
Neurologist focussing on intracerebral haemorrhage, stroke and neurological emergency medicine @MedUniGraz, Austria and @UCLStrokeRes
Joined June 2023
- Tweets 82
- Following 131
- Followers 189
- Likes 116
2 Photos and videos
Pinned Tweet

3 Nov 2024
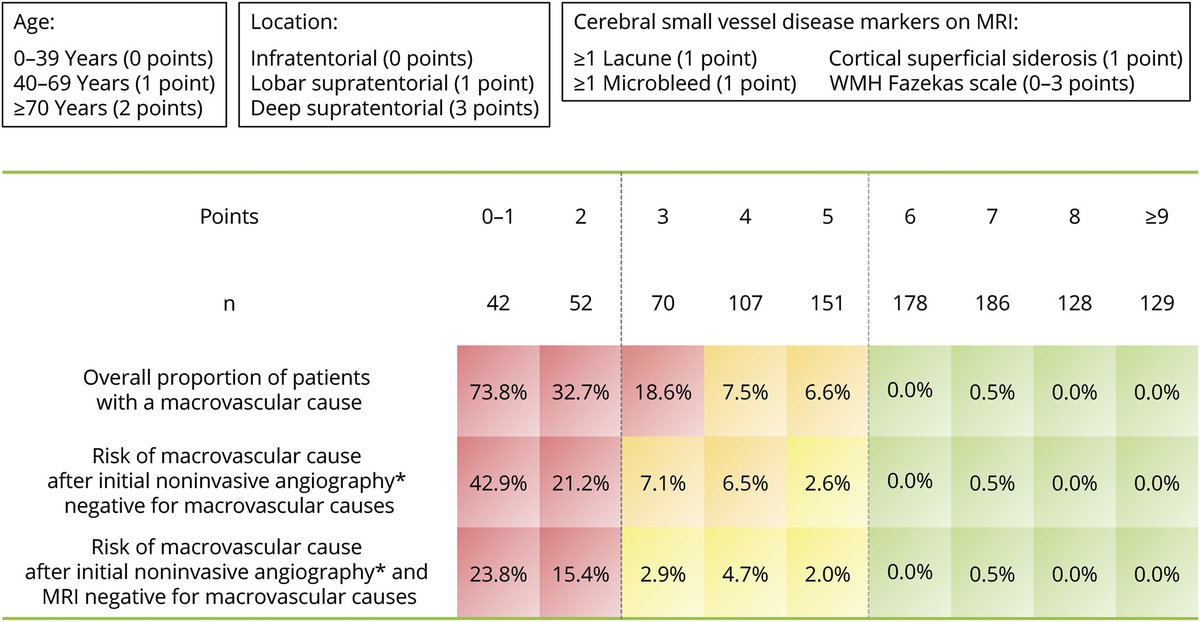
(1/3) In which patients with intracerebral hemorrhage should advanced work-up such as digital subtraction angiography be performed? The MACRO score may help - using a few simple MRI parameters it allows to reliably assess the risk of macrovascular causes: neurology.org/doi/10.1212/WN…
3
29
49
6,775
Simon Fandler-Höfler retweeted

Feb 12
New paper out today - 8 years of work! Prehospital emergency anaesthesia with intubation improves survival by 10.3% in high risk major trauma. Not only life-saving, it is so cost effective (£100m in DALYs/UK/year) it justifies NHS funding of air ambulances thelancet.com/journals/lanre…
3
21
56
4,103
29 Nov 2025
Should patients with AF and history of ICH be treated with oral anticoagulation? A subanalysis of PRESTIGE-AF underlines individualised decisions (based on neuroimaging) - particular risk of recurrent ICH when cortical superficial siderosis and chronic ICH on MRI are present.
27 Nov 2025

