
Professor of Cell Biology at Universitat Politècnica de València, with a particular passion for molecular medicine and a strong interest in natural philosophy.
Joined March 2025
- Tweets 4,504
- Following 452
- Followers 2,440
- Likes 4,547
873 Photos and videos







Pinned Tweet

8 Nov 2025
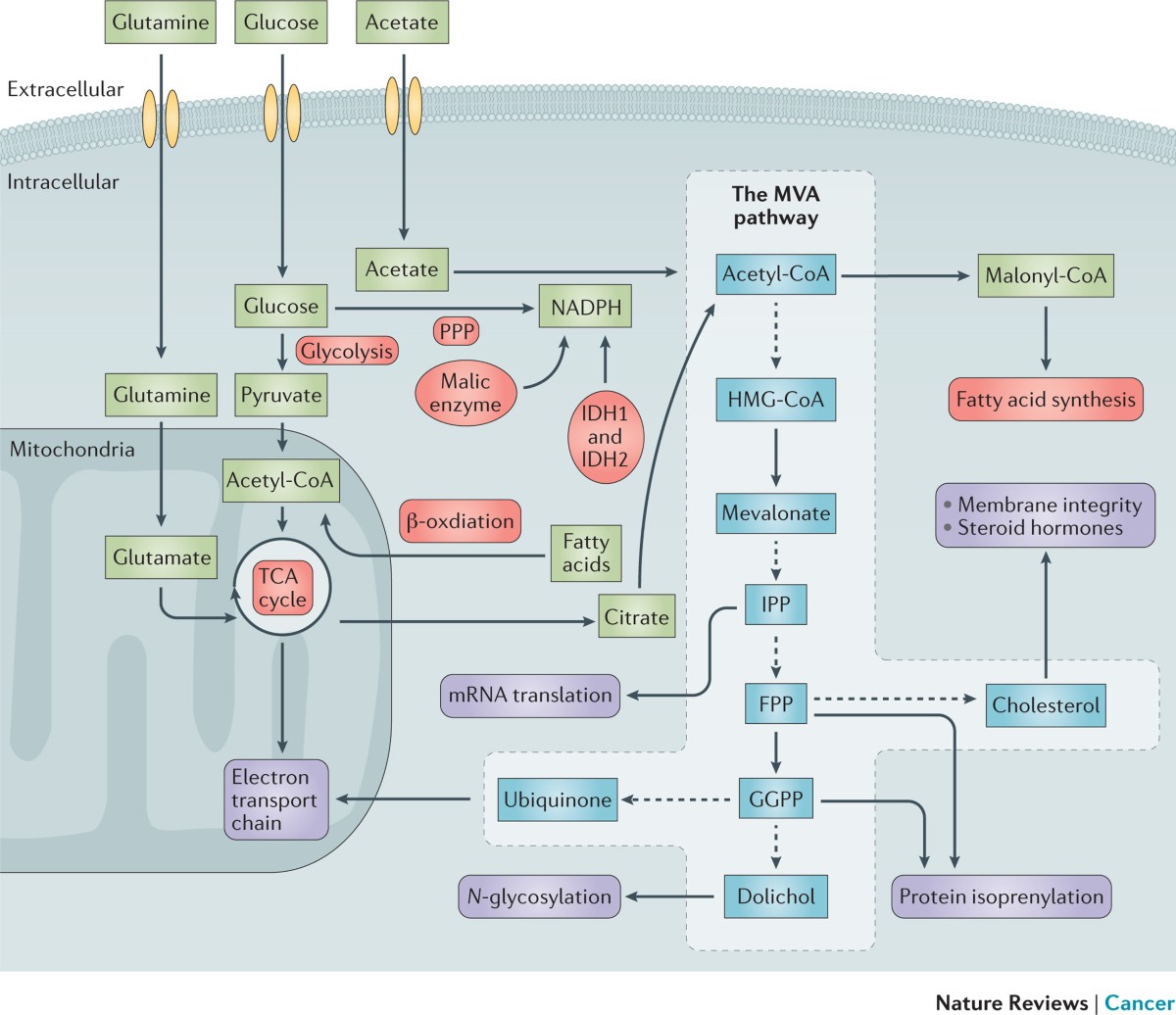
Molecular Medicine is not just a branch of science — it is the very language of life.
It explains how cells communicate, how genes express identity, and how molecules decide between health and disease.
Within its scope lies the most intimate narrative of our existence: the silent choreography of enzymes, receptors, and signals that sustain us every second.
By following this account, you will explore the hidden logic that keeps us alive — and discover what happens when those delicate mechanisms fail, giving rise to illness.
Here, we decode the molecular origins of disease and the rationale behind the action of drugs, tracing every therapeutic effect back to its biochemical root.
Understanding Molecular Medicine is to see medicine itself under a microscope — where every cure begins as a molecular idea.
2
8
69
11,413
Rafael Sirera retweeted

Este editorial de @Nature sostiene que estamos viviendo uno de los mayores cambios en el acceso a la información.
Si la comunicación científica quiere seguir siendo relevante e influyente, deberá adaptarse a estos nuevos formatos sin renunciar al rigor científico.
nature.com/articles/d41586-0…

3
32
85
3,562


You have probably heard of rheumatoid factor (RF) thousands of times.
But do you know what it actually is — and why this old biomarker still matters when considered together with anti-citrullinated protein antibodies?
RF is often treated as a simple laboratory result: positive or negative, high or low. But biologically, it is much more than a diagnostic clue.
It is an autoantibody with the capacity to reshape immune responses, amplify inflammation, and contribute directly to tissue injury.
1⃣ What is rheumatoid factor?
Rheumatoid factor is an autoantibody directed against the Fc portion of IgG.
In other words, RF is an antibody that recognizes another antibody.
This apparently paradoxical interaction is central to its biological relevance. By binding IgG, RF can form immune complexes that persist, activate innate immune pathways, and fuel chronic inflammation.
