
We do not rise to the level of our expectations, we fall to the level of our training.
Joined July 2016
- Tweets 1,715
- Following 624
- Followers 1,075
- Likes 509
304 Photos and videos












Meghana V Kashyap, MD retweeted

Apr 17
A 2.5% “efficiency adjustment” wRVU cut is now in effect.
If your institution hasn’t acknowledged it or discussed its impact, that’s a problem.
With Don Selzer, we outline what this means for productivity benchmarks (@JAMASurgery):
jamanetwork.com/journals/jam…
6
8
2,165
Meghana V Kashyap, MD retweeted
Plenty of doctors promote bad information online.
Certainty does not equal expertise.
I learned long ago that it's better to provide good information that try to battle bad information, so I humbly offer this level 1 evidence on the safety and efficacy of colonoscopy:
1. Colonoscopy is safe, and the risk of perforation during screening is 3.1 per 10,000, or 0.031%. If you are that unlucky 1 in 3,226 people, the risk of it killing you is less than 5%
Source: jamanetwork.com/journals/jam…
2. Colonoscopy reduces your chance of getting colorectal cancer, and it reduces your chance of dying from colorectal cancer. In fact, there's a 68% reduction in CRC mortality with colonoscopy.
Source: acpjournals.org/doi/10.7326/…
I try my best to ignore physicians who use twitter to promote pseudoscience and generate traffic to their websites, but it's Colorectal Cancer Awareness Month, so I feel obligated to share my thoughts.
5
37
75
7,763

In this episode of Gut Check, Jennifer Goldsack, Founder and CEO of the Digital Medicine Society (DiMe), joins our hosts to examine what it truly takes to make digital health safe, effective, and equitable.
As a survivor of late-stage colon cancer, Jennifer offers a perspective that is both personal and powerful—underscoring why patient-centered design cannot be an afterthought in the evolution of medicine.
🔗 Listen now: bit.ly/3YzjpvG
#ColorectalCancerAwarenessMonth #CRCawareness
1
2
311
A debated question in colorectal surgery takes center stage. In this episode, the hosts tackle laparoscopic lavage for acute diverticulitis—when it works, when it doesn’t, and why opinions still differ.
🔗 Listen now: bit.ly/3YzjpvG
Have a tough case or controversy you want explored next? Case Controversies is listener-driven. Share your ideas at communications@fascrs.org.
2
1
414
Meghana V Kashyap, MD retweeted
Feb 14
Text here: estes.house.gov/uploadedfile…
Direct link to take action here: facs.quorum.us/campaign/1536…
1
147
Meghana V Kashyap, MD retweeted
Feb 14
Legislation has been introduced to reverse @CMSGov "efficiency adjustment" that cuts wRVUs of all non-time-based codes by 2.5%. A herculean effort spearheaded by @AmCollSurgeons.
Surgeons - encourage your reps to sign on @SurgeonsVoice
Grateful to @RepTomSuozzi @RepRonEstes
1
2
2
201
Meghana V Kashyap, MD retweeted

Congratulations to Meghana Kashyap, M.D., on being selected as an alternate advisor-in-training on the AMA’s Relative Value Scale Update Committee, representing the American Society of Colon and Rectal Surgeons.
#UTSWSurgery #UTSW
1
5
388
When the case isn’t straightforward, the conversation shouldn’t be either.
Listen as our hosts discuss fistulas with special guest Dr. Jeff Van Eps. Hear practical perspectives, key decision points, and a spirited exchange you won’t want to miss.
🔗 Tune in: bit.ly/3YzjpvG
1
302
Meghana V Kashyap, MD retweeted

13 Dec 2025
We love this video! Quick tour of the abdomen with @e_magination95
More OR QUICK HITS ➡️➡️➡️ app.behindtheknife.org/video…
10
37
3,471
Meghana V Kashyap, MD retweeted

14 Dec 2025
Viewpoint: Delayed start to surgical practice by 1 or more years was associated with significant reductions in lifetime earnings, retirement funds, and home equity. @drdevirgilio ja.ma/4qaBBYb
1
54
275
113,139