In this study the authors assessed the role of neuroimaging in identifying patients with particular susceptibility to #IschemicStroke or intracerebral hemorrhage, with the potential to enable individualized risk stratification: hubs.la/Q03V_lDq0
#NeuroTwitter @SimonFaHo
1
2
57
29 Nov 2025
On the other hand, patients with non-lobar ICH had a higher risk of recurrent ischaemic stroke — possibly due to multiple concurrent stroke mechanisms (AF small vessel disease). Major limitations: modest sample size, few outcome events. Larger meta-analyses needed.
2
28
10 Nov 2025
1/3 Should patients with AF and history of intracerebral haemorrhage treated with oral anticoagulation? This subanalysis of PRESTIGE-AF provides new data, indicating that individualised decisions based on neuroimaging ( clinical profiles) might be prudent: neurology.org/doi/10.1212/WN…
1
2
47
10 Nov 2025
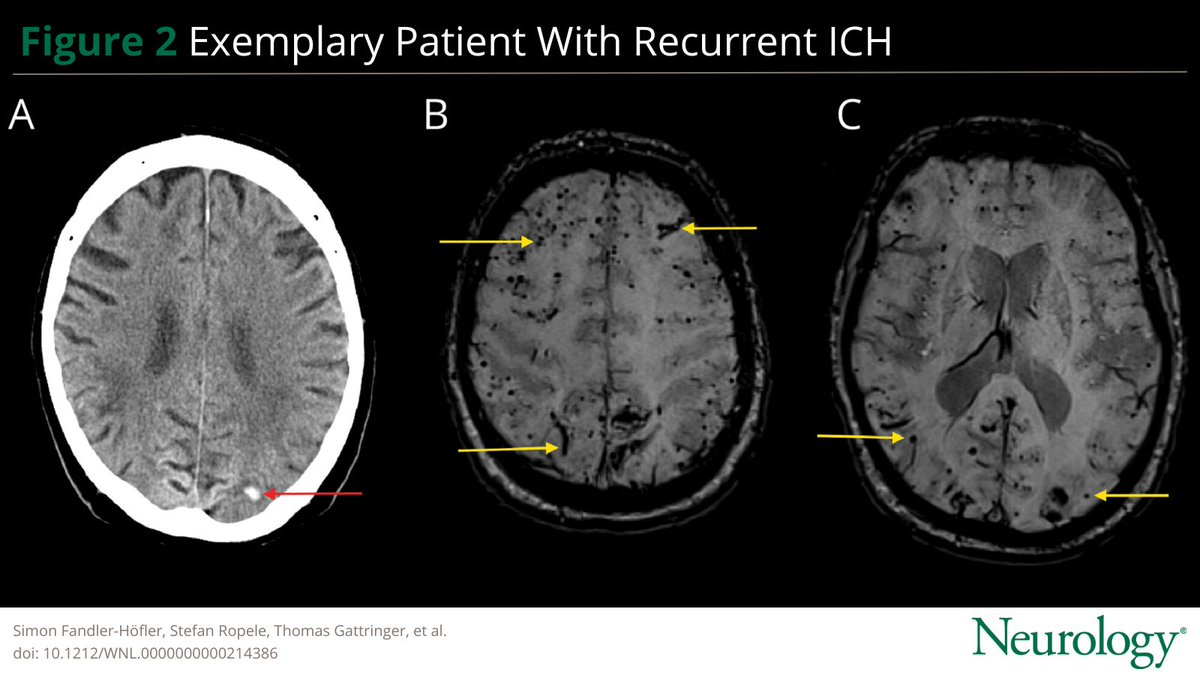
2/3 In this RCT (n=313) randomising patients with AF and prior ICH to anticoagulation vs not, cortical superficial siderosis and chronic intracerebral macrohaemorrhages on MRI strongly predicted recurrent ICH — potentially identifying patients at excess bleeding risk from OAC.
1
2
40
10 Nov 2025
3/3 On the other hand, patients with non-lobar ICH had a higher risk of recurrent ischaemic stroke — possibly due to multiple concurrent stroke mechanisms (AF small vessel disease).
Major limitations: modest sample size, few outcome events. Larger meta-analyses needed.
2
35
Simon Fandler-Höfler retweeted

18 Jul 2025
#FlashbackFriday !
🌍🧠World Stroke Organization (WSO): Global intracerebral hemorrhage factsheet 2025
journals.sagepub.com/doi/ful… @adrianpj1 @WorldStrokeOrg @WorldStrokeEd

15
20
1,352
Simon Fandler-Höfler retweeted
15 Jul 2025
🧠Study of long-term outcome in young patients after ischemic stroke or TIA
⬆️Women had higher risk of post-stroke depression, anxiety & fatigue
🫀🚭Hypertension & smoking were modifiable risk factors contributing to worse outcome
Read more here!👇
journals.sagepub.com/doi/abs…
1
3
391
Simon Fandler-Höfler retweeted

