
Practical, Innovative, Hyper-focused on saving lives. Immunologist, Virologist, Pandemic Nemesis. Posts are mine.
Joined January 2017
- Tweets 11,296
- Following 3,013
- Followers 49,408
- Likes 27,801
150 Photos and videos




Rick Bright retweeted

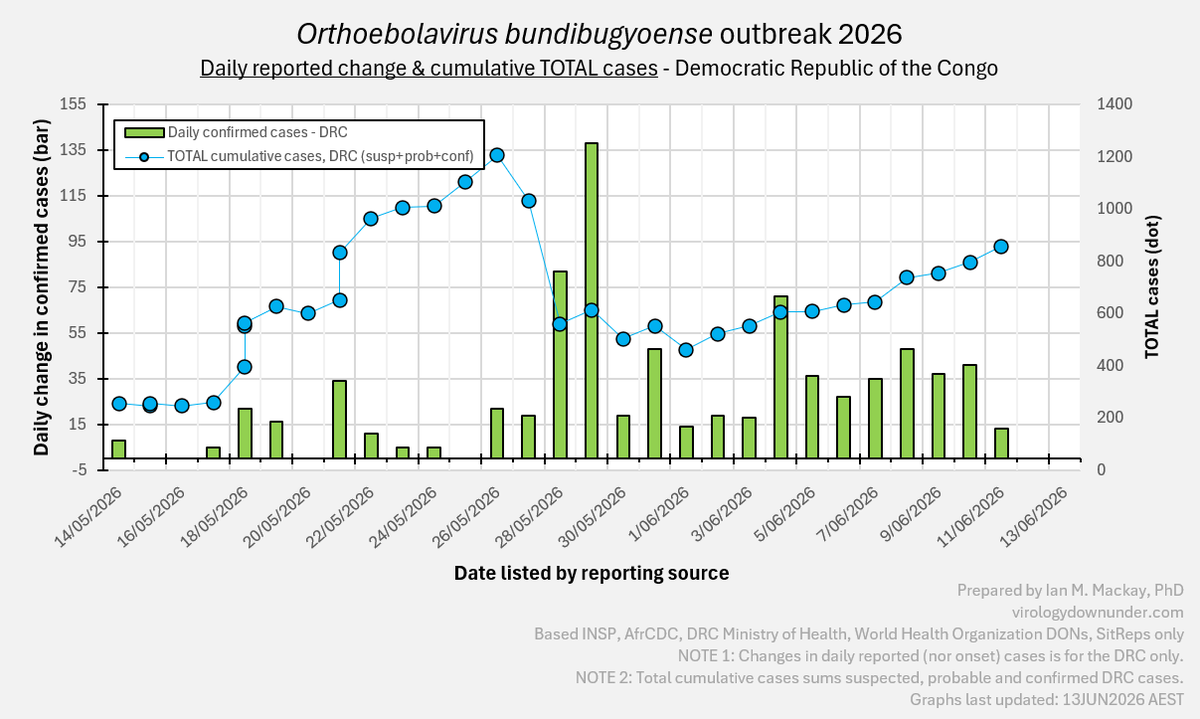
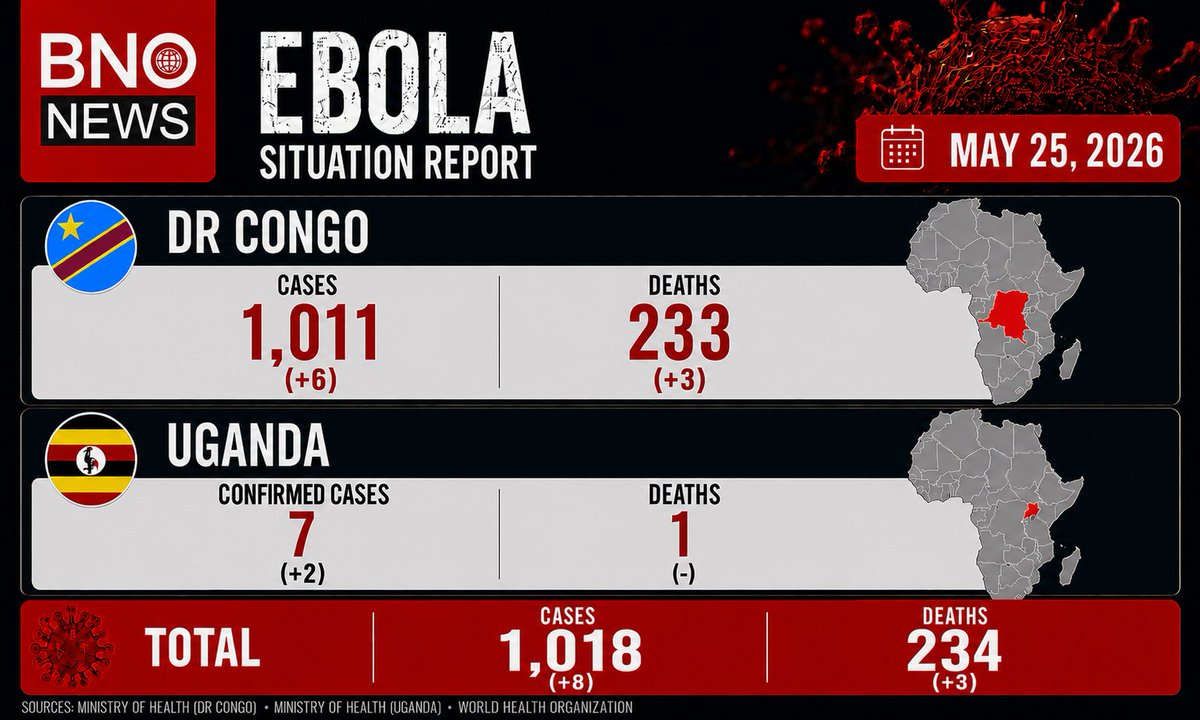
A low number of DRC-located confirmed #Ebola cases overnight - none new in Uganda.
But only 35 samples were analysed in Ituri; none in Nord Kivu (172 delayed) and nothing reported from South Kivu. Good news or a problem?
The contact tracing rate has dropped to 28% - need >90%
1
12
44
2,297
Rick Bright retweeted

