
Interventional Cardiologist at @TridentHealthPR. Trained @WeillCornell @MountSinaiNYC @GUMedicine #radialfirst #TAVR Not medical advice. Views my own.
Joined March 2014
- Tweets 3,326
- Following 1,018
- Followers 1,293
- Likes 21,789
364 Photos and videos









Pinned Tweet

30 Oct 2024
We will demand that everyone admitted to the hospital has quality measures checked. Their blood pressure will be measured at 4 am! Blood thinners for all! Everyone will starve after midnight!
Will that help the patients, sir?
2
2
19
2,245
Patrick M Looser MD retweeted

Jun 13
So why am I lashing out at the AMA, an organization I was a proud member of and worked very hard for when I was at JAMA?
The X-world will learn, as I release documents regarding my litigation against them for firing me for what has been determined by the appropriate agencies as a 'civil rights violation.' You can use your imagination what that means in the context of their being all-in with DEI at the time.
They claimed that I denied the existence of racism in medicine - the exact opposite of what I said in a podcast the AMA edited and published after review by my supervisor. I had no control of that process. The courts agreed with my claim of libel and defamation, a decision the AMA appealed and lost in a unanimous decision. Along the way the courts described the AMA as disingenuous. An organization that holds itself out as representing Americas Physicians to policy makers should not engage in libel and if they do, they should be disqualified from representing us.
You have not heard much recently because the AMA asked the courts to keep the proceeding secret-They do not want the physician community to learn how they do business. However, the closed nature of the documentation is over, and I'll be able to share what I learned during the proceedings. It's not pretty and it shows how the AMA actually functions.
This is not what I wanted in life. I am an academic surgeon. I have no interest in politics. But the AMA destroyed my career and reputation for capricious reasons. I cannot let that stand. The AMA needs to be held accountable, no matter how wealthy they are compared to me.
66
279
1,159
40,688
Patrick M Looser MD retweeted

Great to join @ron_waksman, @DorBen , @MdSatler and @MedStarWHC @MedStarResearch at the DMV Case club to present a great case we did on Redo TAVR of Lotus valve (see attached) with high risk of coronary obstruction.
@CRT_meeting runs a great show!
1
3
10
821
My mayor’s Muslim
My bagel’s Jewish
My cream cheese is chive
KNICKS IN FIVE
31
Patrick M Looser MD retweeted

Hi Dave — thank you for the kind words on our NATURE-CT publication.
You asked a fair question: how would Keto-CTA look if we only looked at the people with CAC ≤ 100, just like we did in NATURE-CT? Any comparison using the original KETO-CTA data is no longer valid. The paper was formally retracted by JACC Advances at the authors’ own request. The retraction notice is here:
jacc.org/doi/10.1016/j.jacad…
Even setting the retraction aside, the plaque progression rates in the keto/LMHR group were much higher than the healthy rates we reported in NATURE-CT:
~18.9 mm³ median NCPV increase vs ~4.9 mm³ annualized in NATURE-CT.
This faster plaque progression is the adverse effect directly linked to the very high ApoB/LDL-C levels caused by the keto diet.
The public should be warned that this is likely a dangerous approach, especially for those who show rapid plaque progression as defined by OUR study.
Standard of care guidelines from the ACC and AHA recommend lowering ApoB and LDL-C to reduce heart disease risk. They advise against allowing sustained high levels like those seen in keto dieters. Caution is essential.
We can now define and treat rapid progressors even before calcium is present, as documented in our First-in-Human paper: jacc.org/doi/10.1016/j.jacca…
This is further supported by performing serial imaging—an approach we first described in 2013 in Atherosclerosis: atherosclerosis-journal.com/…
We subsequently confirmed this over 13 years using current technology in our 2022 paper on serial analysis of coronary artery disease progression by AI-assisted coronary CT angiography: pubmed.ncbi.nlm.nih.gov/3643…
We all agree that baseline plaque strongly predicts future plaque. But decades of research also show that sustained high ApoB/LDL-C drives atherosclerosis progression.
In this group who chose the keto diet often against "standard of evidence advise", close lipid monitoring and careful risk assessment are essential. Keto is likely harmful to arteries for most people, even if some tolerate it well.
Looking forward to continuing open discussion. Best
Ron Karlsberg MD FACP FAHA FACC MSCCT
(Lead author, NATURE-CT)@realDaveFeldman @DLBHATTMD @MichaelAlbertMD @CMichaelGibson @RonBlankstein @chamath @ethanjweiss
RETRACTED: Longitudinal Data From the KETO-CTA Study: Plaque Predicts Plaque, ApoB Does Not
jacc.org 9
22
77
12,612
Patrick M Looser MD retweeted

