
Joined November 2021
- Tweets 24,600
- Following 615
- Followers 979
- Likes 17,182
6,025 Photos and videos











Pinned Tweet

Mar 3
If your Congressional Representatives aren't voting for this they need to be fired immediately.

Please keep our team in your prayers for strength and wisdom today as we embark on an important mission. We will be testifying in front of the Senate on behalf of child exploitation victims and survivors. Tim Tebow Foundation
Be a Voice for the Voiceless: timtebowfoundation.quorum.us…
6
815
Jun 5
Your politicians don't care...
They want to cheat...
This was the way to stop it and an OVERWHELMING amount of Americans wanted it and instead 🙃

21
Jun 5
This right here!!!
Way to go Josh!!!
Jun 5

The Senate just PASSED my legislation with Tim Tebow to RESCUE thousands of children trapped in sex trafficking.
19
Jun 2
When @burtjonesforga supported Senate Bills 68 and 69, also referred to as "Tort Reform" it was actually a ploy to allow the exact behavior 🙄 explained in this video. When the consequences that punitive damages were created for are removed it allows health insurers like Kaiser Permanente to act without consequences... but thats ok if your taking money from them... 😒 🤔 😒
#InsuranceMoney
#HigherRates
#LessProtection
Jun 1

Ford calculated it was cheaper to let people burn alive in the Pinto than to fix the exploding gas tank.
Fix the defect? $137 million.
Pay out for deaths and injuries? Only $49 million.
So they left it that way.
Aaron Siri brought this up on JRE, pointing to similar cases like Vioxx, where the company knew it was causing heart attacks and strokes but downplayed the risks to protect profits.
When corporations are allowed to run cold cost-benefit analyses on human lives, people die so shareholders can earn more. Punitive damages exist precisely to make that math no longer add up.
This isn’t ancient history. It still happens whenever profit is placed above safety.
1
460
Jun 2
And more
x.com/Shock_Wave/status/2043…
Apr 11

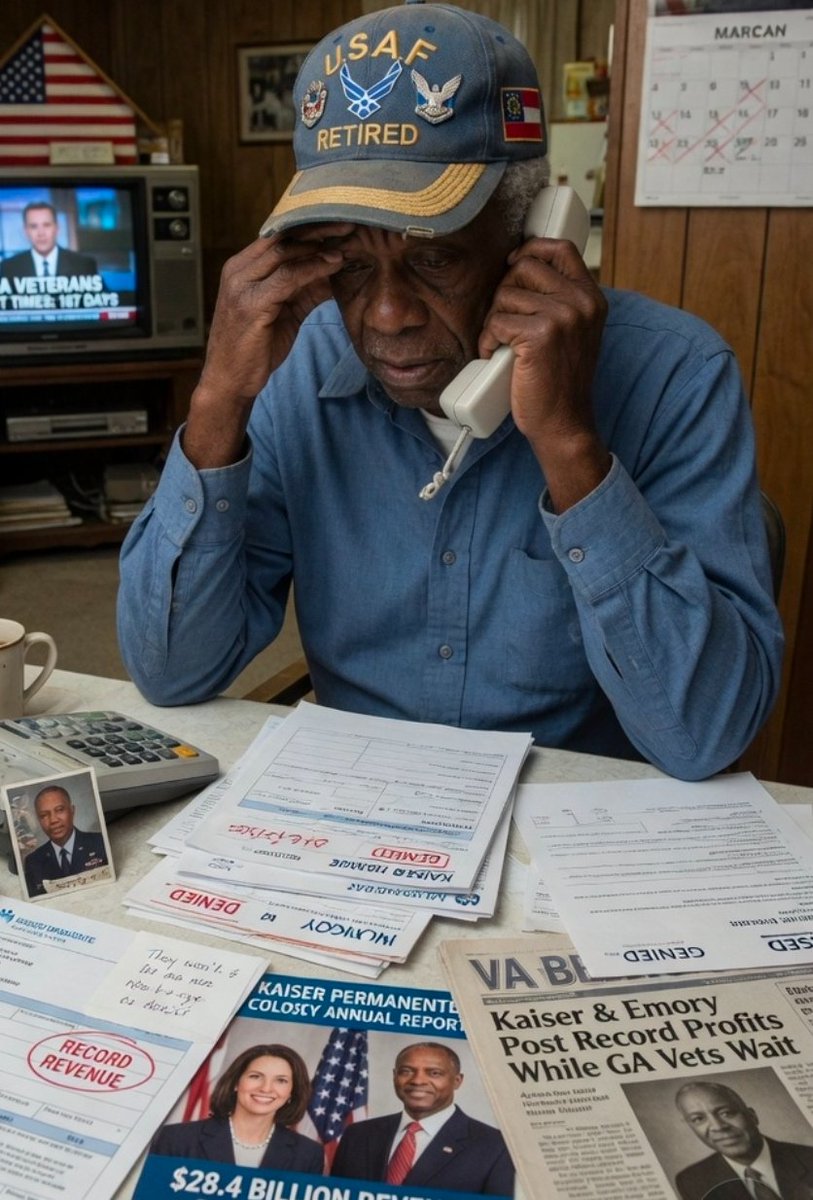
They fought for the #USA 🇺🇸
and now no one's fighting for them....
@SecWar where is OPM... where is congress...
Hey 👋 @RepThomasMassie @SenatorWarnock and @RandPaul and @GOPHELP you won't review this...
@11Alive and @FoxNews you won't report...
@GovKemp your Insurance Commissioner won't look into this..
@DOGE_OPM might look into this..
