
May 19
Common Consent Elements for Research Involving Persons with Disorders of Consciousness (CCE-DOC), new in @NeurocritCareJ @CuringComa
link.springer.com/article/10… #neurology #neuroethics
2
243
Supratentorial Brain Lesions in Unconscious Patients Map to a Common Human Brain Circuit that connects the fronto-insular-limbic association cortex with subcortical arousal nodes and the ventral striato-pallidal circuitry
This observation has zero direct clinical relevance as of now -- but it might in the future.
#curingcoma
onlinelibrary.wiley.com/doi/…
1
4
9
796

Apr 24
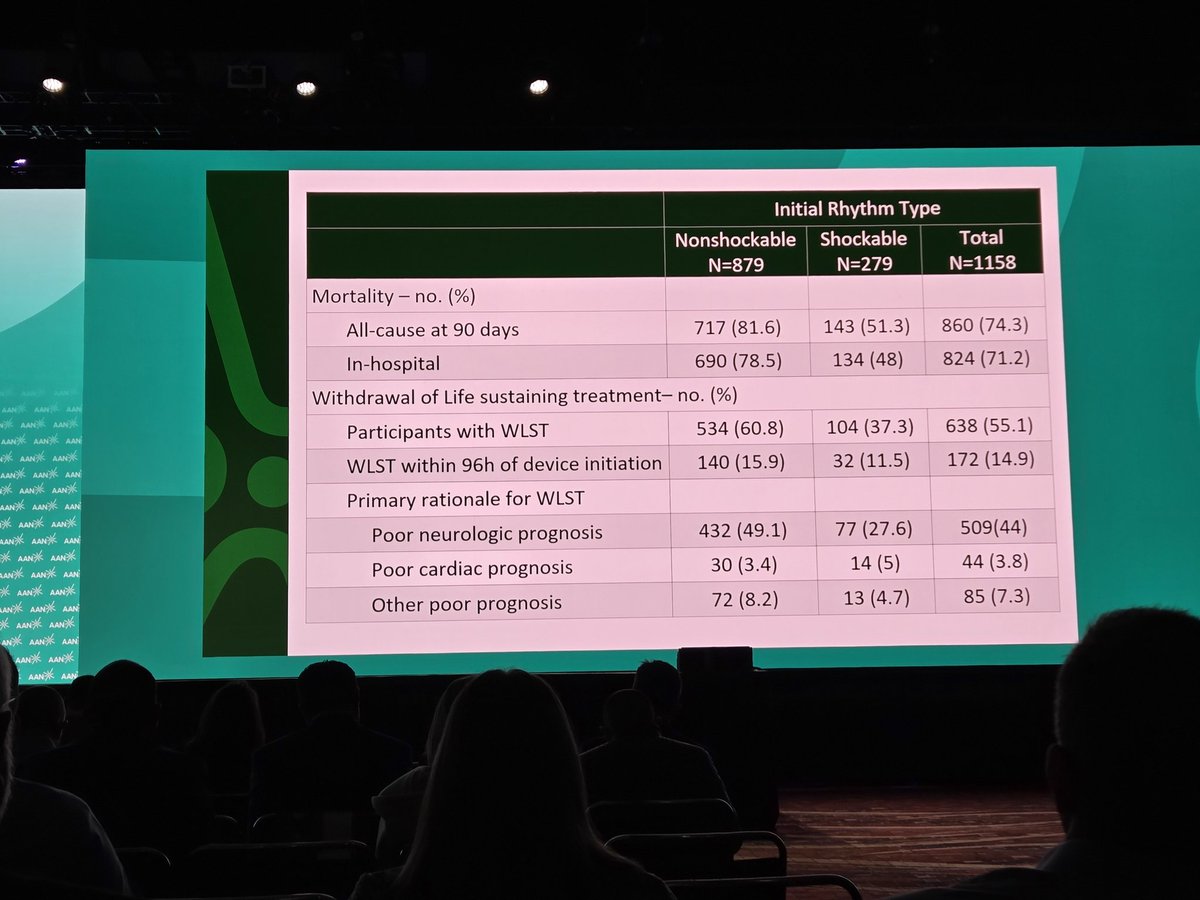
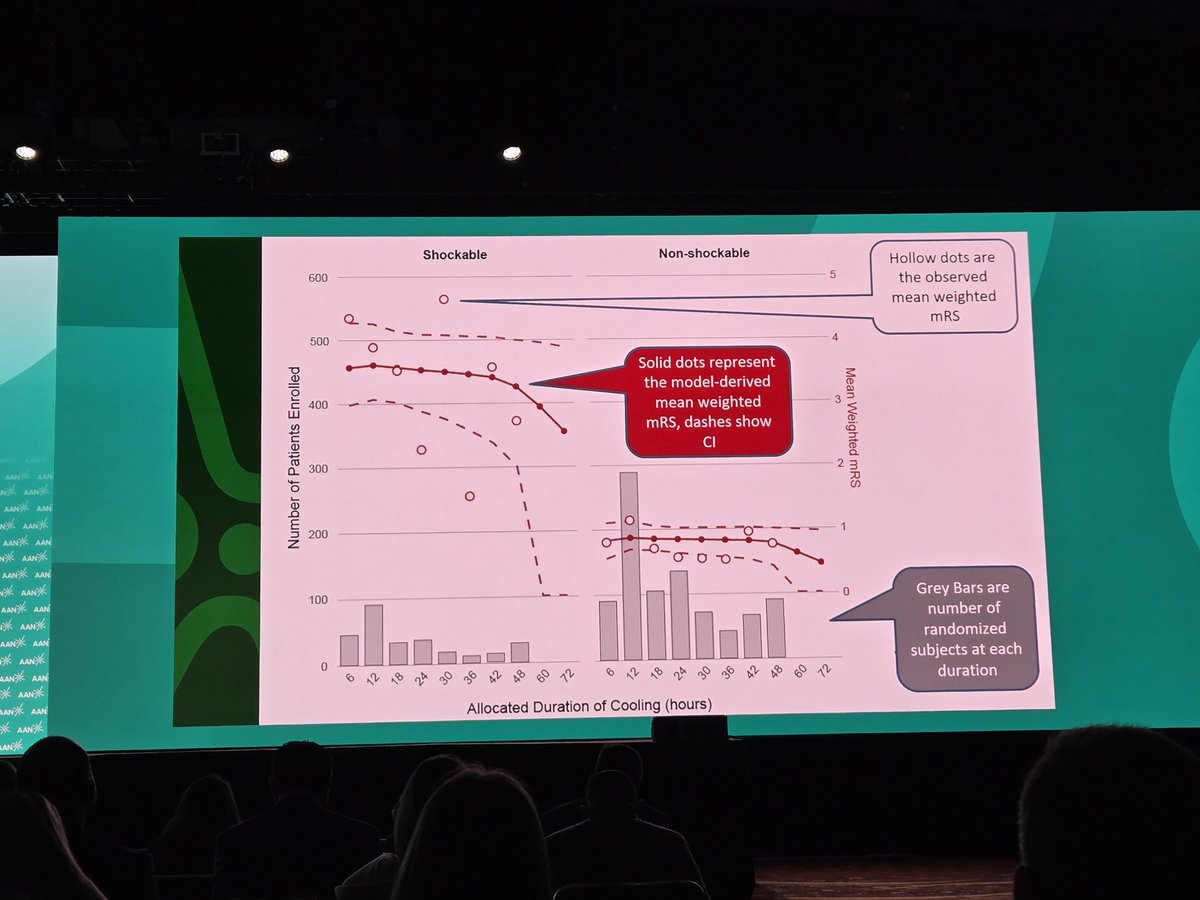
#ICECAP is out. This NIH-funded RCT compared different durations of cooling (12-72 hours) after cardiac arrest and found no impact of longer cooling inervals on survival or functional outcome. But there was no arm without TTM at all -- which is what many centers have now reverted to....
#curingcoma
Apr 22

#ICECAP results from #AANAM . Can we all agree that SOC for post arrest comatose patients should be normothermia?