Jun 4
Early Ebola symptoms mimic malaria & other common infections
With unknown transmission chains, anyone in an active area with these symptoms could have Ebola
PCR can't scale to screen all of them. Rapid tests are needed & could uncover hidden chains
thelancet.com/journals/lance…
3
33
89
7,253
Rick Bright retweeted
One PCR test in the DRC labs is a rapid test from KH Medical in South Korea, relying on the RADIONE extraction & amplification device (1 or 4-sample versions; 60min to result). It uses a range of their kits.
🧬 khmedical.co.kr/eng/products…
🧬 khmedical.co.kr/eng/products…

1
7
23
1,527
Rick Bright retweeted

NOW‼️ I’m now in the Global Coordination Meeting on this, we continue to hear about vaccines and treatments but yet there are no RDTs 17 years after this specie of Ebola was discovered - it is not NEW. Yet we still have no tools, because the people are poor and lives undervalued.
Jun 3

There is no rapid test for the current Ebola strain in eastern Congo. Because early Ebola symptoms are the same as for typhoid or malaria, and all people with those symptoms are isolated together, some people end up being infected with Ebola at the place they came for care. That discourages people who fall ill from seeking care and increases the chance they will infect others. nytimes.com/2026/06/02/healt…
1
11
18
4,245
Rick Bright retweeted

