
Anästhesie/Intensivmedizin. Autismus. Klimaangst. #notjustsad #medtwitter Privat hier. Follow ist nicht Zustimmung
Joined July 2016
- Tweets 8,143
- Following 732
- Followers 214
- Likes 75,817
34 Photos and videos







Pinned Tweet

21 Mar 2025
🧵#askingautistics I am planning an educational session for my team about perioperative care for autistic children (and adults) particularly for anaesthesia and recovery but happy to include pain management and intensive care. There’s literature and personal experience but 1/4
1
1
312
Musstdu Daswissen retweeted

Apr 10
Ozempic does not “force” a caloric deficit like a cattle prod. It changes appetite signaling, satiety, gastric emptying, insulin secretion, glucagon, and in many patients improves glycemic control, fatty liver markers, and cardiometabolic risk. That is metabolism.
The phrase “chemical crutch” is just moralizing in a lab coat. We do not call insulin a crutch, or antihypertensives a crutch, or glasses a crutch. We call them treatment.
And this obsession with “root cause” is usually a racket. Obesity and metabolic disease are not one thing with one sacred origin story. They are genetics, appetite regulation, food environment, insulin resistance, sleep, medications, activity, and yes, inflammation. GLP-1 drugs act on several of those pathways at once.
So no, this is not merely appetite suppression while the “real problem” hides in the basement. It is treatment of the very systems that are dysregulated. The scale is not the only outcome, but pretending improved blood sugar, less visceral fat, and better metabolic function do not count because a drug was involved is ideology, not medicine.
Apr 10

Ozempic isn’t fixing your metabolism, it’s suppressing your appetite while the root cause stays untouched.
By mimicking hunger-regulating hormones, these injections induce significant appetite suppression and delayed gastric emptying, effectively forcing a caloric deficit.
However, this exogenous intervention does little to resolve the underlying biochemical signaling issues or the cellular inflammation that drives weight gain in the first place.
When the focus remains solely on the scale rather than restoring metabolic flexibility, the body remains dependent on a chemical crutch while the root cause often rooted in hyperinsulinemia and poor mitochondrial function continues to simmer beneath the surface.
60
290
1,950
263,313
I took the German or Autistic diagnostic. Results: probably autistic. Wittgenstein would have gotten the same result. german.millermanschool.com/
Which is funny- because I’m German and probably autistic
1
55
Musstdu Daswissen retweeted

Mar 24
For people who read Surviving Sepsis guidelines, we recommend IN ketamine midodrine within 60 seconds. Former to prevent rage assaults, the latter to prevent vasovagal syncope. If the reader agrees with guidelines, high dose IM haldol. Strong recommendation, moderate evidence.
5
28
169
30,493
Musstdu Daswissen retweeted

Remembrance is not a violation.
I met with Ukrainian skeleton racer and member of Ukraine’s National Olympic Team, Vladyslav Heraskevych, and his father, coach of Ukraine’s skeleton team, Mykhailo Heraskevych. I presented Vladyslav with the Order of Freedom.
Ukraine will always have champions and Olympians. But above all, Ukraine’s greatest asset is Ukrainians – those who cherish the truth and the memory of the athletes killed by Russia, athletes who will never compete again because of the Russian aggression.
Thank you for your stance, your strength, and your courage. Glory to Ukraine!




994
8,000
48,663
810,265
Musstdu Daswissen retweeted
Feb 13
We’re being told hospitals are “flooded” with GLP-1 complications and that we’re at the “tip of the iceberg.” I’ve been a bariatric surgeon long enough to remember these drugs when they were still in trials. I’ve prescribed them. I’ve monitored patients on them. And when the ER had a question about one of my patients on a GLP-1, they called me. I am not seeing a flood. What I see — every single shift — are the consequences of untreated obesity: heart failure, uncontrolled diabetes, infections, sleep apnea crises, fatty liver disease progressing quietly toward cirrhosis. That is the deluge.
Yes, GLP-1 medications have side effects. We know what they are. We counsel patients about them. We stop the drug if needed. That’s called medicine. But the claim that a hidden catastrophe is overwhelming hospitals is not something you prove with adjectives. You prove it with data. And if such a signal were real, it would not remain invisible for long in a healthcare system that tracks admissions, billing codes, adverse events, and outcomes with relentless precision.
Obesity is a chronic, relapsing disease with serious downstream consequences. Treating it is not cosmetic vanity, and it is not “forcibly stopping people from eating.” It is modifying disordered physiology — something we do every day with insulin, thyroid hormone, antihypertensives, and chemotherapy. The relevant comparison is not drug risk versus zero. It is drug risk versus the very real morbidity of leaving obesity untreated.
If someone believes there is an iceberg, show the sonar. Until then, what I see in the emergency room is not a wave of GLP-1 disasters. I see the far more predictable damage of a disease we’ve under-treated for decades.
Feb 13

