
Crit/Care research physician. CoAuthor of “The Physician’s War” The Battle between Physicians & Pathological Consensus a.co/d/9vm6vEr
Joined August 2012
- Tweets 8,951
- Following 879
- Followers 1,341
- Likes 2,633
653 Photos and videos








Pinned Tweet

21 Sep 2024
The story of pathological consensus and shortcutting the RCT method of Hill/Fischer with the Petty/Bone science. The lumping paradigm.
The Physician’s War: The Story of the Hidden Battle between Physicians and a Science Based on Pathological Consensus a.co/d/8OtJlVk
4
10
50
10,784
May 21
Discussion of subgroup gates at datamethods.
It would be great to have input from CI exerts.
@soboleffspaces
@eliasbareinboim
discourse.datamethods.org/t/…
1
3
219
May 13
Come contribute to the discussion of causal inference (CI) at Vanderbilt Datamethods.
discourse.datamethods.org/t/…
2
135
May 12
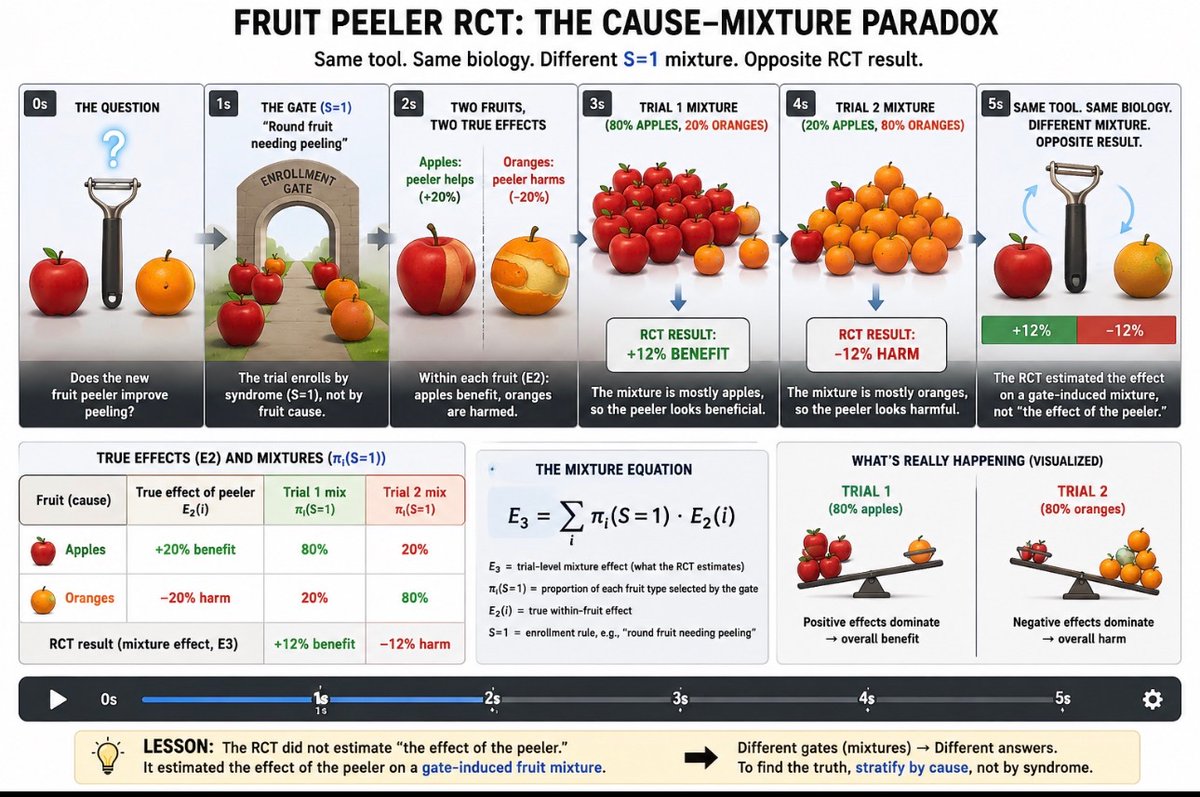
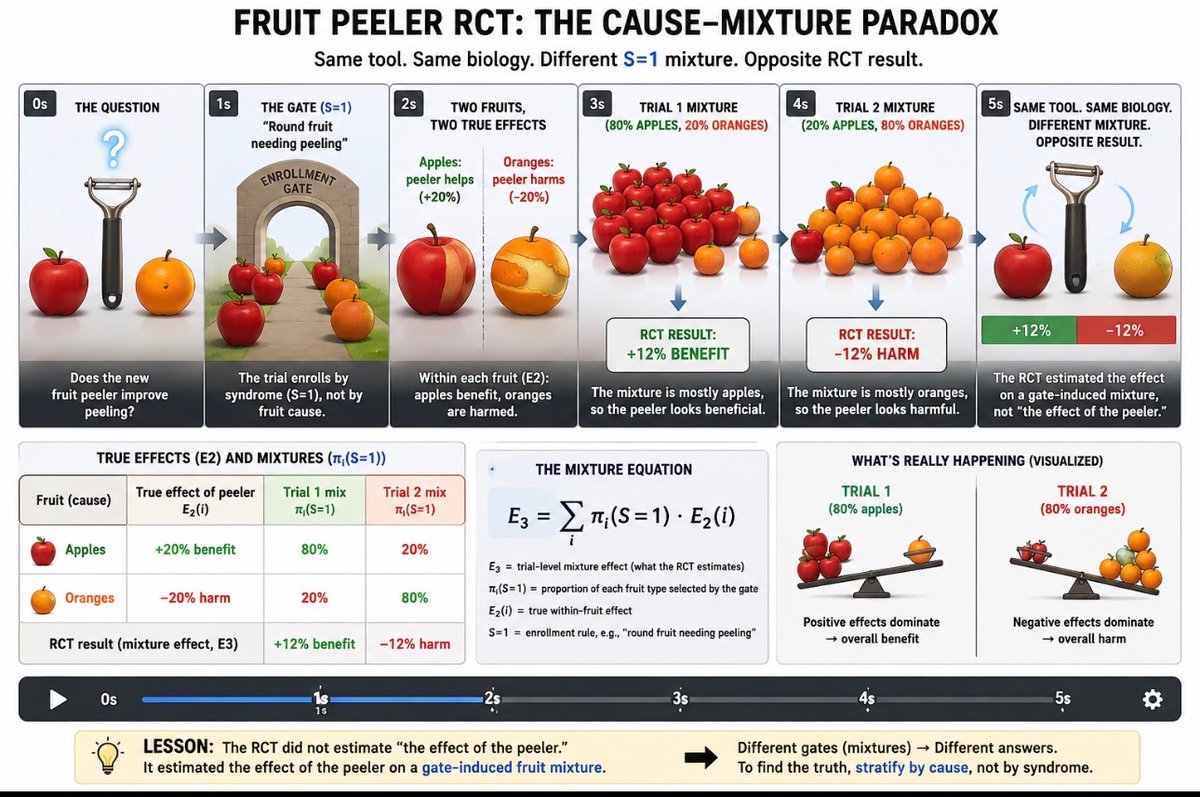
This simple graphic explains ~4 decades of RCT failure and reversed guidelines for harm in critical care. @CritCareReviews @MarionKCampbell @yudapearl
2
3
15
599
May 12
There is a profound resistance to structural causal modeling and structural thinking within parts of modern statistics, a striking anomaly in science.
The result has been that simple structural mistakes cause decades of waste, reversals, and harmful RCT-derived guidelines.
Yet despite repeated failures, the underlying framework remains unquestioned because the RCT itself is an institutional icon beyond structural critique.
1
2
144
May 12
It is frustrating to have to reduce complex structural pathologic methodology to elementary explanations, but the degree of institutional conditioning around the RCT paradigm requires a return to the most simple explanations of the most basic principles which were unknowingly violated, institutionalized and remain hidden within complex mathematical embellishments.