Jun 3
#ebola
⚠️⚠️
➡️ 🇨🇩 🇺🇬 Only the Right Tests Can Stop This Ebola Outbreak. Congo Has Hardly Any.
- A chronic lack of investment in development of better tests has left clinicians blind and allows deadly viruses to spread unchecked.
- ➡️ Months ago, doctors in Ituri Province in northeastern Democratic Republic of Congo started seeing patients with the vomiting, diarrhea and bleeding that are the hallmarks of Ebola. ➡️ The tests kept coming back negative.
- ➡️ It was weeks before samples from sick people — many of whom had already died — made it to the National Institute of Biomedical Research in the capital, Kinshasa. There, researchers used a different test that screened for more species of Ebola and related viruses.
- ➡️ They finally identified the culprit: a species of Ebola significantly different from the one the original test could detect. But by then, the outbreak had seeded across the border into Uganda and become a full-blown public health emergency.
- As health workers battle a devastating virus that has killed at least 49 people and infected 452 more so far, they have been hampered by a chronic lack of investment in high-quality tests for clinicians facing pathogens that surface in the most marginalized places.
- “We were looking for the Zaire strain while it was the Bundibugyo species that was wreaking havoc,” said Dr. Mamadou Kaba Barry, the head of mission in Congo for the aid organization Alliance for International Medical Action. Like many physicians in the region, he has responded to multiple Ebola outbreaks. The doctors who saw the first cases feared what they were seeing, but the negative tests confounded them.
- “There were alerts,” he said. “Yes, we took samples; yes, we did the test, but we did the test on the Zaire strain.”
- Because there is no vaccine to protect against this species of Ebola virus and no proven treatment, only public health measures like contact tracing can bring the outbreak under control. ➡️ Rapid and accurate diagnostics are essential: Health workers need to know who has the virus so they can isolate infected people away from uninfected ones and trace contacts.
- ⚠️ People who come to a health center with symptoms that could be Ebola will be isolated together — even though some may have typhoid or malaria, which can present with similar symptoms — and ⚠️ end up infected with Ebola at the place they came for care. ⚠️ That fear, in turn, discourages people who fall ill from seeking out care and increases the chances they will infect others in their communities.
- ⚠️ “There is no way to work on this disease without having diagnostics that are promptly accessible, and 🚨 we do not have rapid tests,” said Carmen Pérez Casas, the head of pandemic preparedness at Unitaid, a global health agency that funds accelerated access to diagnostics. 🚨 Confronting Ebola without a way to test, she said, “is terrifying.”
- Now, health workers, research labs and test developers are racing to meet the need, with some small improvement. Dr. Samuel-Roger Kamba, ⚠️ Congo’s health minister, told journalists in Bunia, the Ituri capital, on Saturday that ⚠️ testing is no longer delayed. ⚠️ “We have everything we need to cover current testing needs,” he said. ⚠️ “Today, all the samples that arrived — and we had about 71 yesterday — have all already been examined.”
- ➡️ In Bunia, the lab is now testing 150 samples per day, on four machines that screen for the genes of the virus, with no backlog.
- But ➡️ most of the samples come from sick people already in clinics, and ➡️ there is still little contact tracing in the community, the World Health Organization says. ➡️ Many hundreds of samples would need to be collected and tested within hours to bring the outbreak under control.
- In May, ➡️ the researchers at the national laboratory in Kinshasa who first identified Bundibugyo as the source of the outbreak used a genetic testing technology called ➡️ RADI-One, which can screen for all four Ebola species that affect humans as well as Marburg virus, another hemorrhagic fever that has caused outbreaks in the region.