2⃣ Why is IgM RF especially important?
Although RF can belong to different immunoglobulin classes, the most commonly measured and clinically relevant form is IgM RF.
IgM RF binds IgG and promotes the formation of large immune complexes. These complexes are not inert. They can deposit in tissues, engage Fc receptors, activate complement, and create a self-sustaining inflammatory loop.
So RF is not merely a marker of rheumatoid arthritis.
It can become part of the machinery that perpetuates inflammation.
3⃣ Where does genetics enter the story?
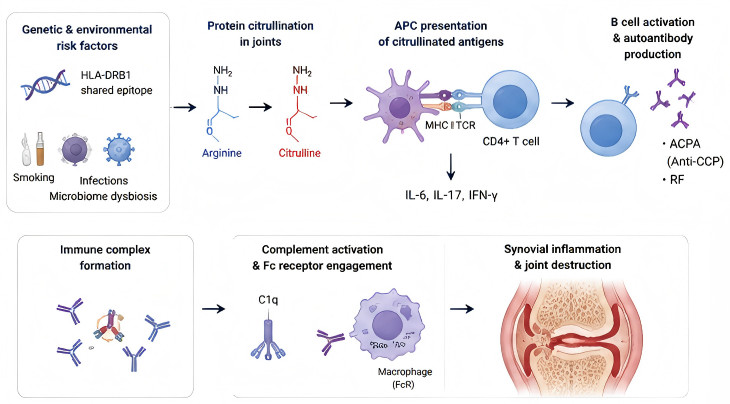
The production of RF is influenced by genetic susceptibility, especially by certain HLA-DRB1 alleles associated with rheumatoid arthritis.
These alleles do not “cause” RF production directly. Rather, they shape the immunological landscape in which tolerance may fail.
In genetically susceptible individuals, antigen presentation, T-cell help, B-cell activation, and chronic immune stimulation may converge to favor the emergence of autoantibodies such as RF.
4⃣ How does RF contribute to inflammation?
When IgM RF binds IgG, immune complexes are formed.
These complexes can activate the complement cascade, recruit inflammatory cells, and stimulate macrophages and neutrophils.
The result is increased production of mediators such as TNF-α, IL-6, IL-1β, and other inflammatory signals that sustain synovitis.
Clinically, this translates into joint swelling, pain, morning stiffness, progressive cartilage damage, and bone erosion.
5⃣ Is RF specific for rheumatoid arthritis?
Not completely.
RF is strongly associated with rheumatoid arthritis, especially when present at high titres, and it often correlates with more severe disease, extra-articular manifestations, and worse prognosis.
But RF can also appear in other autoimmune diseases, chronic infections, liver disease, malignancies, and even in healthy individuals, particularly with ageing.
This is why RF must never be interpreted in isolation.
Its meaning depends on the clinical context, antibody titre, symptoms, inflammatory markers, imaging, and the presence of other autoantibodies such as anti-CCP/ACPA.
6⃣ ACPA means anti-citrullinated protein antibodies.
They are autoantibodies directed against proteins that have undergone citrullination, a post-translational modification in which the amino acid arginine is converted into citrulline.
Anti-CCP means anti-cyclic citrullinated peptide antibodies. This is the laboratory test most commonly used to detect ACPA. The assay uses synthetic cyclic citrullinated peptides as antigenic targets.
7⃣ The key message?
IgM RF is not just a passive biomarker.
It is an antibody against antibodies, a generator of immune complexes, an amplifier of complement activation, and a contributor to the inflammatory architecture of rheumatoid arthritis.
Understanding RF means looking beyond the lab result.
It means seeing the molecular circuitry that connects genetic susceptibility, loss of tolerance, immune-complex biology, cytokine amplification, and joint destruction.
🚩 RF is old as a biomarker, but biologically it remains deeply relevant: a small antibody signal with major inflammatory consequences.
3
5
187
Rafael Sirera retweeted
ESR tells you that inflammation has left a slow systemic footprint.
CRP tells you that the liver is actively responding to cytokines
Procalcitonin tells you that the inflammatory programme may be bacterial or septic in nature.
They are not interchangeable clocks.
They are different biological readouts.
3
42
111
3,208
Rafael Sirera retweeted
Qué interesante!!
Aquí tienes la otra cara de la historia, citando a Carter, el ilustrador, que tan importante es en este libro!!, x.com/ProfSirera/status/2013…
Jan 19

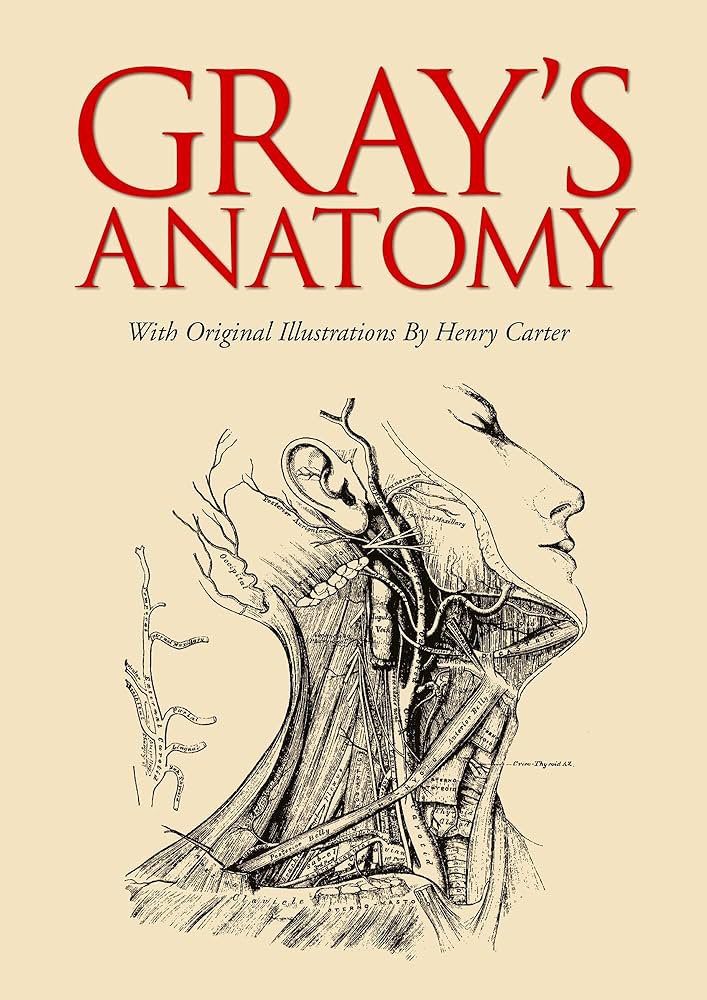
The most iconic book of medicine ever, Gray's Anatomy, is the product of a brilliant and tragic partnership.