2 Jul 2025
This is a breakthrough study that forges a new future — POC biomarkers for identifying #ICH in the prehospital phase.
Rapid Diagnosis of ICH with GFAP Levels on a Point-of-Care Device (DETECT) @neurology #curingcoma neurology.org/doi/10.1212/WN…
1
22
43
2,949
Simon Fandler-Höfler retweeted

21 Apr 2025
#STROKE: In patients with acute ischemic stroke, admission NT-proBNP may predict the in-hospital development of atrial fibrillation detected after stroke (AFDAS), and a threshold of 505 pg/ml confers good discriminatory value. #AHAJournals ahajournals.org/doi/10.1161/…
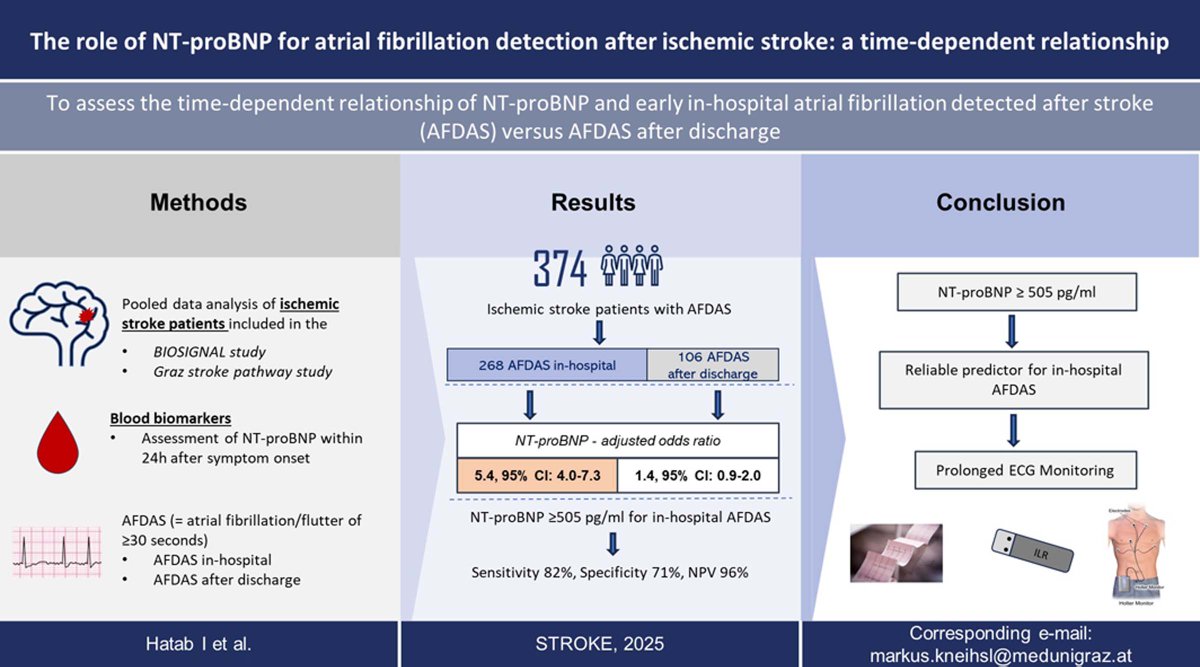
ALT Graphic abstract in Hatab and Kneihsl et al.
2
38
107
10,510
Simon Fandler-Höfler retweeted

