Accredited online CPR, First Aid & BLS certifications—affordable, flexible, life-saving skills for individuals & businesses. Be prepared. Sign up today!
Joined February 2010
- Tweets 1,960
- Following 4,346
- Followers 4,613
- Likes 5,337
497 Photos and videos











30 Apr 2025
With ProTrainings, completing your certification is just the first step in a journey that may lead to you saving someone's life. That's why we continue to supplement your training with weekly refreshers, even after you complete your training.
Find out more >>> bit.ly/41U3Ssv
#CPR #FirstAid #CPRTraining
1
134
29 Apr 2025
"In the moment, all I could think about was ‘This is somebody’s person,'" said Katelyn Williams, a high school senior who saved a life with #CPR at her local YMCA.
When a man collapsed in the locker room, the CPR skills she learned at school gave her the confidence to jump into action and save his life.
Check out the rest of the story from @WKRN >>> bit.ly/4ixOt6A
#CPRSavesLives #FirstAid
1
130
24 Apr 2025
Bridges Medical Services (@CoxHealth) had a problem. They had used one of our competitors for years, but continued logistical problems prompted them to look for a new #CPRTraining program.
Find out how our streamlined online training system helped them reach full #CPR compliance >>> bit.ly/43xXgBm
5,933
17 Apr 2025
Our mission is to make #CPRTraining more accessible, more engaging, and more memorable for everyone who takes it. When you complete our courses, you leave with more than a certification — you have the skills you need to save a life.
Learn how ProTrainings takes the stress out of compliance with our streamlined, online training process >>> bit.ly/41U3Ssv
