
MD | Gender & DEI unbeliever. #LetKidsGrow 🌲 Evidence-driven compassion. 🗽 Free people flourish. 🇺🇸 Do No Harm Senior Fellow. Not med advice.
Joined August 2023
- Tweets 23,195
- Following 1,485
- Followers 5,849
- Likes 128,822
2,298 Photos and videos











Travis Morrell, MD MPH retweeted

Physicians did not lobby for "gender identity" to enter electronic health records, trans activists did. Find out how Epic EHR was captured. x.com/ColoradoDoctors/status…

WHEN EPIC ISN'T REALLY EPIC: How Gender Ideology Was Integrated into Epic Systems' Electronic Health Records
Epic Systems Corporation’s electronic health record (EHR) platform, used by approximately 41% of 🇺🇸 hospitals and historically as many as 80% of outpatient settings, as well as internationally, has systematically incorporated structured fields for self-identified gender identity that are separate from, and often displayed more prominently than, biological sex. The integration happened through a deliberate sequence of internal technical development at Epic, coordinated external advocacy from trans industry organizations, and federal regulatory requirements tied to incentive payments. The result is the Sexual Orientation and Gender Identity (SOGI) SmartForm, (sex) organ inventory tracking, visible patient banners and headers, automated SmartLinks, and configurable MyChart proxy access settings. These features treat gender identity as core, structured, queryable data embedded throughout clinical workflows, notes, portals, faxes, research queries, and national interoperability standards. To gender identity believers, nothing says “evidence-based medicine” quite like elevating subjective self-report to the level of immutable biology.
HOW IT STARTED
The internal catalyst at Epic was Janet Campbell, who joined the company in 2003 immediately after graduating from Carleton College with a computer science degree and additional coursework in gender studies. But, of course. Her first assigned project required building system rules to restrict diagnostic and billing codes according to recorded patient sex, for example, blocking orders for cervical examinations on patients whose record listed “male.” This work quickly revealed that Epic’s longstanding single “sex” field, limited since the company’s founding in 1979 to the options male, female, or unknown, was functionally "overloaded", as per Janet Campbell. It was seen to be simultaneously serving as a proxy for real sex or "sex assigned at birth", legal sex, and the emerging activist concept of gender identity. The resulting mismatches produced billing errors, inappropriate clinical alerts, and unreliable data for research or quality reporting, problems that, in a less ideological era, might have been solved by simply respecting biological reality rather than inventing new fields to accommodate delusuins.
In approximately 2004–2005, Campbell volunteered to deliver an internal educational presentation during Epic’s regular workplace talk series. One slide stated verbatim: “Epic is almost completely unable to deal with this level of complexity, and neither is the medical profession, for that matter.” Sure, Jan. By January 2012 she had posted an internal wiki page proposing a two- or three-step data-capture sequence: sex assigned at birth, legal sex, and gender identity. A cross-functional workgroup was assembled that included several "transgender" and "non-binary" Epic employees - its stated purpose was to assist customers with implementation. In 2013 the group produced and distributed a “SOGI Strategy” handbook that supplied both technical instructions and sections on "transgender cultural competence" and the distinction between identity and sex, helpfully ensuring that every hospital using the system received a gentle primer on why feelings should sometimes trump chromosomes.
INFLUENCE OF THE TRANS INDUSTRY
The external pressure that accelerated these changes came from a sustained advocacy campaign. The coalition involved represented a wide network of LGBT health, HIV advocacy, and related organizations, with prominent leadership from The Fenway Institute at Fenway Health. In January 2013 this coalition of 145 leading LGBT and HIV/AIDS organizations submitted a formal public comment to the Office of the National Coordinator for Health Information Technology (ONC) urging inclusion of sexual orientation and gender identity (SOGI) data collection in Meaningful Use guidelines. Early in 2014 the same network expanded to 153 organizations and submitted recommendations asking ONC to direct the National Library of Medicine to develop new SNOMED code sets specifically to support accurate and effective SO/GI data collection in certified EHRs. These submissions formed part of a broader effort to embed SOGI capacity within the proposed 2015 Edition Certified EHR Technology (CEHRT) criteria for Meaningful Use Stage 3. Because when biology proves stubborn, the next best step is apparently to lobby the government to reprogram the nation’s medical software. Fenway Health, operating through its Fenway Institute and National LGBTQIA Health Education Center, functioned as the central technical and policy coordinator.
As early as 2011, Fenway had begun testing two-step gender identity questions (gender identity asked first, followed by sex assigned at birth) at its own federally qualified health center. In roughly 2012 it published the policy brief “How to Gather Data on Sexual Orientation and Gender Identity in Clinical Settings,” which formalized the two-step approach originally developed by the Philadelphia Transgender Health Advocacy Coalition in 1997 and later endorsed by UCSF’s Center of Excellence for Transgender Health. Fenway partnered with the Center for American Progress on the “Do Ask, Do Tell” project, releasing online toolkits explicitly aimed at EHR vendors and providers. In 2014 Sean Cahill, PhD (Director of Health Policy Research at the Fenway Institute) co-authored key papers and policy statements, including the PLoS One article “Sexual Orientation and Gender Identity Data Collection in Clinical Settings and in Electronic Health Records: A Key to Ending LGBT Health Disparities,” which framed SOGI collection as essential for equity and disparity reduction. Fenway supplemented these writings with slide decks, tip sheets, and formal regulatory comments that repeatedly positioned SOGI capacity as a NON-NEGOTIABLE REQUIREMENT FOR FEDERAL CERTIFICATION 🚩, turning a contested religious belief at best into a certification checkbox.
IT'S ALWAYS THE GOVERNMENT
These advocacy efforts aligned precisely with federal rulemaking. The 2015 ONC and Centers for Medicare & Medicaid Services (CMS) Meaningful Use/Promoting Interoperability final rules mandated that certified EHRs possess the technical capacity to record, store, change, and retrieve structured SOGI data in order to qualify for incentive payments. The requirement applied across approximately 78 percent of outpatient clinics by 2018. In 2016 the Health Resources and Services Administration (HRSA) further embedded the expectation by adding SOGI fields to the Uniform Data System (UDS) reporting obligations for all federally qualified health centers. The combination of coalition pressure and incentive-linked certification created powerful compliance incentives for both vendors and health systems, because nothing motivates hospitals quite like the threat of lost federal dollars for failing to ask patients about their feelings. It's a clear, breathtaking case of policy winning over ethics in the medical field.
EXPANSION WITHIN
Inside Epic, Campbell’s initial workgroup scaled into a 25-person “Volunteer Army.” The team performed a full-system audit and remapped hundreds of references to the original “sex” field throughout patient headers, laboratory normal ranges, genetic pedigrees, clinical decision-support logic, and other modules. Campbell characterized the overhaul as “like the Y2K of the health record.” Development milestones followed in rapid succession: a two-item gender identity update released to clinical customers in June 2016, followed by the complete SOGI SmartForm in November 2016. The SmartForm is a guided questionnaire triggered by clicking the gender or age line in the patient Storyboard or during registration, nursing assessment, or clinical encounters. It begins by recording gender identity; any mismatch with recorded sex automatically prompts follow-up questions on pronouns (including they/them and additional options), transition steps, and an organ inventory that distinguishes organs present at birth from those present currently, because the most reliable way to practice “precision medicine” is apparently to ask patients what their body parts used to be while politely ignoring what they actually are. This also serves as proof of the linguistic weaponization trans activists indulge in - conflating legitimate things like kidney donation with calling an inverted penis lined with scrotal skin a vagina. It's part of the tactic to normalize grotesque and experimental "transgender surgeries" as "just routine medical procedures".
Further refinements to the EPIC EHR in 2017–2018 introduced explicit distinctions among legal sex, gender identity, sex assigned at birth, and “sex for clinical use,” while chosen names and pronouns were propagated system-wide via SmartLinks. By mid-2017 Campbell reported that 10–20 percent of Epic customers had activated the updates. The captured data is structured rather than free-text, making it visible and actionable: chosen name, gender identity, and pronouns appear in patient banners and headers; SmartLinks automatically insert the information into notes, schedules, faxes, and reports. Patients, including minors as young as 12 in many implementations, can enter or update these fields directly through the MyChart portal; changes become part of the official record without mandatory clinical verification, because self-ID is apparently so infallible that no second opinion from a doctor is required. Hospitals frequently incorporate SmartForm completion rates into quality metrics, disparity dashboards, and DEI scorecards, and staff training modules draw heavily on Fenway’s cultural-competence materials.
Campbell has explained the design rationale in public remarks. In 2017 she stated: “Our goal is that patients get the right and appropriate treatment no matter who they are.” On the decision for universal collection she added: “I think that starting to collect this information from everyone will normalize it in many people’s eyes. It’s not that we’re asking certain people whether they happen to be trans, we’re just asking everybody.”
The trans activism is ever present, presented dishonestly. In the August 31, 2022, Clinical Architecture Informonster Podcast (Episode 23: “Discussing Gender Harmony”), recorded with Fenway’s Chris Grasso, Campbell explained that the original single field “had become overloaded and was asked to do double duty.” She described the 2017 safety corrections, such as revised creatinine-clearance calculations based on mismatched legal sex, and noted broader applicability: “The work that we’re doing here will benefit the entire patient community… It’s not just transgender patients who want to be called by a name that’s different than the name on their birth certificate.” Regarding documentation she advised: “If a patient isn’t living their gender identity, don’t document that information in those fields… the system will take your word for it and will put that everywhere.” Right, all that confusion and hoop-jumping due to the religious and fanatical belief in "gender identity", trying to get ahead of the chaos being caused. Epic continues to participate in the HL7 Gender Harmony Project, which has produced a national interoperability standard separating recorded sex/gender, gender identity, and “sex for clinical use,” each with validity periods. The SOGI and organ-inventory data therefore support anatomy-based alerts while preserving identity fields as the primary display element, because the clearest way to avoid clinical confusion is apparently to make identity the banner headline and biology the optional footnote. Gender ideologues purposely calculate to supercede the practice of ethical medicine to bolster their claims, reality be damned.
TARGETING MINORS IS NOT ACCIDENTAL
MyChart proxy access for minors remains configurable by each health system and is age-tiered. Common configurations include independent portal access at age 12 (UF Health Shands), “Teen Plus” limited parental views (Wellstar), and parent-teen access at age 13 (UNC). "Sensitive sections" like SOGI data, preferred pronouns, organ inventory, and transition-related notes, CAN BE HIDDEN FROM PARENTS, frequently extending beyond the original intent of adolescent privacy statutes written for STIs or contraception. A 2025 Do No Harm @donoharm report catalogued these settings and quoted Epic’s own documentation, which states that proxy access “changes as they get older” according to each organization’s interpretation of privacy laws. Vague enough. The cumulative architecture produces a workflow in which gender-identity documentation is routine, frictionless, and self-reinforcing, marketed to the very young and old alike.
DECLINES TO ANSWER
If elderly patients are confused about "personal pronouns", they are marked as "Declined to answer" in a prominent manner in their profiles that anyone opening their chart can see. I have seen this happen to patients with dementia! This phrasing of "refused to cooperate" is meant to create bias in the minds of the clinician that the patient is difficult, and try to force compliance with gender ideology in both the doctor and the patient. Clinicians encounter prompts in core interfaces, data auto-propagates across the record and external systems, and non-use of the features can register as incomplete documentation or failure to meet incentive or equity metrics. These dubious metrics have converted advocacy goals into certification requirements. The outcome is a dominant EHR platform that has embedded self-identified gender identity as a core element across millions of patient records, completely ignoring evidence-based safeguards.
PATIENT SAFETY CONCERNS, THE ULTIMATE EPIC FAIL
Even in electronic health record systems where biologic sex, legal sex, and gender identity are all separately and clearly documented, significant patient-safety concerns remain because downstream clinical systems frequently fail to operationalize those distinctions consistently. Multiple health systems and informatics groups have documented that laboratory software, radiology workflows, preventive screening algorithms, insurance systems, and clinical decision-support tools often still rely on a single operative sex variable despite more sophisticated chart architecture.
At Geisinger Health System, clinicians and informatics staff described needing extensive custom modifications to Epic because standard workflows could not reliably coordinate birth sex, organ inventory, hormone exposure, and preventive screening logic simultaneously. The Veterans Health Administration similarly acknowledged tension between visibility of natal sex and identity-related workflows, warning that suppressing or obscuring biologic sex could impair preventive care and emergency clinical reasoning.
Real-world failures described in the literature include biologically female patients losing automated cervical cancer reminders after administrative sex changes, insurance denials for Pap smears or PSA testing when legal sex conflicted with anatomy, pregnancy-related safeguards failing because workflows operationalized identity-facing fields incorrectly, and laboratory systems inconsistently applying sex-based reference ranges for hemoglobin, creatinine, eGFR, CK, and troponin. Pathologists and laboratorians have repeatedly noted that current systems struggle to interpret altered hormone states because a testosterone-treated female remains biologically female while exhibiting partial shifts in selected analytes, creating ambiguity that simplistic identity-based categorization cannot safely resolve.
Researchers in medical AI and informatics have additionally warned that inconsistent handling of sex, gender identity, legal sex, and hormone exposure produces “sex/gender slippage” in datasets, threatening the reliability of epidemiology, predictive algorithms, and machine-learning models. The central concern raised by clinicians focused on sex-based medicine is therefore not merely missing data fields, but that medicine remains fundamentally organized around biologic sex while many EHR systems and institutional workflows operationalize sex-related variables inconsistently, creating opportunities for diagnostic error, screening failures, inappropriate clinical decision support, and degraded research quality even when all demographic categories are technically present and clearly separated.
The corruption of Epic EHR demonstrates how gender ideology became medical infrastructure when the right mix of activists, incentives, federal cooperation, and software engineers decided that their unfounded beliefs trump reality, endangering patient healthcare in the process. Your mind and body are both the donor organs and the subsequent profit to the trans industry. An EHR is a tool and repository that helps maintain and improve medical records. Using it to cement the nebulous concept of gender identity as fact is subjecting the material reality of patients and doctors to dangerous process errors and repeated trans industry indoctrination. Get your act together, EPIC, and put patient safety first, before it's too late.
SOURCES AND REFERENCES
- Ingraham N, et al. Overcoming technical and cultural challenges to delivering equitable care for LGBTQ individuals in a rural, underserved area. JAMIA Open. 2022.
PMC article
- Klee A, et al. Evolving Sex and Gender in Electronic Health Records. Fed Pract. 2018.
PMC article
- Greene DN, et al. Challenges in Transgender Healthcare: The Pathology Perspective. Clin Chem. 2016.
PMC article
- Cheung AS, et al. Approach to Interpreting Common Laboratory Pathology Tests in Transgender Individuals. J Clin Endocrinol Metab. 2021.
Oxford Academic article
- Keyes O, et al. Sex trouble: Sex/gender slippage, sex confusion, and sex obsession in machine learning using electronic health records. Patterns. 2022.
ScienceDirect article
- Kannan V, et al. Challenges with Accuracy of Gender Fields in Identifying Transgender Patients in Electronic Health Records. AMIA Annu Symp Proc. 2020.
PMC article
- Collecting Sexual Orientation and Gender Identity Data in Electronic Health Records. National Academies Press.
NCBI Bookshelf
- Wired.com, “The Battle to Get Gender Identity Into Your Health Records” (June 30, 2017) – Campbell’s timeline, internal presentation quote, 2012 wiki proposal, workgroup formation, 2013 SOGI Strategy handbook, Volunteer Army audit, Y2K comparison, and technical rollout details.
- Isthmus.com, “UW Health aims to be more sensitive to gender identity” (July 6, 2017) – Campbell’s direct quotes on the SmartForm purpose, normalization through universal collection, and adoption statistics (10–20% of customers, 20–40 providers).
- Clinical Architecture Informonster Podcast, Episode 23: “Discussing Gender Harmony” (August 31, 2022) – Full transcript excerpts of Campbell discussing the overloaded single sex field, 2017 clinical safety fixes, HL7 Gender Harmony collaboration, privacy advice, and benefits for all patients; includes joint discussion with Fenway’s Chris Grasso.
- Do No Harm report, “Parental Access to Children’s Medical Records” (October 2025) – Details on Epic SOGI SmartForm mechanics, organ inventory, MyChart proxy access configurations at specific health systems (UF Health Shands, Wellstar, UNC), and analysis of concealment practices beyond legal minimums.
- Fenway Health / National LGBTQIA Health Education Center, “Collecting Sexual Orientation and Gender Identity (SO/GI) Data in Electronic Health Records” (2016 PDF) – Implementation toolkits, clinical workflows, and ties to Meaningful Use / HRSA requirements.
- Cahill et al., “Sexual Orientation and Gender Identity Data Collection in Clinical Settings and in Electronic Health Records: A Key to Ending LGBT Health Disparities” (PLoS One, 2014) – Core advocacy paper outlining the case for SOGI inclusion.
- Fenway Health, “How to Gather Data on Sexual Orientation and Gender Identity in Clinical Settings” (policy brief, ~2012) – Early testing protocols and two-step question recommendations.
- Center for American Progress / Fenway Institute joint statement (October 7, 2015) – Praise for the 2015 ONC/CMS Meaningful Use rules requiring SOGI capacity in certified EHRs.
- Fenway Health “Do Ask, Do Tell” toolkit and related 2014–2016 publications – Broader SOGI EHR advocacy, promotion of standardized questions, and collaboration with other groups.
ONC/CMS 2015 Edition Certified EHR Technology (CEHRT) Criteria and Meaningful Use/Promoting Interoperability final rules – Federal requirements for SOGI data capacity in certified systems, tied to incentive payments.
- Additional cross-referenced context from HRSA Uniform Data System (UDS) updates (2016), HL7 Gender Harmony Project documentation, and public Epic customer implementation examples (e.g., University of Wisconsin, Geisinger). All information is drawn exclusively from publicly available records as of 2025.
- Cahill S. “Sexual Orientation and Gender Identity Data Collection Update: U.S. Government Takes Steps to Promote Sexual Orientation and Gender Identity Data Collection Through Meaningful Use Guidelines.” LGBT Health (2014/2016 update) – Details on the 153 LGBT and HIV groups’ 2014 recommendations to ONC for SNOMED codes and the 2013 public comment from 145 organizations.
- Cahill S, Makadon H. Related policy briefs and Fenway Institute publications (2012–2016) – Documentation of coalition advocacy, two-step questions, and EHR implementation guidance.
#sexnotgender #genderidentity #epicEHR #epic #epicfail #ehr #medicalethics #MedTwitter #MEDX #donoharm #safety #propaganda
2
5
110
Travis Morrell, MD MPH retweeted