Kaiser's "Non-Profit" Net income 2025
Net income : $9.3 billion
Kaiser Permanente participates in the Federal Employees Health Benefits (FEHB) program as a regional HMO option available in defined service areas across multiple states and regions, including Northern California, Southern California, Colorado, Georgia, Hawaii, the Mid-Atlantic States (District of Columbia, Maryland, Virginia), and the Northwest (Oregon and Washington).
Federal employees, annuitants (retirees), and their families can enroll during Open Season or qualifying life events if they live or work in one of these service areas.
However, in many of these zones, the local infrastructure consists of limited or no Kaiser-owned medical offices, full-service clinics, on-site labs, or pharmacies. Care instead relies heavily on contracted or affiliated private providers and hospitals.
This Structure Creates Widespread Chaos for FEHB Patients Nationwide
Expectation vs. Reality Mismatch:
Enrollees choose Kaiser FEHB for its HMO reputation of seamless, predictable, low-friction care. However in zip codes where service was written under FEHB such as peripheral zones, they face fragmented coordination between contracted local providers and distant Kaiser facilities, duplicated testing, longer wait times, and logistical burdens (e.g., travel to core areas for specialty care). Much of which violates state and Federal Laws that your Senators don't seem to care about....
Strict HMO Rules Without Full Integrated Benefits:
Referrals, prior authorizations, and network-only restrictions still apply fully, but without the usual payoff of easy same-day appointments or shared electronic records across all providers. This leads to more delays, denials, or appeals—even for “covered” services. Kaiser can't even get lab work done for those with serious medical needs...
Administrative and Financial Burdens: Members often deal with denied claim filing for certain services, inconsistent network verification hassles, and higher practical out-of-pocket exposure when local options don’t align perfectly. Chronic conditions, maternity, cancer care, or family needs amplify the disruption for our veterans
Impact on Federal Employees and Veterans: Many FEHB enrollees are veterans (or family members of veterans) who rely on these plans as primary or supplemental coverage. State Governments say its an OPM problem and OPM won't investigate...
Maybe its because the money is going to those to not investigate 🤔 😕
@aboutKP through Lobbyist
Kamala Harris (D-PRES): $1,777,418
DNC Services Corp: $382,587
Donald Trump (R-PRES): $201,426
Democratic Congressional Campaign Cmte: $199,782
Democratic Senatorial Campaign Cmte: $181,900
Jon Tester (D-Sen, MT): $74,637
Adam Schiff (D-House, CA): $64,106
Ruben Gallego (D-House, AZ): $56,968
@EmoryUniversity through Lobbyist
Kamala Harris (D-PRES): $362,974
American Bridge 21st Century (Carey/outside): $275,219
DNC Services Corp: $224,828
Democratic Senatorial Campaign Cmte: $207,684
Georgia Federal Elections Cmte: $139,573
Democratic Congressional Campaign Cmte: $113,165
Why this matters...
5 U.S.C. Chapter 89 (Federal Employees Health Benefits Act / FEHBA): The core statute (Pub. L. 86-382, as amended) authorizing FEHB contracts. Requires carriers to provide the contracted health benefits, including through HMOs that must maintain adequate networks throughout the approved service area. Breaches occur if the HMO cannot deliver “adequate choice of quality primary and specialty medical care” or “reasonable access to network providers” as required for contract approval and continuation.
5 U.S.C. § 8902 (Contracting Authority) and § 8903 (Health Benefits Plans): Authorize OPM to contract only with plans that can actually deliver the promised benefits. HMOs must demonstrate the ability to provide services in the entire defined service area; failure to do so violates the statutory contracting standards and the FEHB contract itself.
Mental Health Parity and Addiction Equity Act of 2008 (MHPAEA), as applied to FEHB (codified at 42 U.S.C. § 300gg-26 and enforced via 5 U.S.C. § 8902(p)): Requires parity in access, including network adequacy for mental health/substance use disorder services compared to medical/surgical benefits. Network composition standards, provider reimbursement, and access metrics are treated as Non-Quantitative Treatment Limitations (NQTLs). Material differences in access (e.g., inadequate MH/SUD providers in parts of the service area) violate parity rules; OPM requires comparative analyses and data on wait times, utilization, and network metrics.
Kaiser can't find Localized care for our #veterans but here are its top salaries.. and @BernieSanders and @SenWarren won't say a word....
Ohh Kaiser is a Non-profit too...
