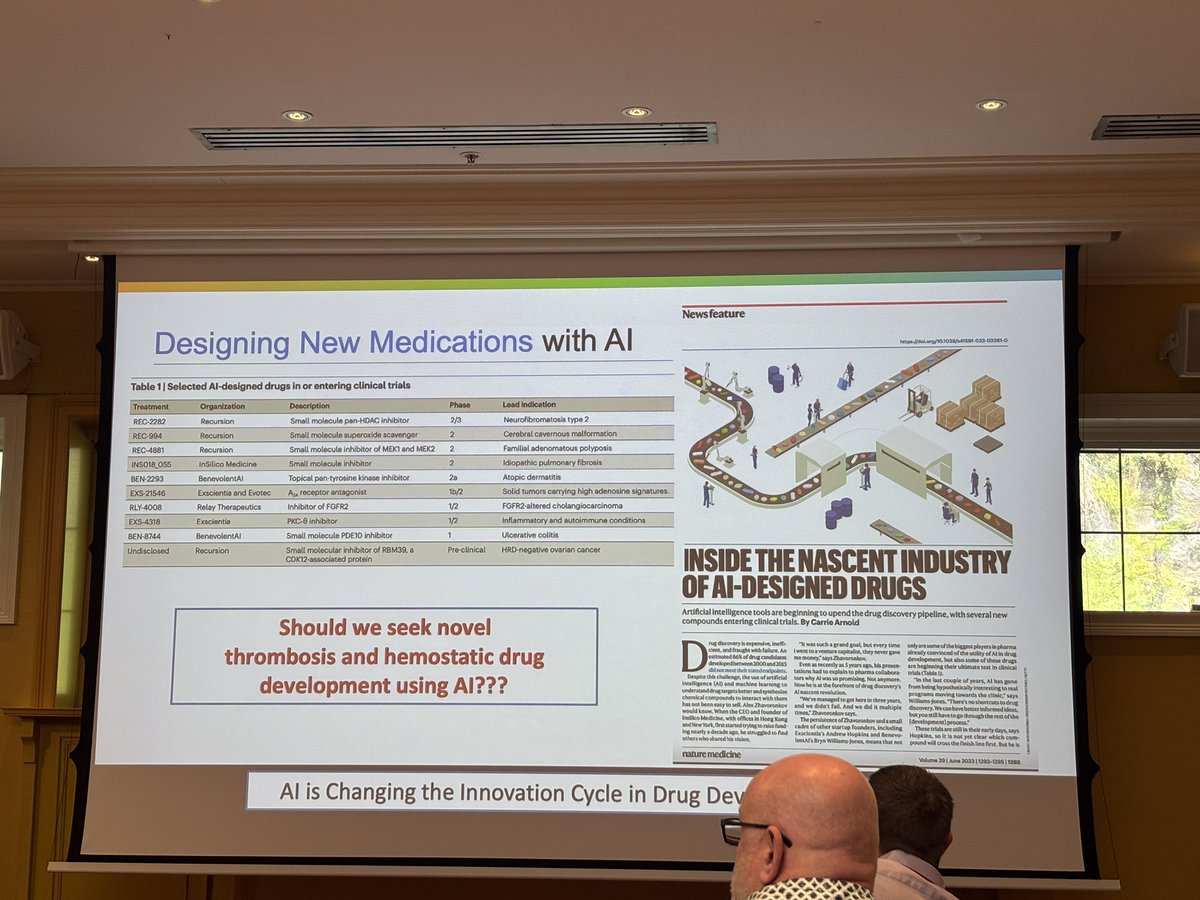
Critical decision-making in trauma- Penetrating Thoraco-abdominal injury. Laparotomy or Thoracotomy?
Success relies not just on operative skill, but on strategic restraint-knowing that CT scans lie about the diaphragm, chest tubes lie about the source of blood, and that surviving the trauma requires deliberately identifying the true source of instability before making the first incision. @MaxMarsden83 #ASGBI2026

3
11
899
Critical decision-making in trauma- @MaxMarsden83 is back, challenging us to think about blunt thoraco-abdominal trauma decisions. #ASGBI2026
4
15
831
Max Marsden retweeted

