
Professor of medicine | medical oncologist | Head @EHCSMonash | Chair, @ANZUPtrials | husband, father, grandfather, blessed | want to make a positive difference
Joined June 2016
- Tweets 10,928
- Following 621
- Followers 2,987
- Likes 16,057
1,146 Photos and videos







Pinned Tweet

10 Jun 2017
Happiness is an empty beach, the wind in your ears, your best friend by your side, and 0/8 feet on the ground

4
5
67
Fun fact: if toothpaste, even so tiny a piece that it cannot be seen, flicks off one bristle and lands in your eye, it stings like anything.
How’s your day going?
2
3
387
Ian Davis (Bluesky @profiand) retweeted

Jun 4
Great to see the @ANZUPtrials #BCGMM trial feature as a @EUplatinum Spotlight Video #ProfDickonHayne @Prof_IanD youtube.com/shorts/wtu8jHr96…
1
1
203
Ian Davis (Bluesky @profiand) retweeted

Twice today already at ASCO I have heard presenters say “patients failed treatment”.
Can we please, please stop that?
Treatments fail patients, not the other way around…
4
14
75
3,558
Let us not discount the importance of grade 2 xerostomia:
CTCAE v5:
“Moderate symptoms; oral intake alterations (e.g., copious water, other
lubricants, diet limited to purees and/or soft, moist foods); unstimulated saliva 0.1 to 0.2 ml/min”
#ASCO26
2
284
Ian Davis (Bluesky @profiand) retweeted