This is the most incredible exposure of what Epic has done to destroy the medical system
WHEN EPIC ISN'T REALLY EPIC: How Gender Ideology Was Integrated into Epic Systems' Electronic Health Records
Epic Systems Corporation’s electronic health record (EHR) platform, used by approximately 41% of 🇺🇸 hospitals and historically as many as 80% of outpatient settings, as well as internationally, has systematically incorporated structured fields for self-identified gender identity that are separate from, and often displayed more prominently than, biological sex. The integration happened through a deliberate sequence of internal technical development at Epic, coordinated external advocacy from trans industry organizations, and federal regulatory requirements tied to incentive payments. The result is the Sexual Orientation and Gender Identity (SOGI) SmartForm, (sex) organ inventory tracking, visible patient banners and headers, automated SmartLinks, and configurable MyChart proxy access settings. These features treat gender identity as core, structured, queryable data embedded throughout clinical workflows, notes, portals, faxes, research queries, and national interoperability standards. To gender identity believers, nothing says “evidence-based medicine” quite like elevating subjective self-report to the level of immutable biology.
HOW IT STARTED
The internal catalyst at Epic was Janet Campbell, who joined the company in 2003 immediately after graduating from Carleton College with a computer science degree and additional coursework in gender studies. But, of course. Her first assigned project required building system rules to restrict diagnostic and billing codes according to recorded patient sex, for example, blocking orders for cervical examinations on patients whose record listed “male.” This work quickly revealed that Epic’s longstanding single “sex” field, limited since the company’s founding in 1979 to the options male, female, or unknown, was functionally "overloaded", as per Janet Campbell. It was seen to be simultaneously serving as a proxy for real sex or "sex assigned at birth", legal sex, and the emerging activist concept of gender identity. The resulting mismatches produced billing errors, inappropriate clinical alerts, and unreliable data for research or quality reporting, problems that, in a less ideological era, might have been solved by simply respecting biological reality rather than inventing new fields to accommodate delusuins.
In approximately 2004–2005, Campbell volunteered to deliver an internal educational presentation during Epic’s regular workplace talk series. One slide stated verbatim: “Epic is almost completely unable to deal with this level of complexity, and neither is the medical profession, for that matter.” Sure, Jan. By January 2012 she had posted an internal wiki page proposing a two- or three-step data-capture sequence: sex assigned at birth, legal sex, and gender identity. A cross-functional workgroup was assembled that included several "transgender" and "non-binary" Epic employees - its stated purpose was to assist customers with implementation. In 2013 the group produced and distributed a “SOGI Strategy” handbook that supplied both technical instructions and sections on "transgender cultural competence" and the distinction between identity and sex, helpfully ensuring that every hospital using the system received a gentle primer on why feelings should sometimes trump chromosomes.
INFLUENCE OF THE TRANS INDUSTRY
The external pressure that accelerated these changes came from a sustained advocacy campaign. The coalition involved represented a wide network of LGBT health, HIV advocacy, and related organizations, with prominent leadership from The Fenway Institute at Fenway Health. In January 2013 this coalition of 145 leading LGBT and HIV/AIDS organizations submitted a formal public comment to the Office of the National Coordinator for Health Information Technology (ONC) urging inclusion of sexual orientation and gender identity (SOGI) data collection in Meaningful Use guidelines. Early in 2014 the same network expanded to 153 organizations and submitted recommendations asking ONC to direct the National Library of Medicine to develop new SNOMED code sets specifically to support accurate and effective SO/GI data collection in certified EHRs. These submissions formed part of a broader effort to embed SOGI capacity within the proposed 2015 Edition Certified EHR Technology (CEHRT) criteria for Meaningful Use Stage 3. Because when biology proves stubborn, the next best step is apparently to lobby the government to reprogram the nation’s medical software. Fenway Health, operating through its Fenway Institute and National LGBTQIA Health Education Center, functioned as the central technical and policy coordinator.
As early as 2011, Fenway had begun testing two-step gender identity questions (gender identity asked first, followed by sex assigned at birth) at its own federally qualified health center. In roughly 2012 it published the policy brief “How to Gather Data on Sexual Orientation and Gender Identity in Clinical Settings,” which formalized the two-step approach originally developed by the Philadelphia Transgender Health Advocacy Coalition in 1997 and later endorsed by UCSF’s Center of Excellence for Transgender Health. Fenway partnered with the Center for American Progress on the “Do Ask, Do Tell” project, releasing online toolkits explicitly aimed at EHR vendors and providers. In 2014 Sean Cahill, PhD (Director of Health Policy Research at the Fenway Institute) co-authored key papers and policy statements, including the PLoS One article “Sexual Orientation and Gender Identity Data Collection in Clinical Settings and in Electronic Health Records: A Key to Ending LGBT Health Disparities,” which framed SOGI collection as essential for equity and disparity reduction. Fenway supplemented these writings with slide decks, tip sheets, and formal regulatory comments that repeatedly positioned SOGI capacity as a NON-NEGOTIABLE REQUIREMENT FOR FEDERAL CERTIFICATION 🚩, turning a contested religious belief at best into a certification checkbox.
IT'S ALWAYS THE GOVERNMENT
These advocacy efforts aligned precisely with federal rulemaking. The 2015 ONC and Centers for Medicare & Medicaid Services (CMS) Meaningful Use/Promoting Interoperability final rules mandated that certified EHRs possess the technical capacity to record, store, change, and retrieve structured SOGI data in order to qualify for incentive payments. The requirement applied across approximately 78 percent of outpatient clinics by 2018. In 2016 the Health Resources and Services Administration (HRSA) further embedded the expectation by adding SOGI fields to the Uniform Data System (UDS) reporting obligations for all federally qualified health centers. The combination of coalition pressure and incentive-linked certification created powerful compliance incentives for both vendors and health systems, because nothing motivates hospitals quite like the threat of lost federal dollars for failing to ask patients about their feelings. It's a clear, breathtaking case of policy winning over ethics in the medical field.
EXPANSION WITHIN
Inside Epic, Campbell’s initial workgroup scaled into a 25-person “Volunteer Army.” The team performed a full-system audit and remapped hundreds of references to the original “sex” field throughout patient headers, laboratory normal ranges, genetic pedigrees, clinical decision-support logic, and other modules. Campbell characterized the overhaul as “like the Y2K of the health record.” Development milestones followed in rapid succession: a two-item gender identity update released to clinical customers in June 2016, followed by the complete SOGI SmartForm in November 2016. The SmartForm is a guided questionnaire triggered by clicking the gender or age line in the patient Storyboard or during registration, nursing assessment, or clinical encounters. It begins by recording gender identity; any mismatch with recorded sex automatically prompts follow-up questions on pronouns (including they/them and additional options), transition steps, and an organ inventory that distinguishes organs present at birth from those present currently, because the most reliable way to practice “precision medicine” is apparently to ask patients what their body parts used to be while politely ignoring what they actually are. This also serves as proof of the linguistic weaponization trans activists indulge in - conflating legitimate things like kidney donation with calling an inverted penis lined with scrotal skin a vagina. It's part of the tactic to normalize grotesque and experimental "transgender surgeries" as "just routine medical procedures".
Further refinements to the EPIC EHR in 2017–2018 introduced explicit distinctions among legal sex, gender identity, sex assigned at birth, and “sex for clinical use,” while chosen names and pronouns were propagated system-wide via SmartLinks. By mid-2017 Campbell reported that 10–20 percent of Epic customers had activated the updates. The captured data is structured rather than free-text, making it visible and actionable: chosen name, gender identity, and pronouns appear in patient banners and headers; SmartLinks automatically insert the information into notes, schedules, faxes, and reports. Patients, including minors as young as 12 in many implementations, can enter or update these fields directly through the MyChart portal; changes become part of the official record without mandatory clinical verification, because self-ID is apparently so infallible that no second opinion from a doctor is required. Hospitals frequently incorporate SmartForm completion rates into quality metrics, disparity dashboards, and DEI scorecards, and staff training modules draw heavily on Fenway’s cultural-competence materials.
Campbell has explained the design rationale in public remarks. In 2017 she stated: “Our goal is that patients get the right and appropriate treatment no matter who they are.” On the decision for universal collection she added: “I think that starting to collect this information from everyone will normalize it in many people’s eyes. It’s not that we’re asking certain people whether they happen to be trans, we’re just asking everybody.”
The trans activism is ever present, presented dishonestly. In the August 31, 2022, Clinical Architecture Informonster Podcast (Episode 23: “Discussing Gender Harmony”), recorded with Fenway’s Chris Grasso, Campbell explained that the original single field “had become overloaded and was asked to do double duty.” She described the 2017 safety corrections, such as revised creatinine-clearance calculations based on mismatched legal sex, and noted broader applicability: “The work that we’re doing here will benefit the entire patient community… It’s not just transgender patients who want to be called by a name that’s different than the name on their birth certificate.” Regarding documentation she advised: “If a patient isn’t living their gender identity, don’t document that information in those fields… the system will take your word for it and will put that everywhere.” Right, all that confusion and hoop-jumping due to the religious and fanatical belief in "gender identity", trying to get ahead of the chaos being caused. Epic continues to participate in the HL7 Gender Harmony Project, which has produced a national interoperability standard separating recorded sex/gender, gender identity, and “sex for clinical use,” each with validity periods. The SOGI and organ-inventory data therefore support anatomy-based alerts while preserving identity fields as the primary display element, because the clearest way to avoid clinical confusion is apparently to make identity the banner headline and biology the optional footnote. Gender ideologues purposely calculate to supercede the practice of ethical medicine to bolster their claims, reality be damned.
TARGETING MINORS IS NOT ACCIDENTAL
MyChart proxy access for minors remains configurable by each health system and is age-tiered. Common configurations include independent portal access at age 12 (UF Health Shands), “Teen Plus” limited parental views (Wellstar), and parent-teen access at age 13 (UNC). "Sensitive sections" like SOGI data, preferred pronouns, organ inventory, and transition-related notes, CAN BE HIDDEN FROM PARENTS, frequently extending beyond the original intent of adolescent privacy statutes written for STIs or contraception. A 2025 Do No Harm @donoharm report catalogued these settings and quoted Epic’s own documentation, which states that proxy access “changes as they get older” according to each organization’s interpretation of privacy laws. Vague enough. The cumulative architecture produces a workflow in which gender-identity documentation is routine, frictionless, and self-reinforcing, marketed to the very young and old alike.
DECLINES TO ANSWER
If elderly patients are confused about "personal pronouns", they are marked as "Declined to answer" in a prominent manner in their profiles that anyone opening their chart can see. I have seen this happen to patients with dementia! This phrasing of "refused to cooperate" is meant to create bias in the minds of the clinician that the patient is difficult, and try to force compliance with gender ideology in both the doctor and the patient. Clinicians encounter prompts in core interfaces, data auto-propagates across the record and external systems, and non-use of the features can register as incomplete documentation or failure to meet incentive or equity metrics. These dubious metrics have converted advocacy goals into certification requirements. The outcome is a dominant EHR platform that has embedded self-identified gender identity as a core element across millions of patient records, completely ignoring evidence-based safeguards.
PATIENT SAFETY CONCERNS, THE ULTIMATE EPIC FAIL
Even in electronic health record systems where biologic sex, legal sex, and gender identity are all separately and clearly documented, significant patient-safety concerns remain because downstream clinical systems frequently fail to operationalize those distinctions consistently. Multiple health systems and informatics groups have documented that laboratory software, radiology workflows, preventive screening algorithms, insurance systems, and clinical decision-support tools often still rely on a single operative sex variable despite more sophisticated chart architecture.
At Geisinger Health System, clinicians and informatics staff described needing extensive custom modifications to Epic because standard workflows could not reliably coordinate birth sex, organ inventory, hormone exposure, and preventive screening logic simultaneously. The Veterans Health Administration similarly acknowledged tension between visibility of natal sex and identity-related workflows, warning that suppressing or obscuring biologic sex could impair preventive care and emergency clinical reasoning.
Real-world failures described in the literature include biologically female patients losing automated cervical cancer reminders after administrative sex changes, insurance denials for Pap smears or PSA testing when legal sex conflicted with anatomy, pregnancy-related safeguards failing because workflows operationalized identity-facing fields incorrectly, and laboratory systems inconsistently applying sex-based reference ranges for hemoglobin, creatinine, eGFR, CK, and troponin. Pathologists and laboratorians have repeatedly noted that current systems struggle to interpret altered hormone states because a testosterone-treated female remains biologically female while exhibiting partial shifts in selected analytes, creating ambiguity that simplistic identity-based categorization cannot safely resolve.
Researchers in medical AI and informatics have additionally warned that inconsistent handling of sex, gender identity, legal sex, and hormone exposure produces “sex/gender slippage” in datasets, threatening the reliability of epidemiology, predictive algorithms, and machine-learning models. The central concern raised by clinicians focused on sex-based medicine is therefore not merely missing data fields, but that medicine remains fundamentally organized around biologic sex while many EHR systems and institutional workflows operationalize sex-related variables inconsistently, creating opportunities for diagnostic error, screening failures, inappropriate clinical decision support, and degraded research quality even when all demographic categories are technically present and clearly separated.
The corruption of Epic EHR demonstrates how gender ideology became medical infrastructure when the right mix of activists, incentives, federal cooperation, and software engineers decided that their unfounded beliefs trump reality, endangering patient healthcare in the process. Your mind and body are both the donor organs and the subsequent profit to the trans industry. An EHR is a tool and repository that helps maintain and improve medical records. Using it to cement the nebulous concept of gender identity as fact is subjecting the material reality of patients and doctors to dangerous process errors and repeated trans industry indoctrination. Get your act together, EPIC, and put patient safety first, before it's too late.
SOURCES AND REFERENCES
- Ingraham N, et al. Overcoming technical and cultural challenges to delivering equitable care for LGBTQ individuals in a rural, underserved area. JAMIA Open. 2022.
PMC article
- Klee A, et al. Evolving Sex and Gender in Electronic Health Records. Fed Pract. 2018.
PMC article
- Greene DN, et al. Challenges in Transgender Healthcare: The Pathology Perspective. Clin Chem. 2016.
PMC article
- Cheung AS, et al. Approach to Interpreting Common Laboratory Pathology Tests in Transgender Individuals. J Clin Endocrinol Metab. 2021.
Oxford Academic article
- Keyes O, et al. Sex trouble: Sex/gender slippage, sex confusion, and sex obsession in machine learning using electronic health records. Patterns. 2022.
ScienceDirect article
- Kannan V, et al. Challenges with Accuracy of Gender Fields in Identifying Transgender Patients in Electronic Health Records. AMIA Annu Symp Proc. 2020.
PMC article
- Collecting Sexual Orientation and Gender Identity Data in Electronic Health Records. National Academies Press.
NCBI Bookshelf
- Wired.com, “The Battle to Get Gender Identity Into Your Health Records” (June 30, 2017) – Campbell’s timeline, internal presentation quote, 2012 wiki proposal, workgroup formation, 2013 SOGI Strategy handbook, Volunteer Army audit, Y2K comparison, and technical rollout details.
- Isthmus.com, “UW Health aims to be more sensitive to gender identity” (July 6, 2017) – Campbell’s direct quotes on the SmartForm purpose, normalization through universal collection, and adoption statistics (10–20% of customers, 20–40 providers).
- Clinical Architecture Informonster Podcast, Episode 23: “Discussing Gender Harmony” (August 31, 2022) – Full transcript excerpts of Campbell discussing the overloaded single sex field, 2017 clinical safety fixes, HL7 Gender Harmony collaboration, privacy advice, and benefits for all patients; includes joint discussion with Fenway’s Chris Grasso.
- Do No Harm report, “Parental Access to Children’s Medical Records” (October 2025) – Details on Epic SOGI SmartForm mechanics, organ inventory, MyChart proxy access configurations at specific health systems (UF Health Shands, Wellstar, UNC), and analysis of concealment practices beyond legal minimums.
- Fenway Health / National LGBTQIA Health Education Center, “Collecting Sexual Orientation and Gender Identity (SO/GI) Data in Electronic Health Records” (2016 PDF) – Implementation toolkits, clinical workflows, and ties to Meaningful Use / HRSA requirements.
- Cahill et al., “Sexual Orientation and Gender Identity Data Collection in Clinical Settings and in Electronic Health Records: A Key to Ending LGBT Health Disparities” (PLoS One, 2014) – Core advocacy paper outlining the case for SOGI inclusion.
- Fenway Health, “How to Gather Data on Sexual Orientation and Gender Identity in Clinical Settings” (policy brief, ~2012) – Early testing protocols and two-step question recommendations.
- Center for American Progress / Fenway Institute joint statement (October 7, 2015) – Praise for the 2015 ONC/CMS Meaningful Use rules requiring SOGI capacity in certified EHRs.
- Fenway Health “Do Ask, Do Tell” toolkit and related 2014–2016 publications – Broader SOGI EHR advocacy, promotion of standardized questions, and collaboration with other groups.
ONC/CMS 2015 Edition Certified EHR Technology (CEHRT) Criteria and Meaningful Use/Promoting Interoperability final rules – Federal requirements for SOGI data capacity in certified systems, tied to incentive payments.
- Additional cross-referenced context from HRSA Uniform Data System (UDS) updates (2016), HL7 Gender Harmony Project documentation, and public Epic customer implementation examples (e.g., University of Wisconsin, Geisinger). All information is drawn exclusively from publicly available records as of 2025.
- Cahill S. “Sexual Orientation and Gender Identity Data Collection Update: U.S. Government Takes Steps to Promote Sexual Orientation and Gender Identity Data Collection Through Meaningful Use Guidelines.” LGBT Health (2014/2016 update) – Details on the 153 LGBT and HIV groups’ 2014 recommendations to ONC for SNOMED codes and the 2013 public comment from 145 organizations.
- Cahill S, Makadon H. Related policy briefs and Fenway Institute publications (2012–2016) – Documentation of coalition advocacy, two-step questions, and EHR implementation guidance.
#sexnotgender #genderidentity #epicEHR #epic #epicfail #ehr #medicalethics #MedTwitter #MEDX #donoharm #safety #propaganda
3
1
5
177
Travis Morrell, MD MPH retweeted