#CPR
2
4,976
17 Apr 2025
Erin Mayfield's husband was jogging around the neighborhood when he faced sudden #CardiacArrest. Luckily for him, bystanders rushed to help and saved his life with #CPR.
Now, she's bringing hands-on #CPRTraining to her school. Here's the full story from @NorthwestISD >>> bit.ly/3DHXVpc
4,480
16 Apr 2025
Our mission is to make #CPRTraining more accessible, more engaging, and more memorable for everyone who takes it. When you complete our courses, you leave with more than a certification — you have the skills you need to save a life.
Learn how ProTrainings takes the stress out of compliance with our streamlined, online training process >>> bit.ly/41U3Ssv
#CPR
2
97
13 Apr 2025
It's a normal day at work... or so you thought. Suddenly, your coworker collapses. They aren't breathing. Do you know what to do next?
Here's how to respond when someone needs your help in the workplace >>> bit.ly/4iirInt
#CPRSavesLives #FirstAid #CPR
3,785
ProTrainings retweeted

3 Apr 2025
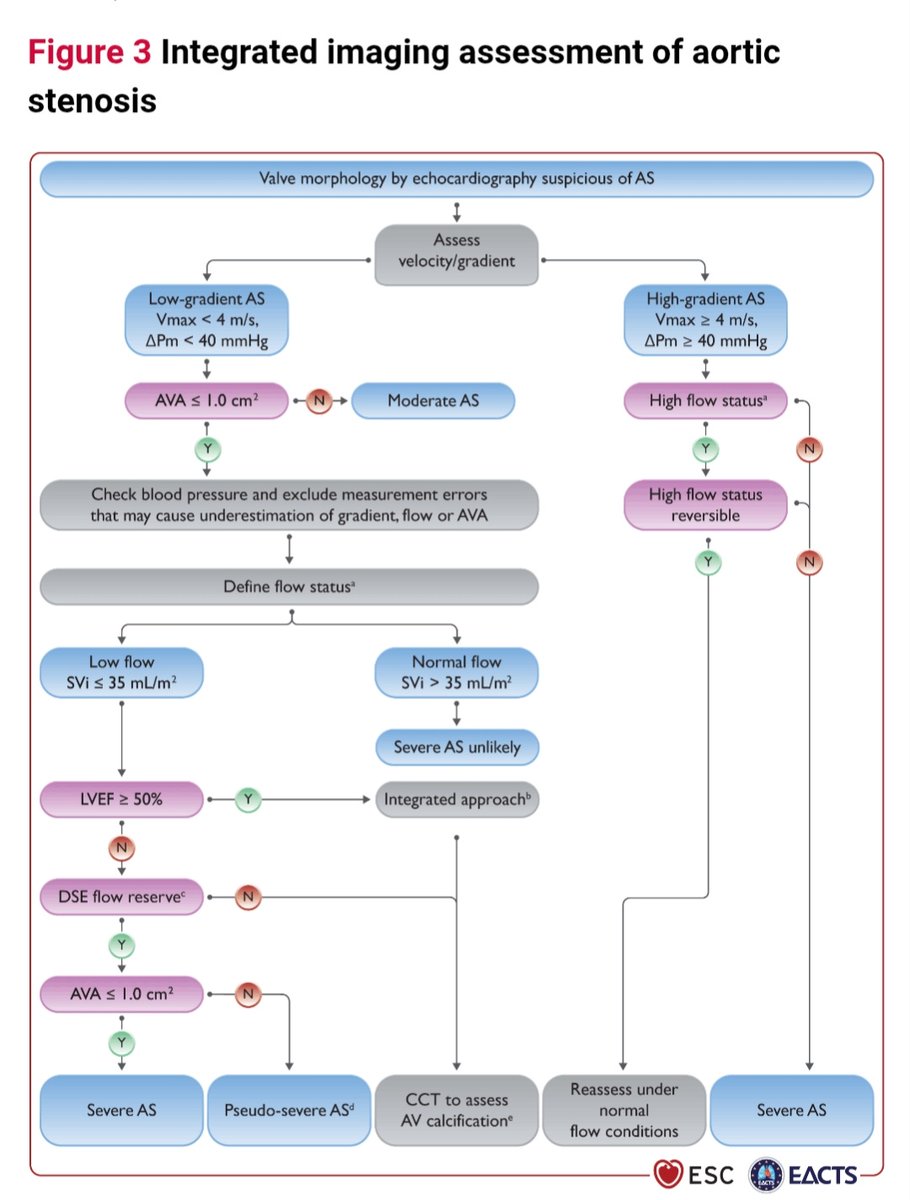
High vs Low gradient severe Aortic Stenosis approach
Check Gradient & Flow status:
●LOW flow,LOW gradient:
EF<50%:DSE to assess Flow Reserve
EF>=50%:CCT to assess AV calcification
CCT also if no Flow reserve after DSE
●Exclude HIGH flow status in HIGH gradient AS
21
125
8,327
ProTrainings retweeted

4 Apr 2025
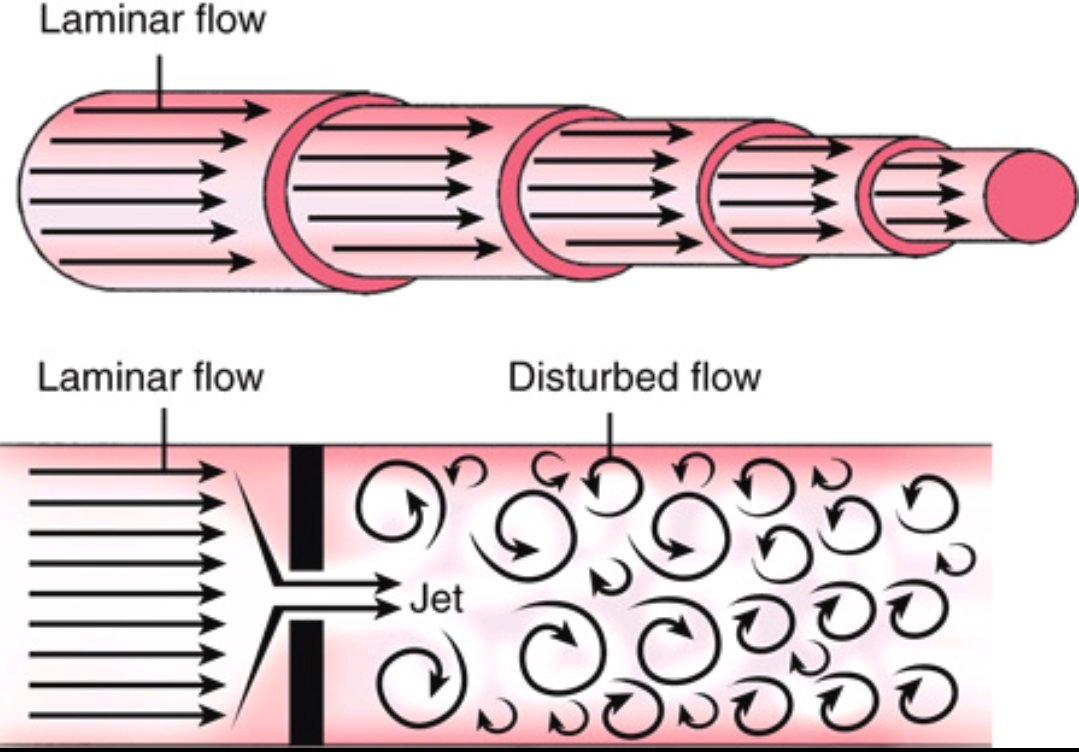
Understanding Intracardiac Blood Flow: Laminar vs. Disturbed Flow
Blood flow in the heart follows distinct patterns, influencing hemodynamics and disease progression.
🔹 Laminar Flow (Top Image) – Smooth, parallel streamlines with uniform velocity, seen in normal arteries and heart chambers. This pattern ensures efficient oxygen delivery and minimizes endothelial stress.
