
POB Santiago de los 30 caballeros
Joined March 2020
- Tweets 21,134
- Following 613
- Followers 1,748
- Likes 7,157
3,654 Photos and videos















Ayer #ElMatutino se traslado a #CasaDEDE en Los Prados. Lugar acogedor y con variedad de platos de ocasion y "el trato DEDE" complaciente y espontaneo. El chocolate es para repetir 3-4 veces. Como siempre el team Sergio-Karina son la diferencia. Gracias invitacion.
1
4
223
PpandeloF1 retweeted

Sabías que… Hasta 2026, al menos 15 jugadores dominicanos o de ascendencia dominicana han estado en la NBA.
Tito Horford fue el primer dominicano en la NBA en 1988, y Al Horford se convirtió en el primer dominicano en ganar un campeonato de la NBA. #seaborad.energíalimpia
2
11
509
PpandeloF1 retweeted


1
2
5
183

PpandeloF1 retweeted

17h
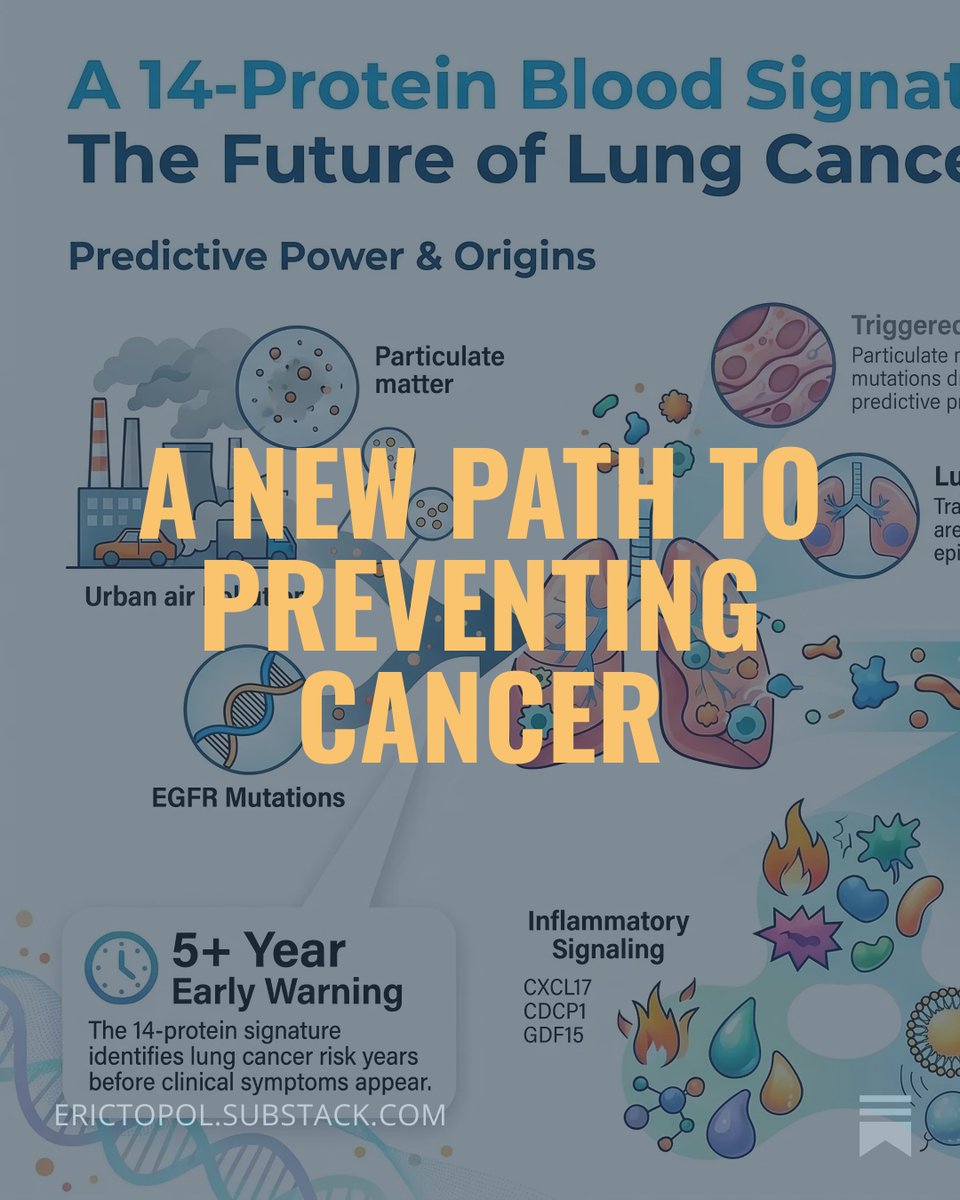
What if we could predict cancer 5 years ahead and prevent it? A new landmark study shows the way
8
102
357
30,906
PpandeloF1 retweeted