4 Apr 2025
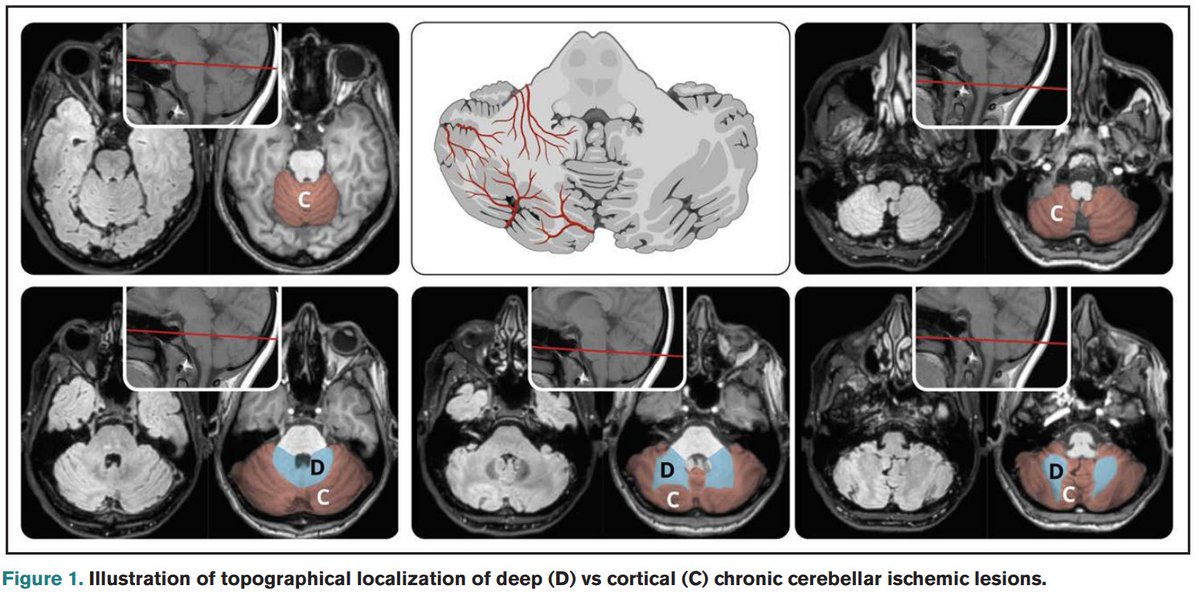
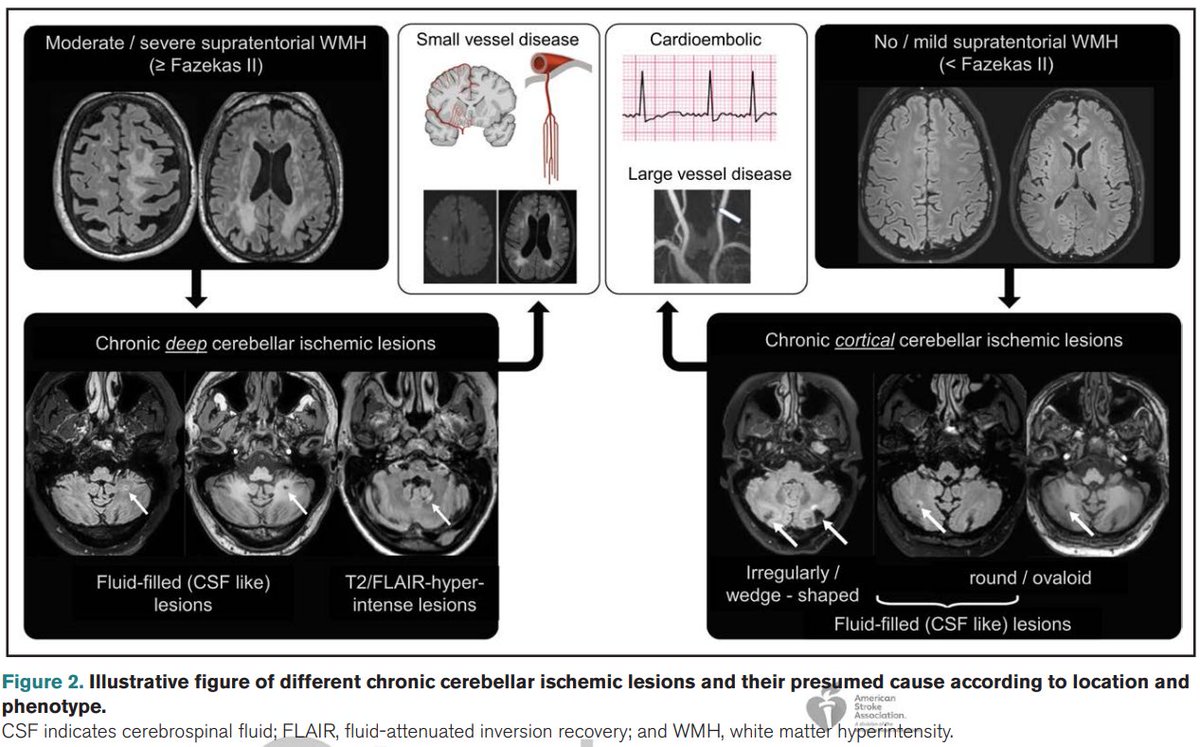
How do chronic ischemic lesions differ in patients with #AtrialFibrillation and #SmallVesselDisease?
We compared MRIs from @ELAN_Trial and #SVD cohorts: whereas AF patients had mostly cortical cerebellar lesions, SVD patients had deep lesions
ahajournals.org/doi/pdf/10.1…
2
27
50
2,815
Simon Fandler-Höfler retweeted