4
16
48
43,192
Patrick M Looser MD retweeted

How many of you also got an early Christmas gift in the mail today?!😡

11
3
42
6,482
Patrick M Looser MD retweeted

May 26
What’s your approach? ACS, focal subtotal oLAD. Lesion persists post 400 IC nitro…(Pay close attention to the size). #ACCFIT #cardiox
@jedicath @evandrofilhobr @nyalborgesmd @realarainmd @SripalBangalore @mmamas1973 @mirvatalasnag
@Hragy @DrRajeshG1 @mandeep_mayo @djc795 @mornei2011 @rickytiago @ziadalinyc @stefan_harb @drandrewsharp
21
13
58
11,378
Patrick M Looser MD retweeted
Nice Redo TAVR case with @HMHNewJersey @vandanMD @PWengrofskyMD
TAVR done 4 yrs prior at OSH (not me!)
Pt furious for not getting SAVR after reading @WSJ
(in fairness, his LVEF was 20% at that time)
Prior 34mm Corevalve (large aortic annulus/bicuspid at baseline). Implant at N6 Sizes to 23mm vs 26mm... we used 26mm Sapien and expanded well
#tavr
4
12
1,521
Spent an hour on the phone lobbying for an “expedited review/appeal” which takes 24-72 hours. For a procedure that is FDA approved and I was told is “off label” and “needs to be done in the context of a clinical trial.” We need prior authorization reform now.

We’ve hit a new low @Humana
FDA approved procedure denied… by an ED physician. Not a board certified cardiologist. Not a board certified cardiac surgeon.
For shame.
3
1
14
4,331
We’ve hit a new low @Humana
FDA approved procedure denied… by an ED physician. Not a board certified cardiologist. Not a board certified cardiac surgeon.
For shame.
17
13
118
24,572
Patrick M Looser MD retweeted