1
6
16
2,307
Apr 24
Nice summary of best #TTM practices in neurocritical care. Please note that proactive TTM for any target 32-37.5 °C and avoidance of fever is the best prioactice for cardiac arrest.
Don't let them spike and then chase the fevers...
#curingcoma
link.springer.com/article/10…
2
11
1,017
It turns out that infratentorial ICP monitoring is feasible, can identify ICP gradients, and offers superior prognostic information to standard supratentorial monitoring in patients with cerebellar mass effect.
#curingcoma
link.springer.com/article/10…
1
5
18
2,077
Case Fatality of Subarachnoid Hemorrhage differs by by Aneurysm Location.
The highest case fatlaity rates are vertebrobasilar (54%) and MCA (40%), followed by A-comm (29%) and ICA (28%).
The majority of excess deaths with Vb and MCA aneurysms is due to pre-hospital sudden death. About 1/3 of all SAH-related mortality is due to sudden pre-hospital cardia arrest.
#curingcoma
|neurology.org/doi/10.1212/WN…
1
11
24
1,050
Rapid response teams are going to become more sophisticated and critical-care capable. Like slamming R heart catheters into inetermediate to submassive PE patirents:
@nejm -- Right-sided Ultrasound-Mediated Catheter-Directed Fibrinolysis (EkoSonic) for Intermediate-Risk Acute Pulmonary Embolism -- in addition to standard anticoagulation.
Primary outcome: Death, cardiopulmonary collapse, or recurrent PE in <7 days:
With UMCDF: 4%
Standard care: 10%
Effect driven by lower risk of cardiopulmonary collapse.
#curingcoma
nejm.org/doi/full/10.1056/NE…
3
9
934

Did you know March 22 was World Coma Day? check out my talk on patient and caregiver empowerment #curingcoma @neurocritical
youtu.be/e2Sx-dXo9PM?si=FhuW…
5
145
Mar 20
As documented in this GWTG analysis, when anticoagulation-associated #ICH patients are transferred, it leads to a massive increase in onset-to-treatment time:
Transfer: 512 mins (~10 hours)
No transfer: 273 mins (4.5 hours)
Both of these are awful of course.
About 1/3 of those transferred didn't get reversed until arriving at the 2nd hospital.
That should never happen!
#curingcoma
#codeich
ahajournals.org/doi/pdf/10.1…
1
1
7
678
Mar 20
A single center non-randomized real world look at Minimally invasive surgery for large #ICH
• 38 underwent MIS
• 61 had open surgery
Those treated with MIS had:
• Better outcomes (favorable 6 mo mRS 40% at 15%)
• Lower mortality (0% vs 15%)
• Higher excellent clot evacuation (90% vs 80%)
• Shorter ICU length of stay (5.5 vs 7.0 days)
Do you perform MIS for ICH at your site?
#codeich
#curingcoma
sciencedirect.com/science/ar…
1
2
10
868
Mar 19
Endovascular vs Medical Treatment of Basilar Artery Occlusion
@JAMANeuro
“At 3 years, the clinical benefit of EVT in patients with acute BAO was durable, with substantially better functional outcomes and reduced mortality compared with medical management.
These results reinforce EVT as the standard of care for BAO and support broader implementation and timely access to thrombectomy services.”
#curingcoma
jamanetwork.com/journals/jam…
1
13
38
2,250