Henry Gray was a meticulous London anatomist, but the detailed, masterful illustrations were the work of Henry Vandyke Carter, a skilled physician and draftsman. Carter, who later had a distinguished career in India, worked for 18 months on the drawings. Yet, in a lasting slight, the original title page read “Anatomy, Descriptive and Surgical by Henry Gray… with Drawings by H.V. Carter.” His secondary credit and modest, lump-sum payment of £150—for images that would become iconic—remains a historical injustice.
An early anecdote highlights the book’s practical aim. To ensure accuracy, Gray and Carter reportedly dissected an unclaimed pauper’s body from the St. George’s Hospital morgue together, with Gray naming structures and Carter sketching in situ. This collaboration between hand and eye, scalpel and pen, created an unprecedented clarity that fused art with science, securing the book’s place as a medical touchstone for over 160 years.
Gray was only 34 when he died of smallpox in 1861, just three years after his seminal work’s first publication. He never saw its monumental, enduring success.
1
3
205
Rafael Sirera retweeted

Meredith Grey es ficción. Henry Gray, no.
Dices “Anatomía de Grey” y casi todo el mundo piensa en el hospital de Seattle. Médicos guapísimos follisqueando en cuartuchos.
Pero ese título bebe de otro anterior. Con A. Gray, sin la “e”. Y digo sin penas que fue mi atlas de anatomía favorito. Información justa, algunas curiosidades, sin agobiar. Nada del aluvión de datos del Netter. Nada del ladrillo del Sobotta. Solo el Prometheus se le acerca.
Lo escribió Henry Gray, un cirujano inglés en la treintena junto a un ilustrador. Hicieron el mapa más preciso del cuerpo humano.
Y un día de 1861, su sobrino de diez años enfermó de viruela. Henry lo cuidó, sin separarse de él. El niño se curó.
Henry no. Murió con 34 años. Pero es que encima, murió la misma mañana en que tenía la entrevista para un puesto que llevaba años persiguiendo.
Esa viruela que se lo llevó es, hoy, la única enfermedad que la humanidad ha borrado del planeta.
Henry Gray nunca llegó a su entrevista. Pero lleva siglo y medio dando clase en cada facultad del mundo. Si, y también la serie…
#LaTraumatologaGeek
10
39
204
3,054
Rafael Sirera retweeted

PERO QUÉ ES ESTO
(y dónde puedo conseguirlo)
133
207
1,735
208,262
Rafael Sirera retweeted
Jun 13
Jun 13
Today you are going to discover the most intense love story ever told. A union that revolutionised biotechnology and, at the same time, taught us why we should not eat raw egg.
To avoid any misunderstanding, I am referring to molecular love, and to another aspect of the egg quite apart from microbial food safety. Let’s get into it.
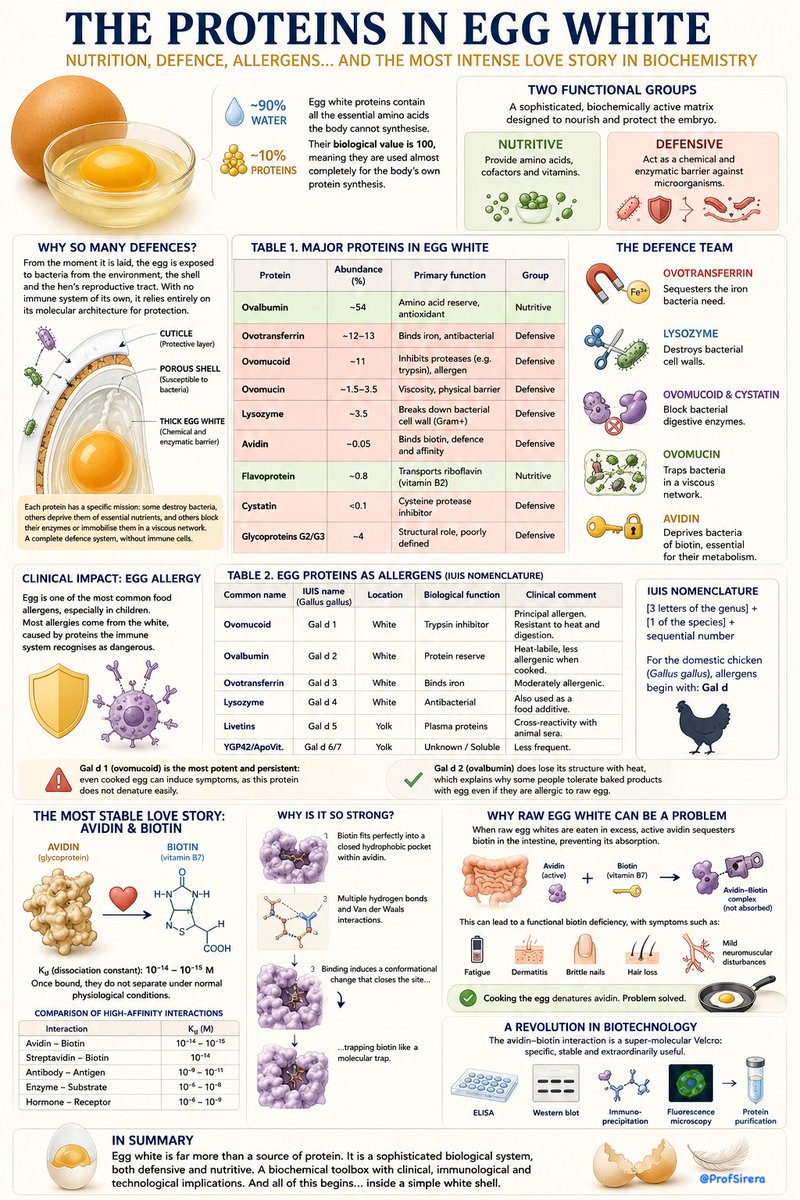
Egg white is composed of approximately 90% water and 10% protein.