Jun 12
電子カルテの性的指向性自認(SOGI)項目は、医療現場の要請じゃなくて「アドボカシー団体+連邦政府+電子カルテ最大手メーカー(EPIC社)」で作られた政策誘導だったという話
性別(sex)をもとにする医療は全部設定しなおし🫨
未成年者の医療情報を保護者から隠す仕組みも実装🫨

WHEN EPIC ISN'T REALLY EPIC: How Gender Ideology Was Integrated into Epic Systems' Electronic Health Records
Epic Systems Corporation’s electronic health record (EHR) platform, used by approximately 41% of 🇺🇸 hospitals and historically as many as 80% of outpatient settings, as well as internationally, has systematically incorporated structured fields for self-identified gender identity that are separate from, and often displayed more prominently than, biological sex. The integration happened through a deliberate sequence of internal technical development at Epic, coordinated external advocacy from trans industry organizations, and federal regulatory requirements tied to incentive payments. The result is the Sexual Orientation and Gender Identity (SOGI) SmartForm, (sex) organ inventory tracking, visible patient banners and headers, automated SmartLinks, and configurable MyChart proxy access settings. These features treat gender identity as core, structured, queryable data embedded throughout clinical workflows, notes, portals, faxes, research queries, and national interoperability standards. To gender identity believers, nothing says “evidence-based medicine” quite like elevating subjective self-report to the level of immutable biology.
HOW IT STARTED
The internal catalyst at Epic was Janet Campbell, who joined the company in 2003 immediately after graduating from Carleton College with a computer science degree and additional coursework in gender studies. But, of course. Her first assigned project required building system rules to restrict diagnostic and billing codes according to recorded patient sex, for example, blocking orders for cervical examinations on patients whose record listed “male.” This work quickly revealed that Epic’s longstanding single “sex” field, limited since the company’s founding in 1979 to the options male, female, or unknown, was functionally "overloaded", as per Janet Campbell. It was seen to be simultaneously serving as a proxy for real sex or "sex assigned at birth", legal sex, and the emerging activist concept of gender identity. The resulting mismatches produced billing errors, inappropriate clinical alerts, and unreliable data for research or quality reporting, problems that, in a less ideological era, might have been solved by simply respecting biological reality rather than inventing new fields to accommodate delusuins.
In approximately 2004–2005, Campbell volunteered to deliver an internal educational presentation during Epic’s regular workplace talk series. One slide stated verbatim: “Epic is almost completely unable to deal with this level of complexity, and neither is the medical profession, for that matter.” Sure, Jan. By January 2012 she had posted an internal wiki page proposing a two- or three-step data-capture sequence: sex assigned at birth, legal sex, and gender identity. A cross-functional workgroup was assembled that included several "transgender" and "non-binary" Epic employees - its stated purpose was to assist customers with implementation. In 2013 the group produced and distributed a “SOGI Strategy” handbook that supplied both technical instructions and sections on "transgender cultural competence" and the distinction between identity and sex, helpfully ensuring that every hospital using the system received a gentle primer on why feelings should sometimes trump chromosomes.
INFLUENCE OF THE TRANS INDUSTRY
The external pressure that accelerated these changes came from a sustained advocacy campaign. The coalition involved represented a wide network of LGBT health, HIV advocacy, and related organizations, with prominent leadership from The Fenway Institute at Fenway Health. In January 2013 this coalition of 145 leading LGBT and HIV/AIDS organizations submitted a formal public comment to the Office of the National Coordinator for Health Information Technology (ONC) urging inclusion of sexual orientation and gender identity (SOGI) data collection in Meaningful Use guidelines. Early in 2014 the same network expanded to 153 organizations and submitted recommendations asking ONC to direct the National Library of Medicine to develop new SNOMED code sets specifically to support accurate and effective SO/GI data collection in certified EHRs. These submissions formed part of a broader effort to embed SOGI capacity within the proposed 2015 Edition Certified EHR Technology (CEHRT) criteria for Meaningful Use Stage 3. Because when biology proves stubborn, the next best step is apparently to lobby the government to reprogram the nation’s medical software. Fenway Health, operating through its Fenway Institute and National LGBTQIA Health Education Center, functioned as the central technical and policy coordinator.
As early as 2011, Fenway had begun testing two-step gender identity questions (gender identity asked first, followed by sex assigned at birth) at its own federally qualified health center. In roughly 2012 it published the policy brief “How to Gather Data on Sexual Orientation and Gender Identity in Clinical Settings,” which formalized the two-step approach originally developed by the Philadelphia Transgender Health Advocacy Coalition in 1997 and later endorsed by UCSF’s Center of Excellence for Transgender Health. Fenway partnered with the Center for American Progress on the “Do Ask, Do Tell” project, releasing online toolkits explicitly aimed at EHR vendors and providers. In 2014 Sean Cahill, PhD (Director of Health Policy Research at the Fenway Institute) co-authored key papers and policy statements, including the PLoS One article “Sexual Orientation and Gender Identity Data Collection in Clinical Settings and in Electronic Health Records: A Key to Ending LGBT Health Disparities,” which framed SOGI collection as essential for equity and disparity reduction. Fenway supplemented these writings with slide decks, tip sheets, and formal regulatory comments that repeatedly positioned SOGI capacity as a NON-NEGOTIABLE REQUIREMENT FOR FEDERAL CERTIFICATION 🚩, turning a contested religious belief at best into a certification checkbox.
IT'S ALWAYS THE GOVERNMENT
These advocacy efforts aligned precisely with federal rulemaking. The 2015 ONC and Centers for Medicare & Medicaid Services (CMS) Meaningful Use/Promoting Interoperability final rules mandated that certified EHRs possess the technical capacity to record, store, change, and retrieve structured SOGI data in order to qualify for incentive payments. The requirement applied across approximately 78 percent of outpatient clinics by 2018. In 2016 the Health Resources and Services Administration (HRSA) further embedded the expectation by adding SOGI fields to the Uniform Data System (UDS) reporting obligations for all federally qualified health centers. The combination of coalition pressure and incentive-linked certification created powerful compliance incentives for both vendors and health systems, because nothing motivates hospitals quite like the threat of lost federal dollars for failing to ask patients about their feelings. It's a clear, breathtaking case of policy winning over ethics in the medical field.
EXPANSION WITHIN
Inside Epic, Campbell’s initial workgroup scaled into a 25-person “Volunteer Army.” The team performed a full-system audit and remapped hundreds of references to the original “sex” field throughout patient headers, laboratory normal ranges, genetic pedigrees, clinical decision-support logic, and other modules. Campbell characterized the overhaul as “like the Y2K of the health record.” Development milestones followed in rapid succession: a two-item gender identity update released to clinical customers in June 2016, followed by the complete SOGI SmartForm in November 2016. The SmartForm is a guided questionnaire triggered by clicking the gender or age line in the patient Storyboard or during registration, nursing assessment, or clinical encounters. It begins by recording gender identity; any mismatch with recorded sex automatically prompts follow-up questions on pronouns (including they/them and additional options), transition steps, and an organ inventory that distinguishes organs present at birth from those present currently, because the most reliable way to practice “precision medicine” is apparently to ask patients what their body parts used to be while politely ignoring what they actually are. This also serves as proof of the linguistic weaponization trans activists indulge in - conflating legitimate things like kidney donation with calling an inverted penis lined with scrotal skin a vagina. It's part of the tactic to normalize grotesque and experimental "transgender surgeries" as "just routine medical procedures".
Further refinements to the EPIC EHR in 2017–2018 introduced explicit distinctions among legal sex, gender identity, sex assigned at birth, and “sex for clinical use,” while chosen names and pronouns were propagated system-wide via SmartLinks. By mid-2017 Campbell reported that 10–20 percent of Epic customers had activated the updates. The captured data is structured rather than free-text, making it visible and actionable: chosen name, gender identity, and pronouns appear in patient banners and headers; SmartLinks automatically insert the information into notes, schedules, faxes, and reports. Patients, including minors as young as 12 in many implementations, can enter or update these fields directly through the MyChart portal; changes become part of the official record without mandatory clinical verification, because self-ID is apparently so infallible that no second opinion from a doctor is required. Hospitals frequently incorporate SmartForm completion rates into quality metrics, disparity dashboards, and DEI scorecards, and staff training modules draw heavily on Fenway’s cultural-competence materials.
Campbell has explained the design rationale in public remarks. In 2017 she stated: “Our goal is that patients get the right and appropriate treatment no matter who they are.” On the decision for universal collection she added: “I think that starting to collect this information from everyone will normalize it in many people’s eyes. It’s not that we’re asking certain people whether they happen to be trans, we’re just asking everybody.”
The trans activism is ever present, presented dishonestly. In the August 31, 2022, Clinical Architecture Informonster Podcast (Episode 23: “Discussing Gender Harmony”), recorded with Fenway’s Chris Grasso, Campbell explained that the original single field “had become overloaded and was asked to do double duty.” She described the 2017 safety corrections, such as revised creatinine-clearance calculations based on mismatched legal sex, and noted broader applicability: “The work that we’re doing here will benefit the entire patient community… It’s not just transgender patients who want to be called by a name that’s different than the name on their birth certificate.” Regarding documentation she advised: “If a patient isn’t living their gender identity, don’t document that information in those fields… the system will take your word for it and will put that everywhere.” Right, all that confusion and hoop-jumping due to the religious and fanatical belief in "gender identity", trying to get ahead of the chaos being caused. Epic continues to participate in the HL7 Gender Harmony Project, which has produced a national interoperability standard separating recorded sex/gender, gender identity, and “sex for clinical use,” each with validity periods. The SOGI and organ-inventory data therefore support anatomy-based alerts while preserving identity fields as the primary display element, because the clearest way to avoid clinical confusion is apparently to make identity the banner headline and biology the optional footnote. Gender ideologues purposely calculate to supercede the practice of ethical medicine to bolster their claims, reality be damned.
TARGETING MINORS IS NOT ACCIDENTAL
MyChart proxy access for minors remains configurable by each health system and is age-tiered. Common configurations include independent portal access at age 12 (UF Health Shands), “Teen Plus” limited parental views (Wellstar), and parent-teen access at age 13 (UNC). "Sensitive sections" like SOGI data, preferred pronouns, organ inventory, and transition-related notes, CAN BE HIDDEN FROM PARENTS, frequently extending beyond the original intent of adolescent privacy statutes written for STIs or contraception. A 2025 Do No Harm @donoharm report catalogued these settings and quoted Epic’s own documentation, which states that proxy access “changes as they get older” according to each organization’s interpretation of privacy laws. Vague enough. The cumulative architecture produces a workflow in which gender-identity documentation is routine, frictionless, and self-reinforcing, marketed to the very young and old alike.
DECLINES TO ANSWER
If elderly patients are confused about "personal pronouns", they are marked as "Declined to answer" in a prominent manner in their profiles that anyone opening their chart can see. I have seen this happen to patients with dementia! This phrasing of "refused to cooperate" is meant to create bias in the minds of the clinician that the patient is difficult, and try to force compliance with gender ideology in both the doctor and the patient. Clinicians encounter prompts in core interfaces, data auto-propagates across the record and external systems, and non-use of the features can register as incomplete documentation or failure to meet incentive or equity metrics. These dubious metrics have converted advocacy goals into certification requirements. The outcome is a dominant EHR platform that has embedded self-identified gender identity as a core element across millions of patient records, completely ignoring evidence-based safeguards.
PATIENT SAFETY CONCERNS, THE ULTIMATE EPIC FAIL
Even in electronic health record systems where biologic sex, legal sex, and gender identity are all separately and clearly documented, significant patient-safety concerns remain because downstream clinical systems frequently fail to operationalize those distinctions consistently. Multiple health systems and informatics groups have documented that laboratory software, radiology workflows, preventive screening algorithms, insurance systems, and clinical decision-support tools often still rely on a single operative sex variable despite more sophisticated chart architecture.
At Geisinger Health System, clinicians and informatics staff described needing extensive custom modifications to Epic because standard workflows could not reliably coordinate birth sex, organ inventory, hormone exposure, and preventive screening logic simultaneously. The Veterans Health Administration similarly acknowledged tension between visibility of natal sex and identity-related workflows, warning that suppressing or obscuring biologic sex could impair preventive care and emergency clinical reasoning.
Real-world failures described in the literature include biologically female patients losing automated cervical cancer reminders after administrative sex changes, insurance denials for Pap smears or PSA testing when legal sex conflicted with anatomy, pregnancy-related safeguards failing because workflows operationalized identity-facing fields incorrectly, and laboratory systems inconsistently applying sex-based reference ranges for hemoglobin, creatinine, eGFR, CK, and troponin. Pathologists and laboratorians have repeatedly noted that current systems struggle to interpret altered hormone states because a testosterone-treated female remains biologically female while exhibiting partial shifts in selected analytes, creating ambiguity that simplistic identity-based categorization cannot safely resolve.
Researchers in medical AI and informatics have additionally warned that inconsistent handling of sex, gender identity, legal sex, and hormone exposure produces “sex/gender slippage” in datasets, threatening the reliability of epidemiology, predictive algorithms, and machine-learning models. The central concern raised by clinicians focused on sex-based medicine is therefore not merely missing data fields, but that medicine remains fundamentally organized around biologic sex while many EHR systems and institutional workflows operationalize sex-related variables inconsistently, creating opportunities for diagnostic error, screening failures, inappropriate clinical decision support, and degraded research quality even when all demographic categories are technically present and clearly separated.
The corruption of Epic EHR demonstrates how gender ideology became medical infrastructure when the right mix of activists, incentives, federal cooperation, and software engineers decided that their unfounded beliefs trump reality, endangering patient healthcare in the process. Your mind and body are both the donor organs and the subsequent profit to the trans industry. An EHR is a tool and repository that helps maintain and improve medical records. Using it to cement the nebulous concept of gender identity as fact is subjecting the material reality of patients and doctors to dangerous process errors and repeated trans industry indoctrination. Get your act together, EPIC, and put patient safety first, before it's too late.
SOURCES AND REFERENCES
- Ingraham N, et al. Overcoming technical and cultural challenges to delivering equitable care for LGBTQ individuals in a rural, underserved area. JAMIA Open. 2022.
PMC article
- Klee A, et al. Evolving Sex and Gender in Electronic Health Records. Fed Pract. 2018.
PMC article
- Greene DN, et al. Challenges in Transgender Healthcare: The Pathology Perspective. Clin Chem. 2016.
PMC article
- Cheung AS, et al. Approach to Interpreting Common Laboratory Pathology Tests in Transgender Individuals. J Clin Endocrinol Metab. 2021.
Oxford Academic article
- Keyes O, et al. Sex trouble: Sex/gender slippage, sex confusion, and sex obsession in machine learning using electronic health records. Patterns. 2022.
ScienceDirect article
- Kannan V, et al. Challenges with Accuracy of Gender Fields in Identifying Transgender Patients in Electronic Health Records. AMIA Annu Symp Proc. 2020.
PMC article
- Collecting Sexual Orientation and Gender Identity Data in Electronic Health Records. National Academies Press.
NCBI Bookshelf
- Wired.com, “The Battle to Get Gender Identity Into Your Health Records” (June 30, 2017) – Campbell’s timeline, internal presentation quote, 2012 wiki proposal, workgroup formation, 2013 SOGI Strategy handbook, Volunteer Army audit, Y2K comparison, and technical rollout details.
- Isthmus.com, “UW Health aims to be more sensitive to gender identity” (July 6, 2017) – Campbell’s direct quotes on the SmartForm purpose, normalization through universal collection, and adoption statistics (10–20% of customers, 20–40 providers).
- Clinical Architecture Informonster Podcast, Episode 23: “Discussing Gender Harmony” (August 31, 2022) – Full transcript excerpts of Campbell discussing the overloaded single sex field, 2017 clinical safety fixes, HL7 Gender Harmony collaboration, privacy advice, and benefits for all patients; includes joint discussion with Fenway’s Chris Grasso.
- Do No Harm report, “Parental Access to Children’s Medical Records” (October 2025) – Details on Epic SOGI SmartForm mechanics, organ inventory, MyChart proxy access configurations at specific health systems (UF Health Shands, Wellstar, UNC), and analysis of concealment practices beyond legal minimums.
- Fenway Health / National LGBTQIA Health Education Center, “Collecting Sexual Orientation and Gender Identity (SO/GI) Data in Electronic Health Records” (2016 PDF) – Implementation toolkits, clinical workflows, and ties to Meaningful Use / HRSA requirements.
- Cahill et al., “Sexual Orientation and Gender Identity Data Collection in Clinical Settings and in Electronic Health Records: A Key to Ending LGBT Health Disparities” (PLoS One, 2014) – Core advocacy paper outlining the case for SOGI inclusion.
- Fenway Health, “How to Gather Data on Sexual Orientation and Gender Identity in Clinical Settings” (policy brief, ~2012) – Early testing protocols and two-step question recommendations.
- Center for American Progress / Fenway Institute joint statement (October 7, 2015) – Praise for the 2015 ONC/CMS Meaningful Use rules requiring SOGI capacity in certified EHRs.
- Fenway Health “Do Ask, Do Tell” toolkit and related 2014–2016 publications – Broader SOGI EHR advocacy, promotion of standardized questions, and collaboration with other groups.
ONC/CMS 2015 Edition Certified EHR Technology (CEHRT) Criteria and Meaningful Use/Promoting Interoperability final rules – Federal requirements for SOGI data capacity in certified systems, tied to incentive payments.
- Additional cross-referenced context from HRSA Uniform Data System (UDS) updates (2016), HL7 Gender Harmony Project documentation, and public Epic customer implementation examples (e.g., University of Wisconsin, Geisinger). All information is drawn exclusively from publicly available records as of 2025.
- Cahill S. “Sexual Orientation and Gender Identity Data Collection Update: U.S. Government Takes Steps to Promote Sexual Orientation and Gender Identity Data Collection Through Meaningful Use Guidelines.” LGBT Health (2014/2016 update) – Details on the 153 LGBT and HIV groups’ 2014 recommendations to ONC for SNOMED codes and the 2013 public comment from 145 organizations.
- Cahill S, Makadon H. Related policy briefs and Fenway Institute publications (2012–2016) – Documentation of coalition advocacy, two-step questions, and EHR implementation guidance.
#sexnotgender #genderidentity #epicEHR #epic #epicfail #ehr #medicalethics #MedTwitter #MEDX #donoharm #safety #propaganda
1
11
27
1,522