2
106
Apr 25
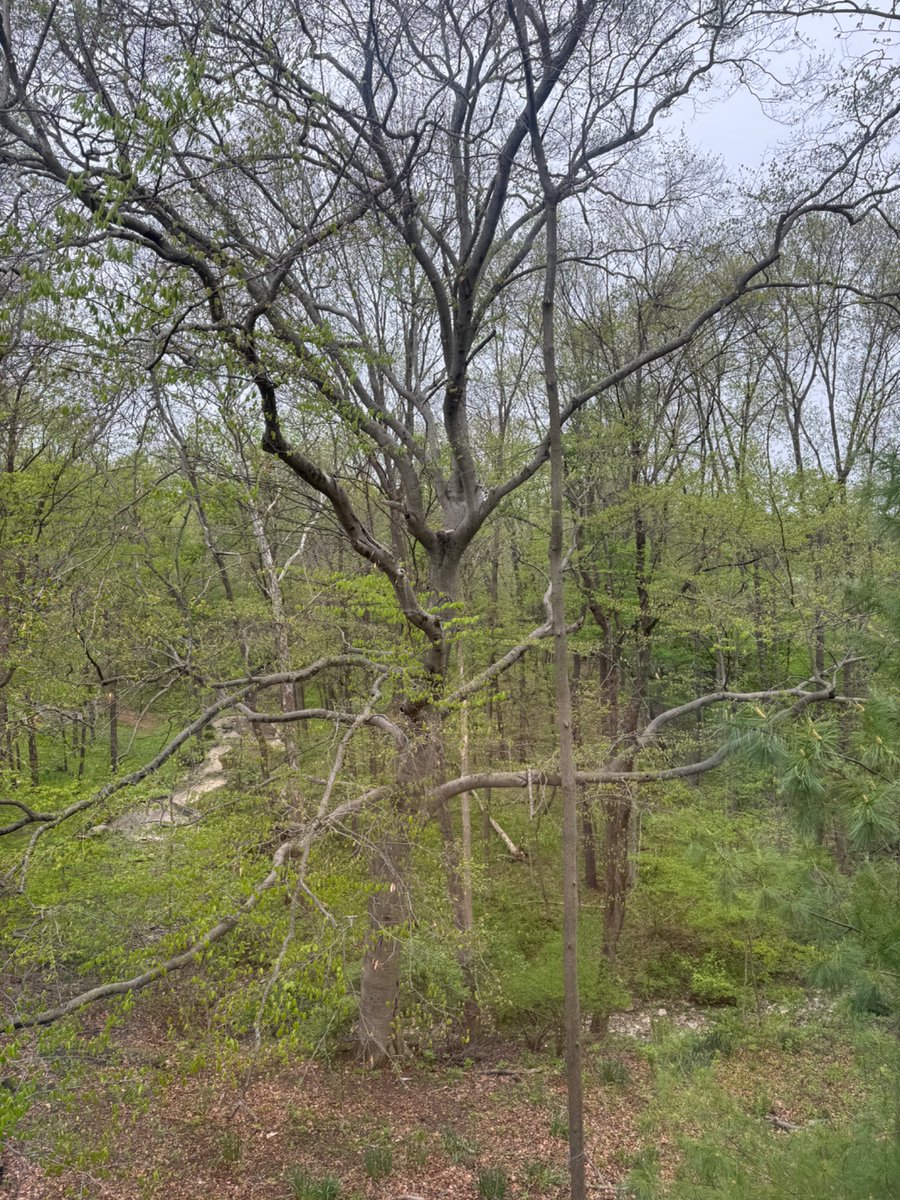
Winning the best mother award.
Large hailstorm a few days ago. Courageous Red Shouldered Hawk Mother protecting her eggs laid in Beech tree near the house. ~Dime size hail
1
5
157
Apr 24
One naturally wonders why a Turing Award winning framework, as articulated by @yudapearl, has no explicit constraints on the admissible S. Or are they provided and I missed it?
I suspect that no one anticipated that investigators would routinely construct selection rules for RCT and OS that generate synthetic data generating processes SDGPs as they do today.
If such pathological derivations of S had been anticipated, where the selection rule does not correspond to a coherent data-generating process, then explicit constraints on admissible S might have been formalized. Hopefully a formalization of S will make it into the Book Of Why II .
1
114
Apr 21
“RCTs are causal by design” is a popular refrain. It’s succinct and persuasive… but is it true?
Functionally no. Not in the sense that clinicians actually require. Critical care physicians have learned this the hard way over 4 decades not to trust that common slogan.
Physicians don’t just care about “technical causality”. They care about “functional causality”. But what is functional causality?
A causal effect is functionally causal if it supports reliable and durable guidelines applicable to real patients, because the estimated effect reflects a mathematically robust, stable, transportable biological (eg physiological) response to intervention because the target during the trial was, and in the population is, a real (non-synthetic) biological data generating process (DGP).