And here is the key point: these proteins contain all the essential amino acids the body needs and cannot synthesise on its own.
That is why their biological value is 100, meaning they are used almost completely for the body’s own protein synthesis.
But egg white is far more than a protein source. It is a viscous, sophisticated, biochemically active matrix, designed to nourish and protect the embryo in an environment that, from the very first moment, is vulnerable to microbial contamination.
Its proteins can be classified into two functional groups:
- Nutritive, which supply the embryo with amino acids, cofactors and vitamins.
- Defensive, which act as a chemical and enzymatic barrier against microorganisms that may enter through the porous shell.
Why so many defences in something we think of simply as food?
Because from the moment it is laid, the egg is exposed to bacteria from the environment, the shell, and the hen’s reproductive tract. And since it has no immune system of its own, it depends entirely on its protective molecular architecture.
The egg is not a sterile environment. Its shell is porous, and although it has a protective cuticle, it remains susceptible to bacterial colonisation.
The egg white acts as a chemical barrier against these attacks. Each protein has a specific mission: some destroy bacteria, others deprive them of essential nutrients such as iron, and others block their enzymes or immobilise them within a viscous network. It is a complete defence system, without the need for immune cells.
In short:
- Ovotransferrin sequesters the iron bacteria need.
- Lysozyme destroys their cell walls.
- Ovomucoid and cystatin block their digestive enzymes
- Ovomucin traps them physically in a viscous network.
And importantly, Avidin deprives them of biotin, which is essential for their metabolism.
And this is the most stable biochemical love story ever observed.
Avidin binds to biotin (vitamin B7) with an almost irreversible strength. Its dissociation constant (Kd) lies between 10⁻¹⁴ and 10⁻¹⁵ M.
Once bound, they do not separate under normal physiological conditions. It is the highest-affinity interaction in nature. Compare it with other strong molecular interactions and the difference is remarkable.
Biotin is an essential water-soluble vitamin.
It is found in liver, oily fish, nuts, legumes, egg yolk… and is also produced in part by your intestinal microbiota.
When raw egg whites are eaten in excess, active avidin sequesters biotin in the intestine, preventing its absorption. This can lead to a functional deficiency, with symptoms such as:
Fatigue
Dermatitis
Brittle nails
Hair loss
Mild neuromuscular disturbances
Cooking the egg denatures avidin. Problem solved.
Why is the avidin–biotin bond so strong?
Biotin fits perfectly into a closed hydrophobic pocket within avidin.
There are multiple hydrogen bonds and Van der Waals forces.
Binding induces a conformational change that physically closes the site, like a molecular trap.
But the story does not end there.
The avidin–biotin interaction has revolutionised molecular biotechnology. It is a kind of super-molecular Velcro: specific, stable, and extraordinarily useful. It is used in:
ELISA
Western blot
Immunoprecipitation
Fluorescence microscopy
Protein purification
This defensive system also has clinical consequences. Egg is one of the most common food allergens, especially in children. Most egg allergies arise from the white and are caused by proteins that the immune system recognises as dangerous.
In summary: egg white is far more than a source of protein.
It is a sophisticated biological system, both defensive and nutritive. A biochemical toolbox with clinical, immunological, and technological implications.
And all of this begins… inside a simple white shell.
2
2
263
Rafael Sirera retweeted
Jun 13
Here is the perfect visual companion to my previous written post on egg white proteins, allergens, and the most intense love story in biochemistry: avidin and biotin.
Because the egg is not just food. It is a molecular fortress: nutritious, defensive, allergenic, and technologically extraordinary.