May 30
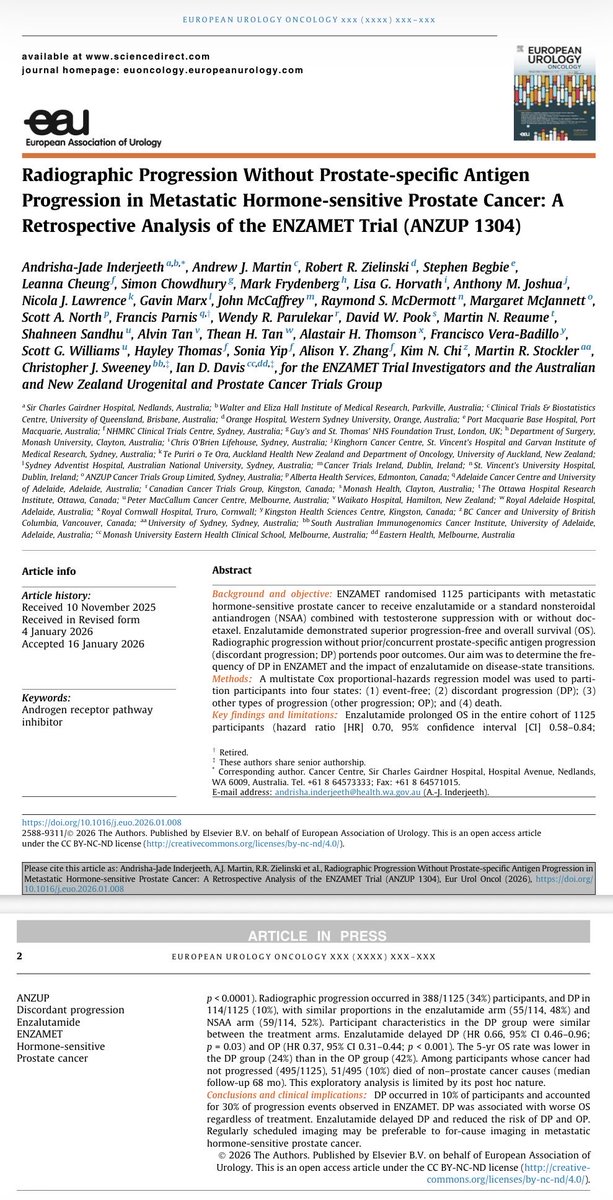
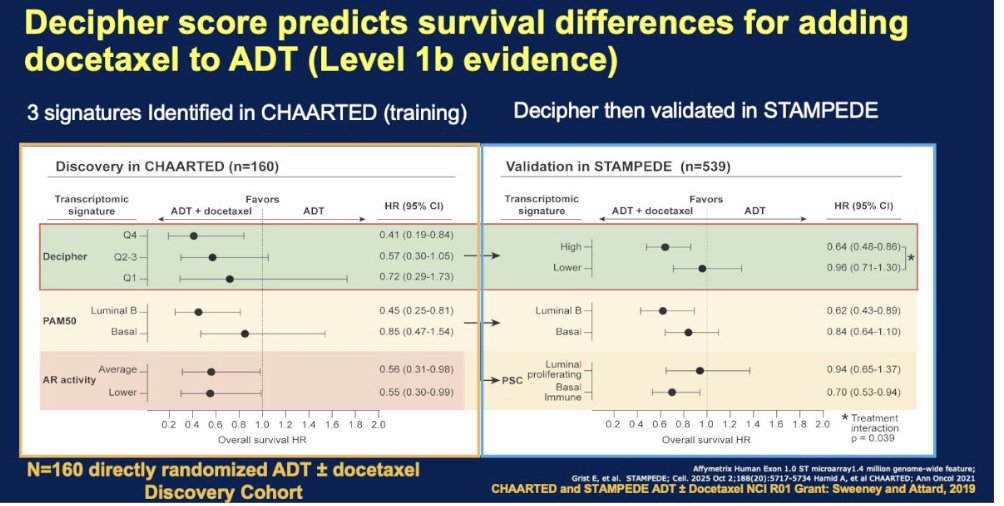
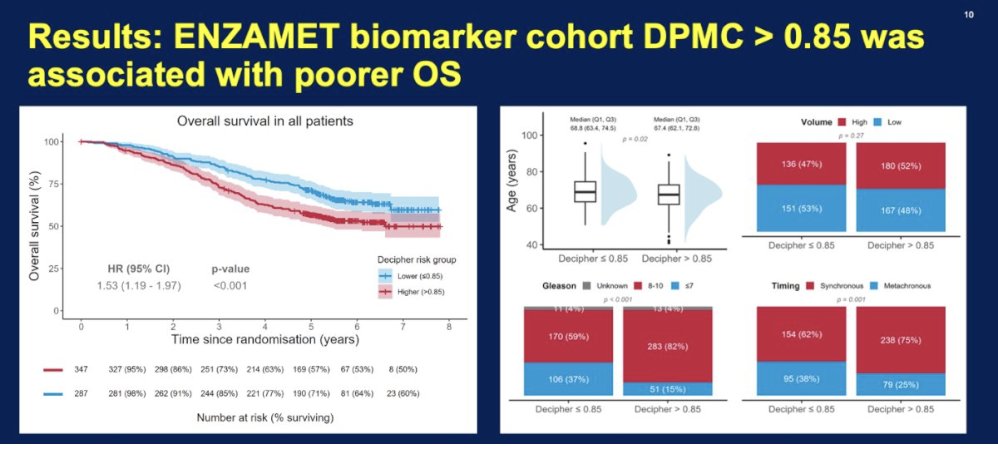
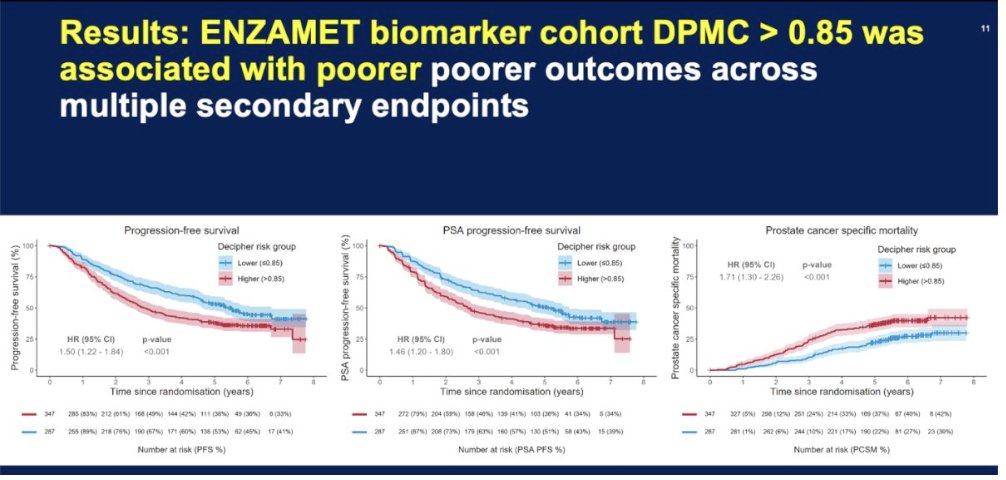
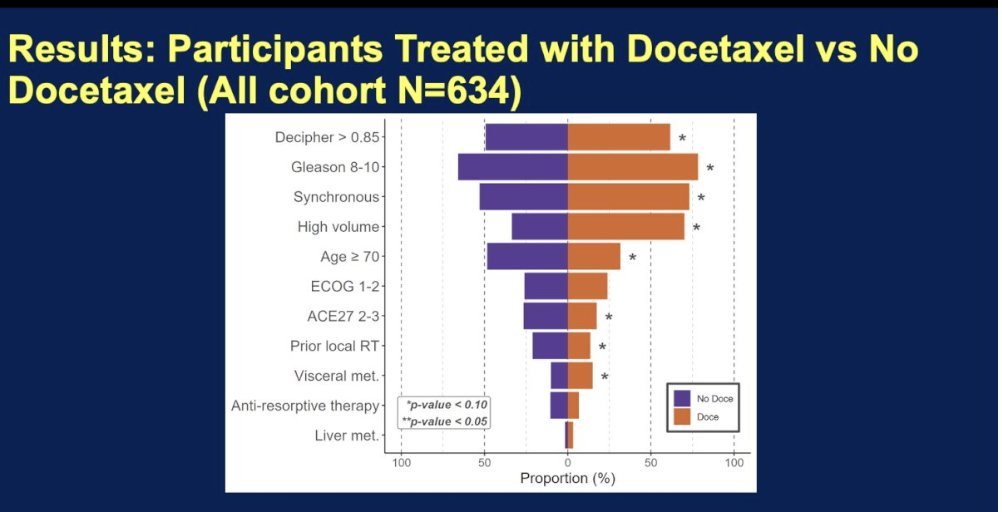
Assessment of the ability of #Decipher #Prostate genomic classifier >0.85 to identify patients who benefit from adding docetaxel to ADT enzalutamide: Level 1B evidence from the #ENZAMET study. Presentation by @ChrisSweens1 @UniofAdelaide. #ASCO26 written coverage by @RKSayyid @UAUrology > bit.ly/4ei2B3J @ASCO @Decipher_VCYT
1
12
19
931
Ian Davis (Bluesky @profiand) retweeted