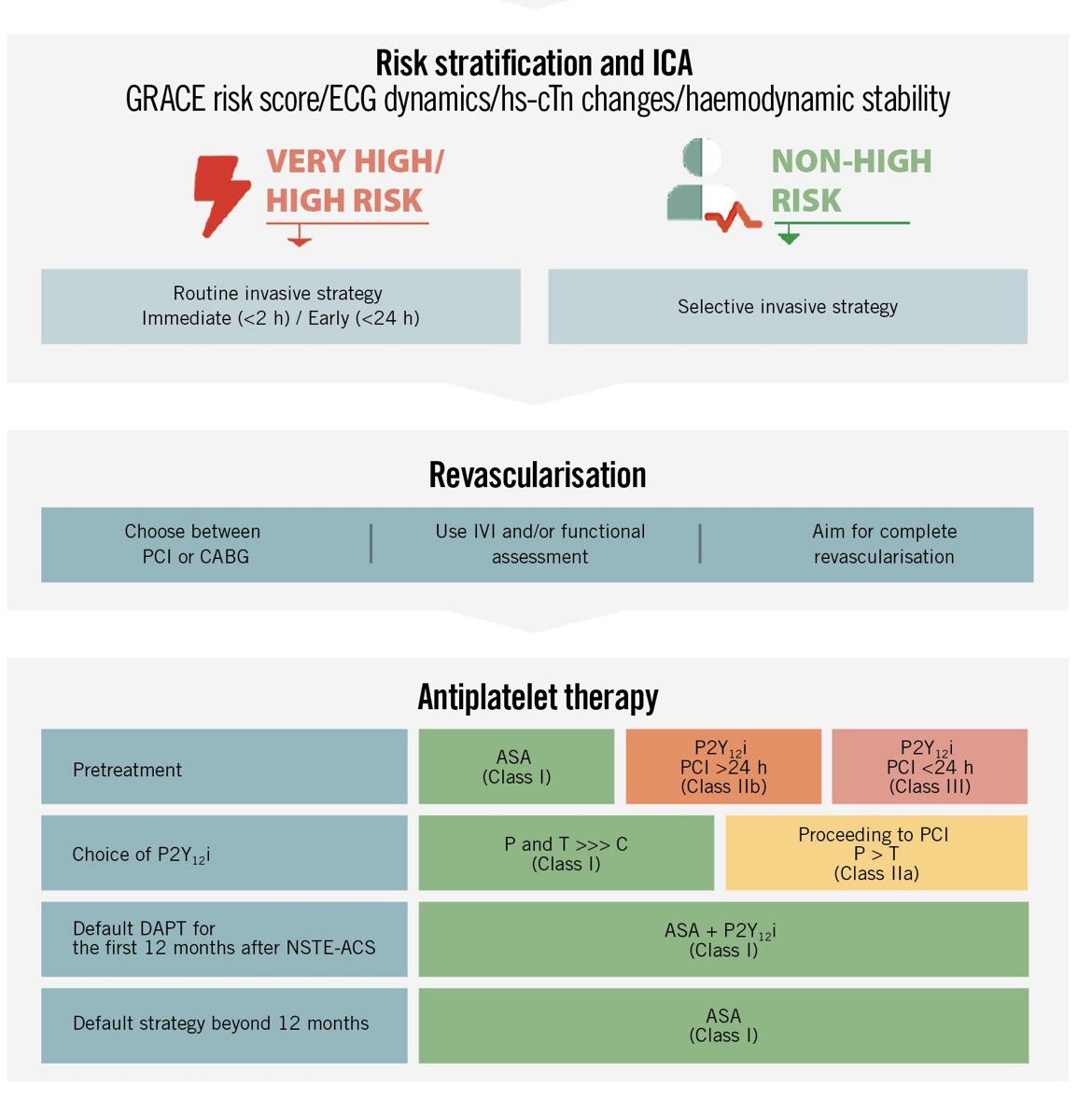
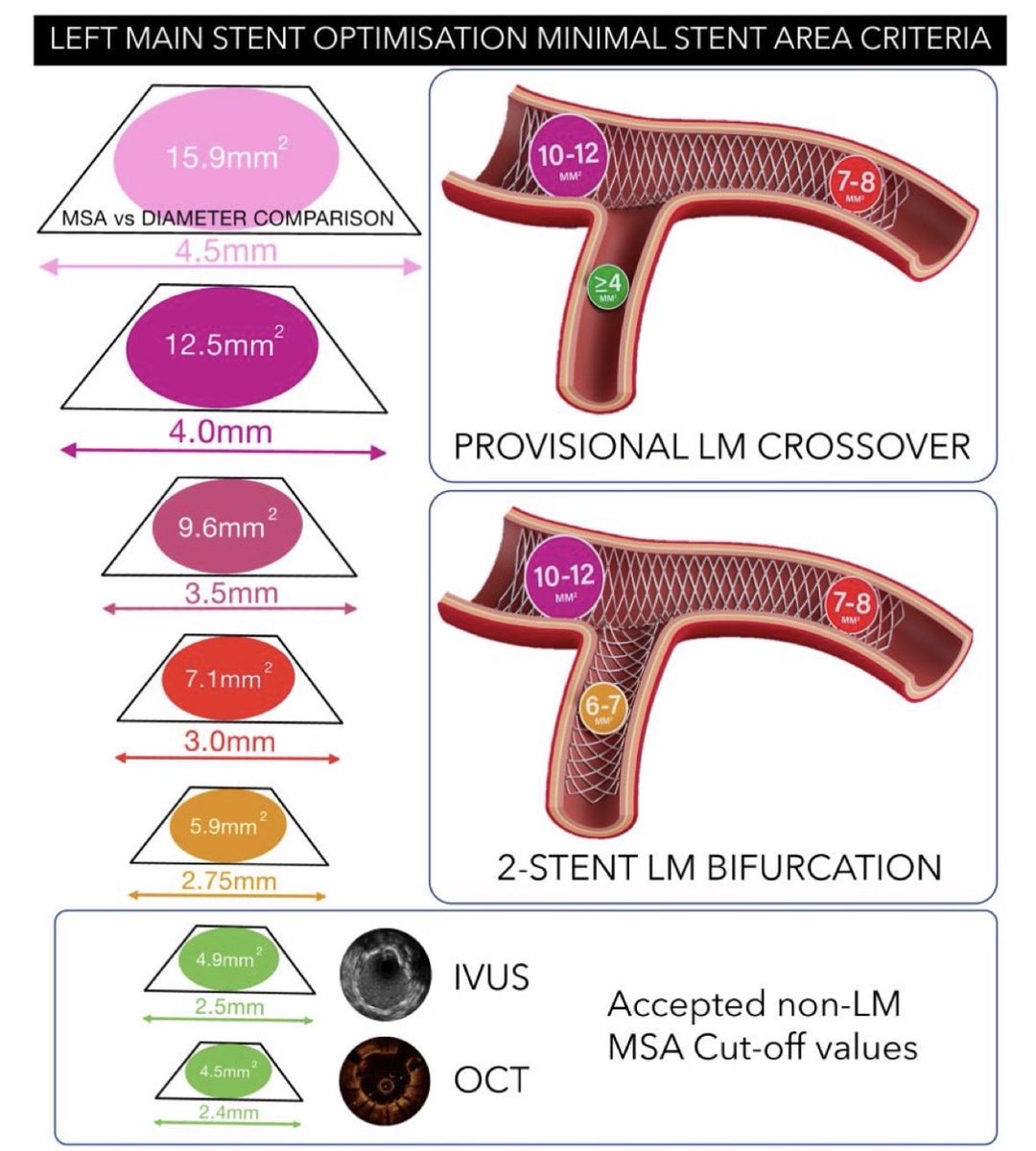
After 2 years of work, the 🇪🇺 consensus on #IVUS #OCT use in #LM #PCI is now published in #EHJ. Great international collaboration coordinated by #EBC and #EAPCI !!!
It includes fantastic practical images that can be hung on the walls of all cath labs…
doi.org/10.1093/eurheartj/eh…
2
82
258
13,897
I’m not saying the answer is coronary angiography. But what is the appropriate ischemic evaluation to see if the patient is a candidate for IC anti arrhythmics?
May 17