- ➡️ The W.H.O. is working with the manufacturer of RADI-One, a small South Korean firm called KH Medical, to install about a dozen more machines in the region, said Dr. Nicksy Gumede-Moeletsi, a medical virologist with the organization.
- ➡️ Expanded access to this testing will address only part of the problem in Congo because ➡️ it relies on taking samples to a central lab — a slow and often fraught process in Ituri, where the road network is limited and violence persists.
- 🚨 There is no rapid test for Ebola like the home tests that became popular during the coronavirus pandemic — kits that would allow health workers in Ituri to quickly separate potential Ebola patients from uninfected people in clinics, and simplify contact tracing. While rapid tests for the virus do exist, they were designed for the Zaire species — and in any case, 🚨 because of the way Ebola viruses behave in the body, a rapid test cannot accurately identify sick people until their viral load is extremely high. ➡️ Such a test could, however, be used to confirm Ebola in people who have already died.
- But while the need for better tests has been clear for years, there has been little investment to develop them because there is no high-income market, said Sonjelle Shilton, who works on access to diagnostics for the aid group Doctors Without Borders.
- “That message was there: ➡️ We need pan-species Ebola tests — because they faced these same problems in the last Bundibugyo outbreak,” Ms. Shilton said. But ➡️ the private sector sees little incentive to invest in research and development for a diagnostic tool that will be used almost exclusively in the world’s poorest places, ➡️ the same reason there are no vaccines or treatments to deploy against Bundibugyo, she said.
- Until this outbreak, the RADI-One technology was not nearly as widely installed in Congo as the world’s most-used molecular diagnostic, GeneXpert.
- ➡️ The tests that originally came up negative for Ebola in the current outbreak were GeneXpert, which is made by the California-based company Cepheid. International funding helped install that technology in laboratories for testing during the coronavirus pandemic, and for H.I.V. and tuberculosis programs.
- However the GeneXpert test that Congolese labs are equipped for detects only the Zaire species of the Ebola virus, which has caused the largest outbreaks in the past.
- ➡️ Cepheid does have a test to detect Bundibugyo as well as other Ebola species. ➡️ The U.S. Food and Drug Administration has approved it for use by the U.S. Defense Department.
- Dr. Connie Savor, the chief medical officer for Cepheid, said ➡️ the company was committed to producing an initial run of 5,000 tests to respond to this outbreak. ➡️ But the test will have to be approved by regulators in Congo and recommended by the W.H.O. before it can be deployed. The slow-moving bureaucracy of these institutions has delayed response in other outbreaks, including Congo’s continuing mpox epidemic.
- “It comes down to, how quickly we can deploy across the different rules and different partners and the requirements of the countries: It could be a matter of weeks or months,” Dr. Savor said.
- She said it would be “premature” to discuss the price Cepheid would charge for these tests.
- Adam Hong, the chief executive of KH Medical, the company that makes the RADI-One tests, said the company was increasing its manufacturing capacity and expanding support activities in Congo and Uganda to respond to the Bundibugyo outbreak.
- While there is limited commercial market for these diagnostics, his company is committed to developing tests for pathogens that mostly affect people in the poorest places, Mr. Hong said. “We believe that strengthening access to diagnostics for emerging and neglected infectious diseases is an essential component of global health security,” he said.
By Stephanie Nolen
Declan Walsh contributed reporting from Bunia, Democratic Republic of Congo.
nytimes.com/2026/06/02/healt…
24
42
2,943
Rick Bright retweeted