Apr 30
A study published today in Science may be the most important AI paper in clinical medicine this year. And it happened to land on the same day I submitted a letter to JAMA arguing that AI can already deliver clinically adequate care for defined tasks.
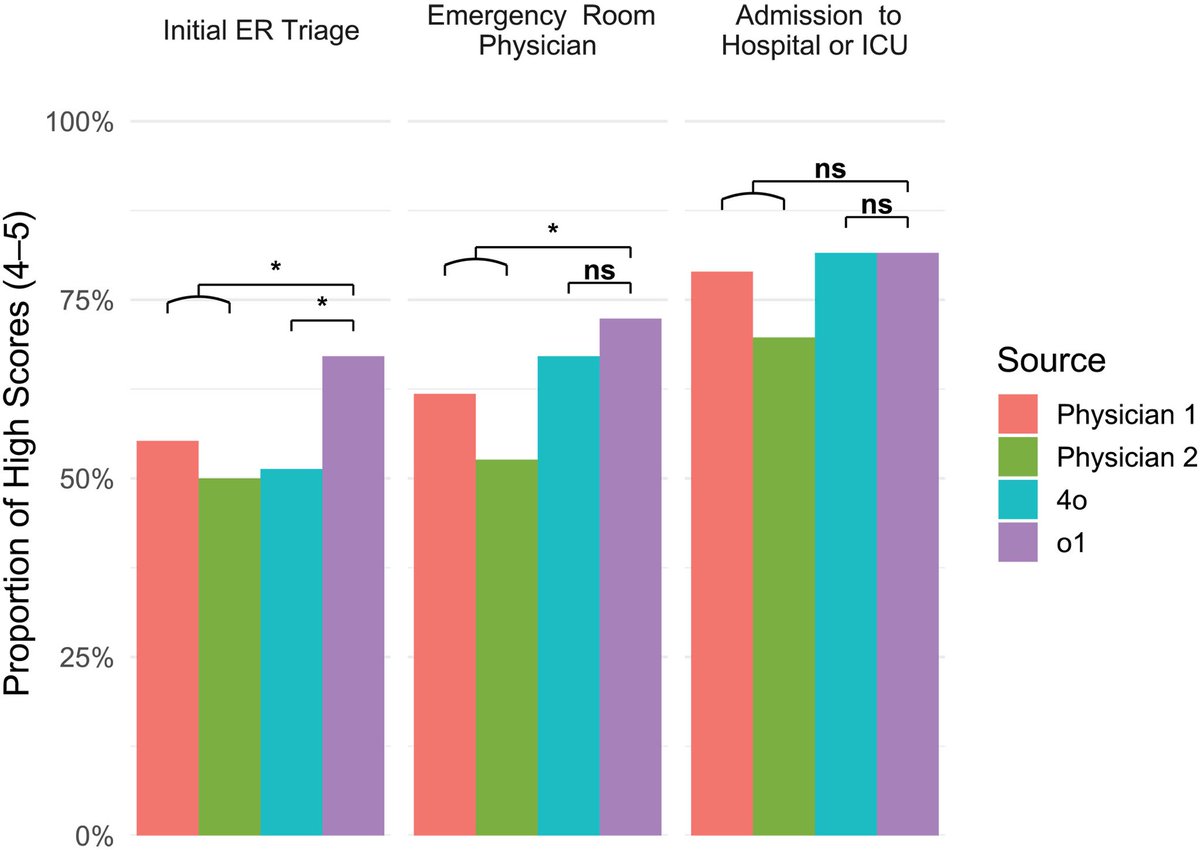
Researchers at Harvard Medical School and Beth Israel Deaconess Medical Center ran six experiments pitting OpenAI's o1 reasoning model against hundreds of physicians across the full spectrum of clinical reasoning: differential diagnosis, management planning, probabilistic reasoning, and clinical documentation. Then they did something most AI studies don't. They tested it on 76 real, unstructured emergency department cases pulled directly from the medical record at a major academic medical center.
The results across all six experiments: the AI outperformed physicians.
On the real ER cases — the messiest, most clinically relevant test — the AI identified the correct or very close diagnosis in 67.1% of cases at initial triage, 72.4% at ER physician evaluation, and 81.6% at hospital admission. The two attending physicians scored 55.3% and 50.0% at triage, 61.8% and 52.6% at ER evaluation, and 78.9% and 69.7% at admission. The gap was widest at initial triage.
On management reasoning using expert-scored clinical vignettes, the AI scored a median of 89%. Physicians with conventional resources scored 34%. That is not a typo.
The physician evaluators were blinded and could not distinguish AI-generated differentials from human ones. One evaluator guessed correctly 15% of the time. The other guessed correctly 3% of the time.
I'm an emergency physician. I work in a rural Texas ED. These are my cases. These are my decision points. And I can tell you that the triage finding is the one that matters most. Triage is where the least information meets the highest stakes — where the wrong call means a patient sits in the waiting room while their sepsis progresses or their STEMI evolves. The AI was 12 to 17 percentage points better than experienced attendings at exactly that moment.
The authors are careful to note this is text-based reasoning only; the AI doesn't see the patient's distress, doesn't hear breath sounds, doesn't read the room. Those are real limitations today. But the cognitive reasoning component of emergency medicine — pattern recognition under uncertainty with incomplete data — is precisely what this model is demonstrating it can do.
This was published in Science. Not a preprint. Not a company blog post. Peer-reviewed, in one of the two most prestigious scientific journals in the world.
The profession needs to stop debating whether AI will be good enough. It needs to start planning for the fact that, for an expanding set of clinical reasoning tasks, it already is.
And yes, this was written with AI. Sorry!!
41
126
384
49,717