That’s another thing that drives me bananas: sending pts w AF for coronary angiography. Dumb. Dumb. Double dumb.
2
1
721
Patrick M Looser MD retweeted

May 12
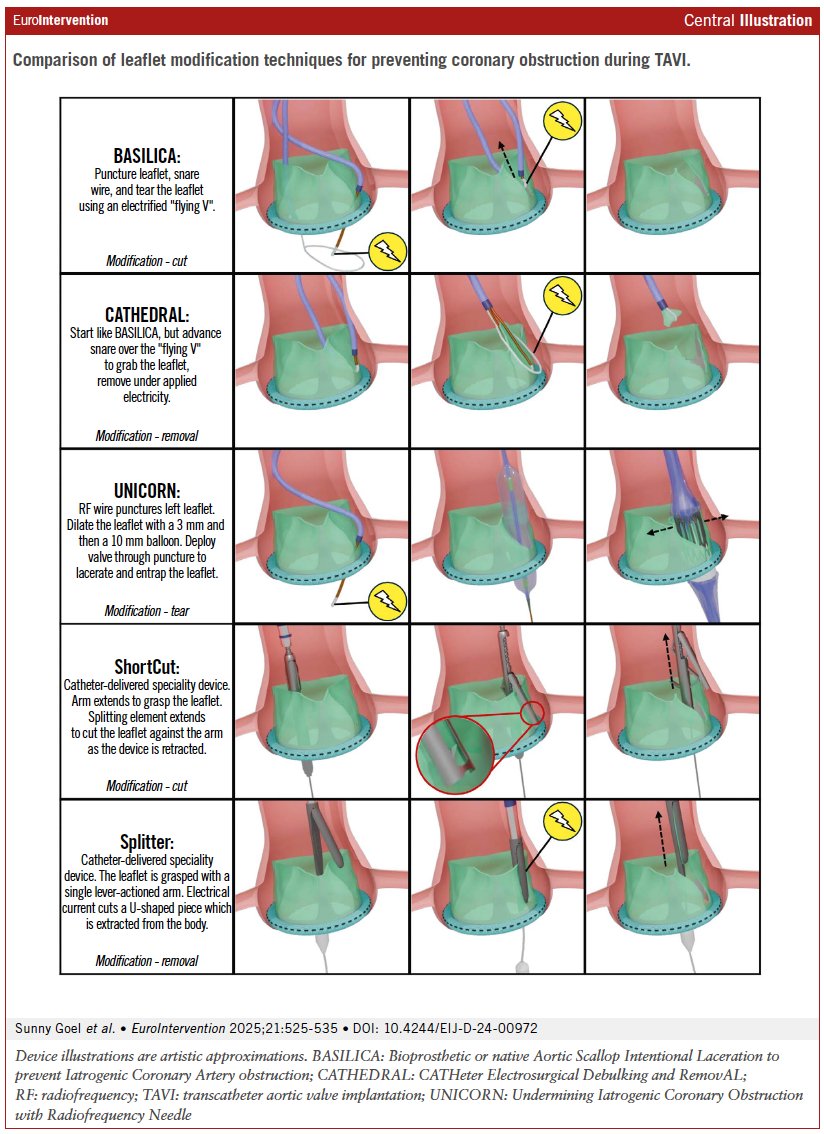
As TAVI expands to younger and more complex patients, preventing coronary obstruction is becoming increasingly important.
This review summarised evolving leaflet modification strategies — from BASILICA to ShortCut and UNICORN — aimed at improving procedural safety in high-risk TAVI and valve-in-valve interventions. #CardioTwitter #TAVI #BASILICA #StructuralHeart
eurointervention.pcronline.c…
@sunnygoelmd @GilbertTangMD
1
65
126
8,419
Pt on GLP1 after a significant weight loss: “I feel hopeful for the first time!”
3
188
Important commentary.
May 4

We Can’t Compromise Our Values for RVUs.
I often hear from a number of docs expressing frustration that "patients don't listen to them". Well.... that's okay!! Let’s dive into this…
One of the hardest conversations in this profession is between the patient who wants something done and the surgeon who knows that something isn't the answer. PTs and docs tell me regularly that they feel stuck, that they've explained the evidence, and the patient still wants the procedure. What do you do?
My answer is that our job is to educate and inform. Not to convince. We can explain what the research shows, what the risks are, and what rehab is likely to accomplish that surgery won't. We can be honest and direct about our clinical judgment. What we cannot do, and shouldn't try to do, is override a patient's autonomy. Informed patients get to make their own decisions. That's not a failure of communication. That's medicine working correctly.
I like to operate. I became a surgeon because I find it meaningful, and I'm decent at it. When surgery is the right answer, I don't hesitate. What I find genuinely puzzling, after all these years, is when a patient tries to convince a knee surgeon with 30 years of experience that they need an operation, and every instinct that surgeon has developed over those 30 years is telling them otherwise. That clinical intuition exists for a reason. It should be trusted, not negotiated away.
The harder version of this is the surgeon who says: If I don't do it, someone down the street will. And that's true. But I can only answer for what I do in my operating room. If I believe surgery might genuinely help, I'll recommend it, and I'll do it. If a patient has moderate arthritis and wants me to clean out a joint that the evidence says won't benefit from cleaning out, I won't do it. Not because I'm judging the patient. Because I can't compromise my principles for RVUs.
This isn't self-righteousness. It's the only way I know how to practice medicine and look at myself in the mirror. The patient may find someone else. That's their right. My obligation is to tell them the truth as clearly as I can, and then let them decide.
1
1
657
Patrick M Looser MD retweeted