3 Dec 2025
THIS. Similarly, why do we have to give our own interpretation of radiographic images to bill appropriately for a complex clinic visit?
2 Dec 2025

Yea and we should be able to bill for our reads as well
1
469
Meghana V Kashyap, MD retweeted

29 Nov 2025
Alex, the US taxpayer rarely pays doctors directly. They typically send money to states (Medicaid) Hospitals and Providers(traditional Medicare), to insurance carriers (MA and ACA), and indirectly through tax savings for individuals and employers )
You are right that we overpay. We spend far too much on healthcare.
We overspend because we send the most money to the carriers and give them every good reason, to scale as big as possible , to contract at inflated prices, to invent fees and to delay and deny care when they can. Then there are the PBMs etc etc
Break up the big carriers by vertical , make intercompany transfers at Medicare rates or best price until then , remove formularies from their PBMs, make extra cash purchase count against the deductible , make non profit hospitals and providers publish every general ledger entry , stop 340b abuse, I can go on for days on how we can reduce the cost of healthcare.
As far as over treating , there are lots of reasons. Lots of paperwork, lots of lawsuits, lots of economic incentives to generate more revenues.
But of all I just mentioned, the people that benefit the least financially, are the actual caregivers. Doctors and nurses get shit on regularly. They should be able to open their own practice and survive financially. They shouldn’t be at the mercy of insurance companies. They should get the same Medicare rates that hospitals get for the same work.
The best part of this is that you can help. Where do you get your insurance and who is your PBM Alex ?
How many companies have you educated to walk away from the biggest insurance carriers and their PBMs ?
29 Nov 2025

"Underpay"
I know you are not this ignorant, @mcuban. The US OVERPAYS at every level in healthcare, which is a key reason we overtreat, which is a key reason our outcomes stink.
We do NOT need to spend more money on medicine in the US, we would be better off spending less.
149
155
1,168
304,308
24 Nov 2025
Being a physician is no longer about patient care. It’s about the bottom line. Don’t think you don’t need to understand the business and finances as a doctor. @cchildersmd joins us on @ASCRS_1 Gut Check for a primer of the recent changes. open.spotify.com/episode/7hH…
1
2
5
1,627
Meghana V Kashyap, MD retweeted
14 Nov 2025
CMS has finalized a 2.5% cut to surgeon wRVUs for most non time-based codes starting on January 1 with additional reductions every 3 years. This WILL impact both private & employed surgeons.
@AmCollSurgeons is fighting this. We encourage all surgeons to learn more: shorturl.at/U6KCe
Watch this short video for important details:
youtube.com/watch?v=F1-CpdWZ…
3
10
33
7,211
Meghana V Kashyap, MD retweeted

17 Nov 2025
The clock is ticking. CMS payment cuts take effect Jan 1 unless Congress acts.
Tell lawmakers: Protect patients. Protect surgery.
Use SurgeonsVoice today. 🗣️ brnw.ch/21wXxXK
5
5
2,087
Meghana V Kashyap, MD retweeted
3 Nov 2025
Glad to see @AmCollSurgeons continuing to advocate on this issue. I'd encourage all physicians impacted by th @CMSGov "efficiency adjustment" to reach out to their representatives. @SurgeonsVoice is a super convenient way to do so. See link and flyer.
facs.org/media/anbetuqo/cms-…

6
8
1,056
Meghana V Kashyap, MD retweeted
1 Nov 2025
A quick primer on the "efficiency adjustment" just finalized by @CMSGov and the implications for surgeons @AmCollSurgeons @acsJACS
tl;dr - Your OR wRVUs are going down by 2.5% next year, time to engage your institutional leadership; more below...
6
21
57
19,322
4 Nov 2025
SURGEONS - pay attention. This is a big deal. We are getting progressively devalued and need to work together to prevent continued cuts.
4 Nov 2025