🔹 Disturbed Flow (Bottom Image) – Occurs beyond stenotic valves, regurgitant orifices, or intracardiac shunts. Chaotic vortices and eddies increase turbulence, shear stress, and risk of endothelial damage or thrombus formation.
🔹 Clinical Example: In Aortic Stenosis, blood is forced through a narrowed valve, creating a high-velocity jet. This jet remains laminar until it exits the stenotic orifice, where turbulence forms. Doppler echocardiography detects this as increased peak velocity and pressure gradients, helping assess stenosis severity.
🔹 Another Example: In Atrial Septal Defect (ASD), left-to-right shunting of blood through the septal defect leads to disturbed flow, visible as color Doppler turbulence in the right atrium. This abnormal flow pattern can cause right heart volume overload over time.
Recognizing these flow patterns is crucial in echocardiography and hemodynamic assessments. #Cardiology #Echo #Hemodynamics
23
82
4,203
ProTrainings retweeted

4 Apr 2025
Who needs a morning coffee when you can start your day with a refreshing walk to work? Happy Walk to Work Day everyone! #walktoworkday spr.ly/6017FTgtd
3
5
495
ProTrainings retweeted

4 Apr 2025
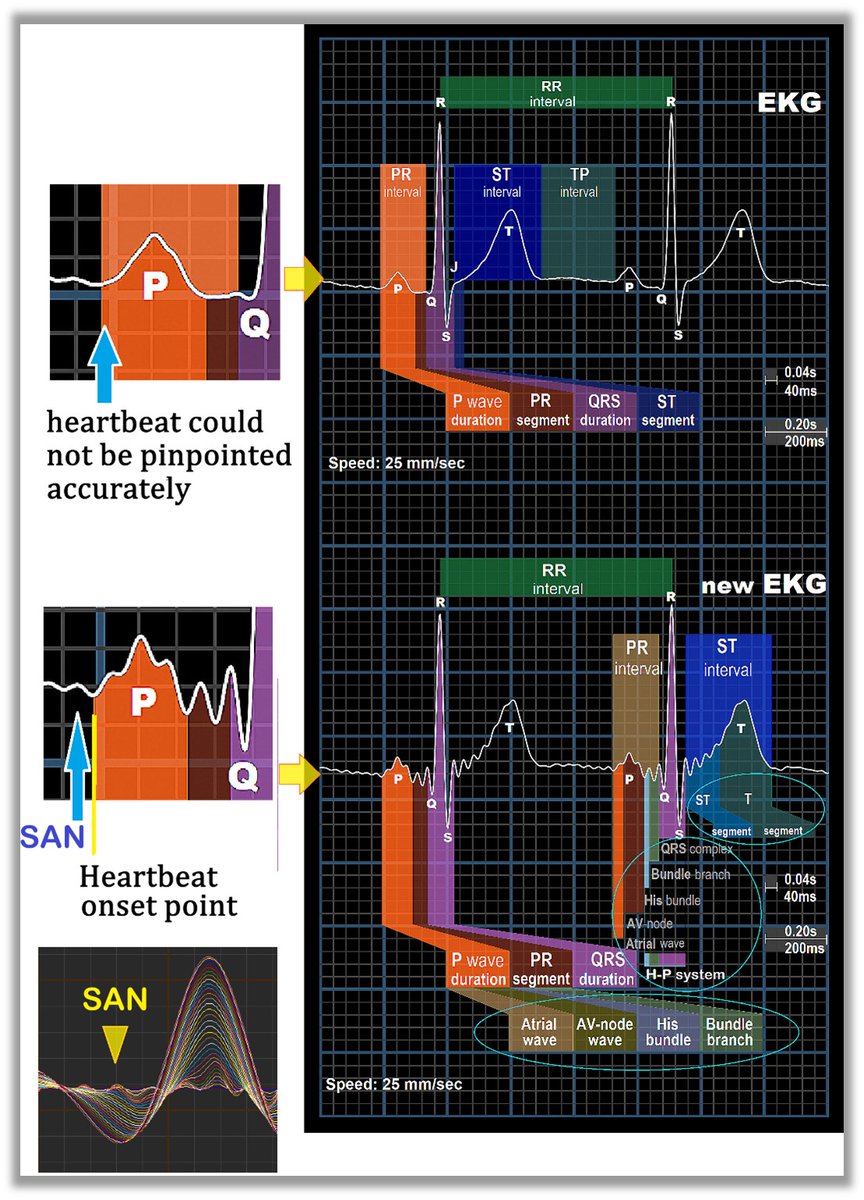
SAN (sinoatrial node)
Precisely locating the starting point of each heartbeat is extremely difficult and has been a challenge for 122 years. The reason is that the P-wave onset in traditional ECGs is a curved corner, and a slight difference amounts to 5–10 milliseconds. Therefore, the unit of measurement with a compass can only be in "seconds," while