2
1
8
599
Patrick M Looser MD retweeted

Apr 30
34 life lessons after turning 34 today.
Jk, this game (life) is simple:
> Find the person that brings you peace/happiness and marry them
> Have kids
> Aim to invest $0.20 of every $1 you earn
> Workout 3-4x/week
> Learn to cook
> Find 1-2 hobbies outside of work/money
16
6
204
18,559
“The burden of proof therefore lies with those claiming that LMHRs somehow escape this biology—that they are an exception to an extremely well-established rule. Two poorly designed observational cohorts are hardly sufficient to counter this mountain of evidence...”
Apr 26

Peter has the patience that I do not. peterattiamd.com/there-is-no…
142
Patrick M Looser MD retweeted

Apr 26
Peter has the patience that I do not. peterattiamd.com/there-is-no…
10
5
54
8,420
Patrick M Looser MD retweeted

Apr 24
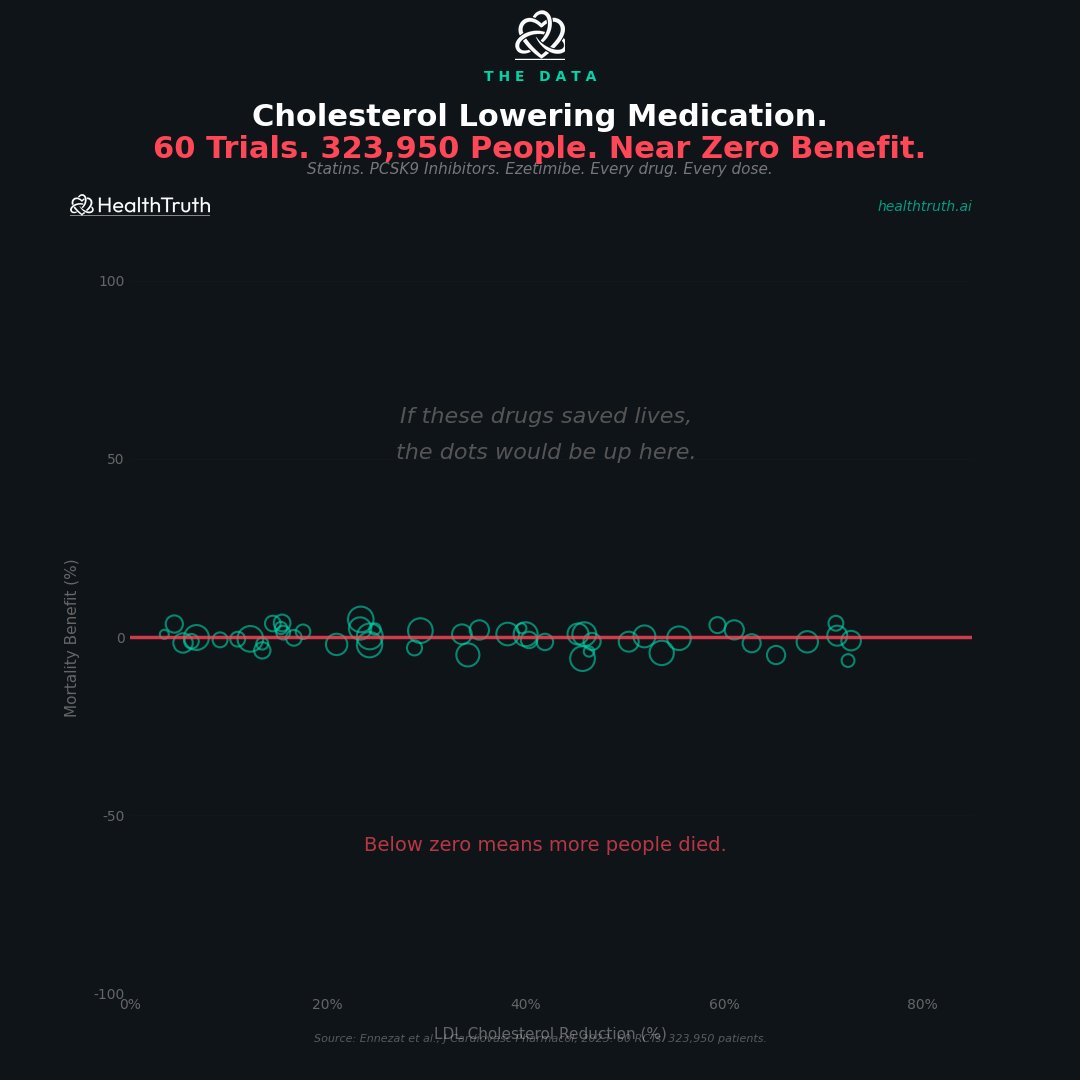
This chart is a great example of how you can make 300,000 people disappear with a bad question.
Let’s be very clear—because you deserved that clarity at 52 after a heart attack:
1) The wrong endpoint is doing all the work
They’re plotting LDL reduction vs all-cause mortality across trials.
That sounds reasonable—until you realize:
Most statin trials were not powered for all-cause mortality
Many include low-risk or mixed populations
Follow-up is often too short to show mortality differences
So the “flat line” is not surprising. It’s expected.
2) This ignores the outcome that actually matters in these trials
Statins were never primarily about “living forever.”
They reduce:
Recurrent heart attacks
Strokes
Cardiovascular death (in higher-risk groups)
If you collapse everything into “all-cause mortality,” you dilute the signal with:
cancer deaths
accidents
unrelated disease
