
Director, Neurovascular/Skull Base & Pituitary Surgery, @neurosurgerynj @CBMCNJ @RWJBarnabas, email: jliu@neurosurgerynj.com
Joined March 2011
- Tweets 1,117
- Following 720
- Followers 5,259
- Likes 1,893
549 Photos and videos









Pinned Tweet

20 Sep 2020
Clipping of giant ophthalmic and A1 lenticulostriate artery #aneurysms using suction decompression Dallas technique #OpVid @RUNeurosurgery @SaintBarnabasNJ @RWJBarnabas @NASBSorg @ASCsurgical @BAFOUND @ASAHStudy_Aust @joseph_quillin @CNS_Update @cvsection @AANSNeuro
13
25
178
May 31
Moments like this remind me of "our why." ✨
I am incredibly humbled and touched by these words from a patient who traveled all the way from Kentucky to our team at Cooperman Barnabas Medical Center. Knowing that our patient felt safe, cared for, and supported after traveling so far for surgery means the world to me.
Complex surgeries for brain tumors and skull base lesions require a massive team effort, and this outcome would not be possible without our world-class, dedicated nursing staff. Thank you to my teams at @CBMCNJ @RWJBarnabas @NeuroSurgeryNJ for your unwavering commitment, and thank you to our patients for trusting us with your care.
Complex care truly takes a village, and I am lucky to work alongside the best. 🙏🏥
#SurgeonLife #PatientCare #HealthcareHeroes #CBMC #Neurosurgery #BrainTumorSupport #paraganglioma @PheoPara

Check out this 5-star Google review from a grateful patient who traveled all the way from Kentucky to New Jersey for a complex surgery with Dr. Liu and our dedicated nursing team at CBMC.

5
389
May 5
Great Stryker Mobile Lab Skull Base Course at @GeisingerHealth!
An outstanding few days of education featuring detailed skull base cadaver dissections, hands-on surgical training, and invaluable experience for our residents. The collaborative environment made it even better—lots of meaningful exchange of ideas, techniques, and perspectives.
A special thanks to @drRMP10 for the kind invitation and excellent organization of the event, and to @StrykerNS for supporting this important educational experience.
Grateful for the opportunity to learn, teach, and grow alongside such a dedicated group. Looking forward to the next one!

1
14
1,235
James K. Liu, MD retweeted

Apr 13
Thank you to our sponsors, educational grant supporters, guest speakers, Northwestern Medicine faculty and attendees who made the 2026 Chicago Advanced Training in Open and Endoscopic Surgery a success. We appreciate the collaboration that made this educational program possible.