Jack Turban says two years of follow up—where 5% of youth already de-identify as “trans”—is great science.
@ColoradoDoctors says: selection bias, short follow up—this is a joke.
Our empathy for gender-distressed kids should be guided by EVIDENCE. This isn’t it.
The study being promoted by trans activist clinician Jack Turban in question is: "Stability of Transgender Identity in Adolescents Seen in Multidisciplinary Specialized Gender Centers: A Multicenter Study in Canada" by Daniel L. Metzger et al. (including Arati Mokashi, Danièle Pacaud, Margaret L. Lawson, and others). It was published online on June 3, 2026, in the Journal of Adolescent Health.
This was a retrospective chart review of 445 adolescents (mean age at first clinic visit: 15.3 years; 74.4% female, 25.6% male) referred to four Canadian pediatric endocrinology gender clinics between 2012 and 2017. All met DSM-5 criteria for "gender dysphoria", received biopsychosocial assessment per WPATH/Endocrine Society guidelines, and had at least 1 year of follow-up after their first clinic visit (median follow-up: 2.4 years, IQR 1.1–7.2 years). Data were extracted from charts in 2018–2020.Key reported results:421/445 (94.6%; 95% CI 92.1–96.3%) continued with their presenting gender identity or reidentified as non-binary per chart notes.
24/445 (5.4%) changed identity; only 13/445 (2.9%) reverted to a binary identity aligned with birth sex. How do you revert a mastectomy?
353/445 (79.3%) started gender-affirming hormones (GAH); 4/353 (1.1%, all females) discontinued them.
Gonadotropin suppression/adjunctive therapy started in 299/445 (67.2%); discontinued in 35/299 (11.7%), with some discontinuations linked to identity change.
Overall, 97.1% continued identifying with a gender "not typically aligned with their birth sex" per records.
The authors, like trans activist psychiatrist Jack Turban here, conclude that discontinuation of hormones was rare and most continued a non-birth-sex-aligned identity in this cohort.
As skeptics of gender ideology (the view that gender identity is an innate, immutable, binary-opposite essence best affirmed via social/medical transition), we are right to scrutinize claims of high "stability" from short-term clinic data. Let's see if the methodology used in this paper holds up to rigorous scientific standards 🔽
1. Selection Bias (Sampling/Referral Bias)
The cohort was not representative of "gender dysphoric" youth. It included only those:
- referred to specialized affirmative-model clinics
- had parental consent
- who pursued or were considered for medical interventions (GST/GAH).
- who had ≥1 year of documented follow-up in the system.
This systematically excludes desisters who never sought care, those without family support, those who dropped out early, or those resolved via watchful waiting/exploratory approaches. Clinics following WPATH guidelines tend to attract more socially transitioned or committed cases. The result is OVERESTIMATION of persistence. Classic selection bias inflates apparent stability because the sample is conditioned on engagement with the affirming pathway.
2. Extremely SHORT Follow-Up and Inadequate Temporal Scope
Median 4 years is too brief for assessing identity "stability" in adolescents whose brains and identities are still developing into the mid-20s. Many participants were still minors or young adults at last chart entry. Desistance, regret, or identity shifts (including post-hormone) often emerge later.
Contrast with other data:
German insurance claims data (large population-based): >60% of youth with gender identity disorder diagnosis no longer carried it after 5 years (persistence ~36% overall; lower in adolescent females).
Historical studies of childhood-onset gender dysphoria (pre-social transition era): Desistance rates often 60–90% by adulthood.
Emerging detransition literature notes that time to detransition frequently exceeds 3–5 years; short clinic follow-up misses those who leave the system.
The study cannot rule out later changes
3. Information/MEASUREMENT BIAS and Poor Outcome Reliability
Identity "change" or persistence was determined solely from chart documentation of self/parent-reported identity at visits, not standardized, validated, blinded, or prospective instruments (e.g., no repeated structured interviews or independent assessors). Charts in affirmative clinics may reflect clinician expectations, social reinforcement, or reluctance to document doubt. Counting "reidentified as non-binary" as "continued" persistence is questionable; non-binary identification is often fluid and can represent a phase or social influence. It simply has no meaning in the real world.
No data is presented on how often identity was actively explored vs. affirmed. With states like Colorado and California passing laws to enable people to sue therapists and psychiatrists for not affirming "gender identity", and therapists explicitly describing pressure to affirm, it's safe to assume a wait and watch approach was not the norm.
Hormone discontinuation (1.1%) is narrowly defined and undercounts true detransition (many stop without notifying the original clinic or changing records officially).
Retrospective chart review is prone to incomplete or biased recording (information bias).
4. NO CONTROLS/Comparison Group and Uncontrolled Confounding
There was no untreated comparator, waitlist control, or exploratory-therapy arm.
You cannot separate:
- Natural course of identity
- Effects of social transition/affirmation
- Peer/social media influence (rapid-onset patterns rose sharply around/after this cohort's era)
- COMORBIDITIES (autism, trauma, mental health issues are common in gender dysphoria referrals, but not quantified here as predictors of outcome)
- No indication of how many of these children experienced same-sex attraction (no account of homosexuality)
The study mentions coexisting conditions were "addressed concurrently" but provides no breakdown or adjustment. Affirmative environments may reinforce identity via iatrogenic effects or sunk-cost dynamics once medical steps begin.
5. LIMITED GENERALIZABILITY and Contextual Issues
This study was specific to four Canadian clinics using affirmative/WPATH protocols in 2012–2017 (pre-peak referral surge and pre-Cass Review)
High female proportion reflects recent demographic shifts, not timeless biology.
Results may not apply to non-clinic populations, different cultures, or post-Cass/European cautionary approaches (UK, Sweden, Finland, Norway restricted youth medicalization citing weak evidence overall)
The Cass Review highlighted low-quality evidence across similar studies for benefits and persistence claims.
6. Other Methodological Limitations:
Retrospective design: Cannot establish temporality or causality; prone to recall/imputation bias (onset age imputed for ~27% of cases).
Descriptive statistics only: No advanced modeling of time-to-event, predictors of change, or adjustment for confounders.
Narrow "detransition" definition: Focuses on identity shift or hormone stop in charts; ignores broader regret, sexual/fertility impacts, or those lost to adult care.
No long-term physical/mental health outcomes (bone density, cardiovascular, fertility, suicidality post-intervention).
Field-wide issues: Gender medicine has faced criticism for publication bias, low-evidence standards, and ideological capture (per independent reviews like Cass). Jack Turban himself is not a neutral party, but someone who firmly advocates for "gender-affirming healthcare" against evidence which has caused most countries to pause these for minors.
BOTTOM LINE: This study shows that, in this highly selected short-term clinic cohort under an affirmative model, most documented identities did not revert per charts, and hormone discontinuation was low. However, its design (selection bias, short follow-up, subjective charting, no controls, narrow outcomes) severely limits causal claims about innate/immutable identity or the necessity/safety of early medicalization. It does not refute historical desistance data, population-level non-persistence findings, or concerns about social influence and exploratory care. Stronger evidence would require prospective, controlled, long-term studies with standardized assessments, minimal loss to follow-up, and comparison arms, standards largely unmet in this field to date. For broader context, the Cass Review (UK) and shifts in several European countries emphasize the weak evidence base for routine affirmation in youth and the importance of addressing comorbidities first.
This study will, of course, be cited endlessly by trans activists, dubious NGOs funded by opaque means, and "gender-affirming" providers who make bank off the nebulous concept of "gender identity", ignoring the poor quality and evident biases present even with a cursory glance. We urge those with a scientific bent to look closely into the authors and understand the conflict of interest.
7
8
40
1,317
Travis Morrell, MD MPH retweeted
The study being promoted by trans activist clinician Jack Turban in question is: "Stability of Transgender Identity in Adolescents Seen in Multidisciplinary Specialized Gender Centers: A Multicenter Study in Canada" by Daniel L. Metzger et al. (including Arati Mokashi, Danièle Pacaud, Margaret L. Lawson, and others). It was published online on June 3, 2026, in the Journal of Adolescent Health.
This was a retrospective chart review of 445 adolescents (mean age at first clinic visit: 15.3 years; 74.4% female, 25.6% male) referred to four Canadian pediatric endocrinology gender clinics between 2012 and 2017. All met DSM-5 criteria for "gender dysphoria", received biopsychosocial assessment per WPATH/Endocrine Society guidelines, and had at least 1 year of follow-up after their first clinic visit (median follow-up: 2.4 years, IQR 1.1–7.2 years). Data were extracted from charts in 2018–2020.Key reported results:421/445 (94.6%; 95% CI 92.1–96.3%) continued with their presenting gender identity or reidentified as non-binary per chart notes.
24/445 (5.4%) changed identity; only 13/445 (2.9%) reverted to a binary identity aligned with birth sex. How do you revert a mastectomy?
353/445 (79.3%) started gender-affirming hormones (GAH); 4/353 (1.1%, all females) discontinued them.
Gonadotropin suppression/adjunctive therapy started in 299/445 (67.2%); discontinued in 35/299 (11.7%), with some discontinuations linked to identity change.
Overall, 97.1% continued identifying with a gender "not typically aligned with their birth sex" per records.
The authors, like trans activist psychiatrist Jack Turban here, conclude that discontinuation of hormones was rare and most continued a non-birth-sex-aligned identity in this cohort.
As skeptics of gender ideology (the view that gender identity is an innate, immutable, binary-opposite essence best affirmed via social/medical transition), we are right to scrutinize claims of high "stability" from short-term clinic data. Let's see if the methodology used in this paper holds up to rigorous scientific standards 🔽
1. Selection Bias (Sampling/Referral Bias)
The cohort was not representative of "gender dysphoric" youth. It included only those:
- referred to specialized affirmative-model clinics
- had parental consent
- who pursued or were considered for medical interventions (GST/GAH).
- who had ≥1 year of documented follow-up in the system.
This systematically excludes desisters who never sought care, those without family support, those who dropped out early, or those resolved via watchful waiting/exploratory approaches. Clinics following WPATH guidelines tend to attract more socially transitioned or committed cases. The result is OVERESTIMATION of persistence. Classic selection bias inflates apparent stability because the sample is conditioned on engagement with the affirming pathway.
2. Extremely SHORT Follow-Up and Inadequate Temporal Scope
Median 4 years is too brief for assessing identity "stability" in adolescents whose brains and identities are still developing into the mid-20s. Many participants were still minors or young adults at last chart entry. Desistance, regret, or identity shifts (including post-hormone) often emerge later.
Contrast with other data:
German insurance claims data (large population-based): >60% of youth with gender identity disorder diagnosis no longer carried it after 5 years (persistence ~36% overall; lower in adolescent females).
Historical studies of childhood-onset gender dysphoria (pre-social transition era): Desistance rates often 60–90% by adulthood.
Emerging detransition literature notes that time to detransition frequently exceeds 3–5 years; short clinic follow-up misses those who leave the system.
The study cannot rule out later changes
3. Information/MEASUREMENT BIAS and Poor Outcome Reliability
Identity "change" or persistence was determined solely from chart documentation of self/parent-reported identity at visits, not standardized, validated, blinded, or prospective instruments (e.g., no repeated structured interviews or independent assessors). Charts in affirmative clinics may reflect clinician expectations, social reinforcement, or reluctance to document doubt. Counting "reidentified as non-binary" as "continued" persistence is questionable; non-binary identification is often fluid and can represent a phase or social influence. It simply has no meaning in the real world.
No data is presented on how often identity was actively explored vs. affirmed. With states like Colorado and California passing laws to enable people to sue therapists and psychiatrists for not affirming "gender identity", and therapists explicitly describing pressure to affirm, it's safe to assume a wait and watch approach was not the norm.
Hormone discontinuation (1.1%) is narrowly defined and undercounts true detransition (many stop without notifying the original clinic or changing records officially).
Retrospective chart review is prone to incomplete or biased recording (information bias).
4. NO CONTROLS/Comparison Group and Uncontrolled Confounding
There was no untreated comparator, waitlist control, or exploratory-therapy arm.
You cannot separate:
- Natural course of identity
- Effects of social transition/affirmation
- Peer/social media influence (rapid-onset patterns rose sharply around/after this cohort's era)
- COMORBIDITIES (autism, trauma, mental health issues are common in gender dysphoria referrals, but not quantified here as predictors of outcome)
- No indication of how many of these children experienced same-sex attraction (no account of homosexuality)
The study mentions coexisting conditions were "addressed concurrently" but provides no breakdown or adjustment. Affirmative environments may reinforce identity via iatrogenic effects or sunk-cost dynamics once medical steps begin.
5. LIMITED GENERALIZABILITY and Contextual Issues
This study was specific to four Canadian clinics using affirmative/WPATH protocols in 2012–2017 (pre-peak referral surge and pre-Cass Review)
High female proportion reflects recent demographic shifts, not timeless biology.
Results may not apply to non-clinic populations, different cultures, or post-Cass/European cautionary approaches (UK, Sweden, Finland, Norway restricted youth medicalization citing weak evidence overall)
The Cass Review highlighted low-quality evidence across similar studies for benefits and persistence claims.
6. Other Methodological Limitations:
Retrospective design: Cannot establish temporality or causality; prone to recall/imputation bias (onset age imputed for ~27% of cases).
Descriptive statistics only: No advanced modeling of time-to-event, predictors of change, or adjustment for confounders.
Narrow "detransition" definition: Focuses on identity shift or hormone stop in charts; ignores broader regret, sexual/fertility impacts, or those lost to adult care.
No long-term physical/mental health outcomes (bone density, cardiovascular, fertility, suicidality post-intervention).
Field-wide issues: Gender medicine has faced criticism for publication bias, low-evidence standards, and ideological capture (per independent reviews like Cass). Jack Turban himself is not a neutral party, but someone who firmly advocates for "gender-affirming healthcare" against evidence which has caused most countries to pause these for minors.
BOTTOM LINE: This study shows that, in this highly selected short-term clinic cohort under an affirmative model, most documented identities did not revert per charts, and hormone discontinuation was low. However, its design (selection bias, short follow-up, subjective charting, no controls, narrow outcomes) severely limits causal claims about innate/immutable identity or the necessity/safety of early medicalization. It does not refute historical desistance data, population-level non-persistence findings, or concerns about social influence and exploratory care. Stronger evidence would require prospective, controlled, long-term studies with standardized assessments, minimal loss to follow-up, and comparison arms, standards largely unmet in this field to date. For broader context, the Cass Review (UK) and shifts in several European countries emphasize the weak evidence base for routine affirmation in youth and the importance of addressing comorbidities first.
This study will, of course, be cited endlessly by trans activists, dubious NGOs funded by opaque means, and "gender-affirming" providers who make bank off the nebulous concept of "gender identity", ignoring the poor quality and evident biases present even with a cursory glance. We urge those with a scientific bent to look closely into the authors and understand the conflict of interest.
Jun 11

