
Author of: Amida - The Final Prophecy (to be released next month.) An orthodox Jewish baal teshuvah zionist settler that hates labels.
Joined March 2023
- Tweets 22,387
- Following 7,831
- Followers 11,258
- Likes 70,018
1,804 Photos and videos









$RVMD $DRTS = New Pancreatic Standard of Care
What many miss about daraxonrasib’s remarkable median overall survival benefit is that its objective response rate remains only about one third of patients.
In the Phase 3 RASolute 302 trial, daraxonrasib roughly doubled median overall survival versus chemotherapy (13.2 vs 6.7 months), yet the ORR was 31.6% in the overall population.
That distinction is critical.
Daraxonrasib may become the powerful systemic backbone PDAC has been waiting for, but it does not appear to eliminate the primary tumor in most patients. Instead, it may allow many patients to live significantly longer while still carrying residual pancreatic tumor burden.
In pancreatic cancer, that matters enormously.
The primary tumor is not just a passive bystander; it can drive some of the most devastating clinical complications of the disease, including severe pain, jaundice, bile-duct obstruction, bowel obstruction, malnutrition, cachexia, and loss of quality of life.
This is precisely where Alpha Tau’s Alpha DaRT could become highly complementary.
DaRT is not trying to compete with daraxonrasib as a systemic therapy. It is aiming at a different and potentially crucial battlefield: local tumor control.
By delivering potent alpha radiation directly into the pancreatic tumor through minimally invasive EUS-guided placement, Alpha DaRT offers a targeted way to attack the primary tumor while potentially avoiding the cumulative toxicity burden of adding yet another systemic agent.
Early pancreatic data make this thesis especially compelling.
Alpha DaRT has already shown strong local disease-control signals, including reported 100% local DCR in evaluable patients from pooled pancreatic analyses.
If daraxonrasib controls systemic RAS-driven disease and extends survival, Alpha DaRT may become the local-control partner that helps convert longer survival into better survival — not merely more months alive, but more months with reduced local progression risk, fewer tumor-driven complications, and potentially better quality of life.
Together, this could represent a powerful new multimodal approach in PDAC: systemic RAS inhibition to suppress the biology driving metastatic disease, paired with precise local alpha radiation to control the primary tumor that continues to cause pain, obstruction, and clinical deterioration.
Daraxonrasib may change how long patients live. Alpha DaRT may help change how well they live during that extended survival window.
@FDA, are you with us? Daraxonrasib creates time; Alpha DaRT likely makes that time more clinically meaningful.
2
4
553
GB retweeted

Alpha Tau Receives FDA Clearance to Complete Enrollment in #REGAIN Recurrent Glioblastoma Trial and Add Two U.S. Clinical Sites; Early Interim Results Showed 100% Local Disease Control
For full PR - Check the firt comment
1
3
10
238
GB retweeted
2
6
143
GB retweeted

JUST IN: The FDA Approves the $DRTS GBM Trial Completion, with the 3 months follow up showing no signs of the cancer!
“This is a truly phenomenal outcome, no adverse events, no toxicity, and remained with complete response”
3
5
30
114,710
Out of curiosity, what is the “race” of the Muslim Arabs that call themselves Palestinians or, more accurately, members of Hamas?
Follow up question: if I see ISIS beheading Yazidis, am I racist for believing their ideology needs to be removed from the world like a metastasizing tumor?
1
3
338

Herzliya was founded in 1924 as a Jewish moshava on land legally purchased in the early 1920s from Arab owners of nearby villages including al-Haram (Sidna Ali) and Jalil. Yehoshua Hankin and the American Zion Commonwealth handled the buys under British Mandate law—24 years before the 1948 war. It was not stolen through conquest. Modern development there sits on that purchased foundation inside pre-1967 Israel.
2
45
1,014
10,001
It’s a western sickness to put claims of racism on top of the priority list above the survival of the Jewish people.
Get treatment for this because Palestinians are not a race. They’re not even a religion.
@nicolelampert I know you know this so do you also understand why you’ve embarrassed yourself?
1
4
141
How on earth does someone intelligent look at the job Smotrich has done as Finance Minister during a time of existential crisis and war and come up with the hot take: Get rid of Bibi so Smotrich is out so that the hills of the Shomron overlooking a massive portion of global Jewry can be gifted to Hamas?
Get immediate neurological help.
I’m serious. You know you shouldn’t be interfering in Israeli politics since you don’t pay taxes to a Jewish government.
And yet you still speak up in an effort to undermine the defense of the eastern side of Israel.
Clearly, you’re having a bad day.
3
11
182
GB retweeted