📢Louder for the folks in the back 📢 #pallonc #supponc #ASCO26
@PallOncCoP
@MazieTsangMD
@DarcyBurbage
@Chaosdyna
@crisbergerot
@GretchenMcnally
@BbaharK
@asfeen_ummul
@veladconmigo
@FionnualaCrowle
@jillfeldman4
@IshwariaMD
@SrinishantR
@AjuVaniBabu
@rabrazzak
@TamrynGray
@anhbl9

And @fizazi_karim just made the critically important points that:
* Referral to clinical trials should always be considered if available
* Palliative care and active treatment can (I think must!) be used together.
My footnote: understand your patient’s goals of care.
#ASCO26
1
4
7
678
Wonderful talk by @drlouiseemmett in #ASCO26 educational session on “How to Better Personalize Treatment With Lu-PSMA,” highlighting the amazing clinical and translational outcomes of many studies especially @ANZUPtrials #TheraP and #ENZAp. These great trials continue to deliver.
2
4
11
667
And @fizazi_karim just made the critically important points that:
* Referral to clinical trials should always be considered if available
* Palliative care and active treatment can (I think must!) be used together.
My footnote: understand your patient’s goals of care.
#ASCO26
1
5
879
A quiet and profound tragedy and indictment on society buried in the footnote of an #ASCO26 slide:
“1 patient off study after cycle 1 due to insurance coverage issues.”
3
1
21
2,734
An admirable quality in family, friends, colleagues, charities…
For a bus going to a specific destination: not so much.
#ASCO26
1
6
260
“Manageable toxicity” at #ASCO26
(thanks to @MelJurgens for inspiration):
4
10
769
Masterful discussion by @declangmurphy of #PROTEUS in #ASCO26 LBA1 plenary, complete with an incidental and effective drive by swipe at inappropriate ARPI switch controls. And nods to #ENZARAD, and to @ANZUPtrials @ChrisSweens1 proposed freedom from clinical detriment endpoint.
4
12
1,283
#ASCO26 plenary sessions are about to start. At least one will warrant a standing ovation and at least one does not, in my opinion. I hope any standing ovations that occur are actually real and not orchestrated (as if such a thing has ever happened before…)
3
1
16
5,225
The piano…
#ASCO26
ohchr.org/en/instruments-mec…
1
2
359
Ian Davis (Bluesky @profiand) retweeted