2
13
32
881
Rafael Sirera retweeted
Jun 13
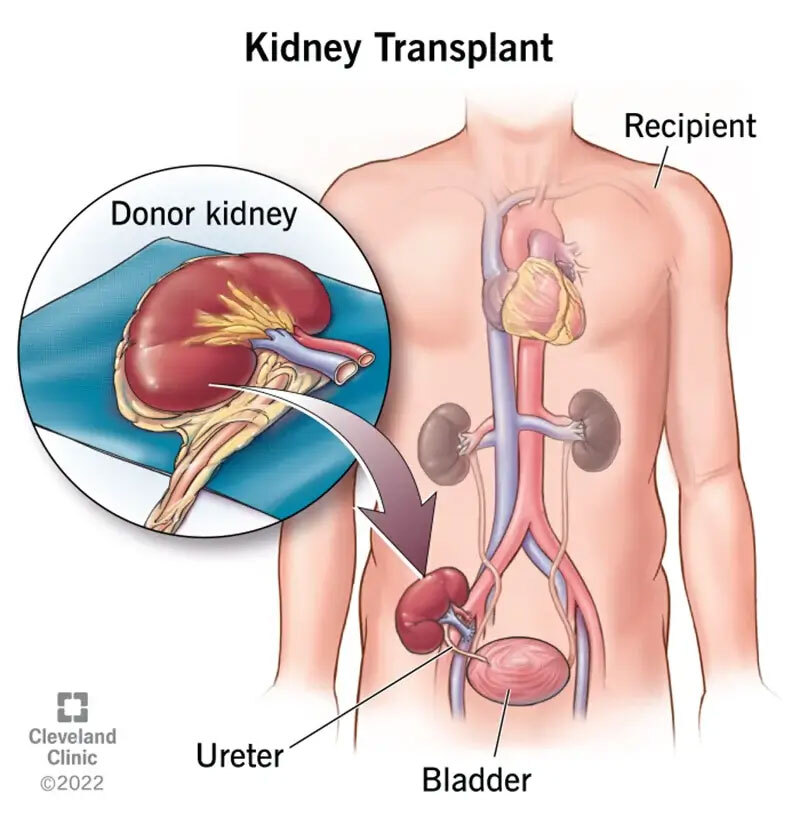
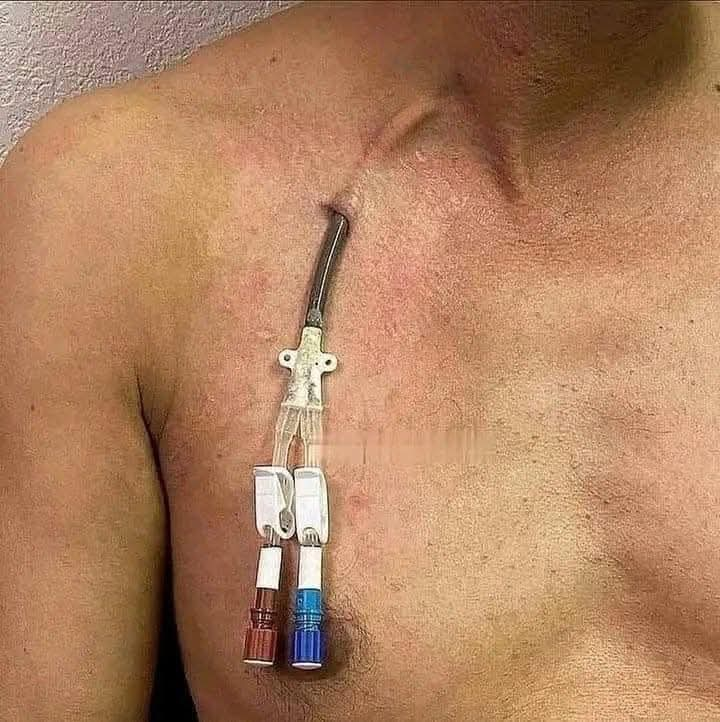
In Spain, where waiting times for transplantation may be only a few weeks in patients with a favourable blood group and immunological genetic profile, many nephrology departments place these catheters not while waiting for a fistula — which has haemodynamic consequences — but while waiting for the transplant itself.
1
4
9
5,955
Rafael Sirera retweeted

What is this catheter called?
50
10
353
189,426
Jun 13
Here is the perfect visual companion to my previous written post on egg white proteins, allergens, and the most intense love story in biochemistry: avidin and biotin.
Because the egg is not just food. It is a molecular fortress: nutritious, defensive, allergenic, and technologically extraordinary.
2
13
32
881
Jun 13
Jun 13
Today you are going to discover the most intense love story ever told. A union that revolutionised biotechnology and, at the same time, taught us why we should not eat raw egg.
To avoid any misunderstanding, I am referring to molecular love, and to another aspect of the egg quite apart from microbial food safety. Let’s get into it.
Egg white is composed of approximately 90% water and 10% protein.
And here is the key point: these proteins contain all the essential amino acids the body needs and cannot synthesise on its own.
That is why their biological value is 100, meaning they are used almost completely for the body’s own protein synthesis.
But egg white is far more than a protein source. It is a viscous, sophisticated, biochemically active matrix, designed to nourish and protect the embryo in an environment that, from the very first moment, is vulnerable to microbial contamination.
Its proteins can be classified into two functional groups:
- Nutritive, which supply the embryo with amino acids, cofactors and vitamins.
- Defensive, which act as a chemical and enzymatic barrier against microorganisms that may enter through the porous shell.
Why so many defences in something we think of simply as food?
Because from the moment it is laid, the egg is exposed to bacteria from the environment, the shell, and the hen’s reproductive tract. And since it has no immune system of its own, it depends entirely on its protective molecular architecture.
The egg is not a sterile environment. Its shell is porous, and although it has a protective cuticle, it remains susceptible to bacterial colonisation.
The egg white acts as a chemical barrier against these attacks. Each protein has a specific mission: some destroy bacteria, others deprive them of essential nutrients such as iron, and others block their enzymes or immobilise them within a viscous network. It is a complete defence system, without the need for immune cells.
In short:
- Ovotransferrin sequesters the iron bacteria need.
- Lysozyme destroys their cell walls.
- Ovomucoid and cystatin block their digestive enzymes
- Ovomucin traps them physically in a viscous network.
And importantly, Avidin deprives them of biotin, which is essential for their metabolism.
And this is the most stable biochemical love story ever observed.
Avidin binds to biotin (vitamin B7) with an almost irreversible strength. Its dissociation constant (Kd) lies between 10⁻¹⁴ and 10⁻¹⁵ M.
Once bound, they do not separate under normal physiological conditions. It is the highest-affinity interaction in nature. Compare it with other strong molecular interactions and the difference is remarkable.
Biotin is an essential water-soluble vitamin.
It is found in liver, oily fish, nuts, legumes, egg yolk… and is also produced in part by your intestinal microbiota.
When raw egg whites are eaten in excess, active avidin sequesters biotin in the intestine, preventing its absorption. This can lead to a functional deficiency, with symptoms such as:
Fatigue
Dermatitis
Brittle nails
Hair loss
Mild neuromuscular disturbances
Cooking the egg denatures avidin. Problem solved.