computer measurements cannot pinpoint it accurately either. Up to now, ECG remains at a rudimentary stage of data values, unable to achieve quantitative diagnosis or meet clinical needs. The heart is an organ that conducts electricity, and undoubtedly, ECG is the most direct targeted indicator of the heart. However, since receiving the Nobel Prize in 1924, it has not been revolutionized. What is recorded is merely a high-frequency trace of the heart's surface (P = atrium, T = ventricle, QRS = pulse wave). What we doctors see is only a superficial electrical trace. Signals such as SCT, various membrane potentials, and ion exchange signals are all completely blank. The correlation between ECG and diseases is simply too far apart.
The SAN (sinoatrial node) is the starting point of each heartbeat and is, of course, of utmost importance because the human heart rate of 60–100 beats per minute is determined by the SAN's working frequency. Electrophysiologists and interventional cardiologists both rely on the SAN, as it is the origin of every heartbeat. The blood supply to the SAN comes from two coronary arteries: the LCx (left circumflex artery) and the RCA (right coronary artery).
**Specialized Cardiac Tissue (SCT) was proposed by Great Hoffman in 1964.
SAN = The source of life, the very place where life resides, and the starting point of every heartbeat.
PhysioSign USA
#ecg #ekg #ep #electrophysiology #medtech #cardiology
13
43
3,104
ProTrainings retweeted

3 Apr 2025
Did you circle the screen? Or zig-zag? It’s important to have a strategy for managing your blood pressure, too. Talk to your doctor about your numbers and how to keep them in a healthy range.