extranet.who.int/prequal/vit… Call for diagnostic companies on their work on ebola bundibugyo
5
10
23
3,143
Rick Bright retweeted

#RDC: Le premier patient guéri de la 17ᵉ épidémie d’Ebola en RDC est sorti ce mercredi de l’hôpital en Ituri, a annoncé l’Incident Manager adjoint de l’Institut national de santé publique (INSP) depuis l’épicentre de la riposte. Un signal encourageant face à la souche Bundibugyo, pour laquelle il n’existe ni vaccin ni traitement homologué.
36
253
825
61,043

May 28
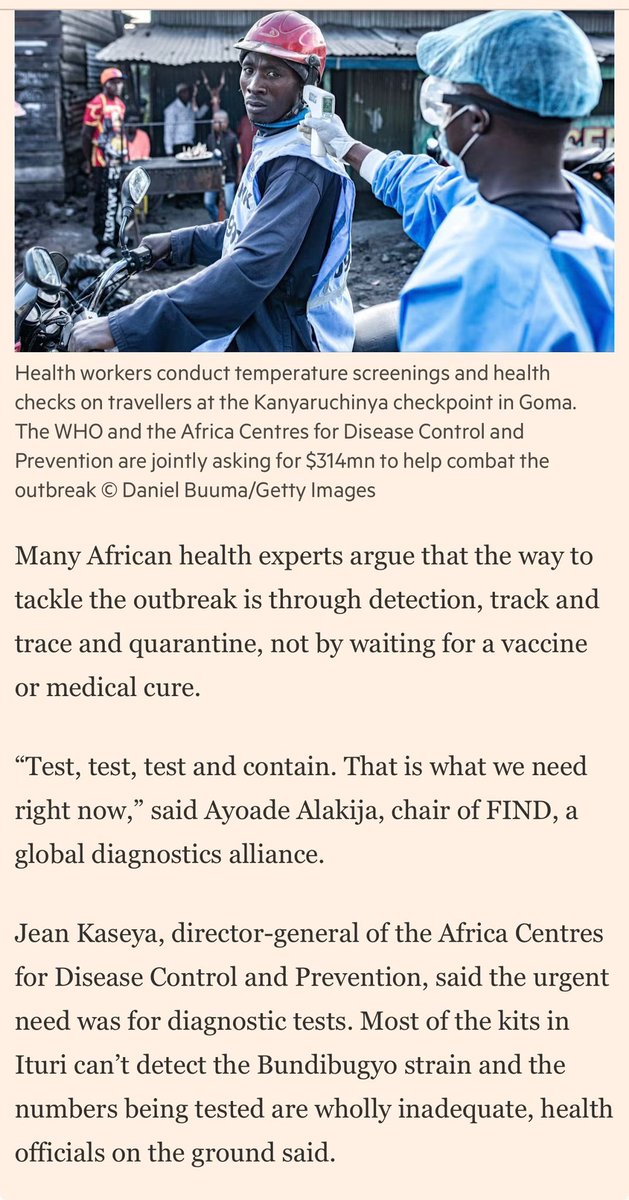
Tests, for diagnosis/for surveillance, are critical tools needed to contain an outbreak. Waiting for drugs/vaccines alone, allows viruses to spread.
Significant funds & coordination have started for vaccine/drugs. Equal effort is needed for test development, production, & distribution.

"Test, test, test and contain. That is what we need right now." My quote in today's @FT on the #Ebola outbreak in DRC, where most kits in Ituri can't even detect the Bundibugyo strain. @FINDdx is deploying. The window to act is closing.
3
19
37
3,278
Rick Bright retweeted

Important clarification on #Ebola terminology:
“Bundibugyo” is not a strain of Ebola virus — it is a separate species within the Ebolavirus genus, distinct from Zaire ebolavirus and Sudan ebolavirus.
A species refers to a major genetic grouping with important differences in virology, epidemiology, and potentially vaccine/therapeutic effectiveness.
A strain is a smaller genetic variation within a species.
17
84
240
17,014
Rick Bright retweeted

May 26
Stopping Ebola transmission requires swift, coordinated public health action.
In my interview with Al Jazeera English, I spoke about the collective mobilisation underway across Africa to contain the outbreak and protect affected communities.
We must get this virus under control. There is no alternative. Strengthening response capacity now is critical to saving lives and protecting communities.
---
Pour mettre fin à la transmission du virus Ebola, il faut une action rapide et coordonnée en matière de santé publique.
Lors de l'interview que j'ai accordée à @AJEnglish, j'ai parlé de la mobilisation collective en cours à travers l'Afrique pour endiguer l'épidémie et protéger les communautés touchées.
Nous devons maîtriser ce virus. Il n'y a pas d'autre solution. Il est essentiel de renforcer dès maintenant nos capacités d'intervention pour sauver des vies et protéger les populations.
🎥 Watch the full interview | Regardez l’interview: youtu.be/uhbjXJbasT4
#AfricaResponds #HealthSecurity
11
15
45
5,597

Rick Bright retweeted

Many have wanted the data - and the final publication for the Nitazoxanide for Norovirus in Transplants Study is out!
Time to stop using nitazoxanide for norovirus - zero impact on virology, no impact on clinical outcomes and clear financial toxicity.
pubmed.ncbi.nlm.nih.gov/4217…
2
11
40
2,330
Rick Bright retweeted