7 Oct 2025
Thanks to @BehindTheKnife For the opportunity and to The awesome co-hosts, Prash, Roisin and Mr Aylwin
1
2
386
7 Oct 2025
After years of listening to Behind the Knife—it even helped me pass my FRCS!—it was brilliant to finally contribute. Dive into London's trauma system management here: [open.spotify.com/episode/59r…]
3
2
13
1,916
Max Marsden retweeted

29 Sep 2025
Juicy new CLINICAL CHALLENGES IN TRAUMA SURGERY ➡️ Stabbed in the Back - Decision Making in a Penetrating Junctional Vascular Injury🩸
Join our elite @LonTraumaSchool team @maxmarsden83 @cjaylwin for an engaging, high-yield conversation.
🎧behindtheknife.org/podcast/c…🎧
5
18
5,961
Max Marsden retweeted

18 Sep 2025
🚨The impact of trauma is massive and goes beyond mortality🚨
Only around half of patients went home within 30 days following the trauma laparotomy to the same level of care they had before their injury 🩼
@AmoskoJoachim @AbdulahiSaidHa1 @EderCaceres5 @MaxMarsden83 @carlosnunog
1
4
5
1,393
7 Jul 2025
RT @georgoff: PENETRATING LUNG 🫁 INJURY?!
Rule of 👍🏼 ➡️ 1500 cc bloody drainage @ time of chest tube placement or > 200 cc/hr 🟰 OR. In r…
13
Max Marsden retweeted

6 Jul 2025
I wasn’t there, but know that the role played by friends. colleagues, and people we don’t know, on 7/7 was extrordimary. There are amazing people in this world, with acts of kindness always outglowing the hate. 🙏🏼 for everyone who was affected, and who played a part to help.
2
31
1,615
Max Marsden retweeted

10 Jun 2025
A woman in West Virginia snapped a one-in-a-million shot of a tree being struck by lightning. Photographed by Donnie Dania.

533
7,724
78,321
2,770,907
Max Marsden retweeted

1 Jun 2025
You didn’t just build a trauma system you set off a ripple effect that reshaped trauma care across the globe.
Thousands of lives saved thousands of learners taught! A model studied and copied.
Legends don’t step down. They leave shockwaves.
Respect, Karim 👊
1
2
22
3,100
Max Marsden retweeted