3
11
24
3,266
ProTrainings retweeted

2 Apr 2025
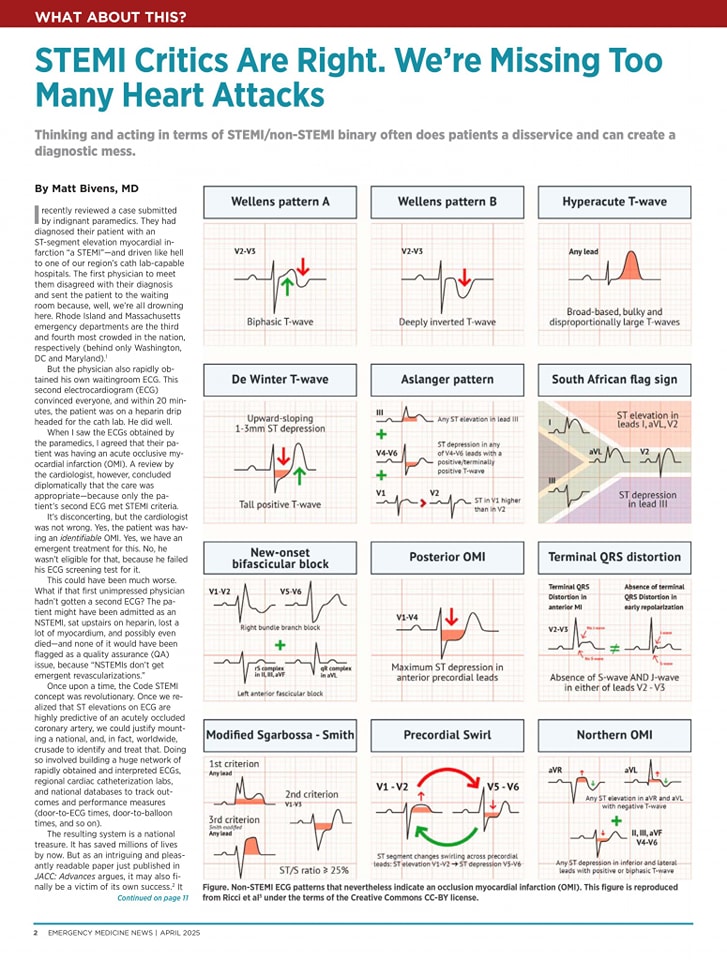
🔴STEMI Critics Are Right. We're Missing Too Many Heart Attacks⤵️ #2025commentary #openaccess
🔹journals.lww.com/em-news/ful…
#CardioEd #Cardiology #CardioX #MedEd #Cardiox #medx #Cardiology #ECG #ekg #EKGInterpretation #Cardiotwitter #cardiotwiteros #medx #meded #medtwitter
1
149
548
43,188
ProTrainings retweeted
3 Apr 2025
Is Angioplasty Better Than Thrombolysis in MI?
For STEMI patients, strong evidence favors primary PCI (PTCA) over thrombolysis, reducing mortality, recurrent MI, and stroke.
🔹 PAMI Trial: PTCA lowered in-hospital & 6-month death recurrent MI.
🔹 GUSTO IIb: Lower rates of death, MI, and stroke at 30 days.
🔹 Meta-analysis: PTCA led to 34% ↓ mortality, 65% ↓ stroke, 91% ↓ hemorrhagic stroke.
📌 Who benefits most from primary PCI?
✅ Cardiogenic shock or CHF
✅ Post-CABG patients (SVG thrombosis)
✅ Contraindications to thrombolysis
⚠️ Limitations: Requires high-volume centers, expertise & cost considerations.