That’s not honesty—that’s statistical camouflage.
3) Secondary prevention (you) is a completely different universe
You had a heart attack.
That puts you in secondary prevention, where the data are not subtle:
Statins reduce major vascular events ~20–25% per mmol/L LDL drop
Clear reductions in recurrent MI and stroke
Mortality benefit shows up more consistently in higher-risk patients
This isn’t fringe—that’s decades of consistent evidence.
4) Mixing drugs = muddy conclusions
They lump together:
statins
PCSK9 inhibitors
ezetimibe
Different mechanisms, different trial designs, different populations.
That’s like averaging antibiotics, chemotherapy, and aspirin and concluding “medicine doesn’t work.”
5) The visual trick
The graph implies:
“If LDL mattered, the dots would go up.”
No.
That assumes:
identical populations
identical baseline risks
identical durations
None of which are true.
It’s a correlation plot across heterogeneous trials, not a causal test.
Apr 24

My doctor put me on a statin after my heart attack at 52.
I trusted him. I took the pill. I never asked a question.
Then I found this study. 60 clinical trials. 323,950 people. Every cholesterol lowering drug ever made. Statins. PCSK9 inhibitors. Ezetimibe.
They measured how much each drug lowered LDL cholesterol. Then they measured whether people lived or died.
The line is flat.
It did not matter if they lowered LDL by 10% or by 70%. The death rate did not change. In some trials people died more.
323,950 people. Near zero benefit. Published in the Journal of Cardiovascular Pharmacology. 2023.
Nobody showed me this chart. Not my cardiologist. Not my pharmacist. Not the drug rep who visited my doctors office every month.
I had to find it myself. After the heart attack.
9
10
57
7,210