Gregory Adams (Chairman & CEO): $12,976,050
Kimberly Horn (EVP, Group President, MOC): $6,474,308
Janet Liang (Regional President,
Northern CA / EVP, Group President & COO): $5,011,705
Kathryn Lancaster (EVP & CFO): $5,004,087
Brandon Cuevas (EVP, Health Plan): $4,354,878
Yazdi Bagli (EVP, Enterprise Business Services): $3,822,029
Carrie Plietz (Regional President, NCAL): $3,326,860
Chuck Bevilacqua (SVP, Health Plan Service and Admin): $3,007,814
Gregory Holmes (SVP, Chief HR Officer): $2,671,910
Paul Swenson (EVP, Chief Admin Officer): $2,648,633
Brand Name 100% Denials
100% denied: Contrave, Emgality Pen, Everolimus, Farxiga, Mounjaro, Myrbetriq, Rhofade, Stelara, Vraylar, Wegovy, Xifaxan
Operating revenue: $127.7 billion
Operating expenses: $126.3 billion
Operating income: $1.4 billion (1.1% operating margin)
Net income (bottom line, including investment gains): $9.3 billion

1
28
Jun 2
Direct Impact to #Veterans
x.com/Shock_Wave/status/2049…
Apr 29
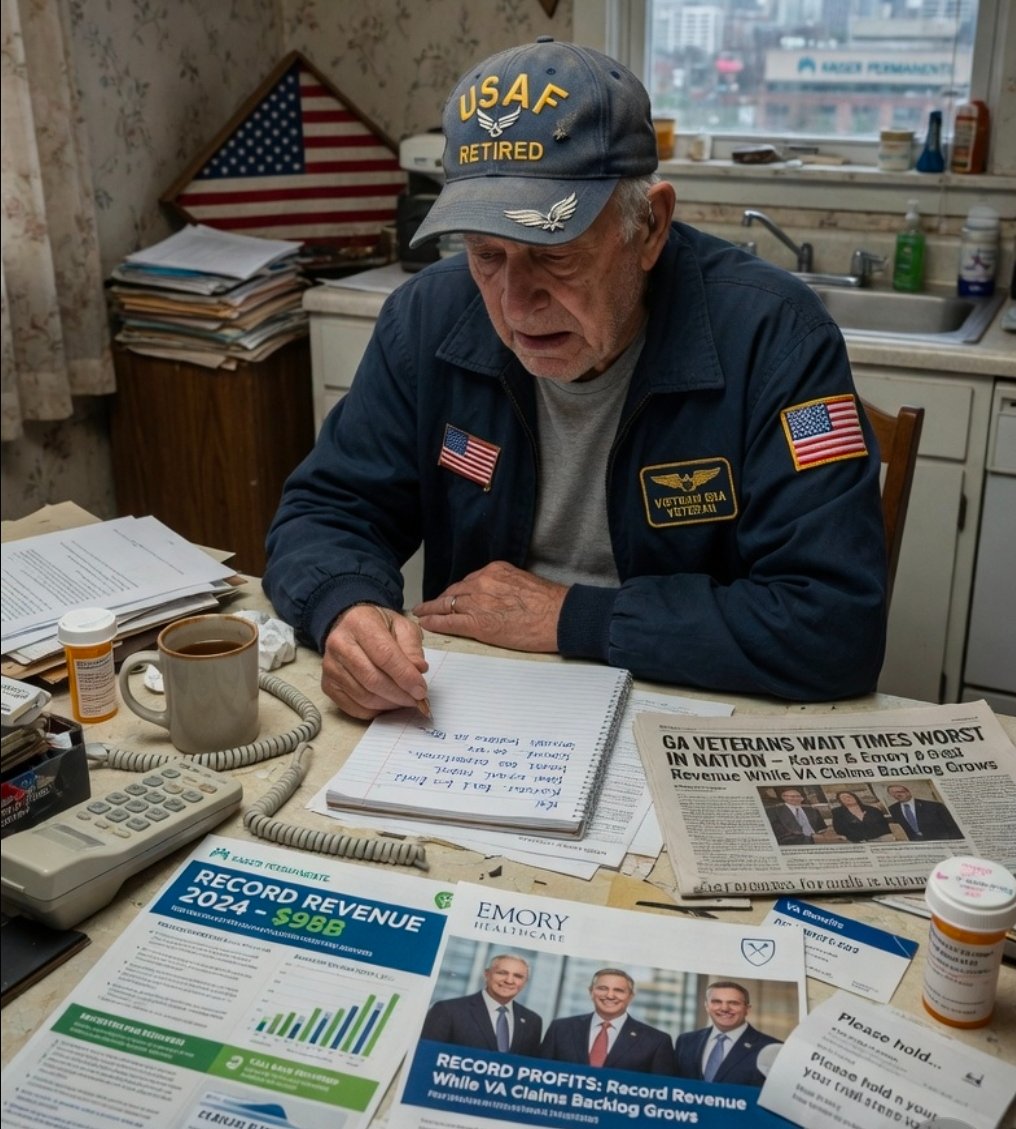
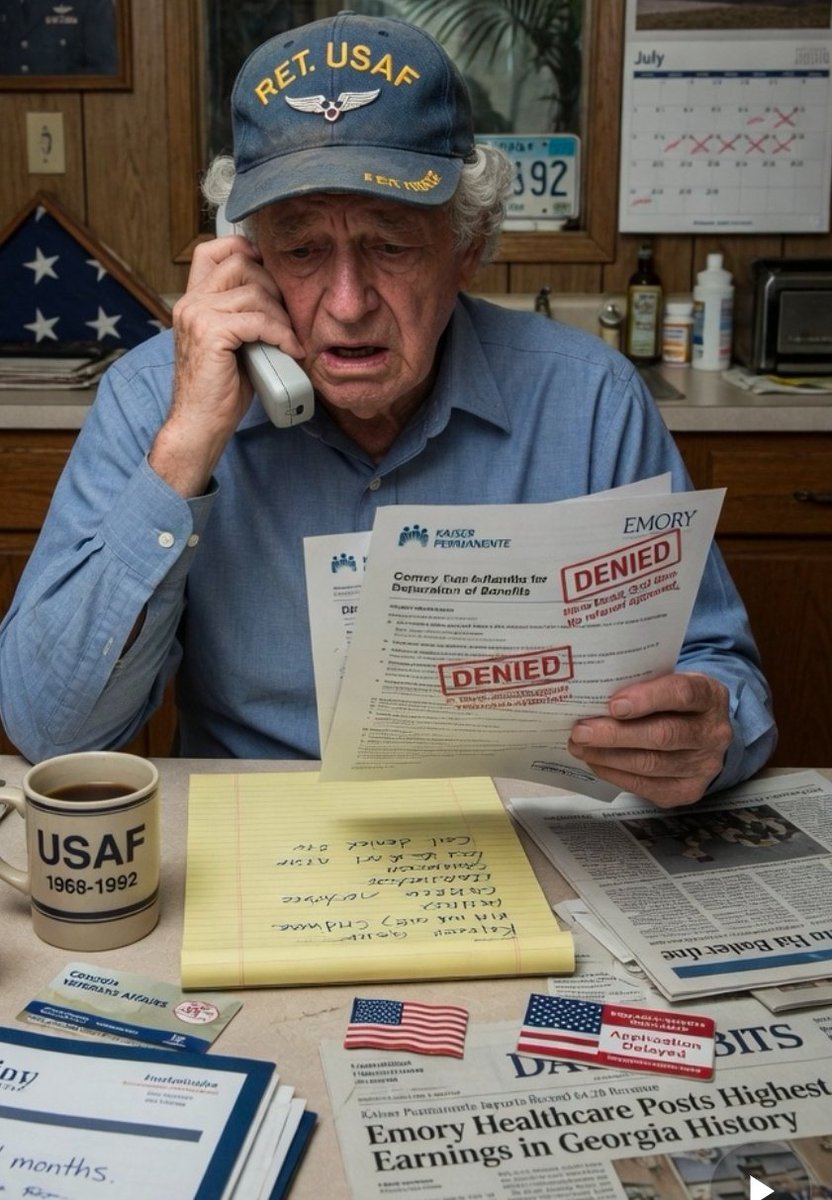
Direct Account from Source:
Today, April 29, 2026, at a @emoryhealthcare office in Georgia, an elderly man wearing a proud U.S. Air Force Retired hat walked up to the window. He was tired and confused after days of trying to reschedule an appointment. The assistant told him:
“Sir, there is nothing we can do. It’s all routed to the call center.”