Should all STEMI patients get primary PCI if feasible? ( Comment Your opinion 🙏)
Ref: Grines CL et al., PAMI Trial
#CardioTwitter #STEMI #PCI #Thrombolysis

15
46
3,083
ProTrainings retweeted
2 Apr 2025
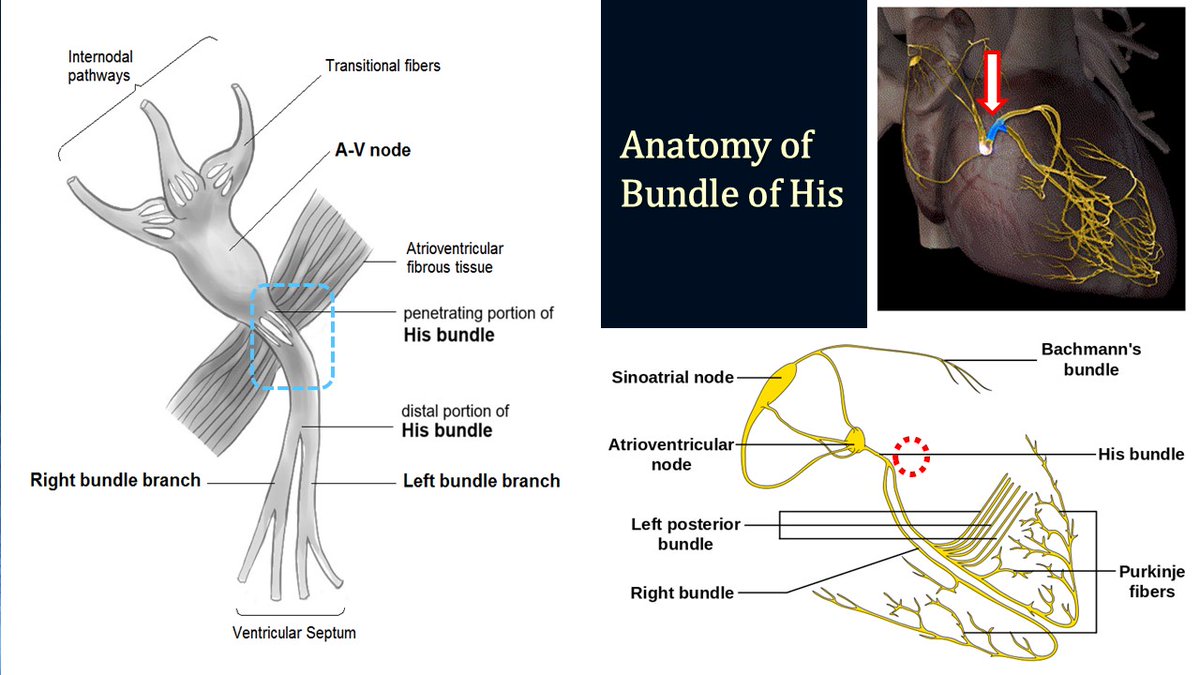
Anatomy of the Bundle of His
The bundle of His is a singular, unidirectional structure located at the atrial outlet, acting as a vital conduit between the atrioventricular node (AVN) and the left and right bundle branches. Its distinct anatomical features highlight its essential role in cardiac conduction, a function that traditional electrocardiography (ECG) cannot capture.