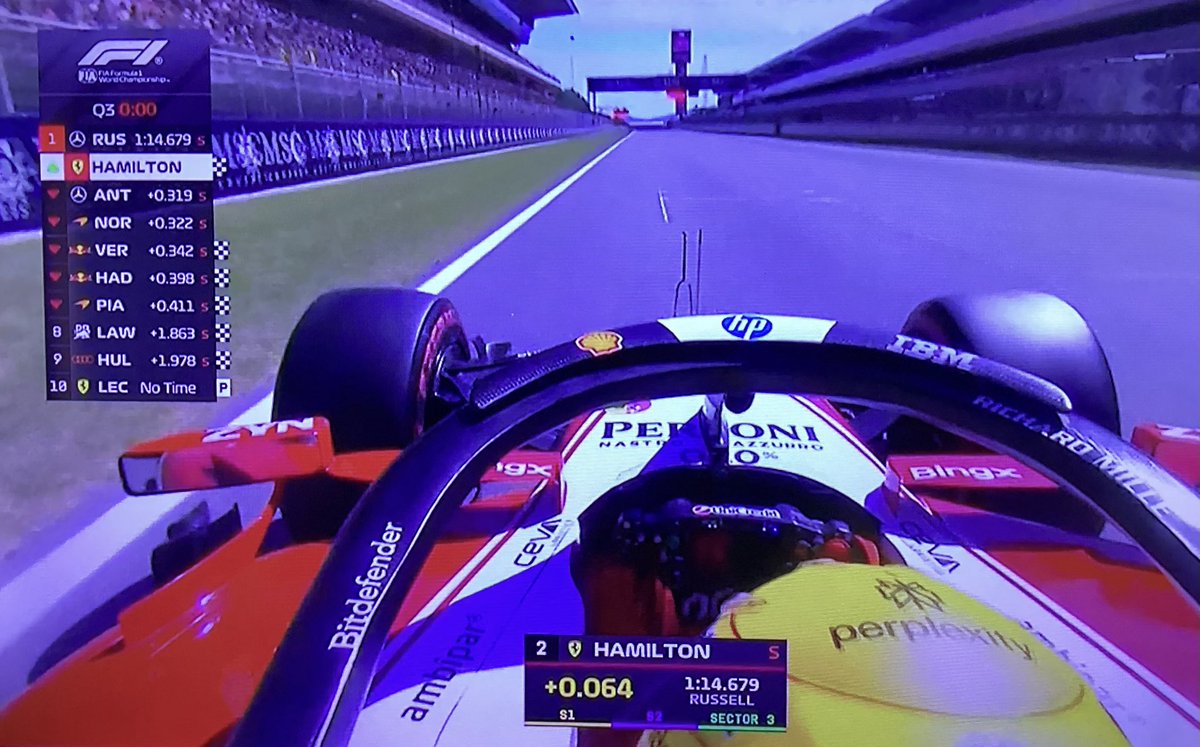
🚨 | Lewis Hamilton on Charles Leclerc's Quali:
"We basically had this exact same setup now in Quali, and, you know, Charles's been quick all weekend.”
“I think on the data, I think I was braking very late into turn four, which had been visible. And I think Charles probably tried to carry a lot of speed into that corner, and unfortunately, it didn't work out for him.”
“But, you know, he's still going to be really quick in the race."


32
175
6,138
275,773
#F1 NO matters, no importa if you sympathize for him, si simpatizas por el..Hater o no Hater.. cuando este #44 estè frente a sus ojos: Shut off/Reverencia/ or feel lucky and proud of living this era .. Y do no forget: Sin carro NO hay éxito, ni magia. Ecouter. Grande Lewis!