A new study of 445 adolescents treated at pediatric gender clinics in Canada found that after a mean 2.4 years, 94.6% still identified as trns.
Of the 353 who started hormonal treatments, 1.1% discontinued them.
jahonline.org/article/S1054-…
3
19
35
6,953
Travis Morrell, MD MPH retweeted

Jun 12
I don't think the Cleveland Clinic settlement is the big win some claim. It's like Karmelo Anthony getting probation restitution to the Metcalf family - technically a 'win,' but the punishment doesn't match the scale of the criminality.
To illustrate this point, consider two conflicting statements...
DOJ says fraudulent claims were used to "secure insurance coverage for sex-rejecting procedures on minors," whereas Cleveland Clinic says this was "an unintentional coding issue involving a small number of claims."
These statements are revealing because they represent two vastly different worlds of criminality - one is intentional (i.e. criminal) while the other unintentional (i.e. civil). Although these two allegations, by definition, cannot exist in the same settlement agreement, they can end up being bedfellows when the proper conditions are met.
Those conditions are when DOJ prosecutors let the hospitals off easy. Because for the Cleveland Clinic to release a statement like this with no consequence (TCH has done the same), they are essentially giving the middle finger to the DOJ and all the victims they have harmed.
The end result is a major children's gender clinic has gotten away with a crime that would send other doctors to prison, and they're writing it off as minor line item on next year's billion dollar annual budget.
Although DOJ has been doing good work, we cannot let these hospitals get away with this conduct so easily.
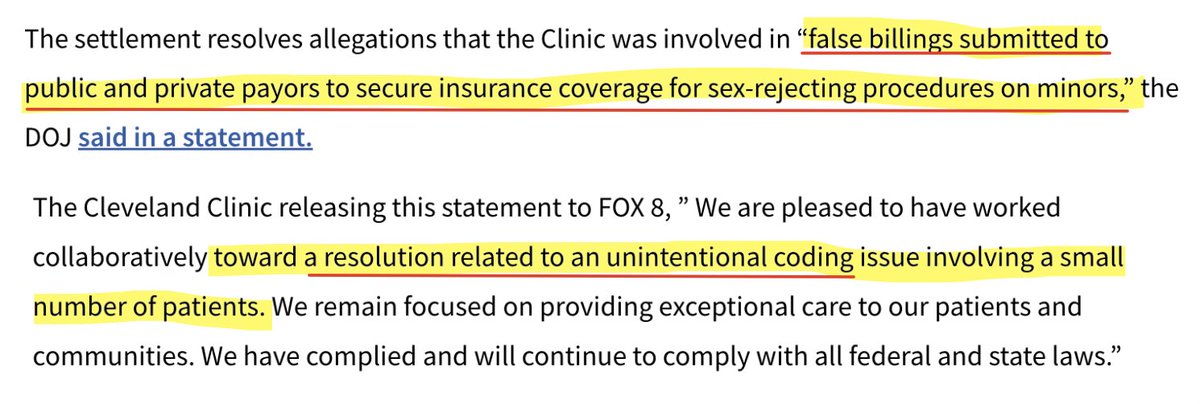
Jun 9

BIG WIN
@ClevelandClinic agrees in settlement with DOJ to commit $2 MILLION for detransition care and a 20-year BAN on s*x change surgeries for minors.
It should be banned forever, but other than that, big win 👏
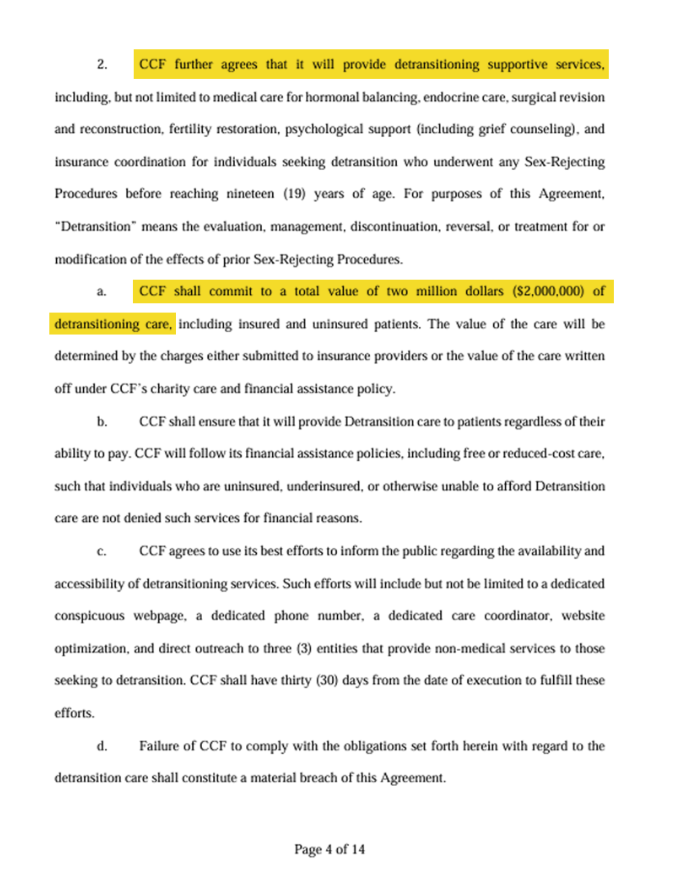
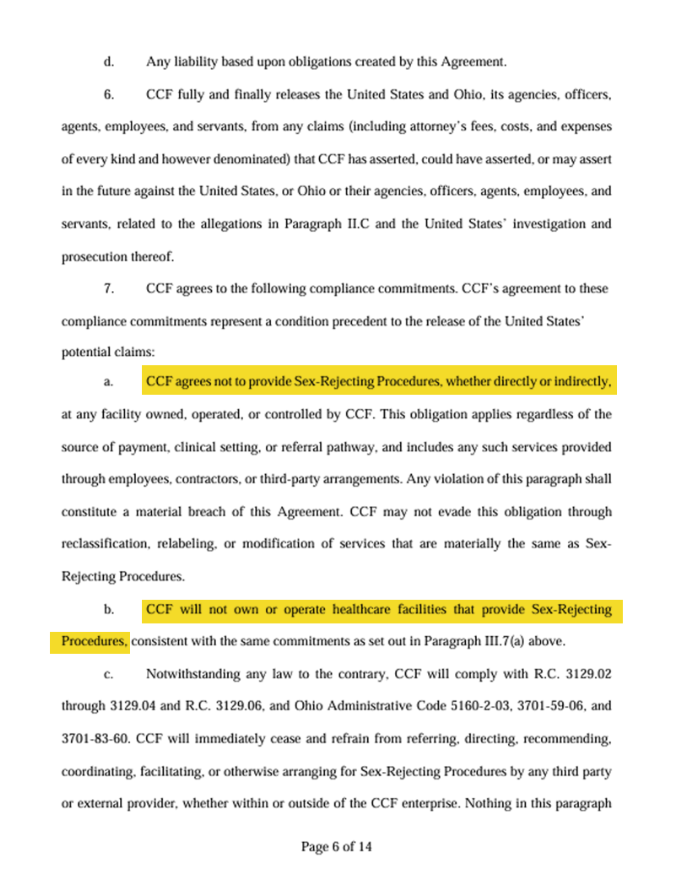
4
12
49
3,327
Travis Morrell, MD MPH retweeted

Jun 12
Thanks to the kind shout out from @NellieBowles in this week’s TGIF for @TheFP:
Jun 9

Over 1 in 250 Natal Girls Were Taking Testosterone By Age 17 in Oregon, From 2016 to 2023
open.substack.com/pub/benrya…
This rate, from a study of data about insured adolescents in Oregon, represents an average over this period. Given swift increases in hormone uptake over time, the rate was likely much higher by 2023.
The use of gender-transition drugs among adolescents in Oregon soared between 2016 and 2023, charting a nearly 10-fold increase among biological girls and a 14-fold increase in natal boys. Across this period, about 1 in 100 insured youth ages 8 to 17 in the Pacific Northwest state were diagnosed with gender dysphoria, a psychiatric condition involving distress stemming from a conflict between an individual’s natal sex and their gender identity.
By age 17, about 1 in 240 insured natal girls were taking testosterone and about 1 in 630 natal boys were taking estrogen in Oregon. These figures are nearly three-fold higher for natal girls and nearly twice as high for natal boys as figures from a study published last year that analyzed national data on commercially insured youth from 2018 to 2022.
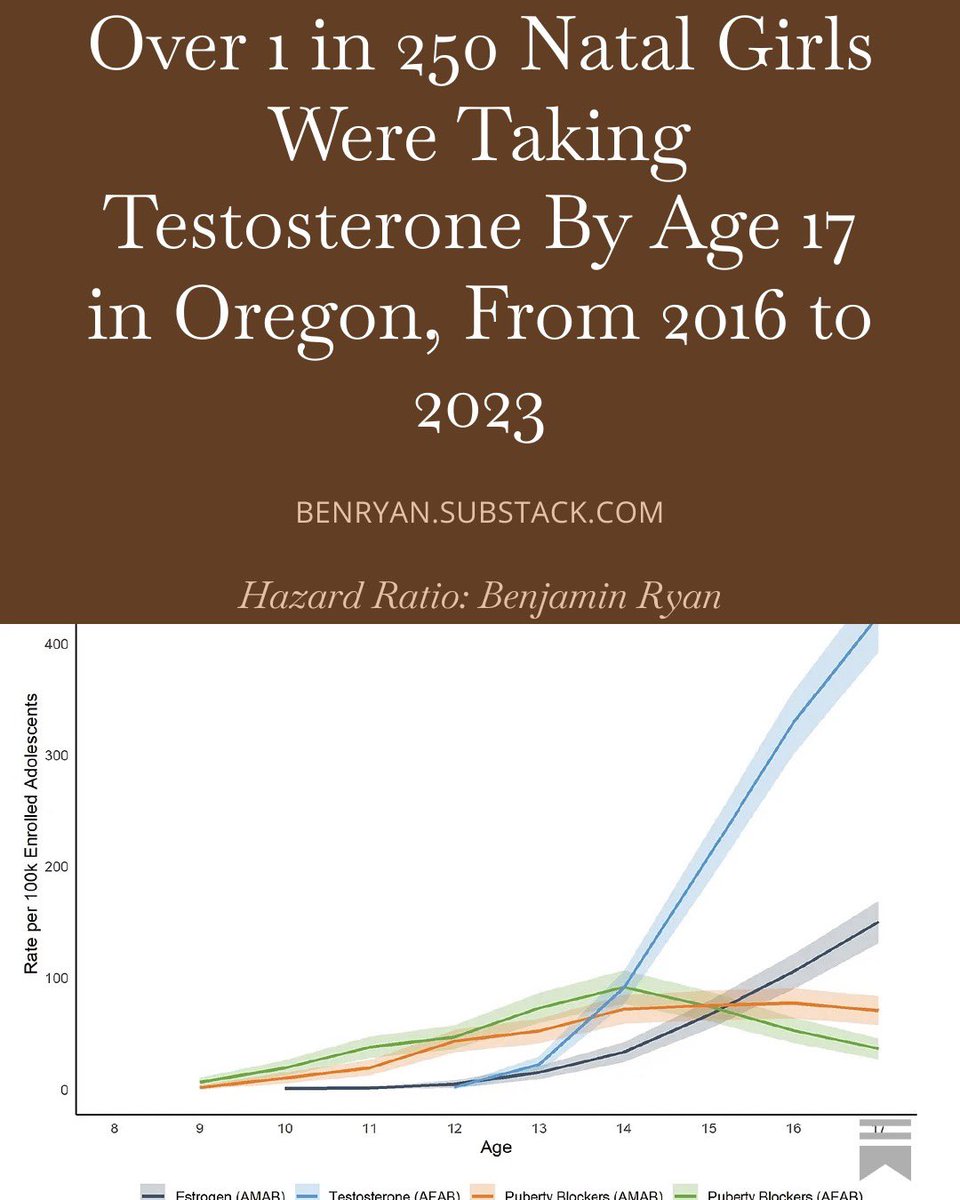
3
7
38
5,922
Travis Morrell, MD MPH retweeted

Jun 12
Let’s make one thing very clear: signing up for girls’ wrestling is in NO way a permission slip for sexual assault.
As @ADFLegal explained in our lawsuit: “Digital penetration falls outside the scope of implied consent to participating in athletics because, under normal circumstances of girls wrestling, it is not a reasonably foreseeable hazard from the perspective of a girl wrestler. Nor is sexual assault or groping generally accepted by society as part of any lawful athletic contest.”
Also: girls who sign up for girls’ wrestling aren’t consenting to wrestle boys. Kallie Keeler was betrayed by multiple adults in authority, who knowingly allowed her to wrestle a male without her knowledge or consent. They bear responsibility for what happened to her—and they are continuing to put female wrestlers in harm’s way through their actions and policies.
That’s why, besides suing governing bodies @wiaawa, @waOSPI, and the Puyallup School District, we’re also suing:
- State superintendent Chris Reykdal
- Kallie’s principal
- Her school district’s Title IX coordinator
- Her opponent’s coach
… and not just in their official capacities, but as individuals.
I’m also glad to hear the local prosecutor is reportedly still considering action against those who failed to report the sexual assault, as required by law. These mandatory reporters should have reported the incident within 48 hours but waited 53 days. They should face consequences.
We won’t rest until Kallie gets justice—and girls in Washington state get their sports back.
Jun 11