This is “guideline-level causality” (GLC)
The structural gap is that an RCT identifies:
P(Y |do(X), S = 1)
But clinicians need something closer to:
P(Y |do(X))
So these are only “functionally equivalent” if:
The trial selection S corresponds to a biologically (pathophysiologically) coherent target captured by S and this is where the slogan fails because CONSORT does not assess this requirement.
This is true because S=1 is ambiguous and as broad as the statistician and trialist desires under CONSORT. S can select a synthetic data generating process (SDGP) such as a the latest biologically cause and disease agnostic consensus derived threshold triage.
Bottom line:
“RCTs are (technically) causal by design, but even well constructed RCT, as defined by CONSORT they are not necessarily clinically useful or safe to transport by design.”
@f2harrell @yudapearl @soboleffspaces @eliasbareinboim
2
2
382
Apr 18
@yudapearl I’m concerned that accepting “RCTs are causal by design” without qualification underplays the role of SCM and my goal of its incorporation into CONSORT.
Randomization identifies P(Y | do(T), S=1), but it does not ensure that S=1 defines a stable causal target. Interrogating the selection mechanism with SCM seems essential at the design stage to distinguish cause-isolating designs from mixture-inducing ones and to assess transportability.
Progress on RCT design and reporting reform will likely be delayed unless the causal inference community engages with this issue.
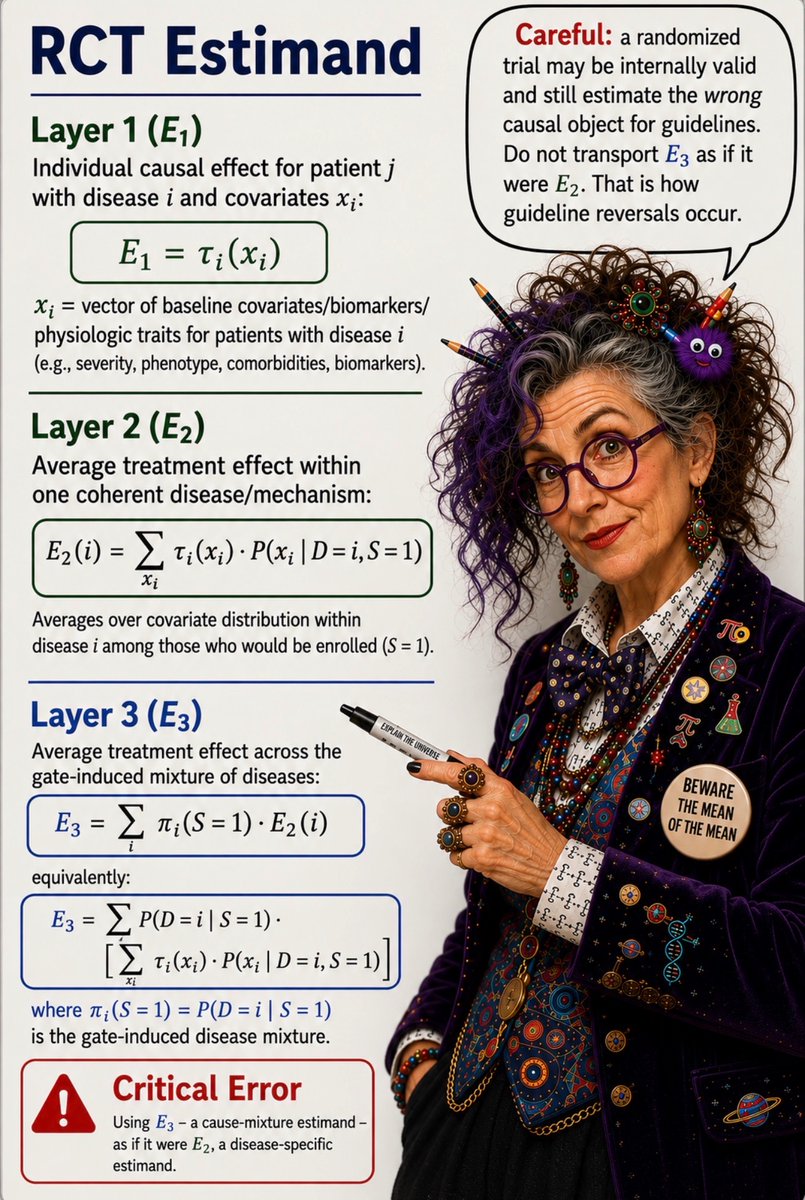
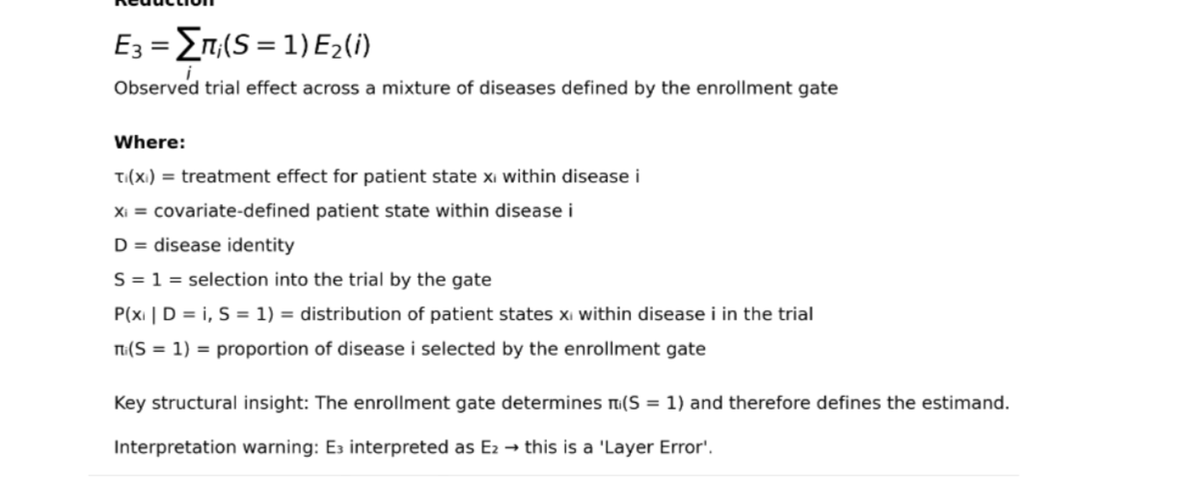
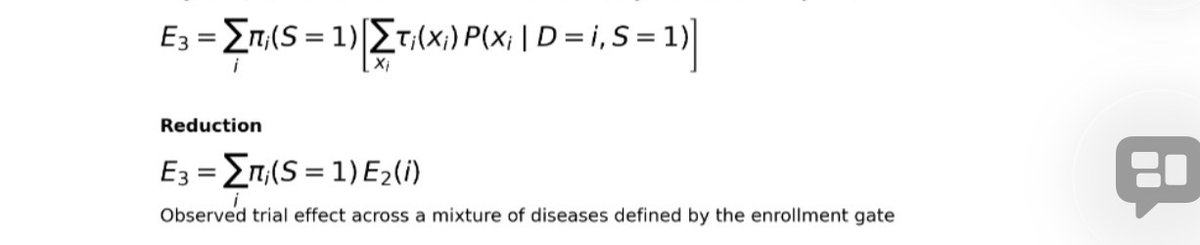
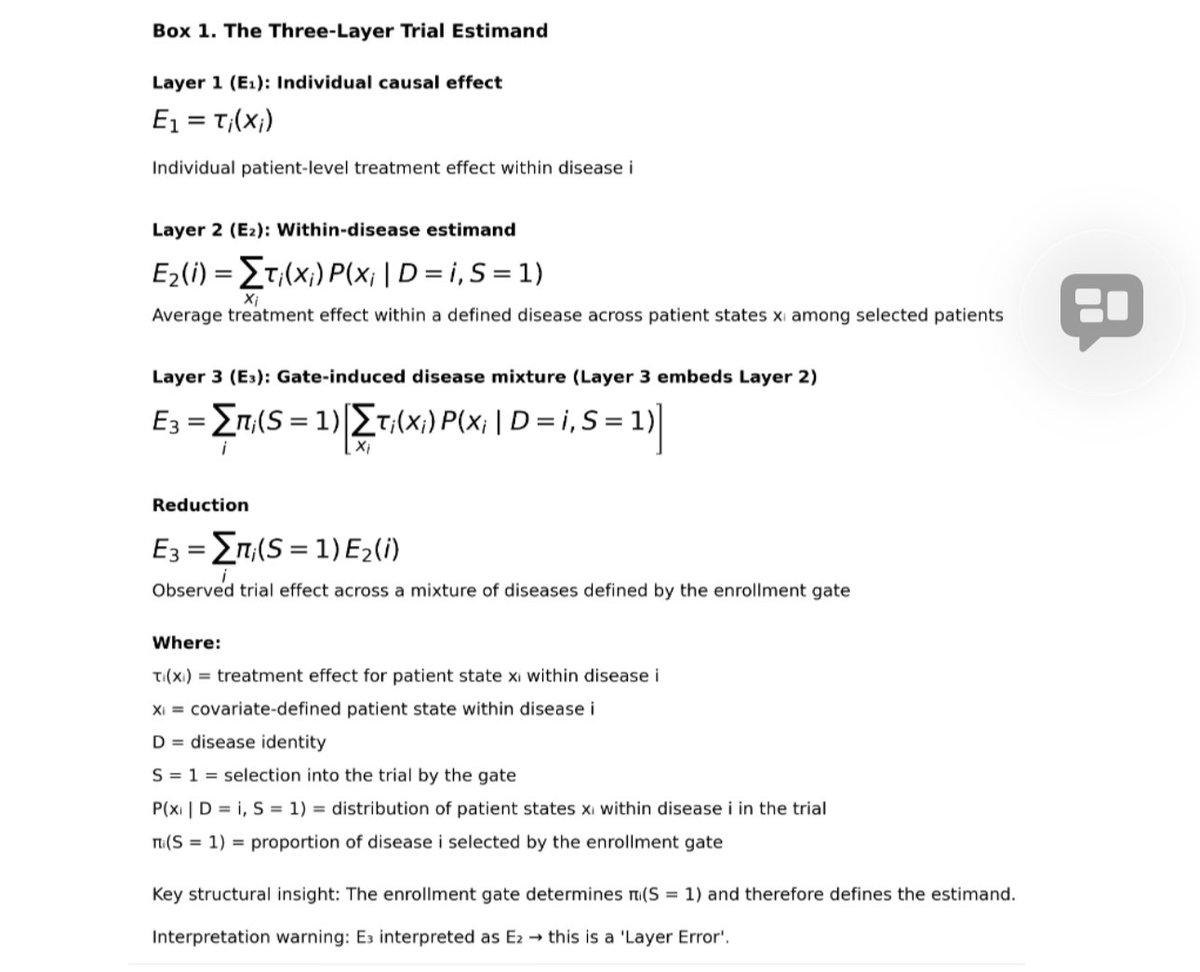
The emerging recognition of the third-layer estimand provides a natural entry point for SCM to inform trial design and ensure that estimands correspond to stable, transportable causal targets.
The causal community should seek to understand “Layer Error” and the generation of synthetic data generating processes.
Apr 10

I agree with almost all claims of this paper, with the exception of this: "Practitioners of causal calculus propose that it to be a necessary ingredient of virtually every causal inference including that from tightly controlled randomized studies." All CI practitioners that I've met would agree that if we have a well conducted Randomized study, you can get causal effects directly from the experiment -- no need for causal calculus. Such needs surface when you want to do more than just find one causal effect. For example, suppose you want to combine findings of two randomized studies, conducted on different variables and perhaps diverse populations. I have not seen a single mortal capable of doing it w/o the calculus, and that includes mortals who claim to be doing "meta analysis".
There is also a foundational problem that is answerable only via the calculus: "What guarantees us that randomized experiments yield causal effects.?" The @Bookofwhy provides a formal proof, which I haven't seen elsewhere, not even in Fisher. But this should not bother practicing trialists, they can benefit from the proof and pretend they don't need causal analysis because, obviously, RCT's give us causal effects. Done. As a computer scientist, I couldn't take it for granted.
1
1
222
Apr 18
In case it’s helpful, here is the preprint currently under review. It is part of a three-part series examining the history of RCT design, estimand structure, and implications for transportability. I would very much welcome feedback, and I think it may be of interest to your students and colleagues. This article is part of a grand ongoing effort to reform the RCT design process by integrating SCM.
zenodo.org/records/19582118
1
120
Apr 16
Once you have seen “the third estimand”you can’t unsee it.
discourse.datamethods.org/t/…
1
1
187
Apr 16
open.substack.com/pub/thetho…
This is a sad tail by @RafaelOliveLeit
The relentless study of “synthetic data generating processes” (SDGPs)
Here, they remain, trapped in the third estimand, confined within synthetic science space.
1
99
Apr 14
The latest preprint (now in review) of the "RCT transport trilogy" examining safety consideratioons of transportability of RCT gates to clinical guidelines.