2
1
14
271
#F1 Q3 #Barcelona este boy necesita S O S Psico assistance. No sabemos si hubo mec falla..apreciamos que “perdió “ el SF26 turning


1
1
5
317
PpandeloF1 retweeted

❤️ Pressure-Volume Loops at the Bedside: Are We Finally Measuring What Really Matters in Cardiogenic Shock?
For decades, cardiogenic shock management has focused on cardiac output, blood pressure, filling pressures, lactate, and cardiac power.
A fascinating multicenter study published in the ASAIO Journal proposes a practical bedside method to estimate pressure-volume (PV) loop energetics using only pulmonary artery catheter and echocardiographic data, avoiding the need for invasive conductance catheters.
Why does this matter?
Traditional hemodynamic variables tell us about flow and pressure.
PV-loop analysis tells us about:
📌 Ventriculoarterial coupling (VAC)
📌 Ventricular efficiency
📌 Stroke work (SW)
📌 Potential energy (PE)
📌 Pressure-volume area (PVA)
📌 Myocardial energetic demand
These parameters may provide a much deeper understanding of whether a therapy truly unloads the failing ventricle.
Key Findings
🔹 Microaxial flow pump support in AMI-related cardiogenic shock
The most striking observation was a reduction in arterial elastance and improved ventriculoarterial coupling, accompanied by increased stroke work but decreased pressure-volume area.
This translated into an improvement in estimated ventricular efficiency from approximately 32% to 40%, suggesting genuine ventricular unloading and lower energetic expenditure.
🔹 IABP support in AMI-related shock
IABP improved ventriculoarterial coupling and reduced filling pressures but produced a more modest energetic effect compared with microaxial support.
🔹 Heart failure-related cardiogenic shock
The physiological response was far more heterogeneous. Changes in pressure-volume area and ventricular energetics were inconsistent, highlighting that device effects may depend strongly on shock etiology.
Why This Study Is Important
This work reinforces a concept increasingly discussed in advanced heart failure and shock programs:
The goal is not simply increasing cardiac output.
The goal is improving systemic perfusion while simultaneously reducing myocardial oxygen consumption and ventricular workload.
A patient can have a higher cardiac output while still operating at an unfavorable energetic state.
Pressure-volume analysis may reveal this hidden physiology.
Practical ICU Takeaway
When evaluating mechanical circulatory support, we should ask three questions:
1️⃣ Is systemic perfusion improving?
2️⃣ Is ventricular filling pressure decreasing?
3️⃣ Is ventricular energetic demand falling?
Only when all three occur simultaneously can we confidently say that true ventricular unloading has been achieved.
The future of cardiogenic shock management may be less about isolated hemodynamic variables and more about understanding the complete interaction between the ventricle and the arterial system.
Reference 📚
Ortega-Hernández JA. ASAIO Journal. 2026. DOI: 10.1097/MAT.0000000000002737.

ALT
1
20
54
2,301
PpandeloF1 retweeted

Jun 12
Rectal bleeding occurring exclusively during menstruation is highly suggestive of catamenial rectal bleeding, and the most important diagnosis to consider is: Bowel Endometriosis