🦠Dr. Scott Gottlieb on Ebola outbreak: This is an outbreak that's out of control in West Africa cnbc.com/video/2026/05/26/dr…
1
21
56
1,942

Rick Bright retweeted
Diagnostics are critical to controlling an #Ebola outbreak. Without rapid testing, you can’t isolate cases, trace contacts, or protect healthcare workers.
But major challenges remain:
• Unreliable electricity and power supply
• Limited lab capacity and trained personnel
• Insecurity making sample transport and access difficult
Diagnostics require much more than just tests, they need infrastructure, logistics, and sustained investment.
3
22
82
5,184
May 25
Ebola risk does not follow borders. It follows broken trust, delayed diagnostics, fragile health systems, and gaps in preparedness.
The 2026 Bundibugyo outbreak is a warning: biological threats are moving faster than our institutions.
@Forbes @wbbsec:
forbes.com/sites/stephenbroz…
15
103
253
6,510
Rick Bright retweeted

Less convening. More delivery.
That’s the shift the next WHO Director-General will need to drive. New clip from my podcast with @jocalynclark (BMJ).
2
1
5
1,811
Rick Bright retweeted
It doesn't look like it took long to get the first 13 samples from the Bunia lab to Kinshasa. And WHO acted extremely quickly once those were confirmed.
Why was there such a delay in hearing about the deaths pre-May 5th? Coinfections confusing results? Fighting disruptions? ?

5
15
57
2,239
Rick Bright retweeted

May 18
Ebola : cinq choses à savoir ce lundi 18 mai
C'est un virus sorti de la forêt, jamais vu chez l'homme
Le séquençage complet du génome, confirmé simultanément par l'INRB à Kinshasa et le laboratoire de Kampala, établit que la variante Bundibugyo qui circule en Ituri ne dérive ni de l'épidémie ougandaise de 2007 ni de celle d'Isiro en 2012. C'est un spillover direct, un passage de l'animal à l'homme depuis un réservoir forestier encore non identifié. Muyembe le dit clairement : l'infirmier de Rwampara, mort le 24 avril, n'est probablement pas le cas index. Quelqu'un d'autre a contracté le virus en forêt avant lui.
Le test de terrain n'est pas conçu pour détecter ce virus
Le GeneXpert, outil de diagnostic rapide très utilisé en RDC, est spécifique à la souche Zaïre. Face à Bundibugyo, il a donné un résultat négatif sur tous les échantillons testés, y compris ceux confirmés positifs par d'autres méthodes. C'est une limite technique du test, pas une erreur humaine. Elle a contribué au retard de détection, avec d'autres facteurs : des échantillons arrivés à Kinshasa en petite quantité et sans respect de la chaîne de froid, un premier test négatif à Bunia, et des équipes de terrain formées à chercher Zaïre en priorité. Bundibugyo ne circule que pour la troisième fois dans l'histoire. Il est rare. Et les outils disponibles ne sont pas tous calibrés pour le reconnaître.
L'épidémie s'étend : 6 zones touchées
En une seule journée, la cartographie de l'épidémie a changé. Butembo-Katwa au Nord-Kivu, Nyankunde en Ituri et Goma s'ajoutent aux zones déjà touchées. Six zones sont désormais officiellement affectées. Parmi les nouveaux cas confirmés figure un médecin américain, prélevé à Bunia. Le bilan des morts suspects est passé de 80 vendredi à 118 ce lundi selon le porte-parole du gouvernement Patrick Muyaya.
Ni vaccin, ni traitement. Et les outils contre Zaïre ne servent probablement pas
Bundibugyo ne dispose d'aucun vaccin ni traitement spécifique approuvé. Muyembe est explicite : être vacciné contre Ebola Zaïre ne protège probablement pas contre cette variante. Pas de preuve de protection croisée. Le traitement est palliatif. Le molnupiravir est évoqué comme piste possible, sous réserve d'autorisation de l'OMS. Des candidats vaccins et des molécules pourraient être proposés pour des essais cliniques d'ici fin mai ou début juin selon Muyembe.
La réponse internationale se durcit, mais les moyens manquent sur le terrain
L'OMS a déclaré une urgence de santé publique de portée internationale le 17 mai. L'UA, l'EAC, Africa CDC, la Banque mondiale sont mobilisés. Les États-Unis ont suspendu toutes leurs opérations de visas à Kampala. Mais à Mongwalu, un médecin de MSF dit qu'il manque de tout : médicaments, équipements de protection, épidémiologistes. Oxfam va plus loin : les coupes dans l'aide humanitaire ont affaibli les systèmes de surveillance et retardé la détection de l'épidémie de plusieurs semaines. C'est la tension centrale de cette crise. La mobilisation est réelle. Les moyens sur le terrain ne suivent pas encore.
PL
18
207
398
79,248
Rick Bright retweeted