Why is the avidin–biotin bond so strong?
Biotin fits perfectly into a closed hydrophobic pocket within avidin.
There are multiple hydrogen bonds and Van der Waals forces.
Binding induces a conformational change that physically closes the site, like a molecular trap.
But the story does not end there.
The avidin–biotin interaction has revolutionised molecular biotechnology. It is a kind of super-molecular Velcro: specific, stable, and extraordinarily useful. It is used in:
ELISA
Western blot
Immunoprecipitation
Fluorescence microscopy
Protein purification
This defensive system also has clinical consequences. Egg is one of the most common food allergens, especially in children. Most egg allergies arise from the white and are caused by proteins that the immune system recognises as dangerous.
In summary: egg white is far more than a source of protein.
It is a sophisticated biological system, both defensive and nutritive. A biochemical toolbox with clinical, immunological, and technological implications.
And all of this begins… inside a simple white shell.
2
2
263
Jun 13
Today you are going to discover the most intense love story ever told. A union that revolutionised biotechnology and, at the same time, taught us why we should not eat raw egg.
To avoid any misunderstanding, I am referring to molecular love, and to another aspect of the egg quite apart from microbial food safety. Let’s get into it.
Egg white is composed of approximately 90% water and 10% protein.
And here is the key point: these proteins contain all the essential amino acids the body needs and cannot synthesise on its own.
That is why their biological value is 100, meaning they are used almost completely for the body’s own protein synthesis.
But egg white is far more than a protein source. It is a viscous, sophisticated, biochemically active matrix, designed to nourish and protect the embryo in an environment that, from the very first moment, is vulnerable to microbial contamination.
Its proteins can be classified into two functional groups:
- Nutritive, which supply the embryo with amino acids, cofactors and vitamins.
- Defensive, which act as a chemical and enzymatic barrier against microorganisms that may enter through the porous shell.
Why so many defences in something we think of simply as food?
Because from the moment it is laid, the egg is exposed to bacteria from the environment, the shell, and the hen’s reproductive tract. And since it has no immune system of its own, it depends entirely on its protective molecular architecture.
The egg is not a sterile environment. Its shell is porous, and although it has a protective cuticle, it remains susceptible to bacterial colonisation.
The egg white acts as a chemical barrier against these attacks. Each protein has a specific mission: some destroy bacteria, others deprive them of essential nutrients such as iron, and others block their enzymes or immobilise them within a viscous network. It is a complete defence system, without the need for immune cells.
In short:
- Ovotransferrin sequesters the iron bacteria need.
- Lysozyme destroys their cell walls.
- Ovomucoid and cystatin block their digestive enzymes
- Ovomucin traps them physically in a viscous network.
And importantly, Avidin deprives them of biotin, which is essential for their metabolism.
And this is the most stable biochemical love story ever observed.
Avidin binds to biotin (vitamin B7) with an almost irreversible strength. Its dissociation constant (Kd) lies between 10⁻¹⁴ and 10⁻¹⁵ M.
Once bound, they do not separate under normal physiological conditions. It is the highest-affinity interaction in nature. Compare it with other strong molecular interactions and the difference is remarkable.
Biotin is an essential water-soluble vitamin.
It is found in liver, oily fish, nuts, legumes, egg yolk… and is also produced in part by your intestinal microbiota.
When raw egg whites are eaten in excess, active avidin sequesters biotin in the intestine, preventing its absorption. This can lead to a functional deficiency, with symptoms such as:
Fatigue
Dermatitis
Brittle nails
Hair loss
Mild neuromuscular disturbances
Cooking the egg denatures avidin. Problem solved.
Why is the avidin–biotin bond so strong?
Biotin fits perfectly into a closed hydrophobic pocket within avidin.
There are multiple hydrogen bonds and Van der Waals forces.
Binding induces a conformational change that physically closes the site, like a molecular trap.
But the story does not end there.
The avidin–biotin interaction has revolutionised molecular biotechnology. It is a kind of super-molecular Velcro: specific, stable, and extraordinarily useful. It is used in:
ELISA
Western blot
Immunoprecipitation
Fluorescence microscopy
Protein purification
This defensive system also has clinical consequences. Egg is one of the most common food allergens, especially in children. Most egg allergies arise from the white and are caused by proteins that the immune system recognises as dangerous.
In summary: egg white is far more than a source of protein.
It is a sophisticated biological system, both defensive and nutritive. A biochemical toolbox with clinical, immunological, and technological implications.
And all of this begins… inside a simple white shell.
3
5
8
792
Jun 13
As far as I know, ovotransferrin is one of the most heat-labile proteins in egg white, more heat-sensitive than ovalbumin. However, denaturation is not the same as loss of allergenicity. Heating unfolds the protein, but the immune system may still recognise remaining linear epitopes.
1
2
137
Rafael Sirera retweeted
Jun 12
Summer arrives and people want to go to the beach and, despite the heat, get as tanned as possible. For several reasons, I do not understand this passion some people have for tanning. Mainly because you burn yourself and, worse still, you put your future health at risk.
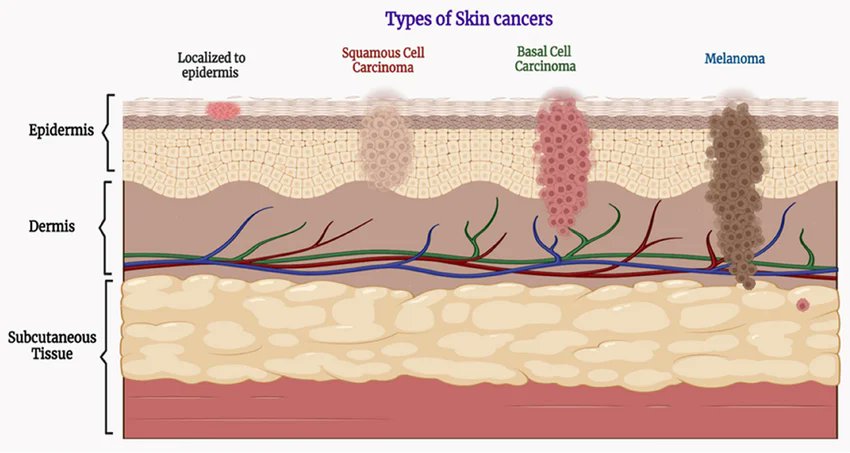
Yes, good guess: I am going to talk about melanoma, the most lethal malignant tumour affecting the skin, and one that in recent years has gone from being a very uncommon tumour to becoming the fifth most commonly diagnosed malignant tumour in countries such as the USA.