Don’t let CMS cut your pay and harm patients’ access to care. We need Congress to stop these harmful cuts before they take effect. Amplify our voice now by using SurgeonsVoice. 🗣️ brnw.ch/21wXaSE
6
36
13,871
Meghana V Kashyap, MD retweeted

2 Nov 2025
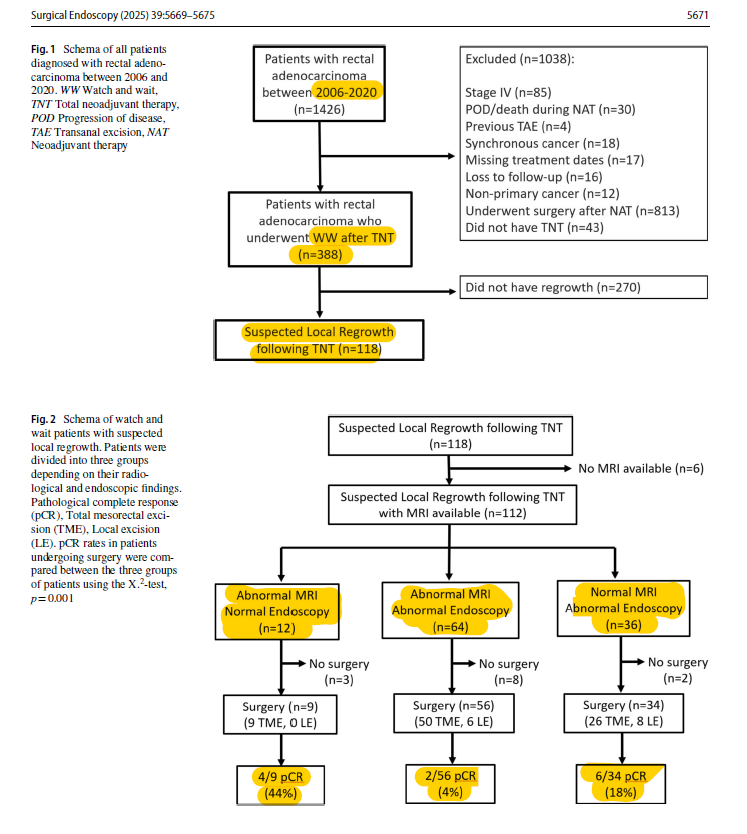
Interesting @SurgEndosc study from @MSKCancerCenter looking at patterns and detection of local regrowth in patients with rectal cancer who experience cCR after TNT and undergo watch-and-wait (2006-2020)
-Suspected local regrowth occurred in 30%
-Abnormal MRI with normal endoscopy was uncommon (11% of suspected regrowths) compared to Normal MRI/abnormal endoscopy (32%) and abnormalities on both MRI and endoscopy (57%)
-For patients undergoing salvage surgery, the rate of pCR was 44% in the MRI/-Endo group, 18% for the -MRI/ Endo group, and 4% for the MRI/ Endo group. This means residual/recurrent cancer was much more likely to be present in the final specimen if the endoscopy was abnormal.
-Of the 99 patients with salvage surgery and recurrent cancer on final pathology, only 1 patient (1%) had this recurrence detected by MRI alone.
Important caveats:
-This study goes back to 2006, and MRIs have certainly evolved during that time (as have TNT, surveillance, etc).
-All false positive MRI findings occurred after 2013, suggesting newer MRIs pick up subtle abnormalities that aren't necessarily cancer regrowth.
-pCR on final pathology shouldn't necessarily be considered a failure in management. These patients do very well.
What I take home from this study is that isolated irregularities on surveillance MRI can be safely monitored without proctectomy in the short-term...ie you can leave the rectum in for a little while and let the problem declare itself.
pubmed.ncbi.nlm.nih.gov/4065…
4
19
44
3,831
4 Oct 2025
What better way to celebrate being a newly BOARD CERTIFIED ✅ colorectal surgeon than a reunion with my co-chiefs from @UNMCSurgery (AKA the Glue) @AmCollSurgeons #ACSCC25?! I’m speaking Tuesday - come learn what is never taught in training!

3
3
21
2,609