3 Mar 2025
EURECA: New data on recurrent ICH: every second recurrence is adjacent to index ICH. Those bleedings occur early and are strongly associated with CAA. Great collaboration lead by @mbgoeldlin @StrokeBern
Author interview podcast: edhub.ama-assn.org/jn-learni…
jamanetwork.com/journals/jam…
3
30
45
2,490
Simon Fandler-Höfler retweeted

1 Mar 2025
New in @JNNP_BMJ - the next chapter in the story of iatrogenic CAA 📕 and it really does seem to be different to sporadic CAA. Presence of deep haemorrhagic pathology in particular is unexpected but persistent signal.
So what does this mean? … 1/3 🧵
jnnp.bmj.com/content/early/2…
2
10
32
2,410
Simon Fandler-Höfler retweeted

22 Feb 2025
Our meta-analysis of 279 stroke studies over 24 years, with 117K participants, found that 1 in 2 stroke patients experience adverse non-motor outcomes. Adjusted meta-regression shows 8/10 domains persist more than 10-years. Time for change in stroke care. jamanetwork.com/journals/jam…
1
16
28
3,241
Simon Fandler-Höfler retweeted

20 Feb 2025
Check out our latest paper providing the most comprehensive description of the phenotype and natural history of iatrogenic Cerebral #Amyloid Angiopathy. A great international collaboration thanks to @SimonFaHo @DrGargiBanerjee @KKaushikMD @LVpanteleenko and many others!
1
10
33
2,962
19 Feb 2025
1/4 Iatrogenic cerebral amyloid angiopathy (iCAA) is a scary rare disease affecting patients 30-50 years after possible CNS exposure to pathological amyloid-beta. In a large international collaboration, we investigated neuroimaging findings and clinical outcomes in 51 patients.
2
7
27
2,591
19 Feb 2025
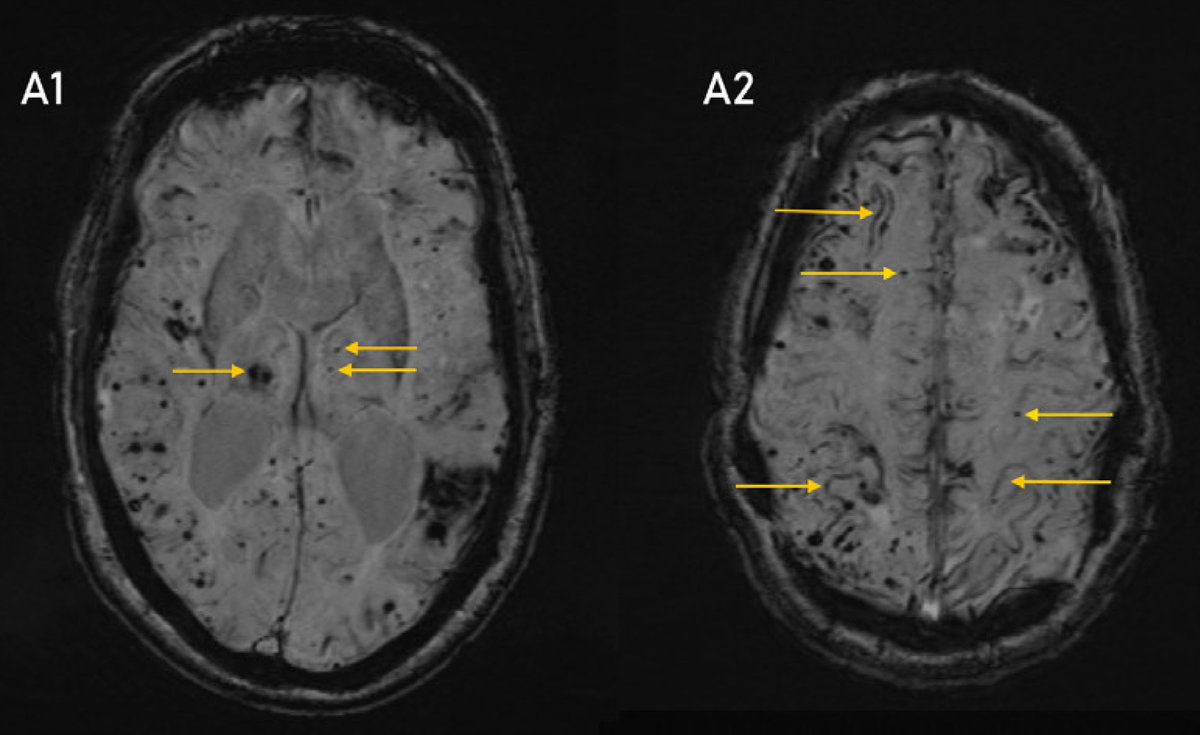
3/4 Besides severe CAA on MRI, we found:
a) major progression of CAA markers over 4 years
b) ipsilateral-dominant spread of haemorrhagic lesions (from amyloid-beta exposure)
c) frequent deep microbleeds
d) frequent inflammatory changes
e) very frequent small intragyral ICH
1
1
196
19 Feb 2025
4/4 This indicates that patients with iCAA appear to have distinctive MRI characteristics, which might differentiate iCAA from other CAA subtypes and provide new insights into disease mechanisms.
jnnp.bmj.com/content/early/2…
@DrGargiBanerjee @UCLStrokeRes @BenStorti @KKaushikMD
2
2
207
Simon Fandler-Höfler retweeted