#ecg #ekg #cardiology #ep
29
137
11,405
ProTrainings retweeted

2 Apr 2025
1
29
68
4,926
ProTrainings retweeted
3 Apr 2025
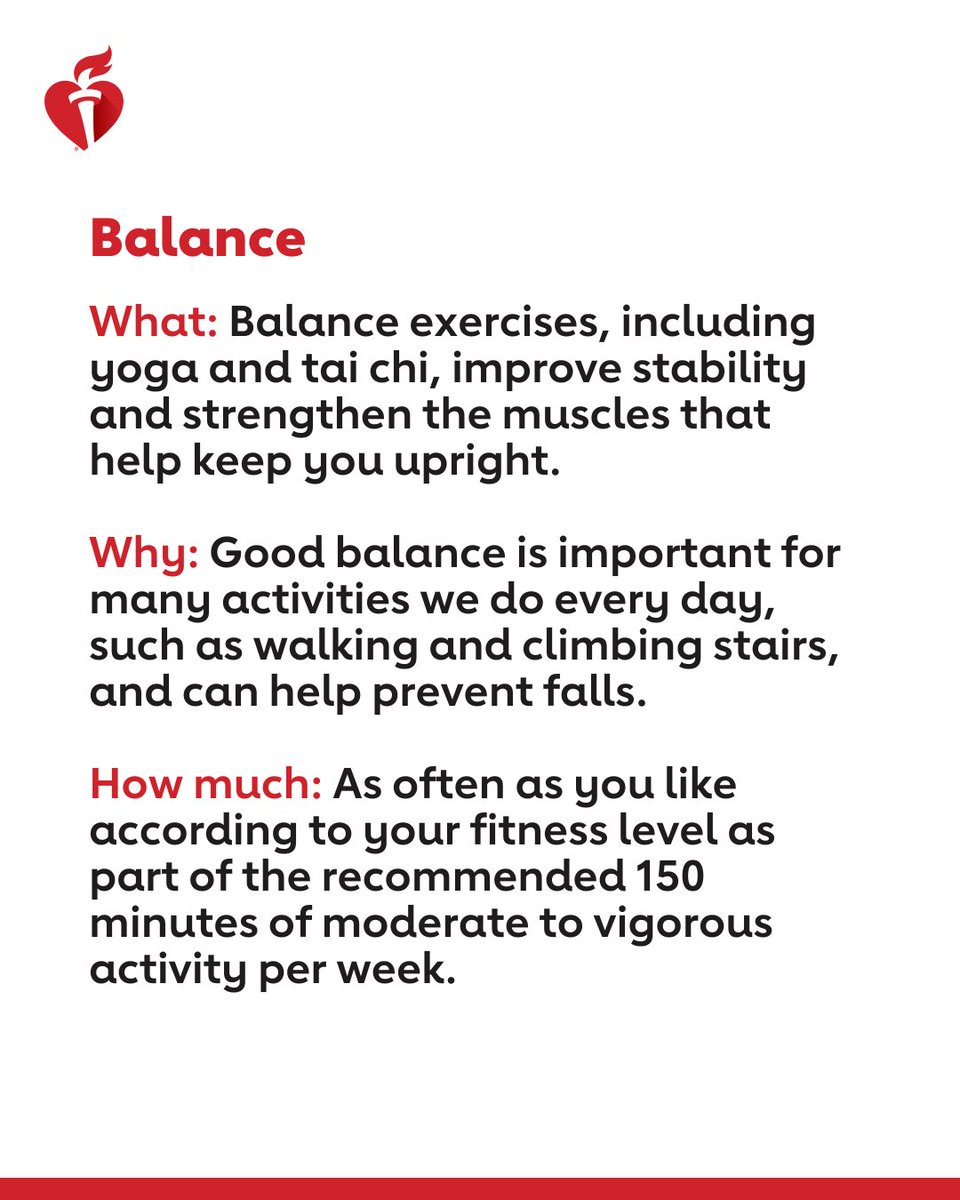
A healthy workout routine is made up of 4 types of exercise: endurance, strength, balance and flexibility. They don’t all need to be done every day, but variety helps keep the body fit and keeps your exercise routine interesting.



4
39
73
5,797
2 Apr 2025
Staying #HeartHealthy goes beyond diet and exercise. #Stress plays a direct role in heart health, and can even lead to heart disease.
Today marks the start of #StressAwarenessMonth, so we're sharing a few tips to help you prevent chronic stress.