1
10
106
12,015
PpandeloF1 retweeted
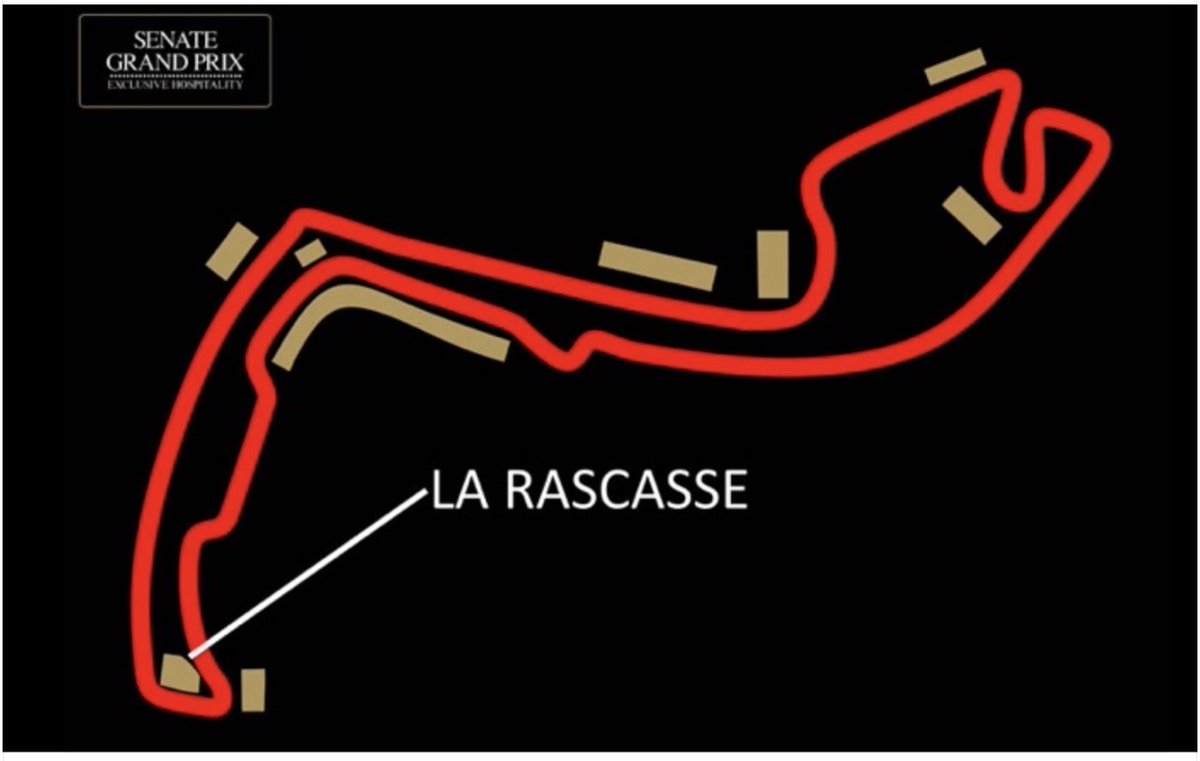
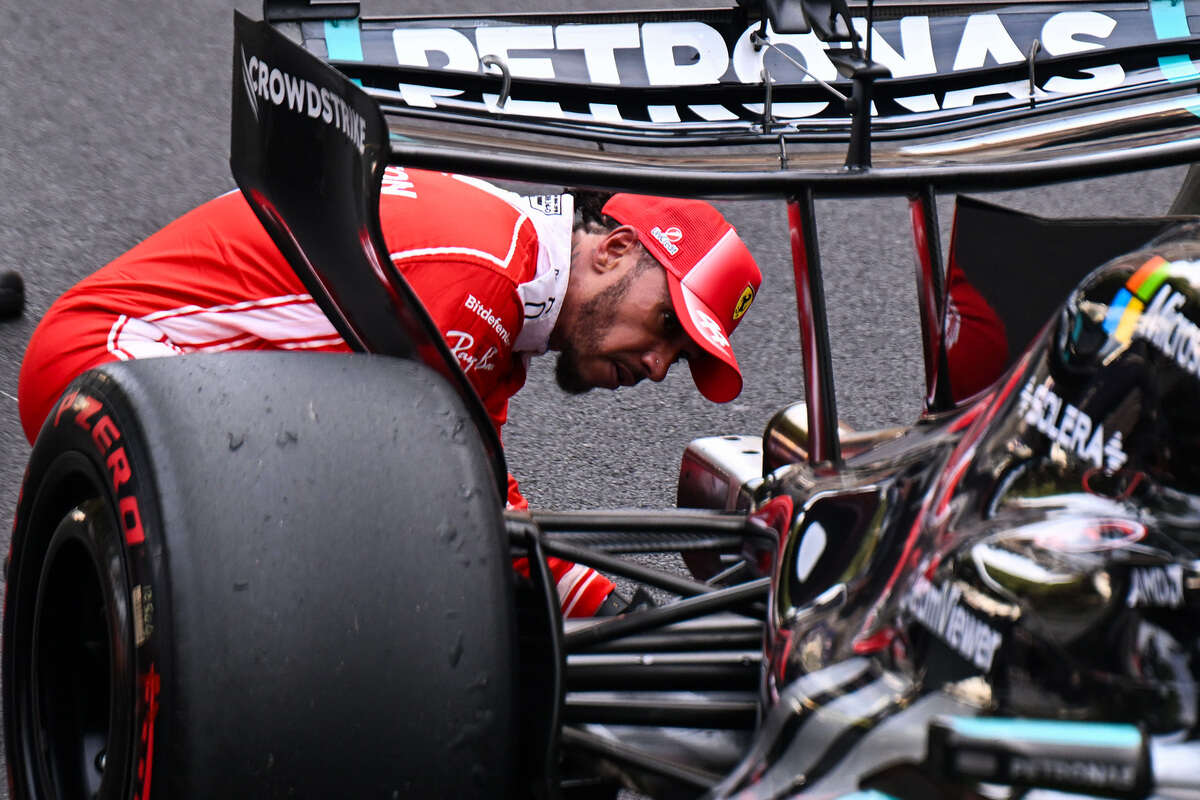
🚨 | FIA rejects Ferrari, approves Mercedes!
Following a FIA clarification requested by Ferrari, Mercedes slightly modified its "serrated" diffuser in Monaco.
Ironically, Ferrari had a similar concept rejected by the FIA before the season started.
Now that FIA has officially ruled the W17 solution legal, Maranello's engineers could revisit their initial idea and translate the concept directly onto the SF-26.
📰 @Auto_Racer_it
111
279
5,618
407,819
PpandeloF1 retweeted