May 19
‼️🦠🚨👉🏻Lo que complica este brote de Ébola y por qué preocupa de forma especial (post largo pero espero aclarar muchas dudas sobre su complejidad )
1) Ocurre en la zona Ituri en RDC que está en conflicto, difícil de accesar y con pocos recursos y además de mucha movilidad, con millones de personas desplazadas y mucho comercio (por las minas de oro/coltan…)
2) Se supo del contagio muy tarde, los primeros casos son de hace un mes, entre ellos trabajadores de la salud; se espera encontrar muchos casos diseminados (hoy se sospechan de 513 probables y más de 130 fallecidos, incrementando las cifras rápidamente)
3) Ya está el virus en al menos 8 zonas de salud afectadas y no solo en regiones rurales sino también ciudades como Goma en RDC y Kempala en Uganda.
4) Las pruebas de diagnóstico inicialmente salían falsamente negativas porque son las convencionales y detectan Ébola de especie Zaire; los centros donde se puede secuenciar el virus están a 2 horas en avión.
5) Para el virus Ébola de Bundibugyo no hay vacuna aprobada ni tratamiento específico…Se tendrá que depender de las medidas de salud pública como rastreo de contactos, aislamiento, equipo de protección personal, entierros seguros, etc.
5) Los recortes a programas como USAID limitan los recursos disponibles; ya las zonas afectadas reportan carencias importantes en material de protección personal y material de soporte (sueros,etc) para contener el brote y ayudar a las personas.
6) La zona afectada, Provincia de Ituri, es frontera con Uganda y Sudán del Sur; ya hay al menos dos casos confirmados en Uganda, y un fallecido, no relacionados entre sí. Ya ha traspasado fronteras.
7) El Mundial moviliza a miles de personas y aunque la mayoría de los jugadores de la RDC juegan en equipos europeos sería ideal se concentren fuera de su país y los aficionados, que seguramente querrán ir a los juegos de Houston, Guadalajara y Atlanta, ya no podrán entrar a Estados Unidos que ha cerrado sus fronteras a personas que en los últimos 21 días han estado en Uganda, RDC o Sudán del Sur.
✅Lo positivo:
1) Ya al declararse Emergencia Internacional (PHEIC) por la OMS se liberan mecanismos de apoyo con recursos materiales, financieros y humanos fundamentales para contener esta epidemia. Se hará con medidas de aislamiento, rastreo de contactos, material de protección y soporte médico,…comunicación y apoyo comunitario.
2) Se está pensando probar la vacuna contra Ébola de Zaire para ver si tendría algún efecto de protección cruzada
3) Este es el brote No. 17 de Ébola en RDC; tienen cierta experiencia de como actuar.
⚠️Importante para saber:
1) Ahora para la población fuera de esta zona el riesgo es BAJO, hay que estar atentos, pero no alarmados.
2) Países como Mexico debieran estar preparados para poder diagnosticar, aislar, tratar y hacer trabajo epidemiológico de una enfermedad que nunca hemos tenido que manejar. Se emitió aviso de precaución para viajeros.
3) La delegación de fútbol de RDC debiera concentrarse al menos 21 días fuera de Africa antes de su primer partido. Y tomar medidas epidemiologicas estrictas para los aficionados que buscarán viajar.
🙏🏻Para reflexionar:
Este virus, genéticamente no tiene que ver con los virus de Ébola de Bundibugyo que causaron los brotes de 2007 y 2012 evidenciando que aunque es la misma especie, este evento es resultado de una zoonosis nueva, un evento de spillover de la selva! Recordándonos lecciones importantes sobre no invadir ecosistemas y tener precaución al interaccionar con fauna silvestre 🙏🏻🙌🏻