2
5,864
ProTrainings retweeted
1 Apr 2025
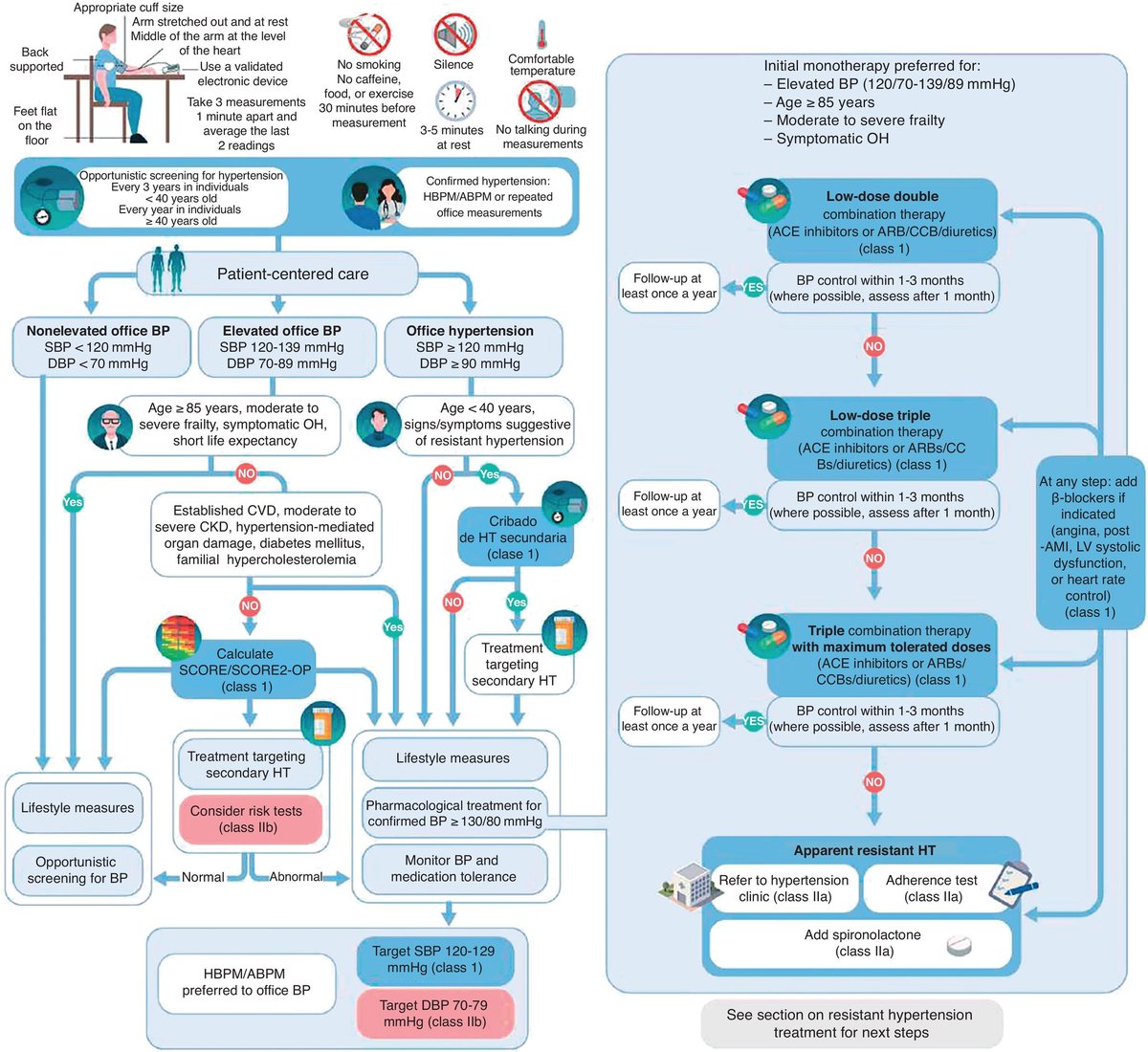
🔴Comments on the 2024 ESC guidelines for the management of elevated blood pressure and hypertension⤵️ #2025commentary #OpenAccess
🔹revespcardiol.org/en-comment…
#Cardiology #FOAMed #MedEd #medstudent #paramedic #Cardiology #CardioEd #medtwitter #meded
46
166
17,343
ProTrainings retweeted
1 Apr 2025
Join @American_Heart & @RubenStuddard on April 2 for National Walking Day!
🌤️ Enjoy the fresh air.
👟 Get some extra steps.
😎 Stress less.
Share YOUR view with us! #WalkingDay
4
6
18
2,881