NEW: Prosecutors say they will not charge trans wrestler with alleged sexual assault of Kallie Keeler because of "case law concerning consent in athletic contests." If only the state of Washington had given Kallie the option to consent to being touched by a male.
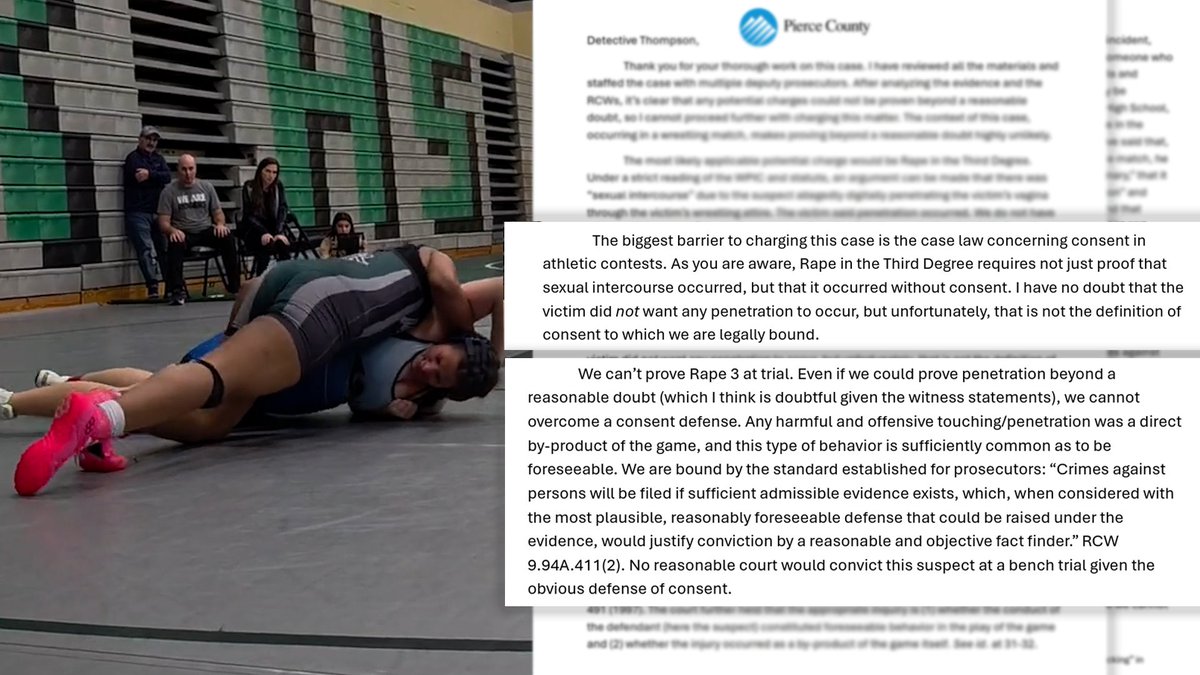
233
1,980
7,424
110,434
Travis Morrell, MD MPH retweeted

Jun 12
ARIZONA
Legislation providing remedies for individuals harmed by "gender medicine" is much needed. AZ's legislators recognize this. But not the governor.

My testimony in favor of Arizona SB 1094, a bill that would give detransitioners recourse for treatment.
If detransitioners aren’t common, it won’t be a problem….
Unfortunately, Arizona’s Governor Hobbs has vetoed this bill, leaving harmed patients out in the cold.
1
1
1
122
Travis Morrell, MD MPH retweeted

ICYMI: To kick off Pride Month, Gov. Jared Polis signed HB26-1322 — a bill letting “conversion therapy” (biological reality) recipients sue counselors, employers, and even parents for unlimited damages.
*He was surrounded by One Colorado, the tax-payer-funded opposition to our ballot measures while signing this into law*
This directly defies the Supreme Court’s recent 8-1 ruling in Chiles v. Salazar striking down Colorado’s prior ban (HB19-1129) as unconstitutional viewpoint discrimination.
Democrats doubled down: no statute of limitations, reversed burden of proof, and heavy liability for any provider OR PARENT who affirms biological reality instead of pushing wrong-sex confusion.
Colorado has made gender ideology its state mandated religion — with over 20 laws forcing it on kids, schools, and families. Dissent = lawsuits.
Biological truth isn’t hate. Helping children be comfortable in their body & biological sex isn’t “conversion therapy.” Our freedom to tell our children the truth isn’t optional.
Parents, counselors, Coloradans: your rights are under attack.
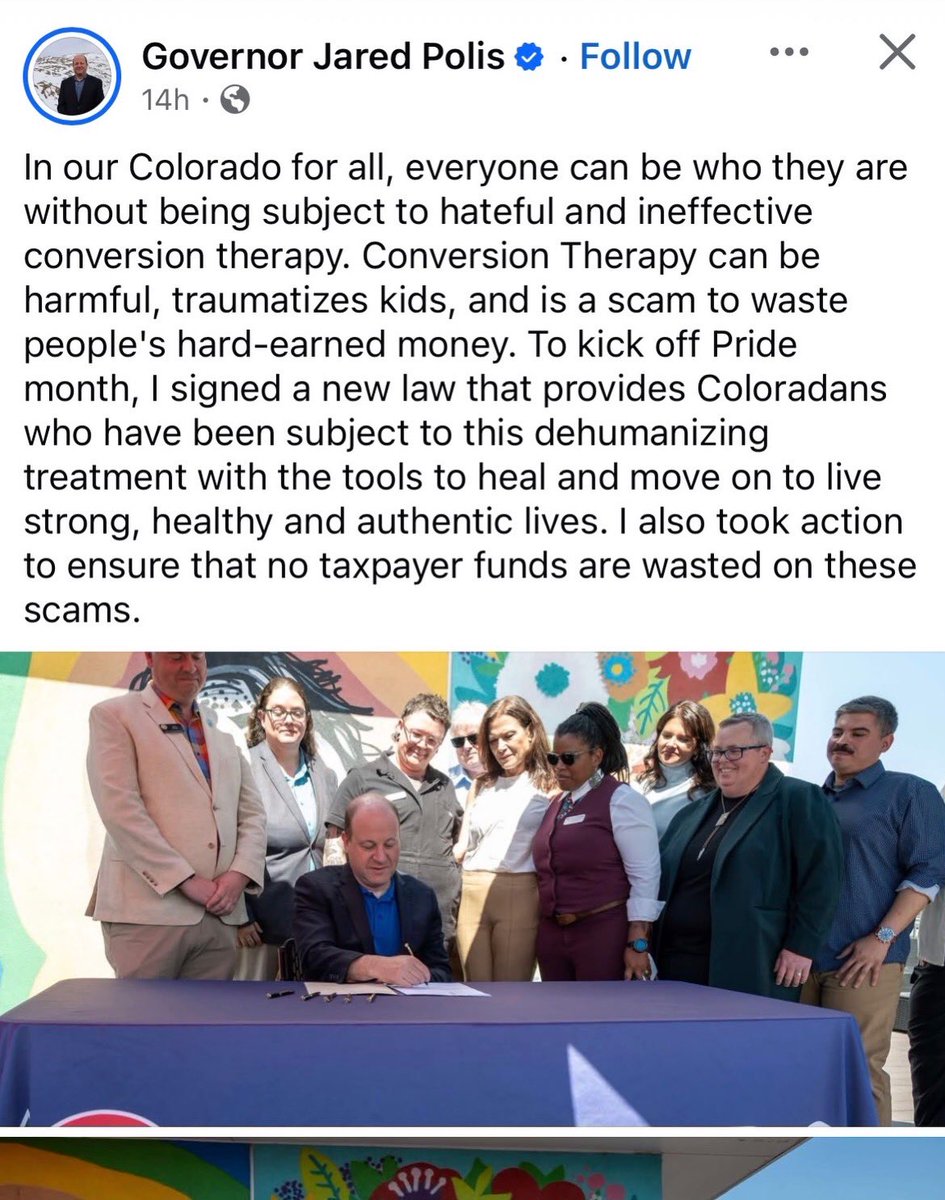
43
135
307
7,943
Travis Morrell, MD MPH retweeted

Jun 12
I was always kind to rich, he was in my mind little chat group for a while. And now he blocks me and talks crap about me on a platform I'm not even on.
I'm sorry rich, did you get mad because I didn't want to retweet your posts of you bragging about being on newsmax and Fox News? Literally he would just DM post and post of him attention whoring, not even stuff that helps the cause here in CO. Im so tired of all these people I helped and had no problems with turning around and coming at me. Seems to happen a lot once they start working with the homewrecker caucus. Now you have the dark mark too.
20
3
91
5,469
Travis Morrell, MD MPH retweeted
Jun 12
Gender activists are using the bogus results of the Utah Review to claim puberty blockers are "safe and beneficial."
But it's only "safe and beneficial" because they excluded the significant and expected harm - like infertility! (see video)
It's like publishing a study advocating for people to become alcoholics by citing evidence that increased consumption is correlated to better mental health outcomes because over the short term, you will have a really good time (technically true).
But left out of this study are all the expected harms - like all of your organs, namely your liver, turning into dog meat and dying an awful painful death (trust me, this is one of the worst ways to go).
All the while, Democrat politicians nod along like this is totally normal and "evidenced-based."
Jun 11

A recent letter from Democrats in the Congressional Equality Caucus (@EqualityCaucus) to HHS Secretary Robert Kennedy, Jr. (@SecKennedy) cites the Utah review as proof that puberty blockers and cross-sex hormones are "safe and beneficial" for adolescents.