2/ As some of you may know, I am very interested in the topic of #CovertConsciousness and do believe this will become a major player in our ability to better prognosticate in #coma patients.
I suspect the future of #neuroritcare will be around this. #CuringComa.
1
4
111
1/ 👋 there #neurotwitter #neurosky #neurocritcare, as part of my @neurocritcarej #SoMeAmbassador role, today we will be breaking down the following article:
link.springer.com/article/10…
about #covertconsciousness and #NIRS! #CuringComa
3
3
5
402
Mar 18
Another new publication by the great team at @nymedcollege @WMCHealth @nymcbrainspine
In this retrospective cohort study of 10,375 adult patients with ruptured AVMs, vasospasm occurred in approximately 3%. Risk factors for vasospasm included subarachnoid hemorrhage, male sex, hydrocephalus, and leukocytosis.
Delayed arterial spasm more than doubles the risk of mortality at 3, 6, and 12 months.
Perhaps continuous ventricular irrigation (e.g. IRRAFlow) can be a better way when large amounts of IVH are present?
#curingcoma
link.springer.com/article/10…
3
13
1,026
Mar 14
I really get excited about high-impact papers. This one is an instant classic.
The investigators surveyed ~250 TBI survivors and ~250 TBI caregivers, an average of 12 years after the injury.
They asked – what is the minimally acceptable outcome that is acceptible after severe TBI?
Both survivors and care givers agreed –– recovery of yes/no communication is the basic common denominator.
Being able to have any semblance of control about what happens to you. A basic human right, worth experiencing. So interesting.
In my ICU end of life conversations moving forward, I am going to use "yes/no" and "following commands" in equal balance when descibing MCS/coma outcomes.
Saying yes or no –– sounds a way lot better than following commands.
#curingcoma
@HarvardHealth
@VUMCDiscoveries
Perspectives of Persons With Lived Experience on Acceptable ... : Critical Care Medicine journals.lww.com/ccmjournal/…
4
16
64
6,142
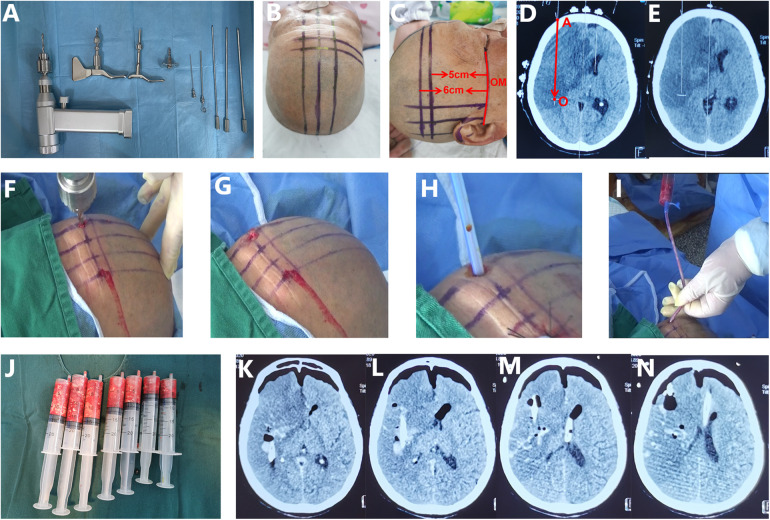
Get ready for this. These Chinese investigators report a cohort of 121 malignant MCA infarction patients age >60, 47 of whom underwent drill-assisted sterotactic aspiration of the infarcted tissue from 24-72 hrs after onset. Check out the CT images and the 70 mL of nectrotic brain tissue in the image below to give you an idera of what they were doing.
Retrospective, not randomized -- but the results were great.
Herniation: 47% vs 9%
Death: 65% vs 9%
Favorable mRS (0-3): 3% vs 26%
Not only #curingcoma –– cheating death.
pmc.ncbi.nlm.nih.gov/article…
5
60
168
24,328
Here's a free PDF of a recent editorial in Intensive Care Medicine outling some of the nuances of using a lumbar drain in addition to a ventricular drain in high-grade SAH with significant amounts of IVH. Very enlightening! Makes me want to try this out...
#curingcoma
boa.unimib.it/bitstream/1028…
1
4
20
1,681

Feb 12
link.springer.com/article/10…
I wanted to share our latest study (last study fully completed at Phoenix Children's, before I left), now published in Neurocritical Care, where we demonstrated a method using EEG to detect signs of covert conscious processing in comatose-appearing critically ill children.
Access to the full article can be seen here: rdcu.be/e3xW3
This study was difficult and challenging - probably the most challenging study I've done at this point in my career. Everything that could've gone wrong did go wrong. There were many points where I thought the study would halt, but it was seen to the end, and now it's complete and published.
Thanks to everyone who supported this work, especially my co-authors.
@PNCRGtweets @CuringComa @NeurocritCareJ @neurocritical
4
5
499
Jan 28
Welcoming Dr David Fischer front left) to @NeurologyNymc Grand Rounds today! Great talk on coma prognostication
#curingcoma
@PennNeurology
@WMCHealth
@almuftifawaz
@A_Bauerschmidt

21
1,340