Jun 9
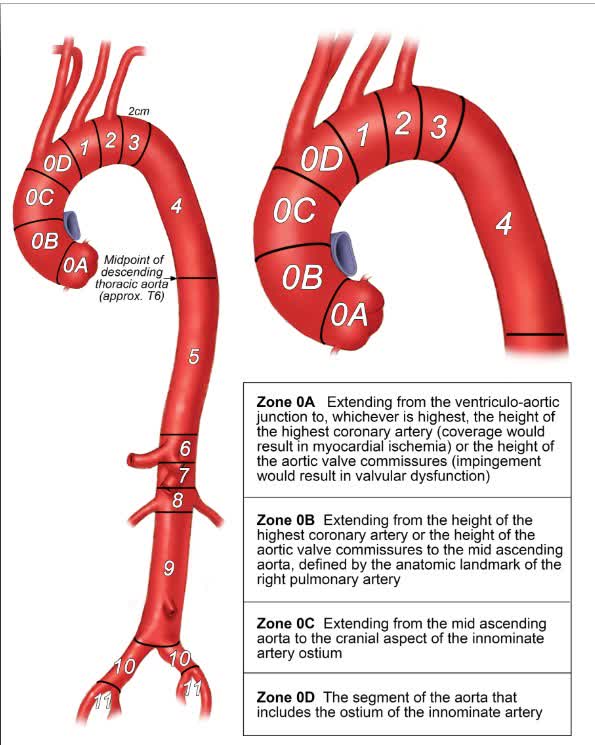
#InDepth on the global, multidisciplinary ARCH-ARC consensus statement to standardize reporting for thoracic aortic repair. ahajrnls.org/4dXF6xP
1
57
145
16,462
PpandeloF1 retweeted
Jun 10
A review of the effects of marathon running on the heart
bmjopensem.bmj.com/content/1…
including release of blood biomarkers cardiac troponin, NT-proBNP without known clinical significance
8
39
230
48,569
PpandeloF1 retweeted