This man fought for our country. He served in the Air Force to protect the freedoms we all enjoy. And in his later years, when he simply needed help, he was dismissed like he didn’t matter.
It broke our hearts.
This is the same Kaiser that has performed gender-altering surgeries and care on minors with gender dysphoria in its facilities (including patients touching Georgia), only pausing under outside pressure — while everyday veterans and seniors are told “nothing we can do.”
Our leaders — @burtjonesforga Lieutenant Governor Burt Jones and Speaker Jon Burns — have done nothing, Zero responses. Zero oversight. Zero protection for the very people who served this state and nation. @GASenatePress and @GaHouseHub on Insurance Committees are too busy trying to win votes with Ads instead of Actions
Georgia doesn’t need more excuses.
Georgia doesn't need more direct mailers.
Georgia needs real leadership.
The current leaders are failing us.
Georgia voters deserve to know who actually stands with veterans and patients — and who protects the insurance companies instead...
Spread the word and let's get real change in #Healthcare
Many Georgians are watching.
Many more will speak up.
#Georgia #KaiserFail #VeteransDeserveBetter #HoldThemAccountable #LeadershipMatters
ALT Veterans Deserve Better
24
May 26
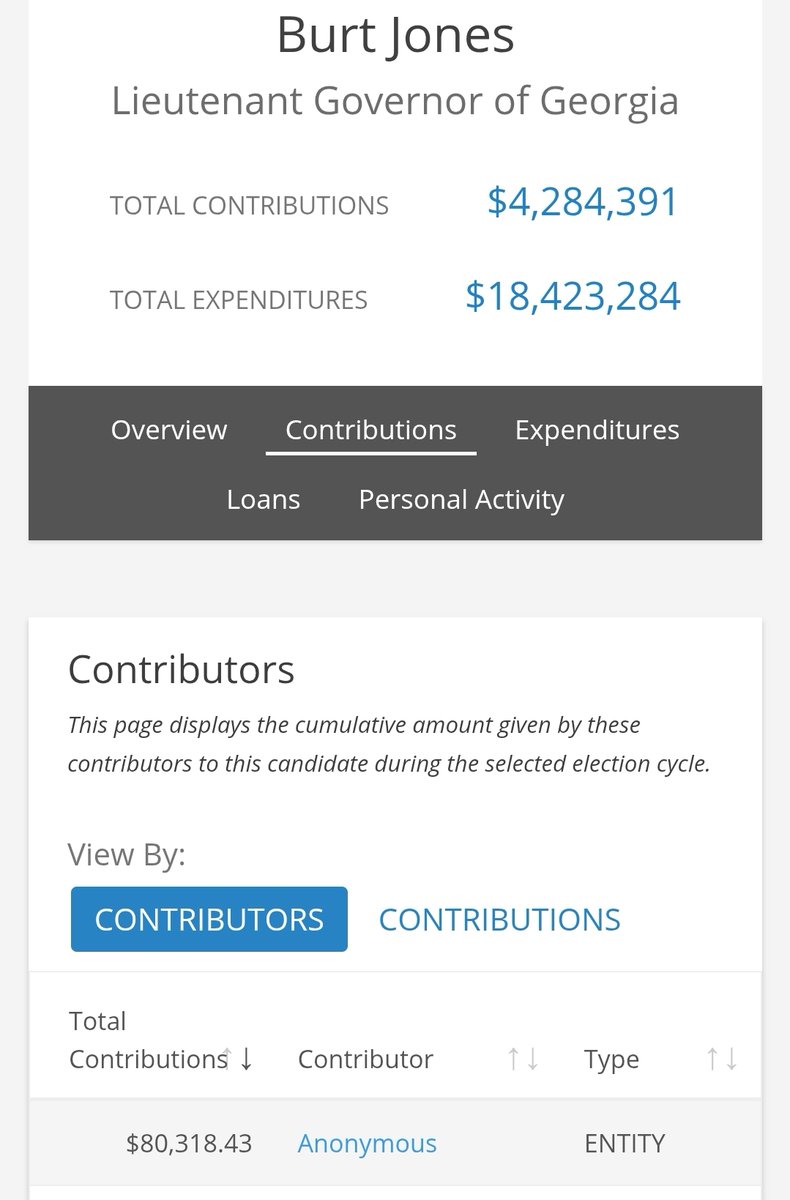
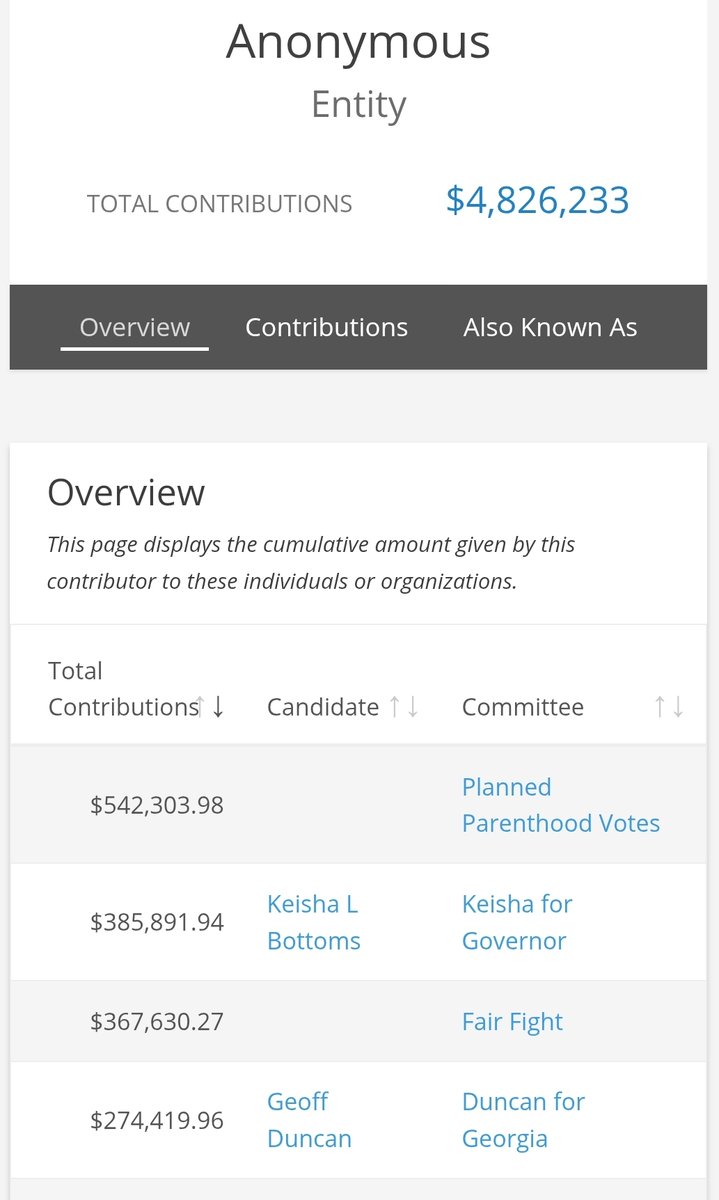
Hey 👋 @burtjonesforga who is this
"Anonymous" entity giving money to @burtjonesforga , Planned Parenthood, and Keisha Bottoms?
How as LT Governor is your oversight allowing an Anonymous entity?
3
1
2
4,807
May 21
Wake ⏰️ UP GA 🚨
Burt Jones @burtjonesforga AKA @LtGovJonesGA took money from a company that operated along with others on 3,678 kids.
Full stop ✋️ Kids 😟😥 gender surgery... yeah that kind...
That company ( Kaiser Permanente ) is currently being sued for looking the other way concerning child abuse
pcva.law/news/first-michael-…
Then when other issues in Georgia about that company were reported he refused to investigate them or provide oversight in 2026 along with @JonBurnsGA and the entire Senate and Representatives Insurance committees. We have receipts from sources that contacted them multiple times.