Hospitals are getting a ton of admissions with side effects from GLP-1 injections. People in the USA can’t see it, because there is no centralized data collection.
Thankfully, countries like the UK do collect all the data and can see it. We are only at the tip of the iceberg with this disaster.
It’s a terrible idea that millions of people are on a hormone-like substance to forcibly stop them from eating too much

125
313
3,763
1,154,352
Musstdu Daswissen retweeted

summer olympics: look at this teenager run really fast
winter olympics: look at this 41 year old mother of three do a backflip off the side of a mountain
44
7,891
186,400
1,671,597
Musstdu Daswissen retweeted

25 Dec 2025
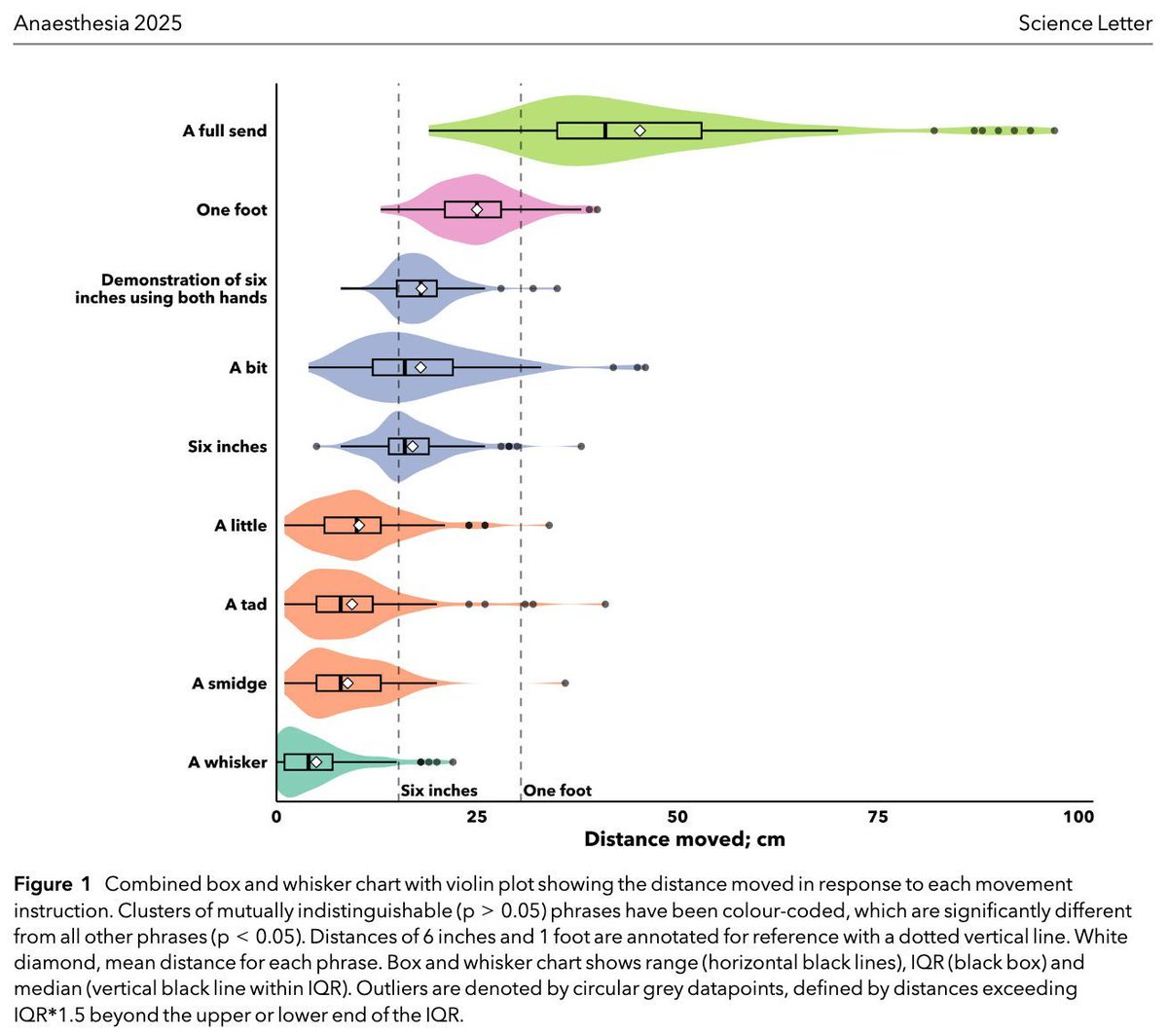
How do you know how far to reposition your patient!?
"Around 6 inches"?
"a smidge"?
Check out RUDOLPH - Rough Units of Distance in Operating theatre Longitudinal Patient Handling
#anaesthesia #MedTwitter
doi.org/10.1111/anae.70108
4
34
97
15,507
Musstdu Daswissen retweeted