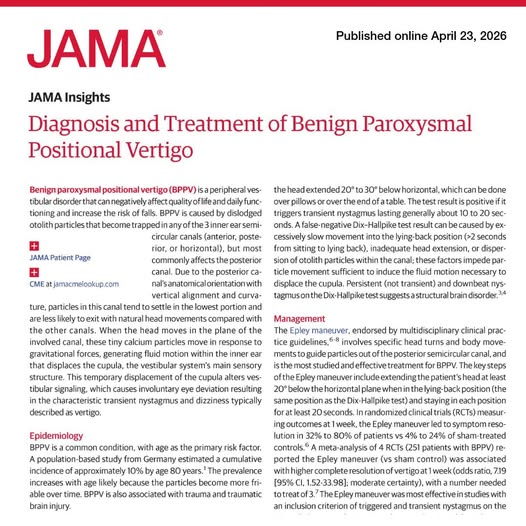
Jun 9
Brief, positionally triggered vertigo with transient nystagmus on the Dix-Hallpike test is characteristic of #BPPV, a common and treatable cause of dizziness.
📊 Learn more in this JAMA Insights. ja.ma/4xjxbT6
1
42
120
7,898
PpandeloF1 retweeted
Jun 8
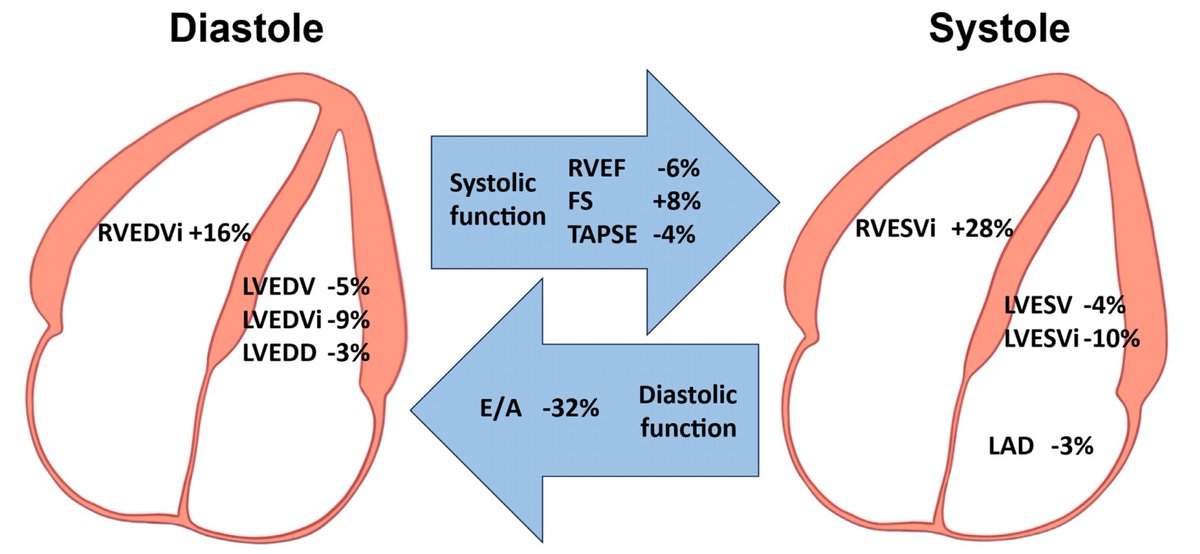
In today's @TheLancet there are 3 papers on cardiometabolic disease: biology, epidemiology, prevention/treatment.
The sobering and all to common story from womb to tomb conveyed in this graphic
thelancet.com/journals/lance…
thelancet.com/journals/lance…
thelancet.com/journals/lance…

9
258
753
54,734
PpandeloF1 retweeted

Jun 8
Of interest - Sequential theoretical addition of ezetimibe and bempedoic acid increased LDL‑C goal achievement and was associated with modeled reductions in MACE. Risk estimates were inferred from LDL‑C lowering in the simulation. sciencedirect.com/science/ar…

2
14
36
4,120
PpandeloF1 retweeted

Jun 9
Identification and management of non-obstructive high-risk coronary artery plaque
Please read the article and enjoy an in-depth interview between @jhfrudd and the first author, University of Edinburgh's Dr Craig Balmforth
Publication - bit.ly/4dHJwJd
Podcast - apple.co/4uRifua

21
61
3,903
PpandeloF1 retweeted

👉Cardiometabolic Disease: The Silent Pandemic We Keep Underestimating
1️⃣ Kills ~20 million people every year worldwide — twice as many as all cancers combined.
2️⃣ Accounts for ~31% of all global deaths, compared with ~16% for cancer.
3️⃣ Often strikes suddenly and without warning, frequently outside the hospital and before a diagnosis is ever made.
4️⃣ Cardiovascular disease, diabetes, and chronic kidney disease progress together, damaging multiple organs simultaneously.
5️⃣ The disease develops silently over decades, making prevention and early intervention essential.
6️⃣ The annual global economic burden exceeds US$4.7 trillion, nearly 4 times greater than that of cancer.
7️⃣ The greatest opportunity in modern medicine is not treating late disease—it’s identifying high-risk patients early and preventing the first event.
8️⃣ A patient-centered cardiorenometabolic approach has become one of the most important public health priorities of our time.
☝️Bottom line:
Cardiorenometabolic disease is not just the leading cause of death—it is the leading cause of lost healthy life and healthcare costs worldwide. Prevention can no longer wait.
@society_eas
@nationallipid
@escardio
@fhpatienteurope
@ACCinTouch
@AHAScience