20 May 2025
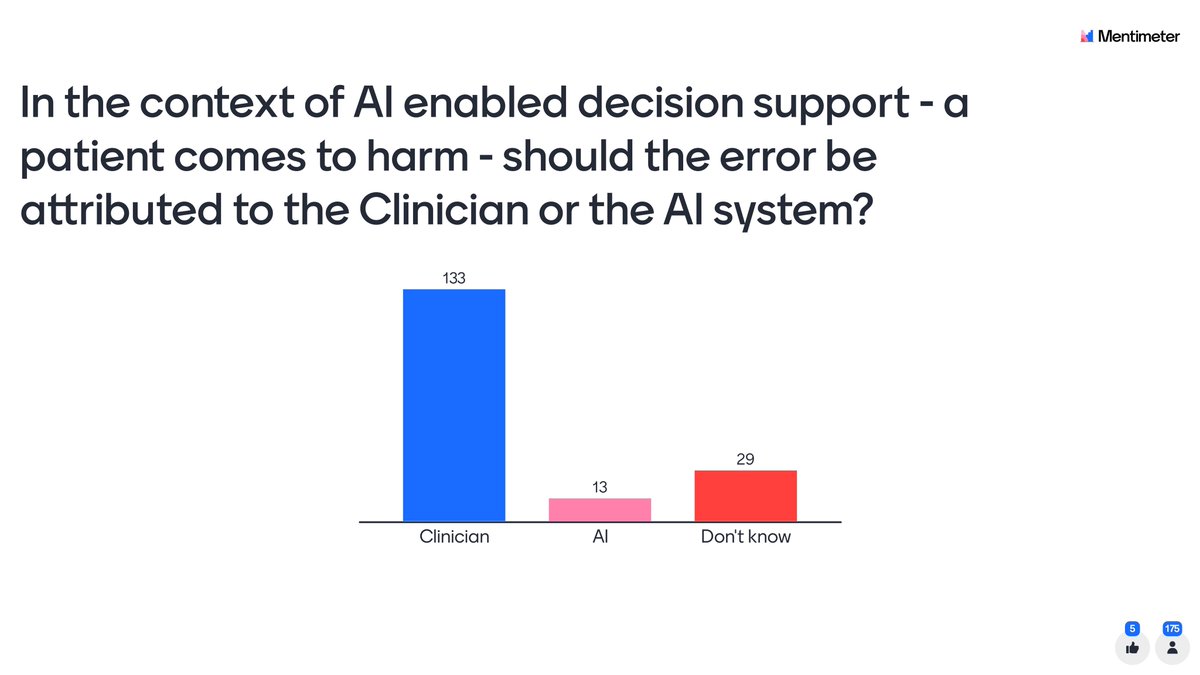
Awesome panel on the role of AI in decision making in trauma patients, expertly presented by @MaxMarsden83, and @callcura at @theTHORnetwork #THOR2025

1
4
6
731
Max Marsden retweeted

13 May 2025
An excellent turnout from @LeedsEGS at the @asgbi Gala Dinner last night! Superb location and excellent craic with a ceilidh to top things off! @abppc @josiewalshaw1

6
29
1,715

Hey, what do you think? IV or IO?
This video in our partnership with @DGlaucomflecken summarizes new research comparing initial attempts at intraosseous or intravenous vascular access in adults who had out-of-hospital cardiac arrest.
Full trial: nej.md/DrG14
23
109
620
73,320

📣📣 > 300 data entries so far for MORF: UK
‼️Not started yet? Hurry up and join us! Email the study team at morf.uk2024@gmail.com to get involved!
@karimbrohi @NaTRIC_Research @ceribattle @MaxMarsden83
3
5
624
Max Marsden retweeted

28 Mar 2025
Our first Trauma session of the day happening 🩸with @MaxMarsden83 our MA Alumni Trauma Lead
#MaOncall #masterclass #trauma #FRCS
1
3
15
969
Max Marsden retweeted