We are dealing with a scenario very similar to tobacco. I am sorry to say it, but for me there is a clear parallel between people who deliberately sunbathe today and smokers several decades ago.
Both are tumours with high incidence, and the worst part — or the best, depending on how one looks at it — is that they are clearly preventable because we know their main trigger. Do not smoke and do not expose yourself excessively to the sun, and the problem largely disappears.
Fortunately, in Western countries, fewer and fewer people smoke. In the USA, adult smoking fell from 21% in 2005 to 13% in 2020. Education and preventive measures are doing their work. Now it is melanoma’s turn.
UV light accounts for approximately 10% of the radiation emitted by the Sun, although humans cannot see it. It is non-ionising radiation. Although it enables vitamin D formation in vertebrates, it also burns the skin and damages DNA.
For life to progress, therefore, living organisms had to “develop and invent” ways of protecting themselves from UV rays. This radiation creates pyrimidine dimers, which distort the DNA strand and prevent it from being properly read.
First came what we might call an indirect conquest: the creation of the ozone layer. In the upper layers of the atmosphere, oxygen can naturally combine into this triatomic form, which has the ability to absorb a large proportion of UV radiation.
But that is not enough to free us from its harmful effects. Living organisms also had to invent a biological system to reverse the damage that UV radiation causes to DNA, to the genetic information of living beings.
This mechanism is universal. All living organisms must be able to correct UV-induced mutations in the genome. LUCA, the last universal common ancestor of all living beings, already possessed it.
The simplest and most widespread mechanism is based on photolyases, enzymes capable of reversing this damage, mainly that caused by the formation of thymine dimers. There are also other, more complex mechanisms that can repair these errors.