One of the best parts of #ASCO26 is reconnecting with friends and colleagues. Always wonderful to see @Prof_IanD @oncology_bg @PauloBergerot during the poster session and catch up amidst the excitement of the meeting! @ASCO
4
19
722

Ian Davis (Bluesky @profiand) retweeted

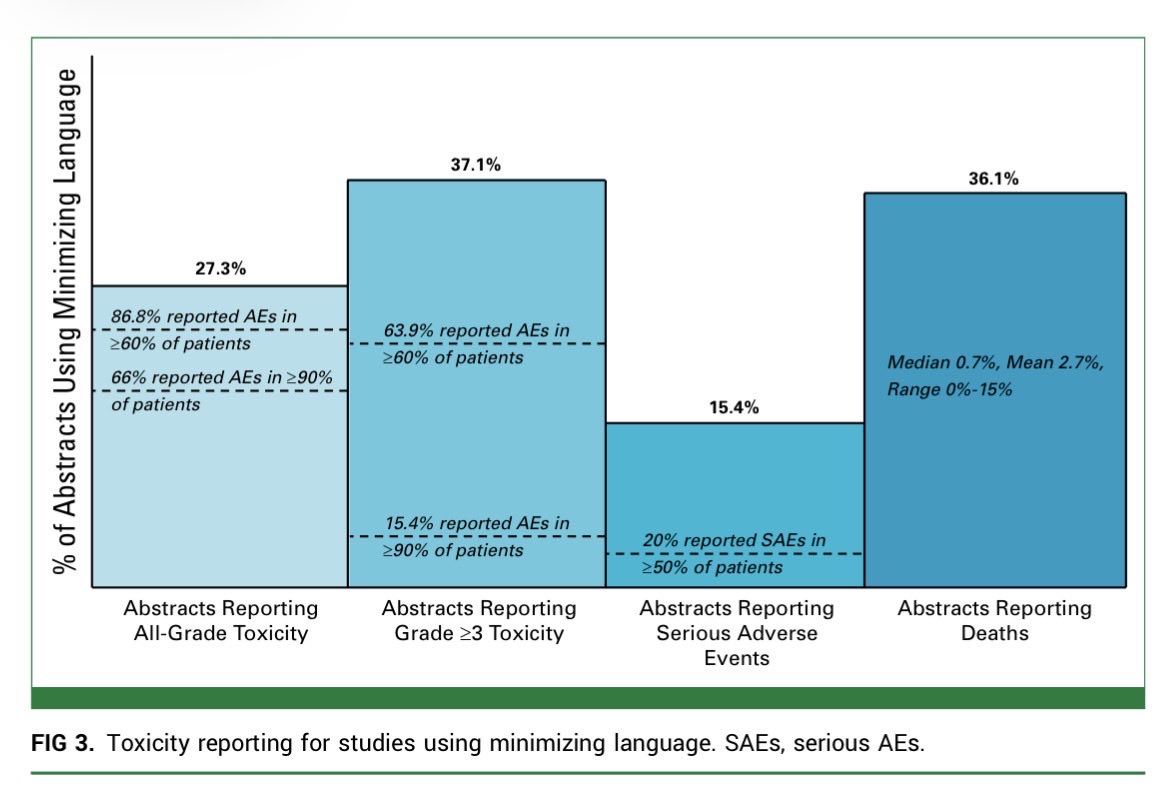
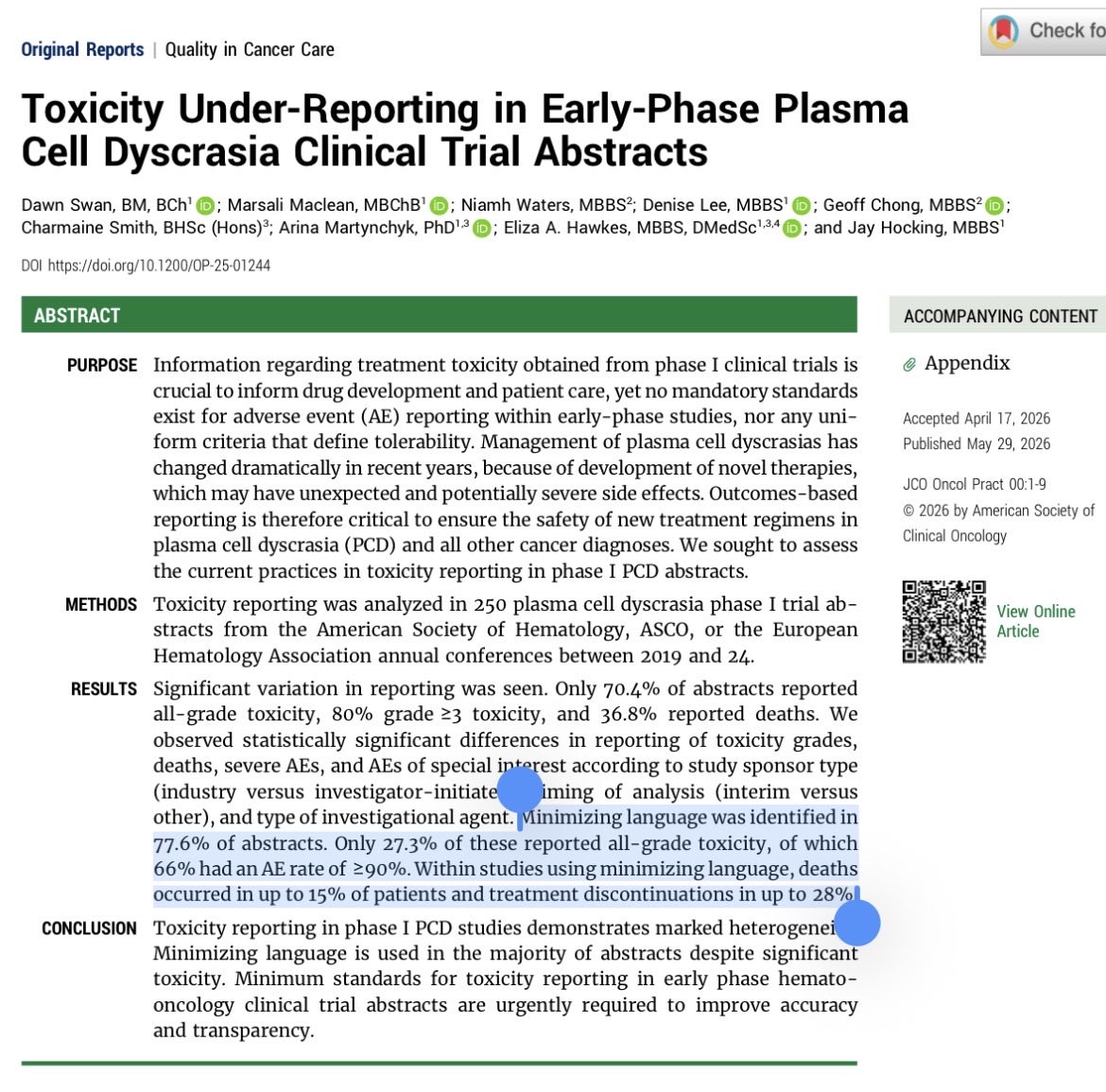
And the flip side of this, “well-tolerated”
In 250 Ph1 #MMSM ASCO/ASH/EHA abstracts, 194 (78%) used it or similar terms…
In those studies 15% of patients died & 28% had to discontinue tx.
#ASCO26 #ASH26
ascopubs.org/doi/10.1200/OP-…

Did not have to wait long at #ASCO26 to hear “numerically greater”…
2
7
14
3,955