May 18

Ebola : cinq choses à savoir ce lundi 18 mai
C'est un virus sorti de la forêt, jamais vu chez l'homme
Le séquençage complet du génome, confirmé simultanément par l'INRB à Kinshasa et le laboratoire de Kampala, établit que la variante Bundibugyo qui circule en Ituri ne dérive ni de l'épidémie ougandaise de 2007 ni de celle d'Isiro en 2012. C'est un spillover direct, un passage de l'animal à l'homme depuis un réservoir forestier encore non identifié. Muyembe le dit clairement : l'infirmier de Rwampara, mort le 24 avril, n'est probablement pas le cas index. Quelqu'un d'autre a contracté le virus en forêt avant lui.
Le test de terrain n'est pas conçu pour détecter ce virus
Le GeneXpert, outil de diagnostic rapide très utilisé en RDC, est spécifique à la souche Zaïre. Face à Bundibugyo, il a donné un résultat négatif sur tous les échantillons testés, y compris ceux confirmés positifs par d'autres méthodes. C'est une limite technique du test, pas une erreur humaine. Elle a contribué au retard de détection, avec d'autres facteurs : des échantillons arrivés à Kinshasa en petite quantité et sans respect de la chaîne de froid, un premier test négatif à Bunia, et des équipes de terrain formées à chercher Zaïre en priorité. Bundibugyo ne circule que pour la troisième fois dans l'histoire. Il est rare. Et les outils disponibles ne sont pas tous calibrés pour le reconnaître.
L'épidémie s'étend : 6 zones touchées
En une seule journée, la cartographie de l'épidémie a changé. Butembo-Katwa au Nord-Kivu, Nyankunde en Ituri et Goma s'ajoutent aux zones déjà touchées. Six zones sont désormais officiellement affectées. Parmi les nouveaux cas confirmés figure un médecin américain, prélevé à Bunia. Le bilan des morts suspects est passé de 80 vendredi à 118 ce lundi selon le porte-parole du gouvernement Patrick Muyaya.
Ni vaccin, ni traitement. Et les outils contre Zaïre ne servent probablement pas
Bundibugyo ne dispose d'aucun vaccin ni traitement spécifique approuvé. Muyembe est explicite : être vacciné contre Ebola Zaïre ne protège probablement pas contre cette variante. Pas de preuve de protection croisée. Le traitement est palliatif. Le molnupiravir est évoqué comme piste possible, sous réserve d'autorisation de l'OMS. Des candidats vaccins et des molécules pourraient être proposés pour des essais cliniques d'ici fin mai ou début juin selon Muyembe.
La réponse internationale se durcit, mais les moyens manquent sur le terrain
L'OMS a déclaré une urgence de santé publique de portée internationale le 17 mai. L'UA, l'EAC, Africa CDC, la Banque mondiale sont mobilisés. Les États-Unis ont suspendu toutes leurs opérations de visas à Kampala. Mais à Mongwalu, un médecin de MSF dit qu'il manque de tout : médicaments, équipements de protection, épidémiologistes. Oxfam va plus loin : les coupes dans l'aide humanitaire ont affaibli les systèmes de surveillance et retardé la détection de l'épidémie de plusieurs semaines. C'est la tension centrale de cette crise. La mobilisation est réelle. Les moyens sur le terrain ne suivent pas encore.
PL
12
181
389
37,695