This one introduces the "layered estimands" and in particular the "third estimand" as derived from RCT of "synthetic data generating processes" (SDGP) and the associated production of the "cause-mix paradox".
@yudapearl @soboleffspaces @eliasbareinboim
doi.org/10.5281/zenodo.19581…
1
1
148
Lawrence Lynn retweeted

Mar 24
I’ve attended to ISICM, AHA, brazilian Congress and now to the CCC from SCCM and i have to say: our only hope is DEFINETELY the H&R. The only place you will hear about applied (and correct) physiology, physiologically-based resuscitation skills and POCUS. Truste me! Dont miss this congress! @ThinkingCC @KiranRikhraj
6
22
5,125
Mar 23
“SYNTHETIC DEBATE” is a form of pseudo-scientific argument that occurs when people debate within a shared but invalid premise, rather than questioning the premise itself.
A synthetic debate:
-Assume a flawed framework is true (e.g., a cause agnostic RCT with a guessed triage gate is suitable for safe transport to a guideline.
-Focuses discussion on secondary issues within that framework (p-values, effect sizes, subgroup analyses, etc.)
-Creates the false appearance of rigorous scientific disagreement
-But never engages the underlying causal error, so no real knowledge is generated.
Look we know the @SCCM thought leaders can’t step away, but you have no right to hide this from your fellows with “synthetic debate”. They should make up their own minds lest they wind up indoctrinated like their mentors were, by Petty & Bone’s simple idea of the modified triage threshold gated RCT.
@SCCM2026 @ChrisCarrollMD @Paul_Wischmeyer @nickmmark

🚨 LIVE #SCCM2026 PRO/CON DEBATE TOMORROW 🚨
3:15 PM - 4:15 PM
Is Personalized Medicine ready for primetime in the ICU or are Guidelines still best?
Join Dr. Sandra Kane-Gill & I as we debate this critical question at @SCCM
👉 Guidelines vs Personalized Medicine
Expect:
⚡ High-level evidence
⚡ Real-world ICU cases
⚡ Strong opinions on both sides
📅 Monday, 3/23
This is one you don’t want to miss if you care about the future of critical care.
💬 Are you pro-guidelines or pro-personalization?
🔗 View session details: congress2026.eventscribe.net…
#SCCM #criticalcare #medtwitter #FOAMcc #meded #ICUNutrition
1
3
312
Mar 22
The “guideline vs personalized medicine” debate at #SCCM2024 sidesteps the real PRO–CON question.
The primary issue facing the science issue isn’t personalization, it’s whether the present method critical care syndrome guideline derivation itself is valid.
Specifically why has transport from guessed, cause-agnostic, threshold-based, triage-gated RCTs produced so much public harm? And is this even mathematically defensible?
Will those questions be raised or debated openly? Unlikely.
Instead, expect a “synthetic debate”: a superficial exchange that avoids questioning the underlying scientific methods themselves.
Mar 22

We can’t pretend the lack of reform in critical care guideline derivation is a neutral choice.
Petty & Bone’s modified, cause-agnostic RCT design, the current standard, has the longest and worst record of producing guideline reversals for harm of any clinical testing to transport methodology.
Their 1980s departure from Fisher/Hill, to a triage-gated, threshold-based, synthetic syndrome enrollment, is not just weak; it is mathematically indefensible as a basis for causal transport to guidelines. Its real-world track record has been even worse.
We all once thought those modified RCTs were valid. There is no shame but you can no longer ignore both mathematical indefensibility AND mathematically predictably harmful results of that guideline derivation method.
The link below outlines the actual history of synthetic syndrome guideline derivation.
If you won’t engage, at least send this link to your fellows so the discussion can move forward. Better yet, send a few who are willing to debate syndrome based guideline science openly. Let’s get this in the open where real science belongs.
No more “silence defense”.
pubmed.ncbi.nlm.nih.gov/4140…
1
5
678
Lawrence Lynn retweeted

Same can be said amount flossing. As a nephrologist who ran the kidney stone prevention clinic here for years one has to be open to people using not just water to meet their fluid goals. They also need to know that whatever they do is working (so integrating periodic urine collections or even UA strips with SG help)
2
2
9
555
Lawrence Lynn retweeted

Feb 2
Totally amped to announce HR26 registration is open! Foundations Reimagined. Lets rake everyone’s game to another level!!! thinkingcriticalcare.com/202…
1
13
28
10,934