27 Feb 2025
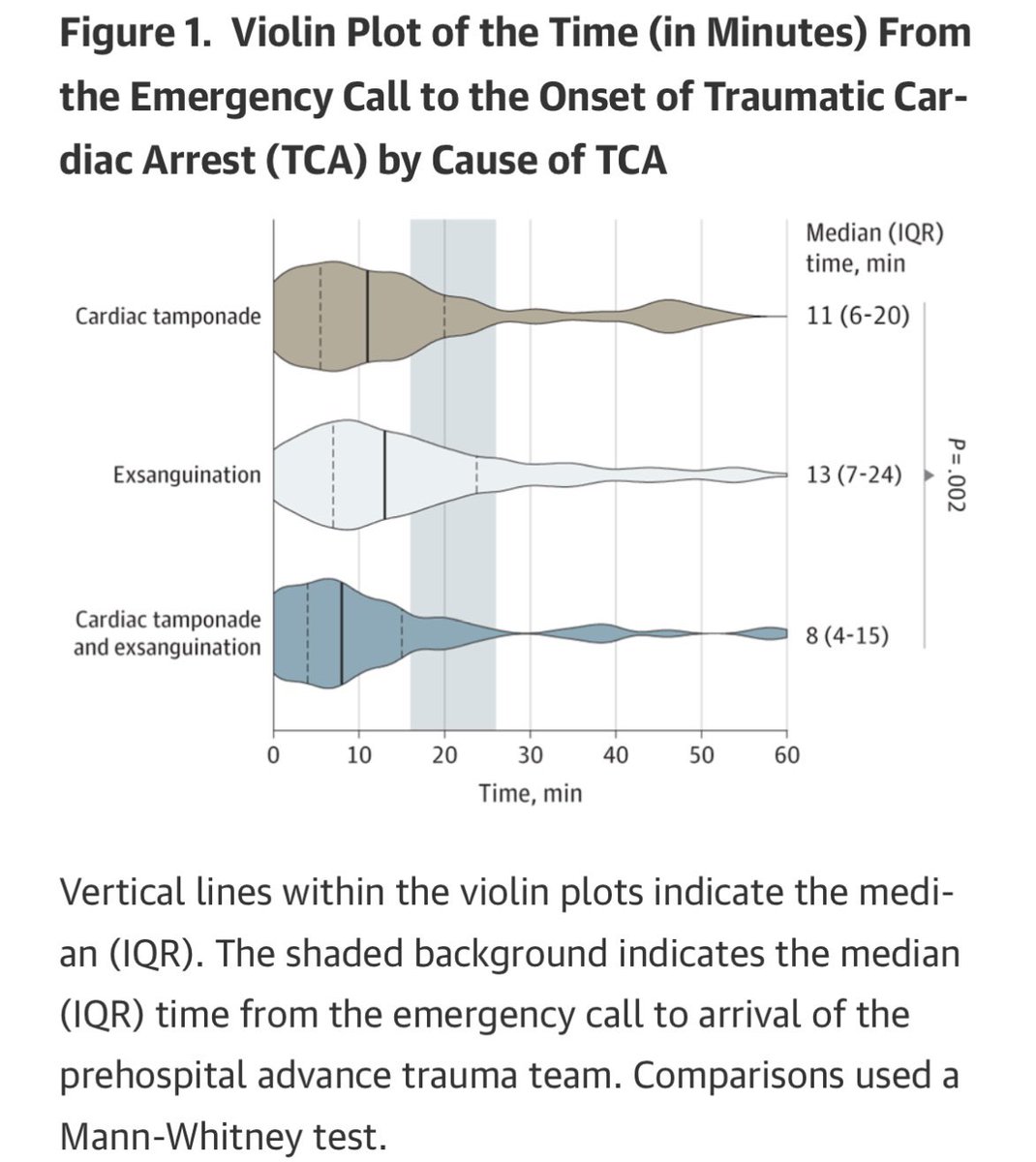
Prehospital Resuscitative Thoracotomy for Traumatic Cardiac Arrest - @LDNairamb's experience from 20 years. Amazing effort @ZBPerkins @GreenhalghRob @robbielendrum et al jamanetwork.com/journals/jam… #HEMS #TCA
51
108
7,955
Max Marsden retweeted