7
23
68
5,072
PpandeloF1 retweeted

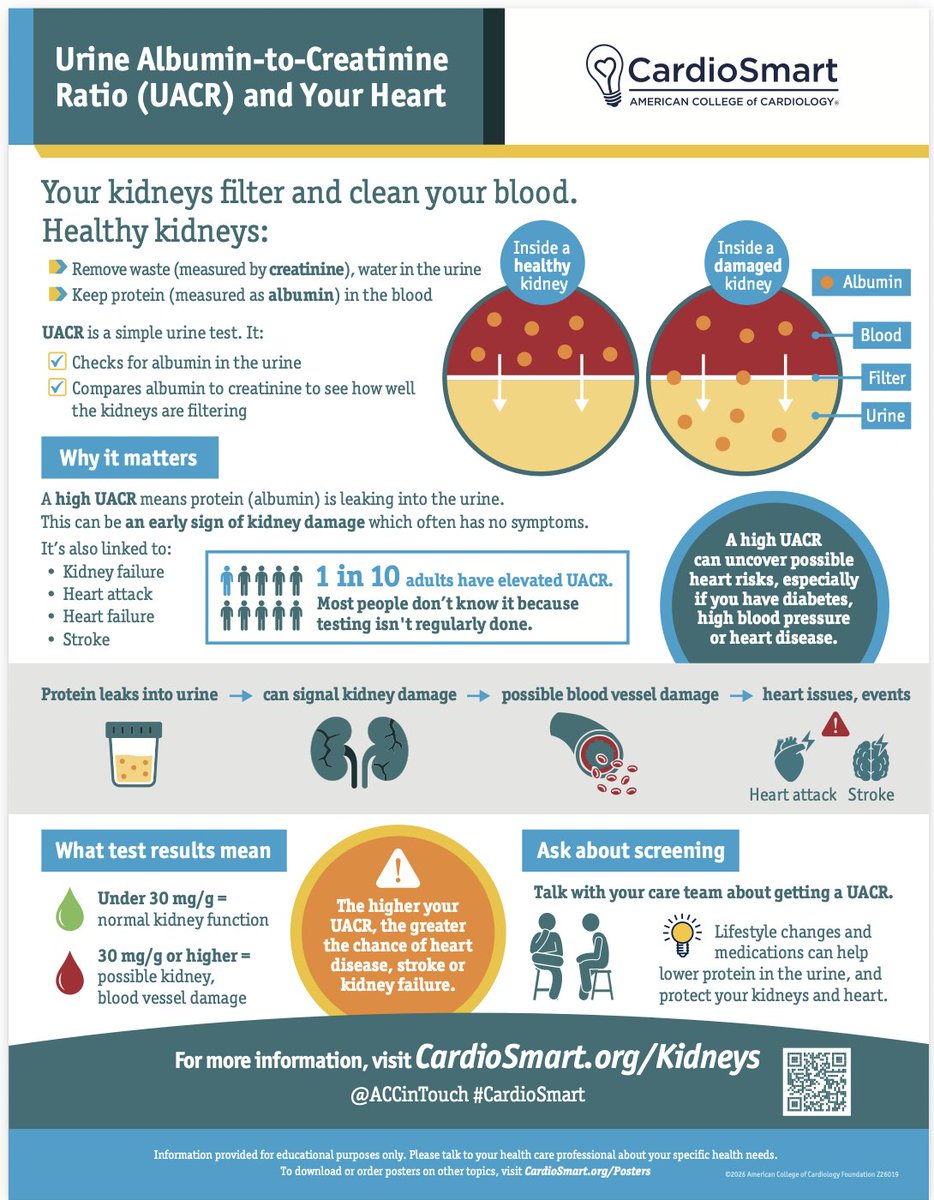
Explaining why you check #UACR has never been easier!
Thanks to #CardioSmart, we have the infographic that everyone should have up in clinic @ACCinTouch
We just need to identify the patients who need this checked. If you have #hypertension, #diabetes or #HeartDisease, you need this checked annually! #CVPrev #CardioTwitter #cardionephro
3
47
131
5,978
PpandeloF1 retweeted

Jun 9
Published today, the first-ever clinical practice guideline on cardiovascular-kidney-metabolic (CKM) syndrome from the American Heart Association and @ACCinTouch.
The focus of this clinical practice guideline is to create a living, working document that provides current knowledge in the field of CKM syndrome aimed at all practicing cardiologists, endocrinologists, nephrologists, and primary care and specialty clinicians who manage these patients.
✍🏼 @ChiadiNdumele @HeartDocSadiya @kardiologykazi @noshreza @virani_md @biykemb @NutritionHF @mandeepbajaj65 @KatherineTuttl8 @RangaswJ @lisaVWMD @KBreathettMD @EmoryFamMed @ShoaClarke @mad_sters @jmortonmd @sripalbangalore @AnumSaeedMD
5
244
491
58,754