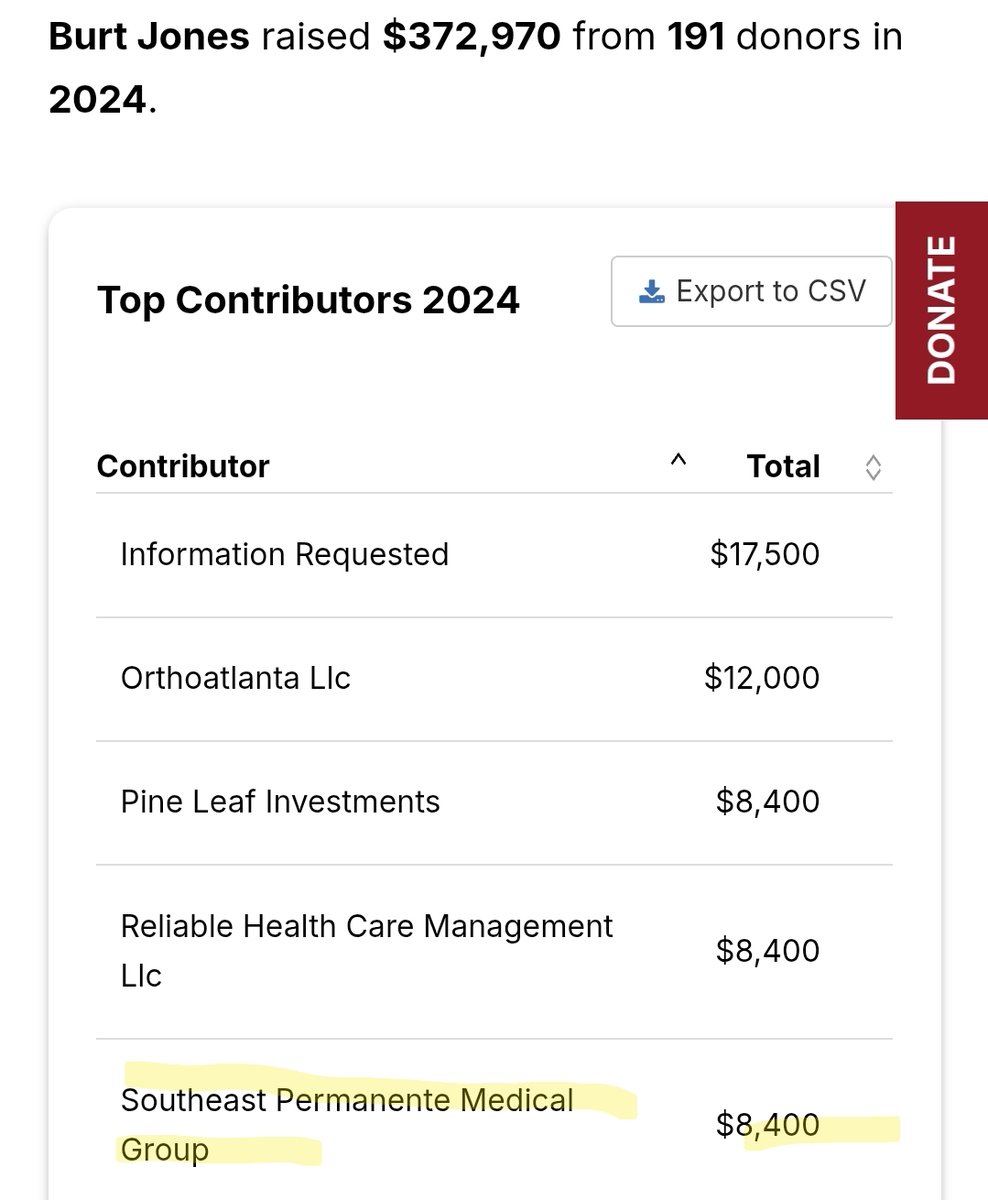
He was too busy flying around on his private jet for his campaign... to date he has spent roughly 74K on private jets, that figure also represents direct payments from the campaign/leadership committee to a company tied to Burt Jones’ family.
Jones Petroleum Transport Co. – $73,506.62
"The Southeast Permanente Medical Group, Inc. (TSPMG) is the physician-led, multi-specialty medical group that exclusively serves Kaiser Permanente members in Georgia (and the broader Southeast region)."
Kaiser Settlements in GA:
$46 million (privacy/data tracking, 2026, includes Georgia members)
$556 million (Medicare fraud, 2026, national/system-wide)
$130,000 (ADA disability discrimination, 2021, Georgia-specific)
Confidential amount (medical malpractice/wrongful death, 2019, Georgia case)
Nationwide Gender Surgery Numbers (2016–2020, JAMA study – 48,019 total patients):
2016: 4,552
2017: 7,397
2018: 10,242
2019: 13,011
2020: 12,818
By procedure type:
Breast/chest: 27,187 (56.6%)
Genital reconstruction: 16,872 (35.1%)
Facial/cosmetic: 6,669 (13.9%)
By age:
Ages 12–18 (minors): 3,678 (7.7%; ~405 genital)
#Receipts #SaveTheChildren
opensecrets.org/officeholder…
Over 200 done at ONE FACILITY
gender-affirming mastectomies (top surgery) performed on adolescents (ages 12–17 at the time of referral) at Kaiser Permanente Northern California from January 2013 to July 2020.
ALT Campaign Contributions from a company that performed Gender-altering surgery on Minors
4
5
8
8,629
May 18
That's an unprecedented level of corruption 😳

2
134
May 17
This is very interesting 🤔
x.com/georgiatruths/status/2…
May 17

Burt is a corrupt compromised swamp creature who has perfected lying.. here’s a few examples… (open secrets)



3
112
May 11
Hey 👋
@LtGovJonesGA and @JonBurnsGA and @SenatorWarnock care to explain? We have direct source information you were asked to investigate Kaiser Permanente in GA on Multiple occasions and didn't respond...
Neither did the GA insurance Committee or GA Insurance Commissioner 🤔 😕 😐