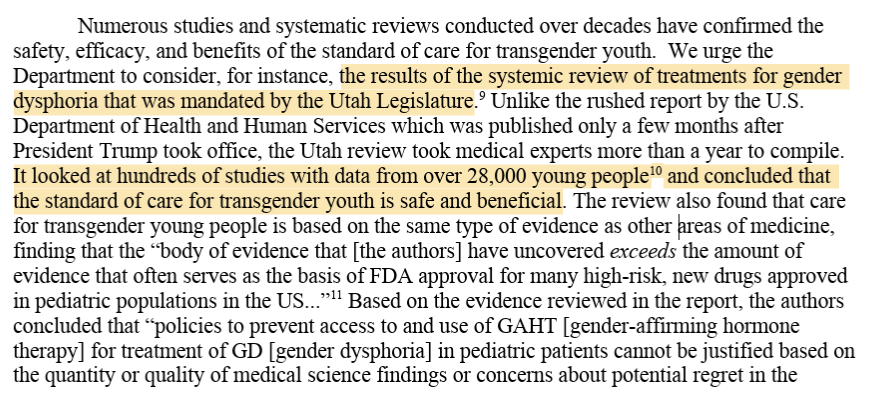
4
51
173
4,836
EPIC FAIL:
How activists used a massive gov’t-protected industry to invade YOUR life:
- force “gender” compliance
- give kids secret access
- bias doctors & nurses against elderly patients
- put women’s health at risk
Another 🔥 in-depth from @ColoradoDoctors’ Unpaid Intern🧑⚕️
WHEN EPIC ISN'T REALLY EPIC: How Gender Ideology Was Integrated into Epic Systems' Electronic Health Records
Epic Systems Corporation’s electronic health record (EHR) platform, used by approximately 41% of 🇺🇸 hospitals and historically as many as 80% of outpatient settings, as well as internationally, has systematically incorporated structured fields for self-identified gender identity that are separate from, and often displayed more prominently than, biological sex. The integration happened through a deliberate sequence of internal technical development at Epic, coordinated external advocacy from trans industry organizations, and federal regulatory requirements tied to incentive payments. The result is the Sexual Orientation and Gender Identity (SOGI) SmartForm, (sex) organ inventory tracking, visible patient banners and headers, automated SmartLinks, and configurable MyChart proxy access settings. These features treat gender identity as core, structured, queryable data embedded throughout clinical workflows, notes, portals, faxes, research queries, and national interoperability standards. To gender identity believers, nothing says “evidence-based medicine” quite like elevating subjective self-report to the level of immutable biology.
HOW IT STARTED
The internal catalyst at Epic was Janet Campbell, who joined the company in 2003 immediately after graduating from Carleton College with a computer science degree and additional coursework in gender studies. But, of course. Her first assigned project required building system rules to restrict diagnostic and billing codes according to recorded patient sex, for example, blocking orders for cervical examinations on patients whose record listed “male.” This work quickly revealed that Epic’s longstanding single “sex” field, limited since the company’s founding in 1979 to the options male, female, or unknown, was functionally "overloaded", as per Janet Campbell. It was seen to be simultaneously serving as a proxy for real sex or "sex assigned at birth", legal sex, and the emerging activist concept of gender identity. The resulting mismatches produced billing errors, inappropriate clinical alerts, and unreliable data for research or quality reporting, problems that, in a less ideological era, might have been solved by simply respecting biological reality rather than inventing new fields to accommodate delusuins.
In approximately 2004–2005, Campbell volunteered to deliver an internal educational presentation during Epic’s regular workplace talk series. One slide stated verbatim: “Epic is almost completely unable to deal with this level of complexity, and neither is the medical profession, for that matter.” Sure, Jan. By January 2012 she had posted an internal wiki page proposing a two- or three-step data-capture sequence: sex assigned at birth, legal sex, and gender identity. A cross-functional workgroup was assembled that included several "transgender" and "non-binary" Epic employees - its stated purpose was to assist customers with implementation. In 2013 the group produced and distributed a “SOGI Strategy” handbook that supplied both technical instructions and sections on "transgender cultural competence" and the distinction between identity and sex, helpfully ensuring that every hospital using the system received a gentle primer on why feelings should sometimes trump chromosomes.
INFLUENCE OF THE TRANS INDUSTRY
The external pressure that accelerated these changes came from a sustained advocacy campaign. The coalition involved represented a wide network of LGBT health, HIV advocacy, and related organizations, with prominent leadership from The Fenway Institute at Fenway Health. In January 2013 this coalition of 145 leading LGBT and HIV/AIDS organizations submitted a formal public comment to the Office of the National Coordinator for Health Information Technology (ONC) urging inclusion of sexual orientation and gender identity (SOGI) data collection in Meaningful Use guidelines. Early in 2014 the same network expanded to 153 organizations and submitted recommendations asking ONC to direct the National Library of Medicine to develop new SNOMED code sets specifically to support accurate and effective SO/GI data collection in certified EHRs. These submissions formed part of a broader effort to embed SOGI capacity within the proposed 2015 Edition Certified EHR Technology (CEHRT) criteria for Meaningful Use Stage 3. Because when biology proves stubborn, the next best step is apparently to lobby the government to reprogram the nation’s medical software. Fenway Health, operating through its Fenway Institute and National LGBTQIA Health Education Center, functioned as the central technical and policy coordinator.
As early as 2011, Fenway had begun testing two-step gender identity questions (gender identity asked first, followed by sex assigned at birth) at its own federally qualified health center. In roughly 2012 it published the policy brief “How to Gather Data on Sexual Orientation and Gender Identity in Clinical Settings,” which formalized the two-step approach originally developed by the Philadelphia Transgender Health Advocacy Coalition in 1997 and later endorsed by UCSF’s Center of Excellence for Transgender Health. Fenway partnered with the Center for American Progress on the “Do Ask, Do Tell” project, releasing online toolkits explicitly aimed at EHR vendors and providers. In 2014 Sean Cahill, PhD (Director of Health Policy Research at the Fenway Institute) co-authored key papers and policy statements, including the PLoS One article “Sexual Orientation and Gender Identity Data Collection in Clinical Settings and in Electronic Health Records: A Key to Ending LGBT Health Disparities,” which framed SOGI collection as essential for equity and disparity reduction. Fenway supplemented these writings with slide decks, tip sheets, and formal regulatory comments that repeatedly positioned SOGI capacity as a NON-NEGOTIABLE REQUIREMENT FOR FEDERAL CERTIFICATION 🚩, turning a contested religious belief at best into a certification checkbox.
IT'S ALWAYS THE GOVERNMENT
These advocacy efforts aligned precisely with federal rulemaking. The 2015 ONC and Centers for Medicare & Medicaid Services (CMS) Meaningful Use/Promoting Interoperability final rules mandated that certified EHRs possess the technical capacity to record, store, change, and retrieve structured SOGI data in order to qualify for incentive payments. The requirement applied across approximately 78 percent of outpatient clinics by 2018. In 2016 the Health Resources and Services Administration (HRSA) further embedded the expectation by adding SOGI fields to the Uniform Data System (UDS) reporting obligations for all federally qualified health centers. The combination of coalition pressure and incentive-linked certification created powerful compliance incentives for both vendors and health systems, because nothing motivates hospitals quite like the threat of lost federal dollars for failing to ask patients about their feelings. It's a clear, breathtaking case of policy winning over ethics in the medical field.
EXPANSION WITHIN
Inside Epic, Campbell’s initial workgroup scaled into a 25-person “Volunteer Army.” The team performed a full-system audit and remapped hundreds of references to the original “sex” field throughout patient headers, laboratory normal ranges, genetic pedigrees, clinical decision-support logic, and other modules. Campbell characterized the overhaul as “like the Y2K of the health record.” Development milestones followed in rapid succession: a two-item gender identity update released to clinical customers in June 2016, followed by the complete SOGI SmartForm in November 2016. The SmartForm is a guided questionnaire triggered by clicking the gender or age line in the patient Storyboard or during registration, nursing assessment, or clinical encounters. It begins by recording gender identity; any mismatch with recorded sex automatically prompts follow-up questions on pronouns (including they/them and additional options), transition steps, and an organ inventory that distinguishes organs present at birth from those present currently, because the most reliable way to practice “precision medicine” is apparently to ask patients what their body parts used to be while politely ignoring what they actually are. This also serves as proof of the linguistic weaponization trans activists indulge in - conflating legitimate things like kidney donation with calling an inverted penis lined with scrotal skin a vagina. It's part of the tactic to normalize grotesque and experimental "transgender surgeries" as "just routine medical procedures".
Further refinements to the EPIC EHR in 2017–2018 introduced explicit distinctions among legal sex, gender identity, sex assigned at birth, and “sex for clinical use,” while chosen names and pronouns were propagated system-wide via SmartLinks. By mid-2017 Campbell reported that 10–20 percent of Epic customers had activated the updates. The captured data is structured rather than free-text, making it visible and actionable: chosen name, gender identity, and pronouns appear in patient banners and headers; SmartLinks automatically insert the information into notes, schedules, faxes, and reports. Patients, including minors as young as 12 in many implementations, can enter or update these fields directly through the MyChart portal; changes become part of the official record without mandatory clinical verification, because self-ID is apparently so infallible that no second opinion from a doctor is required. Hospitals frequently incorporate SmartForm completion rates into quality metrics, disparity dashboards, and DEI scorecards, and staff training modules draw heavily on Fenway’s cultural-competence materials.
Campbell has explained the design rationale in public remarks. In 2017 she stated: “Our goal is that patients get the right and appropriate treatment no matter who they are.” On the decision for universal collection she added: “I think that starting to collect this information from everyone will normalize it in many people’s eyes. It’s not that we’re asking certain people whether they happen to be trans, we’re just asking everybody.”
The trans activism is ever present, presented dishonestly. In the August 31, 2022, Clinical Architecture Informonster Podcast (Episode 23: “Discussing Gender Harmony”), recorded with Fenway’s Chris Grasso, Campbell explained that the original single field “had become overloaded and was asked to do double duty.” She described the 2017 safety corrections, such as revised creatinine-clearance calculations based on mismatched legal sex, and noted broader applicability: “The work that we’re doing here will benefit the entire patient community… It’s not just transgender patients who want to be called by a name that’s different than the name on their birth certificate.” Regarding documentation she advised: “If a patient isn’t living their gender identity, don’t document that information in those fields… the system will take your word for it and will put that everywhere.” Right, all that confusion and hoop-jumping due to the religious and fanatical belief in "gender identity", trying to get ahead of the chaos being caused. Epic continues to participate in the HL7 Gender Harmony Project, which has produced a national interoperability standard separating recorded sex/gender, gender identity, and “sex for clinical use,” each with validity periods. The SOGI and organ-inventory data therefore support anatomy-based alerts while preserving identity fields as the primary display element, because the clearest way to avoid clinical confusion is apparently to make identity the banner headline and biology the optional footnote. Gender ideologues purposely calculate to supercede the practice of ethical medicine to bolster their claims, reality be damned.
TARGETING MINORS IS NOT ACCIDENTAL
MyChart proxy access for minors remains configurable by each health system and is age-tiered. Common configurations include independent portal access at age 12 (UF Health Shands), “Teen Plus” limited parental views (Wellstar), and parent-teen access at age 13 (UNC). "Sensitive sections" like SOGI data, preferred pronouns, organ inventory, and transition-related notes, CAN BE HIDDEN FROM PARENTS, frequently extending beyond the original intent of adolescent privacy statutes written for STIs or contraception. A 2025 Do No Harm @donoharm report catalogued these settings and quoted Epic’s own documentation, which states that proxy access “changes as they get older” according to each organization’s interpretation of privacy laws. Vague enough. The cumulative architecture produces a workflow in which gender-identity documentation is routine, frictionless, and self-reinforcing, marketed to the very young and old alike.
DECLINES TO ANSWER
If elderly patients are confused about "personal pronouns", they are marked as "Declined to answer" in a prominent manner in their profiles that anyone opening their chart can see. I have seen this happen to patients with dementia! This phrasing of "refused to cooperate" is meant to create bias in the minds of the clinician that the patient is difficult, and try to force compliance with gender ideology in both the doctor and the patient. Clinicians encounter prompts in core interfaces, data auto-propagates across the record and external systems, and non-use of the features can register as incomplete documentation or failure to meet incentive or equity metrics. These dubious metrics have converted advocacy goals into certification requirements. The outcome is a dominant EHR platform that has embedded self-identified gender identity as a core element across millions of patient records, completely ignoring evidence-based safeguards.
PATIENT SAFETY CONCERNS, THE ULTIMATE EPIC FAIL
Even in electronic health record systems where biologic sex, legal sex, and gender identity are all separately and clearly documented, significant patient-safety concerns remain because downstream clinical systems frequently fail to operationalize those distinctions consistently. Multiple health systems and informatics groups have documented that laboratory software, radiology workflows, preventive screening algorithms, insurance systems, and clinical decision-support tools often still rely on a single operative sex variable despite more sophisticated chart architecture.
At Geisinger Health System, clinicians and informatics staff described needing extensive custom modifications to Epic because standard workflows could not reliably coordinate birth sex, organ inventory, hormone exposure, and preventive screening logic simultaneously. The Veterans Health Administration similarly acknowledged tension between visibility of natal sex and identity-related workflows, warning that suppressing or obscuring biologic sex could impair preventive care and emergency clinical reasoning.
Real-world failures described in the literature include biologically female patients losing automated cervical cancer reminders after administrative sex changes, insurance denials for Pap smears or PSA testing when legal sex conflicted with anatomy, pregnancy-related safeguards failing because workflows operationalized identity-facing fields incorrectly, and laboratory systems inconsistently applying sex-based reference ranges for hemoglobin, creatinine, eGFR, CK, and troponin. Pathologists and laboratorians have repeatedly noted that current systems struggle to interpret altered hormone states because a testosterone-treated female remains biologically female while exhibiting partial shifts in selected analytes, creating ambiguity that simplistic identity-based categorization cannot safely resolve.
Researchers in medical AI and informatics have additionally warned that inconsistent handling of sex, gender identity, legal sex, and hormone exposure produces “sex/gender slippage” in datasets, threatening the reliability of epidemiology, predictive algorithms, and machine-learning models. The central concern raised by clinicians focused on sex-based medicine is therefore not merely missing data fields, but that medicine remains fundamentally organized around biologic sex while many EHR systems and institutional workflows operationalize sex-related variables inconsistently, creating opportunities for diagnostic error, screening failures, inappropriate clinical decision support, and degraded research quality even when all demographic categories are technically present and clearly separated.
The corruption of Epic EHR demonstrates how gender ideology became medical infrastructure when the right mix of activists, incentives, federal cooperation, and software engineers decided that their unfounded beliefs trump reality, endangering patient healthcare in the process. Your mind and body are both the donor organs and the subsequent profit to the trans industry. An EHR is a tool and repository that helps maintain and improve medical records. Using it to cement the nebulous concept of gender identity as fact is subjecting the material reality of patients and doctors to dangerous process errors and repeated trans industry indoctrination. Get your act together, EPIC, and put patient safety first, before it's too late.
SOURCES AND REFERENCES
- Ingraham N, et al. Overcoming technical and cultural challenges to delivering equitable care for LGBTQ individuals in a rural, underserved area. JAMIA Open. 2022.
PMC article
- Klee A, et al. Evolving Sex and Gender in Electronic Health Records. Fed Pract. 2018.
PMC article
- Greene DN, et al. Challenges in Transgender Healthcare: The Pathology Perspective. Clin Chem. 2016.
PMC article
- Cheung AS, et al. Approach to Interpreting Common Laboratory Pathology Tests in Transgender Individuals. J Clin Endocrinol Metab. 2021.
Oxford Academic article
- Keyes O, et al. Sex trouble: Sex/gender slippage, sex confusion, and sex obsession in machine learning using electronic health records. Patterns. 2022.
ScienceDirect article
- Kannan V, et al. Challenges with Accuracy of Gender Fields in Identifying Transgender Patients in Electronic Health Records. AMIA Annu Symp Proc. 2020.
PMC article
- Collecting Sexual Orientation and Gender Identity Data in Electronic Health Records. National Academies Press.
NCBI Bookshelf
- Wired.com, “The Battle to Get Gender Identity Into Your Health Records” (June 30, 2017) – Campbell’s timeline, internal presentation quote, 2012 wiki proposal, workgroup formation, 2013 SOGI Strategy handbook, Volunteer Army audit, Y2K comparison, and technical rollout details.
- Isthmus.com, “UW Health aims to be more sensitive to gender identity” (July 6, 2017) – Campbell’s direct quotes on the SmartForm purpose, normalization through universal collection, and adoption statistics (10–20% of customers, 20–40 providers).
- Clinical Architecture Informonster Podcast, Episode 23: “Discussing Gender Harmony” (August 31, 2022) – Full transcript excerpts of Campbell discussing the overloaded single sex field, 2017 clinical safety fixes, HL7 Gender Harmony collaboration, privacy advice, and benefits for all patients; includes joint discussion with Fenway’s Chris Grasso.
- Do No Harm report, “Parental Access to Children’s Medical Records” (October 2025) – Details on Epic SOGI SmartForm mechanics, organ inventory, MyChart proxy access configurations at specific health systems (UF Health Shands, Wellstar, UNC), and analysis of concealment practices beyond legal minimums.
- Fenway Health / National LGBTQIA Health Education Center, “Collecting Sexual Orientation and Gender Identity (SO/GI) Data in Electronic Health Records” (2016 PDF) – Implementation toolkits, clinical workflows, and ties to Meaningful Use / HRSA requirements.
- Cahill et al., “Sexual Orientation and Gender Identity Data Collection in Clinical Settings and in Electronic Health Records: A Key to Ending LGBT Health Disparities” (PLoS One, 2014) – Core advocacy paper outlining the case for SOGI inclusion.
- Fenway Health, “How to Gather Data on Sexual Orientation and Gender Identity in Clinical Settings” (policy brief, ~2012) – Early testing protocols and two-step question recommendations.
- Center for American Progress / Fenway Institute joint statement (October 7, 2015) – Praise for the 2015 ONC/CMS Meaningful Use rules requiring SOGI capacity in certified EHRs.
- Fenway Health “Do Ask, Do Tell” toolkit and related 2014–2016 publications – Broader SOGI EHR advocacy, promotion of standardized questions, and collaboration with other groups.
ONC/CMS 2015 Edition Certified EHR Technology (CEHRT) Criteria and Meaningful Use/Promoting Interoperability final rules – Federal requirements for SOGI data capacity in certified systems, tied to incentive payments.
- Additional cross-referenced context from HRSA Uniform Data System (UDS) updates (2016), HL7 Gender Harmony Project documentation, and public Epic customer implementation examples (e.g., University of Wisconsin, Geisinger). All information is drawn exclusively from publicly available records as of 2025.
- Cahill S. “Sexual Orientation and Gender Identity Data Collection Update: U.S. Government Takes Steps to Promote Sexual Orientation and Gender Identity Data Collection Through Meaningful Use Guidelines.” LGBT Health (2014/2016 update) – Details on the 153 LGBT and HIV groups’ 2014 recommendations to ONC for SNOMED codes and the 2013 public comment from 145 organizations.
- Cahill S, Makadon H. Related policy briefs and Fenway Institute publications (2012–2016) – Documentation of coalition advocacy, two-step questions, and EHR implementation guidance.
#sexnotgender #genderidentity #epicEHR #epic #epicfail #ehr #medicalethics #MedTwitter #MEDX #donoharm #safety #propaganda
3
31
61
5,761
A few activists drove gender ideology in a massive company—politicians mandate its use—so one person at EPIC can effectively mandate aspects of medical practice ACROSS THE COUNTRY.
Yet no one gets to vote on whether medical records mandate gender ideology (or even whether they work well).
This is how we get a few unelected activists running aspects of the country.
7
90
When all of social media hates you
0.029% of real people agree
Jun 12

Most people don't understand extrapolation. If you know of 100K people online who believe X, that sounds like a lot -- until you realize that it's ~0.029% of the population (just in the US).
100K people yelling at you looks and feels like a lot more.
2
64
My testimony in favor of Arizona SB 1094, a bill that would give detransitioners recourse for treatment.
If detransitioners aren’t common, it won’t be a problem….
Unfortunately, Arizona’s Governor Hobbs has vetoed this bill, leaving harmed patients out in the cold.
12
34
136
4,769
Travis Morrell, MD MPH retweeted

This dumb standard is the pillar that DEI stands upon. If it falls, DEI is rekt.
Jun 10

The Justice Department has released new guidelines that find the EEOC’s use of “disparate impact” is unconstitutional.
Good.
Disparate impact is a woke legal doctrine that’s rewritten American standards:
16
131
603
11,651
Travis Morrell, MD MPH retweeted