15 Dec 2025
IV fluids are one of the most commonly prescribed therapies in hospital...
...yet leadership, education, audit and decision support are systemically absent.
This isn’t a knowledge problem. It’s a systems failure.
New BMJ Open Quality paper calls for national IV fluid stewardship – exactly as NICE intended back in 2013
Time for @Turningthe_Tide
bmjopenquality.bmj.com/conte…
4
25
134
16,931

Musstdu Daswissen retweeted

24 Oct 2025
‼️Danke an alle Schwurbler, Desinformanten und paramedizinischen Scharlatane.
Ach ja, und an die Socialmedia Fake-Grafiken-Impfschaden Deppen.
‼️Oh, und eh ich es vergesse: mein besonderer Dank gilt dem ÖRR für seine unwissenschaftliche Clickbait Fakenews Berichterstattung.
🤡

20
66
332
4,767
Musstdu Daswissen retweeted

24 Oct 2025
Thanks Trump

576
995
10,499
486,824
Musstdu Daswissen retweeted

23 Oct 2025
Was für ein Pech! Epstein-Akten waren im Ostflügel des Weißen Hauses gelagert der-postillon.com/2025/10/os…
21
227
2,118
44,459

The majority of the No Kings protests have dispersed at this time and all traffic closures have been lifted.
We had more than 100,000 people across all five boroughs peacefully exercising their first amendment rights and the NYPD made zero protest-related arrests.
1,391
11,093
110,678
9,824,642
Musstdu Daswissen retweeted

19 Oct 2025
Only in 2025 could the President post an AI video of himself dropping poop from a jet and people still treat it like normal politics. The bar for leadership is underground at this point. We’ve gone from dignity to deepfakes, and everyone’s just laughing instead of asking how insane this has become.
207
207
5,907
216,938
Musstdu Daswissen retweeted

19 Oct 2025
Can a reporter please ask Trump why he posted an AI video of himself dropping poop on me from a fighter jet? That would be great thanks
17,260
6,870
120,686
22,141,643
Musstdu Daswissen retweeted