May 11

A lawsuit was filed against Kaiser Permanente in Clark County, alleging the healthcare company failed to protect patients against a doctor with decades of child sexual abuse accusations. fox13seattle.com/news/kaiser…
7
3
13
18,291
May 11
Additional information
x.com/Shock_Wave/status/2043…
Apr 11
They fought for the #USA 🇺🇸
and now no one's fighting for them....
@SecWar where is OPM... where is congress...
Hey 👋 @RepThomasMassie @SenatorWarnock and @RandPaul and @GOPHELP you won't review this...
@11Alive and @FoxNews you won't report...
@GovKemp your Insurance Commissioner won't look into this..
@DOGE_OPM might look into this..
Kaiser's "Non-Profit" Net income 2025
Net income : $9.3 billion
Kaiser Permanente participates in the Federal Employees Health Benefits (FEHB) program as a regional HMO option available in defined service areas across multiple states and regions, including Northern California, Southern California, Colorado, Georgia, Hawaii, the Mid-Atlantic States (District of Columbia, Maryland, Virginia), and the Northwest (Oregon and Washington).
Federal employees, annuitants (retirees), and their families can enroll during Open Season or qualifying life events if they live or work in one of these service areas.
However, in many of these zones, the local infrastructure consists of limited or no Kaiser-owned medical offices, full-service clinics, on-site labs, or pharmacies. Care instead relies heavily on contracted or affiliated private providers and hospitals.
This Structure Creates Widespread Chaos for FEHB Patients Nationwide
Expectation vs. Reality Mismatch:
Enrollees choose Kaiser FEHB for its HMO reputation of seamless, predictable, low-friction care. However in zip codes where service was written under FEHB such as peripheral zones, they face fragmented coordination between contracted local providers and distant Kaiser facilities, duplicated testing, longer wait times, and logistical burdens (e.g., travel to core areas for specialty care). Much of which violates state and Federal Laws that your Senators don't seem to care about....