11 Feb 2025
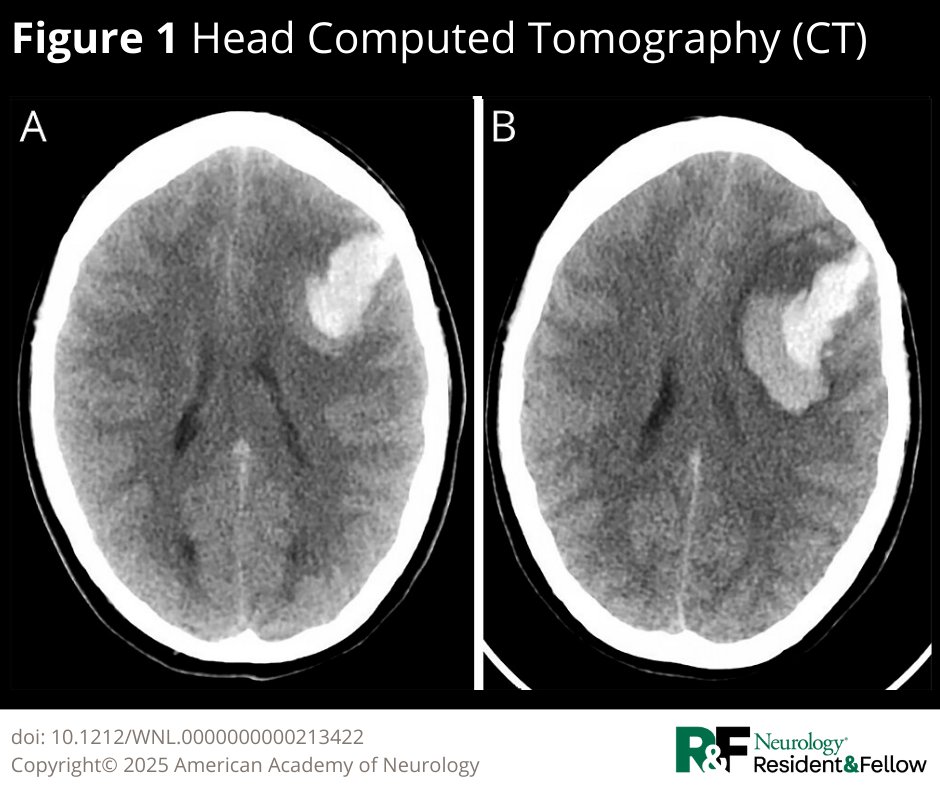
This case highlights the diagnostic approach and importance of thorough clinical evaluation of young patients with intracerebral hemorrhages.
hubs.la/Q035vSv10
#NeurologyRF #NeuroTwitter
1
22
60
7,534