So it is curious that all living organisms have had to protect themselves from this solar radiation, and yet we humans decide to expose ourselves to it so aggressively. As if this problem somehow did not apply to us. But it most certainly does.
Skin cancers are the most common malignant tumours in humans. Yes, you heard that correctly. The most common. It is estimated that, in the USA alone, more than 2 million were diagnosed in 2025. Fortunately, many of them are completely treatable.
But among these millions, around 1 in 20 are melanomas, which, without treatment, can become invasive and lethal. A major problem is that the number of melanomas is increasing.
Between 1950 and 2007, its incidence increased 17-fold in men and 9-fold in women.
Dermatologists several decades ago might see the occasional melanoma during their residency. Today, they see several cases every month. Melanoma is the most commonly diagnosed cancer in women aged 25 to 29.
Melanoma is currently the fifth most commonly diagnosed cancer in the USA. There are additional risk factors. Fair skin increases the risk 20- to 30-fold. Freckles and pigmented lesions also increase the risk.
Other factors include polymorphisms or mutations in DNA repair systems, as well as immunosuppression. And as a final note, we should remember that this damage is cumulative. Today’s exposures will take their toll in the future.
Do not expose yourself excessively to the sun. And if you do, use sunscreen.

2
4
282
Jun 13
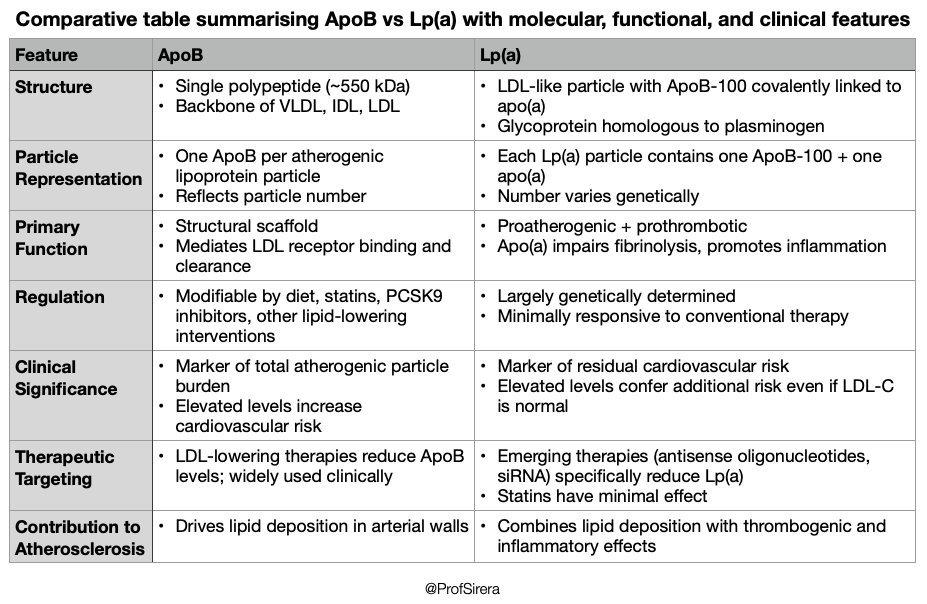
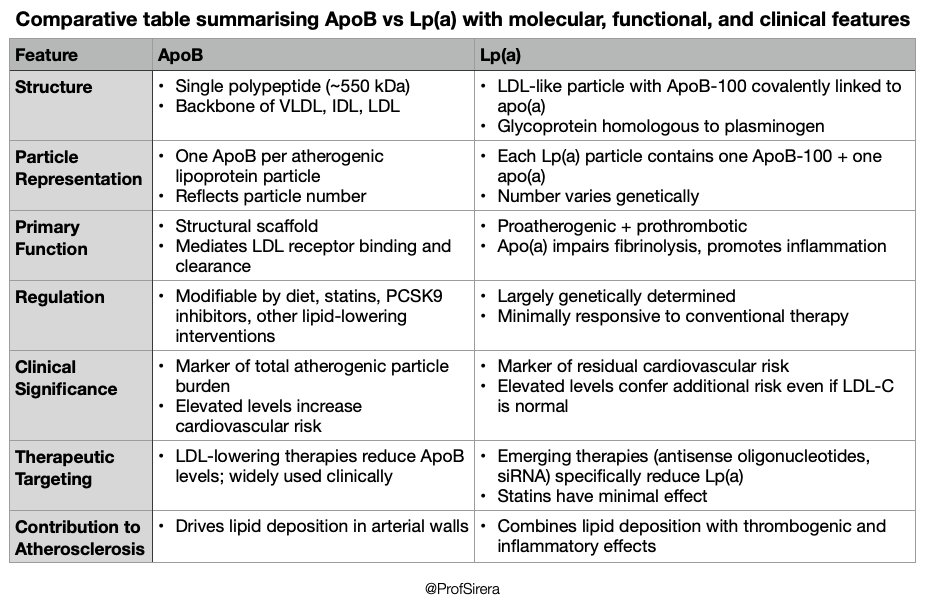
RT @Khalid78blue: 📋Interesting comparison between 2 particles driving the future for optimized ways in reducing cardiovascular risks ❤️
1
Rafael Sirera retweeted
Jun 12
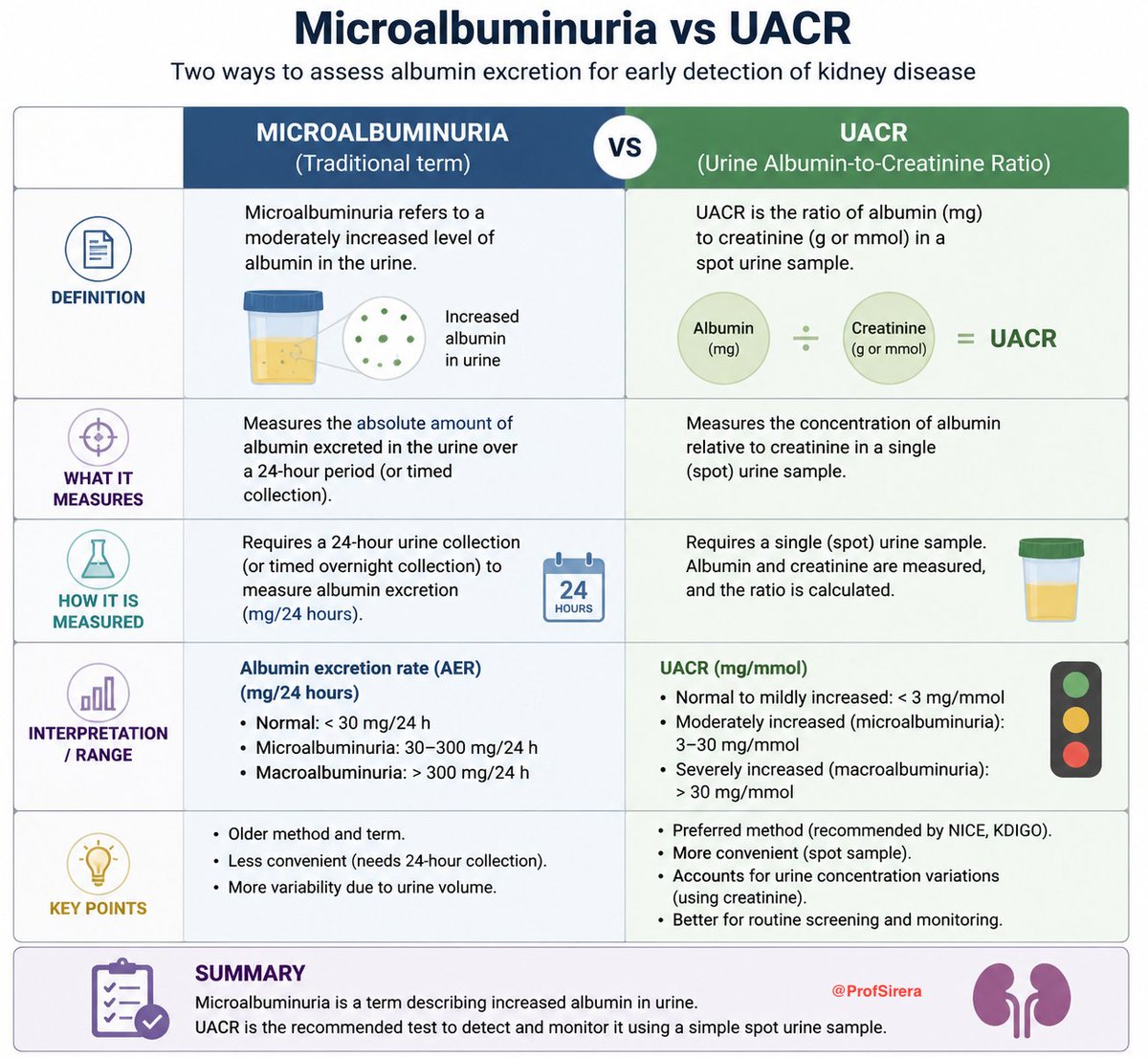
Urine Albumin-to-Creatinine Ratio (UACR) has largely replaced traditional microalbuminuria measurement in modern practice because it is simpler, reliable, and more practical for population screening, especially in patients with diabetes or hypertension. Microalbuminuria remains relevant as a historical concept or when 24-hour urine collections are specifically required.
44
81
2,470