Strict HMO Rules Without Full Integrated Benefits:
Referrals, prior authorizations, and network-only restrictions still apply fully, but without the usual payoff of easy same-day appointments or shared electronic records across all providers. This leads to more delays, denials, or appeals—even for “covered” services. Kaiser can't even get lab work done for those with serious medical needs...
Administrative and Financial Burdens: Members often deal with denied claim filing for certain services, inconsistent network verification hassles, and higher practical out-of-pocket exposure when local options don’t align perfectly. Chronic conditions, maternity, cancer care, or family needs amplify the disruption for our veterans
Impact on Federal Employees and Veterans: Many FEHB enrollees are veterans (or family members of veterans) who rely on these plans as primary or supplemental coverage. State Governments say its an OPM problem and OPM won't investigate...
Maybe its because the money is going to those to not investigate 🤔 😕
@aboutKP through Lobbyist
Kamala Harris (D-PRES): $1,777,418
DNC Services Corp: $382,587
Donald Trump (R-PRES): $201,426
Democratic Congressional Campaign Cmte: $199,782
Democratic Senatorial Campaign Cmte: $181,900
Jon Tester (D-Sen, MT): $74,637
Adam Schiff (D-House, CA): $64,106
Ruben Gallego (D-House, AZ): $56,968
@EmoryUniversity through Lobbyist
Kamala Harris (D-PRES): $362,974
American Bridge 21st Century (Carey/outside): $275,219
DNC Services Corp: $224,828
Democratic Senatorial Campaign Cmte: $207,684
Georgia Federal Elections Cmte: $139,573
Democratic Congressional Campaign Cmte: $113,165
Why this matters...
5 U.S.C. Chapter 89 (Federal Employees Health Benefits Act / FEHBA): The core statute (Pub. L. 86-382, as amended) authorizing FEHB contracts. Requires carriers to provide the contracted health benefits, including through HMOs that must maintain adequate networks throughout the approved service area. Breaches occur if the HMO cannot deliver “adequate choice of quality primary and specialty medical care” or “reasonable access to network providers” as required for contract approval and continuation.
5 U.S.C. § 8902 (Contracting Authority) and § 8903 (Health Benefits Plans): Authorize OPM to contract only with plans that can actually deliver the promised benefits. HMOs must demonstrate the ability to provide services in the entire defined service area; failure to do so violates the statutory contracting standards and the FEHB contract itself.
Mental Health Parity and Addiction Equity Act of 2008 (MHPAEA), as applied to FEHB (codified at 42 U.S.C. § 300gg-26 and enforced via 5 U.S.C. § 8902(p)): Requires parity in access, including network adequacy for mental health/substance use disorder services compared to medical/surgical benefits. Network composition standards, provider reimbursement, and access metrics are treated as Non-Quantitative Treatment Limitations (NQTLs). Material differences in access (e.g., inadequate MH/SUD providers in parts of the service area) violate parity rules; OPM requires comparative analyses and data on wait times, utilization, and network metrics.
Kaiser can't find Localized care for our #veterans but here are its top salaries.. and @BernieSanders and @SenWarren won't say a word....
Ohh Kaiser is a Non-profit too...
Gregory Adams (Chairman & CEO): $12,976,050
Kimberly Horn (EVP, Group President, MOC): $6,474,308
Janet Liang (Regional President,
Northern CA / EVP, Group President & COO): $5,011,705
Kathryn Lancaster (EVP & CFO): $5,004,087
Brandon Cuevas (EVP, Health Plan): $4,354,878
Yazdi Bagli (EVP, Enterprise Business Services): $3,822,029
Carrie Plietz (Regional President, NCAL): $3,326,860
Chuck Bevilacqua (SVP, Health Plan Service and Admin): $3,007,814
Gregory Holmes (SVP, Chief HR Officer): $2,671,910
Paul Swenson (EVP, Chief Admin Officer): $2,648,633
Brand Name 100% Denials
100% denied: Contrave, Emgality Pen, Everolimus, Farxiga, Mounjaro, Myrbetriq, Rhofade, Stelara, Vraylar, Wegovy, Xifaxan
Operating revenue: $127.7 billion
Operating expenses: $126.3 billion
Operating income: $1.4 billion (1.1% operating margin)
Net income (bottom line, including investment gains): $9.3 billion
3
382
May 11
Additional info
x.com/Shock_Wave/status/2049…
Apr 29
Direct Account from Source:
Today, April 29, 2026, at a @emoryhealthcare office in Georgia, an elderly man wearing a proud U.S. Air Force Retired hat walked up to the window. He was tired and confused after days of trying to reschedule an appointment. The assistant told him:
“Sir, there is nothing we can do. It’s all routed to the call center.”
This man fought for our country. He served in the Air Force to protect the freedoms we all enjoy. And in his later years, when he simply needed help, he was dismissed like he didn’t matter.
It broke our hearts.
This is the same Kaiser that has performed gender-altering surgeries and care on minors with gender dysphoria in its facilities (including patients touching Georgia), only pausing under outside pressure — while everyday veterans and seniors are told “nothing we can do.”
Our leaders — @burtjonesforga Lieutenant Governor Burt Jones and Speaker Jon Burns — have done nothing, Zero responses. Zero oversight. Zero protection for the very people who served this state and nation. @GASenatePress and @GaHouseHub on Insurance Committees are too busy trying to win votes with Ads instead of Actions
Georgia doesn’t need more excuses.
Georgia doesn't need more direct mailers.
Georgia needs real leadership.
The current leaders are failing us.
Georgia voters deserve to know who actually stands with veterans and patients — and who protects the insurance companies instead...
Spread the word and let's get real change in #Healthcare
Many Georgians are watching.
Many more will speak up.