The utah review has one purpose: to give people who put ideology before science something science-y to chew on so they would not look like captured.
Jun 11
A recent letter from Democrats in the Congressional Equality Caucus (@EqualityCaucus) to HHS Secretary Robert Kennedy, Jr. (@SecKennedy) cites the Utah review as proof that puberty blockers and cross-sex hormones are "safe and beneficial" for adolescents.
1
6
38
1,071
Just because “no one” is disagreeing doesn’t mean everyone agrees.
Maybe everyone is afraid to speak. Or hoping others will speak first.
Another great video from MJ.
5
9
71
971
Travis Morrell, MD MPH retweeted
The ACLU seems scared of people finding out how captured by the trans industry they really are. x.com/ColoradoDoctors/status…
The American Civil Liberties Union (ACLU) is a famous non-governmental organization (NGO) that has been at the forefront of legally implementing gender ideology framework across the 🇺🇸 over decades, beginning with challenges to cross-dressing ordinances, & evolving into extensive litigation, policy advocacy, and defense of "gender-affirming" interventions framed as necessary for individuals identifying as "transgender".
TIMELINE
EARLY INVOLVEMENT (1960s–1980s)
In 1967, ACLU attorney Jean Martin played a central role in efforts to challenge Los Angeles Municipal Ordinance Rule No. 9, which barred (drag) performers from “impersonating” a person of the opposite sex by means of costume or dress. The case arose after police threatened the owner of the Red Foxx Club over performances by Sir Lady Java, male performer. With ACLU assistance, Sir Lady Java sued the city. The California Supreme Court ultimately declined to hear the case. By 1980, the ACLU of Southern California established the Transsexual Rights Committee, later chaired by Diane Saunders, to integrate transsexual issues into its civil liberties agenda. Saunders corresponded on these matters with trans activist Lou Sullivan (a woman writer who identified as a man) as late as 1984, and the committee advanced changes for "transsexual people" in California, while providing materials to attorneys challenging cross-dressing laws elsewhere.
In 1973, the national ACLU launched its Sexual Privacy Project under the direction of attorney Marilyn Haft (NYU Law ’68), which addressed cross-dressing challenges by teaming it alongside other issues like prostitution. The project, funded by the Playboy Foundation, operated until 1977 and pursued test cases in multiple jurisdictions including St. Louis, Louisville, and Winston-Salem, though it lost many of the cases it litigated.
The ACLU of Florida collaborated in 1971 with the Gay Activists Alliance of Miami and the National Coalition of Gay Organizations to challenge Miami Beach’s anti-drag and anti-cross-dressing ordinances as unconstitutionally vague; attorneys demonstrated the laws’ ambiguity by presenting unisex apparel to the chief of police, who conceded enforcement would “depend on the person and the circumstances.” The organization formally endorsed gay rights principles in 1966 and created the Sexual Privacy Project shortly thereafter; in 1986 it launched the Lesbian and Gay Rights Project (later the LGBTQ & HIV Project).
EXPANSION IN THE 2000s AND 2010s
By the 2000s, efforts intensified around identity documents, employment, prisons, schools, and health care.
In 2005–2010, the ACLU represented Diane Schroer, a trans-identifying man and retired Army colonel, in a Title VII sex-discrimination suit against the Library of Congress. Schroer, who had begun transitioning after 25 years of Army service including Special Forces and counterterrorism work, was offered a position as a terrorism research analyst but had the offer rescinded after disclosing the transition to the future supervisor. The ACLU argued this constituted sex discrimination. The court allowed the case to proceed, ruling that Title VII protections against sex discrimination may extend to such situations because “sex” is not limited to chromosomes and that discriminating against someone for failing to conform to sex stereotypes or for transitioning violates the law. The court ultimately awarded Schroer the maximum $500,000 in compensation.
In 2011, after a six-year battle in Fields v. Smith (helped by NGO Lambda Legal), the ACLU secured a 7th Circuit ruling striking down a Wisconsin law that barred hormone therapy or sex reassignment surgery for individuals identifying as the opposite sex in state custody. The court held the ban amounted to deliberate indifference to serious medical needs under the Eighth Amendment.
In 2012, court rulings and settlements in Alaska and Illinois eased requirements (surgery or otherwise) for updating gender markers on driver’s licenses and birth certificates.
The ACLU contributed to broader federal policy shifts, including 2010 Obama administration inclusion of "gender identity" in equal employment opportunity policies. It has been counsel or involved in multiple Supreme Court-related LGBTQ cases, including work tied to the 2020 Bostock v. Clayton County decision (and consolidated cases), which held that Title VII protections against sex discrimination extend to gay and trans-identifying individuals. Several ffiliates of ACLU have helped enact gender-identity nondiscrimination laws in employment, housing, and public accommodations in 16 states.
SCHOOL AND FACILITIES ACCESS LITIGATION
Changing school and facilities access cases for the have been some of their proudest 🤢 work, directly opposing privacy and safety of females among other social disruption.
The ACLU represented Gavin Grimm, a trans-identifying woman (female), in Grimm v. Gloucester County School Board. Grimm sued after the school board adopted a policy requiring students to use restrooms matching biological sex following complaints about her use of the boys’ restroom. The ACLU argued this violated Title IX and the Equal Protection Clause by discriminating on the basis of gender identity and sex stereotypes.
Similar litigation occurred in Indiana (A.C. v. Metropolitan School District of Martinsville and Vigo County cases), where courts affirmed access to bathrooms/locker rooms matching stated gender identity for students identifying as the opposite sex.
The ACLU intervened in Oregon’s Parents for Privacy v. William P. (Dallas School District) and Ohio’s Bethel Local School District case to defend policies allowing access based on gender identity. In 2023, the 7th Circuit upheld rulings requiring Indiana schools to provide such access.
SPORTS PARTICIPATION LITIGATION
Sports participation cases, fighting to remove sex-based sports teams, rendering female sports pretty meaningless, accelerated in the 2020s.
The ACLU, often with Lambda Legal and Legal Voice, challenged state laws restricting participation on teams based on sex, trying to destroy female sports.
Key cases include Hecox v. Little (Idaho’s Fairness in Women’s Sports Act, 2020), which barred biological males from female-designated sports teams. The ACLU represented trans-identifying male athletes seeking to compete in women’s categories, securing a preliminary injunction on Equal Protection and Title IX grounds (later subject to Supreme Court consideration and motions to dismiss). In B.P.J. v. West Virginia State Board of Education (West Virginia’s 2021 ban on males in female sports), the ACLU similarly challenged the law. The case was combined with Idaho’s for Supreme Court review in the 2025–2026 term on Equal Protection and Title IX grounds. The ACLU argued these bans violate constitutional and statutory protections, and courts issued injunctions allowing participation in some instances pending appeals. Additional challenges targeted NCAA policies and state laws in other jurisdictions. Little v. Hecox and West Virginia v. B.P.J. are both currently pending before the U.S. Supreme Court after being granted review in 2025. They were argued together on January 13, 2026, and a decision is expected by the end of the Court’s current term (likely June or early July 2026).
PRISON AND DETENTION LITIGATION
Prison and detention cases focused on medical access and housing.
In Fields v. Smith, the ACLU challenged Wisconsin’s ban on "gender-affirming care" for inmates identifying as the opposite sex. It represented Reiyn Keohane, a trans-identifying man, in Keohane v. Inch (Florida Department of Corrections denial of cross-sex hormones and "gender-affirming" surgery while housed in men’s prison, invoking deliberate indifference under the Eighth Amendment).
In North Carolina, the ACLU sought relief for Kanautica Zayre-Brown, a trans-identifying man denied "gender-affirming" surgery and earlier housed in men’s facilities. The organization has invoked the Eighth Amendment, PREA standards, and deliberate-indifference doctrines in filings emphasizing screening, housing consistent with gender identity, and treatment for inmates identifying as the opposite sex.
ACLU affiliates filed complaints over restroom/locker access for staff or inmates identifying as the opposite sex, always males wanting access to female spaces. It has been accused of egregious practices like giving male criminals false names in court and moving them into women's prisons, despite no legal name changes, so they become harder to trace in the system by journalists and the public.
MEDICAL INTERVENTIONS AND RELATED LITIGATION FOR "TRANS KIDS"
"Gender-affirming care" for minors cases proliferated after 2020. The ACLU has sued over state restrictions on puberty blockers, cross-sex hormones, and surgeries for minors diagnosed with gender dysphoria, often with Lambda Legal and others.
Examples include Brandt v. Rutledge (Arkansas 2021 law banning such interventions for minors). The ACLU secured mixed outcomes, including some permanent injunctions on due-process grounds even after the Supreme Court’s U.S. v. Skrmetti decision).
In Loe v. Kansas (2025 challenge to SB 63 banning care for those under 18), a state court temporarily blocked enforcement.
The ACLU challenged Texas directives treating "gender-affirming care" for minors as potential child abuse (Doe v. Abbott).
It filed in South Carolina (Misanin v. Wilson), and brought federal suits against Trump administration executive orders restricting funding or access (2025 filings with PFLAG and GLMA).
By 2025-2026, approximately 18 states faced ACLU-led or joined suits against youth care bans, with the Supreme Court hearing U.S. v. Skrmetti (Tennessee ban on gender-affirming care for minors) in 2024–2025 before upholding the state law on equal-protection grounds while leaving some injunctions intact on other bases. The ACLU has repeatedly described these interventions as medically necessary and life-saving, ignoring all evidence to the contrary.
FUNDING SOURCES AND NETWORKS 💵 💵 💵
Around 2009, the Tides Foundation awarded $150,000 to the ACLU of Florida through its State Equality Fund, a philanthropic partnership that included the Gill Foundation, the Evelyn & Walter Haas, Jr. Fund, and anonymous donors. The grant supported the ACLU’s work to defend its trial court victory ending Florida’s ban on adoption by gays and lesbians, along with related public education efforts.
In the 2015 LGBTQ Grantmaking by U.S. Foundations report, documenting grants awarded that year, the ACLU received $2,766,000 from various foundation sources for LGBTQ-related work. Top funders of LGBTQ causes overall: Arcus Foundation (Jon Stryker), Gill Foundation (Tim Gill), Open Society Foundations, Ford Foundation, Tides Foundation, have supported the ACLU directly or through coalitions for advocacy, litigation, and policy on gender identity and individuals identifying as the opposite sex. Arcus, in particular, has backed the ACLU alongside Transgender Law Center and other groups. Collaborations include joint litigation with Lambda Legal, Transgender Law Center, Legal Voice, PFLAG, GLMA, and state affiliates.
The ACLU has managed to intentionally keep a lot of its funding sources private, and their dubious methods misusing the law to do this would be a whole book. Judging by the millions of dollars at its disposal, it's safe to say big money is exchanging hands to virulently litigate the reality of binary sex into legal disuse to benefit the trans industry.
PROMINENT ACLU LAWYERS AND PERSONAL STAKES
Chase Strangio serves as Co-Director of the ACLU’s LGBTQ & HIV Project and Deputy Director for Transgender Justice. Born October 29, 1982, in Newton, Massachusetts, she graduated from Grinnell College with a BA in history in 2004 and earned a JD from Northeastern University School of Law in 2010. She started to identify as "trans" during law school. Prior to joining the ACLU, Strangio was an Equal Justice Works fellow and Director of Prisoner Justice Initiatives at the Sylvia Rivera Law Project, where she represented individuals identifying as "transgender" in confinement settings. This means that she worked hard personally to put men in women's prisons. She co-founded the Lorena Borjas Community Fund. The fund was created to help "LGBTQ immigrants and" transgender people, especially trans Latina sex workers and detainees" pay bail, secure legal assistance, and avoid prolonged detention.
Strangio has been lead or key counsel in cases including Grimm v. Gloucester, the challenge to North Carolina’s HB2 bathroom bill, the Trump-era military ban on individuals identifying as the opposite sex (Stone v. Trump), R.G. & G.R. Harris Funeral Homes v. EEOC (part of the Bostock trial), representation of Chelsea Manning, and multiple youth "gender-affirming care" challenges.
In December 2024, she became the first openly trans-identifying woman to argue before the U.S. Supreme Court in U.S. v. Skrmetti. She has reluctantly testified in court that evidence does NOT point to "gender-affirming care" decreasing suicide rates, despite it being a common emotional blackmailing point of trans activism in general. She has been named to TIME magazine’s 100 Most Influential People list (2020) and received numerous awards, including an honorary doctorate from Grinnell College.
Strangio’s public statements have drawn strong criticism. In November 2020, she tweeted regarding Abigail Shrier’s book Irreversible Damage: The Transgender Craze Seducing Our Daughters: “stopping the circulation of this book and these ideas is 100% a hill I will die on.” She later deleted the tweet, stating it did not represent the ACLU and citing exhaustion from calls for her firing. Journalist Glenn Greenwald criticized the comments as inconsistent with traditional free-speech advocacy. In leaked audio after the Skrmetti decision, Strangio called certain New York Times coverage of issues involving "transgender" individuals “insidious” and “absolutely terrible,” asserting the paper is led by “this idea that they can situate us as a people to be hated.” A Washington Post opinion piece on the Skrmetti loss for ACLU stated: “The ACLU bet big on a trans rights case. Its loss was predictable,” noting that advocates “failed to see the fragility of the liberal consensus.”
James Esseks is Director (and former Co-Director) of the ACLU’s LGBTQ & HIV Project. A Harvard Law School graduate, he has overseen litigation, legislative efforts, and advocacy on LGBTQ issues since joining the project. Esseks has been involved in major cases on marriage equality (United States v. Windsor), adoption and foster care challenges (including Florida and Arkansas cases), and matters involving individuals identifying as the opposite sex. He has worked to oppose state bills restricting such identification or related medical interventions.
Leslie Cooper is a senior staff attorney (and at times deputy legal director) in the ACLU’s LGBTQ & HIV Project, having joined in 1998. Much of her work has centered on protecting the rights of "LGBT" parents and children, including lead counsel roles in adoption, foster care, and parental rights litigation. She has appeared on briefs and motions in cases involving medical interventions for minors identifying as the opposite sex, such as Brandt v. Rutledge, and prison health care challenges. Cooper is a 1995 graduate of New York University School of Law and has been recognized for two decades of LGBTQ advocacy.
Other ACLU attorneys involved in gender identity and related litigation include Li Nowlin-Sohl (staff attorney on multiple youth care and related briefs), Harper Seldin, and Barbara Schwabauer (state-level school access and youth care matters). The organization often has collaborated with external groups such as Lambda Legal and the Transgender Law Center in joint filings, with their own dogged attorneys.
OVERALL LITIGATION TRENDS AND OUTCOMES
The ACLU leads the fight for gender ideology, with state legislative responses to "transgender" medicalization, as well as sports, bathrooms, and prisons, mainly the "trans rights" of males to female-only events and spaces. The ACLU has tracked and opposed over 100 state laws since 2020 concerning issues of gender identity, while pursuing challenges in courts and legislatures. Outcomes have included injunctions against restrictions of "gender-affirming care" despite medical consequences, expanded access for males to female single-sex facilities/care/participation based on stated identity while ignoring dissent, and reinterpretations of Title IX and equal protection that treat gender identity as encompassed within sex discrimination.
Interestingly, West Virginia officials filed a letter with the U.S. Supreme Court on May 26, 2026, correcting factual representations made by the ACLU in the pending West Virginia v. B.P.J. case. The letter clarifies that trans-identifying male Becky Pepper-Jackson, a sophomore competing as a girl under a Fourth Circuit injunction, won the Class AAA girls’ state shot put championship with a personal-best throw of 38 feet, 11¾ inches and finished fourth in the discus, directly contradicting the ACLU’s false claim that B.P.J. had been finishing “near the back of the pack." The devil, they say, is in the details. How many times has the ACLU previously lied in court?
Once a proud organization that stood to protect the rights and freedoms of all people in the US, the ACLU has sadly been influenced and funded by the trans industry to deny the fundamental truth of male and female as being vital to human existence. The intent has been framed as noble, but all it does is ironically:
- sexualize and destroy sexual function in vulnerable minors and adults.
- violate and destroy sex-based rights of women and girls
- attempt to force-team with to use, but ultimately erase homosexuality.
As always, follow the money.
It's going to take a long time to undo the damage to, and misuse of, the American legal system by the fascist efforts of the ACLU. Efforts are ongoing.
SOURCES AND REFERENCES
- ACLU official document: “The Work of the ACLU: Linking Gender Identity and Gay Rights” (December 31, 2000; aclu.org), detailing Jean Martin’s role in the 1967 Sir Lady Java/Rule No. 9 challenge.
- ACLU History: Advocacy on Behalf of Transgender People (aclu.org/documents/aclu-hist…).
- ACLU LGBTQ Rights pages and press releases on specific cases (aclu.org/issues/lgbtq-rights…; individual case profiles), including Schroer v. Library of Congress press releases (2006–2009) detailing the job offer rescission and $500,000 award.
- Court records: Fields v. Smith (7th Cir.); Hecox v. Little; B.P.J. v. West Virginia State Board of Education; Grimm v. Gloucester County School Board; Keohane v. Inch; Brandt v. Rutledge; U.S. v. Skrmetti; Loe v. Kansas; additional state cases; Sir Lady Java/Rule No. 9 challenge (1967).
- Tides Foundation/ACLU of Florida joint press release (July 23, 2009): “Tides Foundation Awards $150,000 to ACLU of Florida to End State’s Gay Adoption Ban.”
- Funders for LGBTQ Issues / “LGBTQ Grantmaking by U.S. Foundations” 2015 tracking report (covering grants awarded in 2015; published 2017; lgbtfunders.org or hrfn.org PDF listing ACLU at $2,766,000).
- Additional philanthropy reports: “40 Years of LGBTQ Philanthropy,” 2018 and 2023 Resource Tracking Reports (lgbtfunders.org); Arcus Foundation, Gill Foundation, Open Society Foundations, Ford Foundation, and Tides Foundation materials on supported initiatives.
- Chase Strangio ACLU biography (aclu.org/bios/chase-strangio); New Yorker profile by Masha Gessen (October 12, 2020); PBS, NBC, and ACLU press releases on Supreme Court arguments (2024–2025); TIME 100 Most Influential (2020).
- ACLU official biographies: James Esseks (aclu.org/bios/james-esseks), Leslie Cooper (aclu.org/bios/leslie-cooper); NYU Law coverage on Leslie Cooper (February 12, 2018).
- Washington Post opinion: “The ACLU bet big on a trans rights case. Its loss was predictable” (June 21, 2025).
- Benjamin Ryan Substack: “‘Insidious’: The ACLU’s Chase Strangio Slams The New York Times In Leaked Audio” (post-Skrmetti comments).
- K. Redburn, “Before Equal Protection: The Fall of Cross-Dressing Bans and the Transgender Legal Movement, 1963–86,” Law and History Review (2022; Cambridge University Press), detailing ACLU roles, Marilyn Haft’s Sexual Privacy Project (1973–1977), Diane Saunders as Transsexual Rights Committee Chairwoman (1984 correspondence), 1971 Florida ACLU collaboration, and broader early challenges including John Miller case amicus support.
- Additional sources on Marilyn Haft: NYU Law profile (2019); law review articles including “How Sex Became a Civil Liberty” and “The Price of Privacy” referencing her direction of the Sexual Privacy Project.
- Cambridge Law and History Review article on cross-dressing bans and the trans legal movement (full Redburn citation above).
- KFF Policy Tracker on youth gender-affirming care.
- Sir Lady Java case coverage: TransGriot blog (2010) and related historical accounts confirming Jean Martin’s ACLU involvement.
- Digital Transgender Archive references to ACLU Transsexual Rights Committee and Diane Saunders.
- ACLU press releases on Schroer v. Library of Congress (2006–2009) confirming case facts and court rulings on sex discrimination.
#aclu #humanrights #fightthepower #sexnotgender #sexbasedrights #ProtectKids #genderidentity #fascism #genderaffirmingcare #fraud #unitedstates #usa #ngo #legal

3
14
145