27 Feb 2025
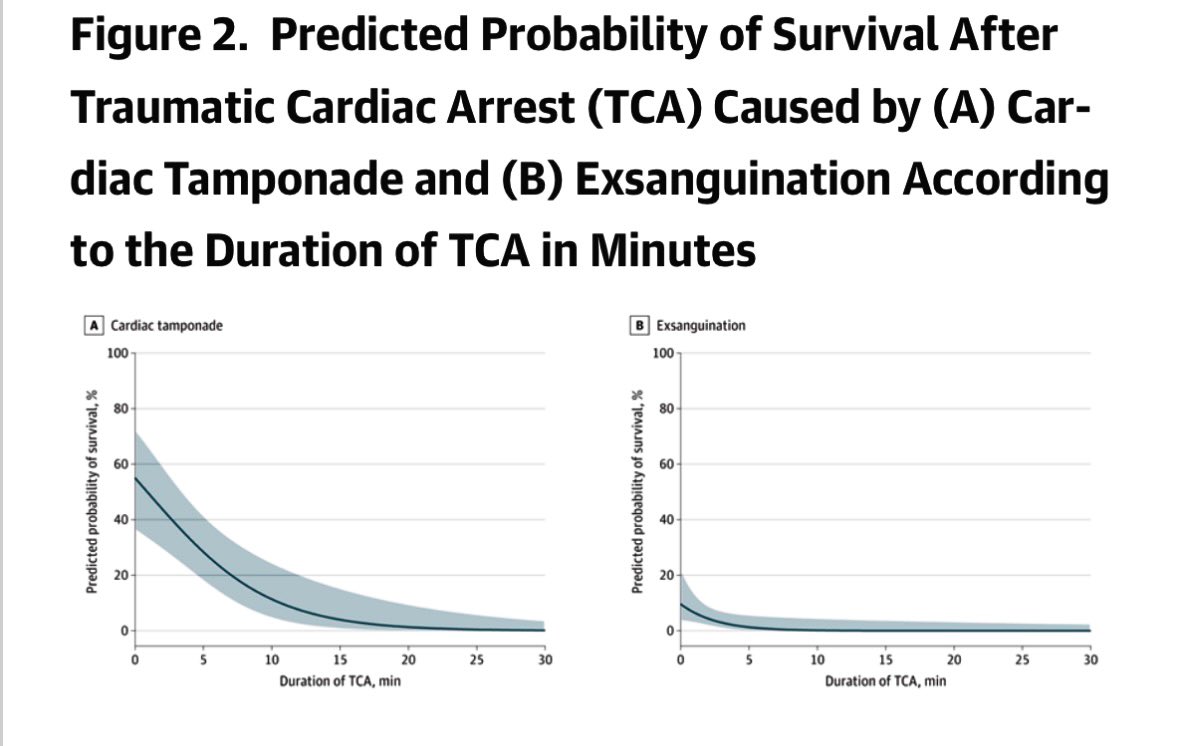
Median time from injury to TCA (tamponade) 11 mins, but there is a window to intervene in this system (on scene 20 mins post injury).
Survival 52% (tamponade) if RT at point of TCA or within 1 minute!… not a treatment for exsanguination in this cohort jamanetwork.com/journals/jam…
22
72
6,723
Max Marsden retweeted

17 Jan 2025
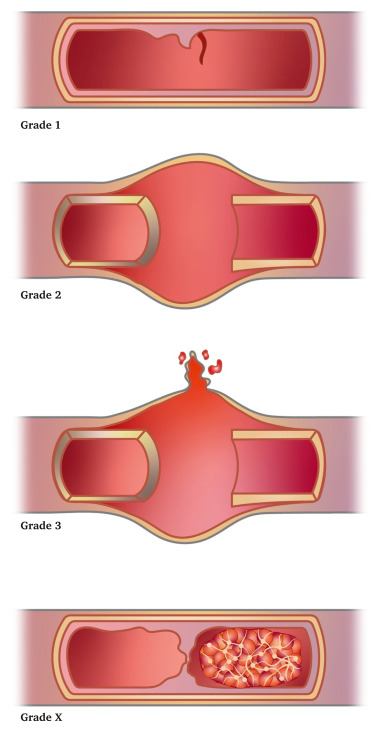
A quick primer on the new ESVS vascular injury scale. This can be applied to ALL vascular injuries and should provide a general understanding of the approach to these injuries.
ESVS grading is 1, 2, 3 or X. 1-3 are grades of wall injury, X is complete occlusion. So.. 🧵
14 Jan 2025

The new ESVS Vascular Trauma Guidelines 2025 have just been published, open access.
ejves.com/article/S1078-5884…
A massive piece of work, to bring vascular trauma kicking and screaming into the 21st century.
Your grandpa vascular surgeon ain't going to like them!
1
11
21
6,560
The MORF-UK study is underway
The protocol is published
Sites across the UK are open and collecting data - it’s not too late to join us‼️
Send us a DM or email morf.uk2024@gmail.com to get involved
@NaTRIC_Research @karimbrohi @TraumaEMC @ceribattle
13
21
4,528