#Georgia #KaiserFail #VeteransDeserveBetter #HoldThemAccountable #LeadershipMatters
ALT Veterans Deserve Better
1
2
731
May 10
A data center drained 30M gallons of water unnoticed — until residents complained about low water pressure - POLITICO
politico.com/news/2026/05/08…
Where was @burtjonesforga ?
Where was @JonBurnsGA ?
Where was @SenatorWarnock ?
Where was @ossoff ?
Where was @GASenatePress ?
"Residents in Fayetteville, Georgia, noticed low water pressure last year"
This is what happens when your Leaders are sleeping 😴 ....
82
May 3
🚨 #GABoardOfPharmacy FAILS VETERANS STATEWIDE
The Georgia State Board of Pharmacy is an eight-member board appointed by the Governor to protect, promote and preserve the public health. If @LtGovJonesGA won't oversee now, who will be put in later?
On Apr 22, 2026, Exec Dir J. Clinton Joiner closed w/ “NO VIOLATION” & zero action a detailed complaint against @aboutKP Kaiser GA pharmacies—despite irrefutable documented evidence of ongoing violations. Board refused to reopen, produce investigative file, explain its “no violation” finding, or perform mandatory duties under O.C.G.A. §26-4-28(a)(5)(15)(16). This is nonfeasance & dereliction of duty.
Direct from source:
(complainant file Joiner’s Apr 22 denial letter):
Dec 26, 2025: Pharmacy technician (no tag, impersonated pharmacist) dispensed Schedule IV controlled substance ( PTSD/anxiety med) with no licensed pharmacist on-site or supervising—explicit violation of O.C.G.A. §26-4-88 & Board Rule 480-15-.03. Security called when patient asked about Quantity Limits (QL).
Feb 2024–Apr 2026 pattern: missed/delayed fills; repeated excuses no change
QL/formulary non-disclosure & false “system/calendar errors” despite 4 formal requests (violates 5 C.F.R. §890.105, OPM Carrier Letter 2024-02, GAC 480-31/480-15-.03, OCGA §26-4-88); chronic inventory shortages (Rule 480-6-.01); unilateral
Rx closure w/o notice; grievances answered with provably false statements & generic form letters (no corrective action) by Kaiser.
This is not isolated—widespread systemic pattern across GA hitting veterans/FEHB members hardest:
QL barriers act as de facto denials for controlled anxiety/depression/PTSD meds (high rural prevalence), network inadequacy, PBM opacity, and grievance stonewalling. Same “soft barriers” inside Kaiser workflows that its own safety guidelines warn against—yet executed to block even formulary-listed, MD-necessary meds.
Due to lack of in area coverage but writing policies anyway...Rural vets face 150 mile round trips; continuity broken.
GA Senate Insurance & Labor Committee oversight FAILED:
Chair Sen. Marty Harbin, Sen. Larry Walker—where is accountability? The entire board was contacted and refused to answer. Escalation to @LtGovJonesGA and no answers...
Board’s refusal to investigate violates plain statutory text & public trust.
This needs to stop ✋️
Veterans deserve better than bureaucratic cover-up.
#VeteransCare #PTSD #GAPharmacyBoard #KaiserPermanente #PharmacyAccountability #FeHB #GAVets

1
2
2
755
Apr 29
Direct Account from Source:
Today, April 29, 2026, at a @emoryhealthcare office in Georgia, an elderly man wearing a proud U.S. Air Force Retired hat walked up to the window. He was tired and confused after days of trying to reschedule an appointment. The assistant told him:
“Sir, there is nothing we can do. It’s all routed to the call center.”
This man fought for our country. He served in the Air Force to protect the freedoms we all enjoy. And in his later years, when he simply needed help, he was dismissed like he didn’t matter.
It broke our hearts.
This is the same Kaiser that has performed gender-altering surgeries and care on minors with gender dysphoria in its facilities (including patients touching Georgia), only pausing under outside pressure — while everyday veterans and seniors are told “nothing we can do.”
Our leaders — @burtjonesforga Lieutenant Governor Burt Jones and Speaker Jon Burns — have done nothing, Zero responses. Zero oversight. Zero protection for the very people who served this state and nation. @GASenatePress and @GaHouseHub on Insurance Committees are too busy trying to win votes with Ads instead of Actions
Georgia doesn’t need more excuses.
Georgia doesn't need more direct mailers.
Georgia needs real leadership.
The current leaders are failing us.
Georgia voters deserve to know who actually stands with veterans and patients — and who protects the insurance companies instead...
Spread the word and let's get real change in #Healthcare
Many Georgians are watching.
Many more will speak up.
#Georgia #KaiserFail #VeteransDeserveBetter #HoldThemAccountable #LeadershipMatters
ALT Veterans Deserve Better
11
14
28
11,024
Apr 25
Planned Parenthood will regain eligibility for federal Medicaid reimbursements for non-abortion services after July 4, 2026.
In a 50-48 vote @HawleyMO
tried to stop it. Next time you vote for any democrat remember this is what your voting for... the exploitation of children
FullStop
Apr 23

WATCH: Planned Parenthood executive caught bragging about selling aborted baby body parts and harvested organs, revealing just how lucrative it is.
“I want a Lamborghini!”
Defund & shut them down!
135
Apr 25
Planned Parenthood and similar qualifying providers will regain eligibility for federal Medicaid reimbursements for non-abortion services after July 4, 2026.
In a 50-48 vote @HawleyMO tried to stop it. Next time you vote for any democrat remember this is what your voting for... the exploitation of children
FullStop
Apr 24
Defund & shut down Planned Parenthood now!
This was their “sex-ed” to a minor:
Planned Parenthood: "You can gag them, whip them... Some guys want you to walk 'em around on a leash & pretend they're a dog.
Pure evil.
107