16 Oct 2025

9
547
3,489
62,186
Musstdu Daswissen retweeted

15 Oct 2025
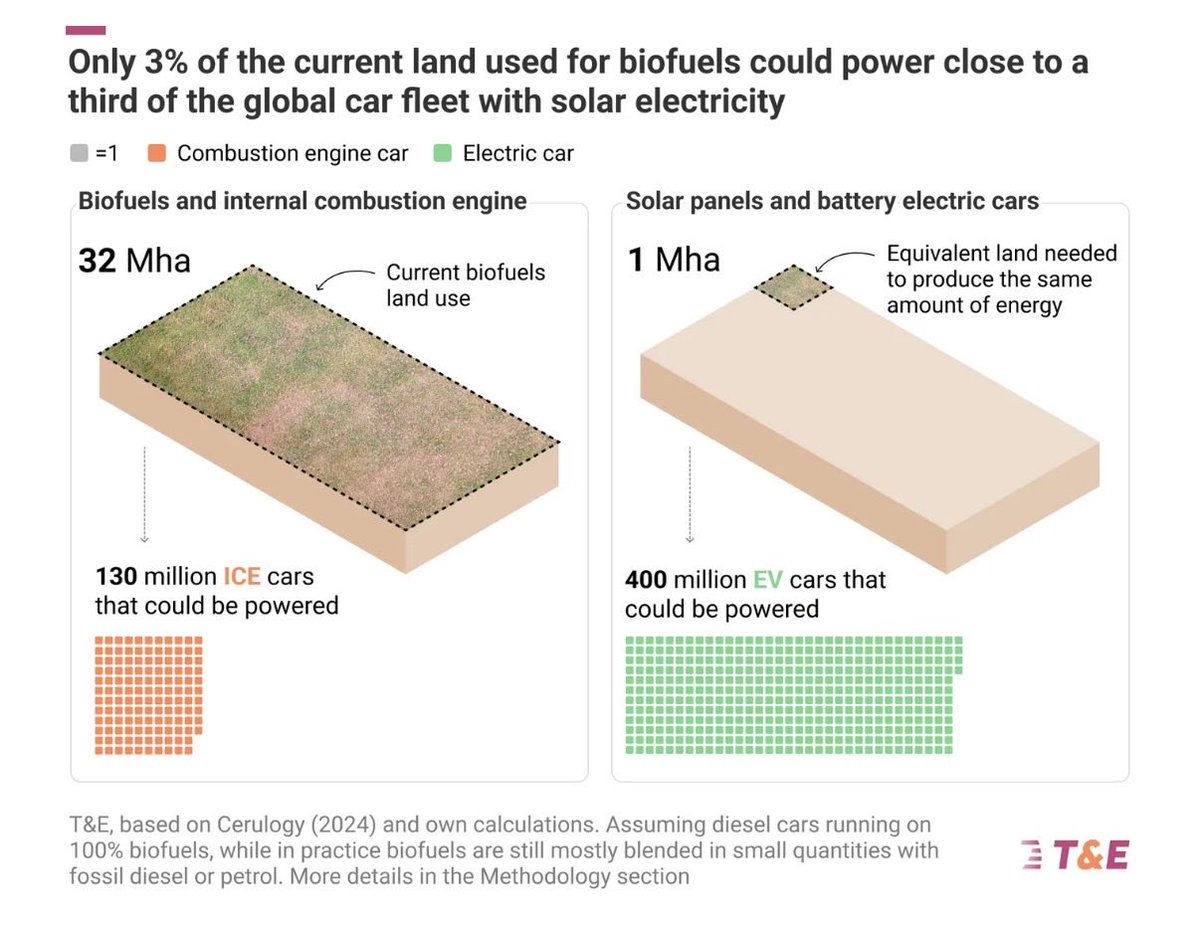
We warned in a report for the government in 2008 that biofuels are not sustainable and recommended to discontinue their use. wbgu.de/fileadmin/user_uploa…
15 Oct 2025

“When crops are burned for fuel, new land can be needed to grow new crops for food or fuel. This can lead to indirect land clearance and deforestation. Staggeringly, biofuels globally therefore today emit 16% more CO₂ emissions than the fossil fuels they replace.”
24
273
700
23,274
Musstdu Daswissen retweeted

10 Oct 2025
a friend of mine in antifa told me that antifa's headquarters is SHEIN and if the company fell the whole network would fall
65
673
13,607
235,576
Musstdu Daswissen retweeted

8 Oct 2025
Vurst - dann nennen wir's doch jetzt einfach Vurst. Das V steht für vegan oder vegetarisch. Vurst ist auch kürzer als "vegane Wurst" oder "vegetarische Wurst". Isch eh vurschd.
190
195
3,195
59,735

In case you wonder about the health effects of *just* 1 night of #sleepdeprivation, in this study of 15 healthy participants (age, 22.3±0.5 y; BMI, 22.6±0.5kg/m2), the researchers found that
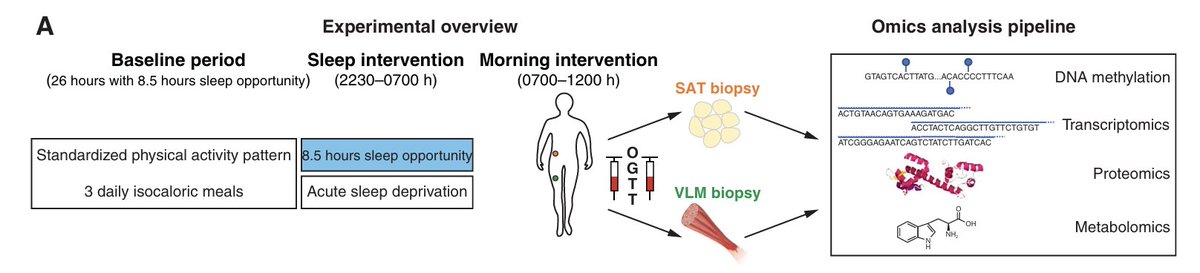
8
49
135
39,083