Jun 11
מצחיק איך הצלחתם לשכנע את עצמכם ששבעה באוקטובר הוא אשמת הימין. רוב הציבור זז ימינה. כלומר זוקף את האירוע לחובת השמאל. כי בעיני הרוב זו הייתה הוכחה לדבר מאוד פשוט: שהאופטימיזם של השמאל היה מופרך, והפסימיזם של הימין היה מוצדק.
לכן הסיכוי היחיד של הגוש שלכם לנצח, הוא מספיק מפלגות שיעמידו פנים שהן ימין.
אם היינו שומעים לכם, היינו נכנסים כבר ברפיח ואז היינו חיים עכשיו במזרח תיכון תחת הגמוניה (גרעינית) איראנית.
אבל אל תפריעו לעצמכם לשכנע את עצמכם.
30
39
407
3,197
As always, the answer is in the Torah.
Go back to the book of Genesis. What’s the story before we meet our great grandfather Abraham?
The Tower of Babel.
Why does that matter?
Because the generation of the tower hated and feared God. They wanted to fight Him. And then they were dispersed all over the world.
And that’s exactly the world that Jews who represent God on Earth expanded into.
Jew haters hate God. Much easier to torture and murder and lie about His people than Him.
2
2
11
828
GB retweeted

Most people have no idea how practically deployable $DRTS Alpha DaRT actually is. Just read the clinical best practices paper (PMC12036777) and I can't find negative observations when I actively seek them out.
pmc.ncbi.nlm.nih.gov/article…
1
4
4
9
579
GB retweeted
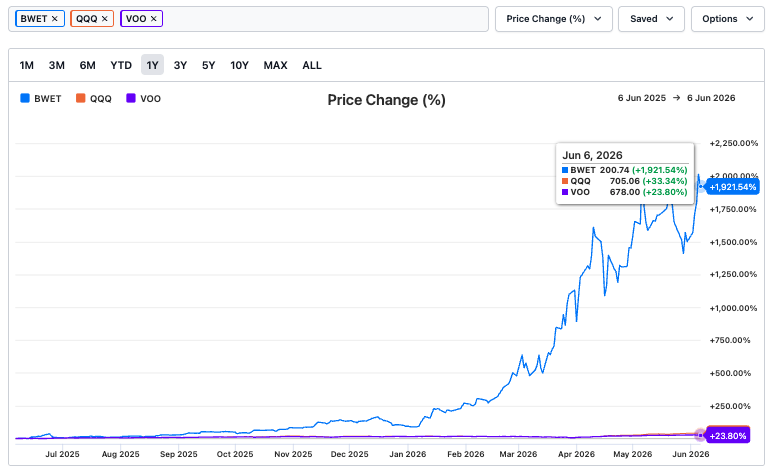
The Billion Dollar Ice Cream Flavor.
How One $DRTS Deal Changes Everything.
6
5
55
599,343
The biggest issue I have with Dave Matthews @davematthewsbnd @davematthewsdmb @AboutDMB is that I remember him from a much earlier time. He seemed to generally care about people.
Wearing the keffiyah of death cult members who filmed themselves raping, beheading, and murdering teenage rave concert attendees tells you there's something really dark and repugnant about Dave's lack of humanity.
He can stand up and claim it's not antisemitism but that's not the point at all is it?
Teenagers go to raves and concerts and they enjoy music. I did it for DMB when I was younger and kids today pay a lot more but they enjoy going as well.
Now, imagine that nearly 1,000 jihadist death cult members, most of them drugged up, come running through the rave shooting, stabbing, and murdering the panicked attendees who have no where to run in the open field. They are chased down and raped (both men and women) and they are beheaded (clearly seen on the video.) These same sadistic bastards will go through porta-potties to put bullets into the heads of panicked, screaming, crying teenagers who only wanted to dance.
This is happening at the same moment that their accomplices are burning families alive in nearby towns. And if they're not raping and murdering people, they are dragging young people away to either murder later or to hold hostage in underground tunnels.
And Dave Matthews puts on their keffiyah and announces his solidarity with them.
Where is the humanity? Where is the decency? Where is the moral outrage? You don't get to support monsters who murder concert goers and then turn around and claim you have Jewish friends - at a concert - and escape from the reality that you're not a decent human being.
It's really quite simple and anyone who wants to "whatabout" with the Jews or "whatabout" with Israel or "whatabout" with anything else has missed the point.
If you own any Dave Matthews Band material, my suggestion is to burn it, the same way his heroes burned alive the people that just wanted to dance to the music.
1
2
20
464
Dear President Trump. @POTUS
In the Middle East, you must speak the language.
The language is speaks is strength.
You can't demonstrate it through the air.
You can't demonstrate it on the water.
The only way to speak the language is via land.
TAKE KHARG ISLAND.
American must not appear weak or it will embolden the Iranian regime and their death cult followers.
Signed,
Civilization
4
17
294