2
10
509
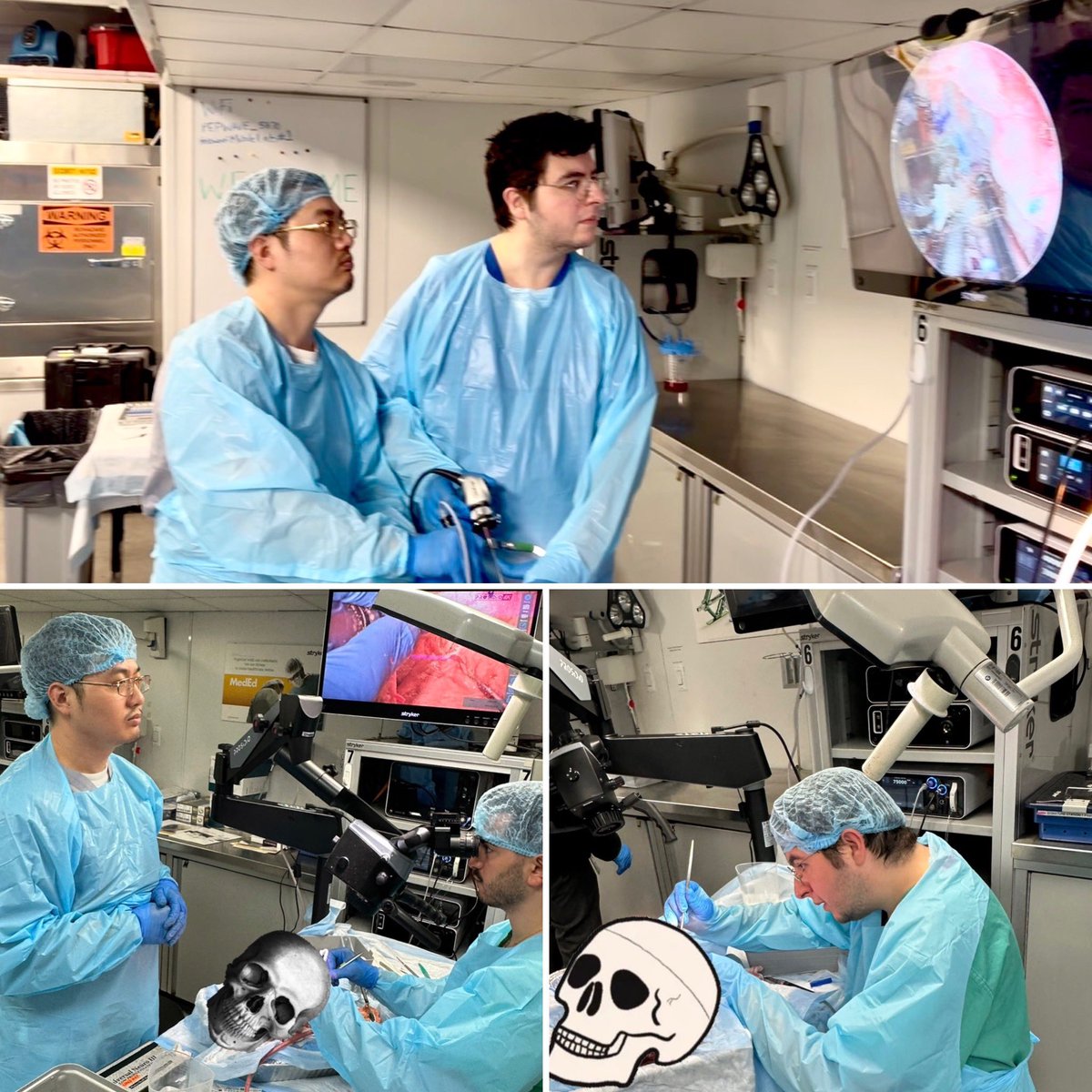
Apr 13
Had an amazing time at the Northwestern @NMskullbase Skull Base Course—truly an outstanding experience.
Northwestern is where my career began nearly 20 years ago, so it was especially meaningful to return and participate as faculty in such a fantastic course. Coming back to where it all started brings things full circle in the best way.
A big thanks to Jim Chandler for the kind invitation and for directing such a high-quality program.
It was also great catching up with friends and colleagues, and especially rewarding to see two of my former medical student mentees @phabinly @gurk_kohli now thriving in their neurosurgery residencies. Moments like these remind me why we do what we do.
instagram.com/reel/DXDil1Bt7…
@DoctorZada @PrevedelloDanny @StephenTMagill @KaraParikh @phabinly @NeuroSurgeryNJ @CBMCNJ @gurk_kohli


1
6
36
2,278
James K. Liu, MD retweeted
Apr 11
That’s a wrap on Day 1 of the 2026 Advanced Training in Open and Endoscopic Surgery. Thank you to our guest speakers and faculty for an outstanding day of presentations and hands-on training.



3
13
937
James K. Liu, MD retweeted
Apr 11
James Liu, MD (@SkullBaseMD), will present on transcranial suprasellar approaches, including the orbitozygomatic approach, ahead of the first dissection of the day.

2
18
1,086
Mar 12
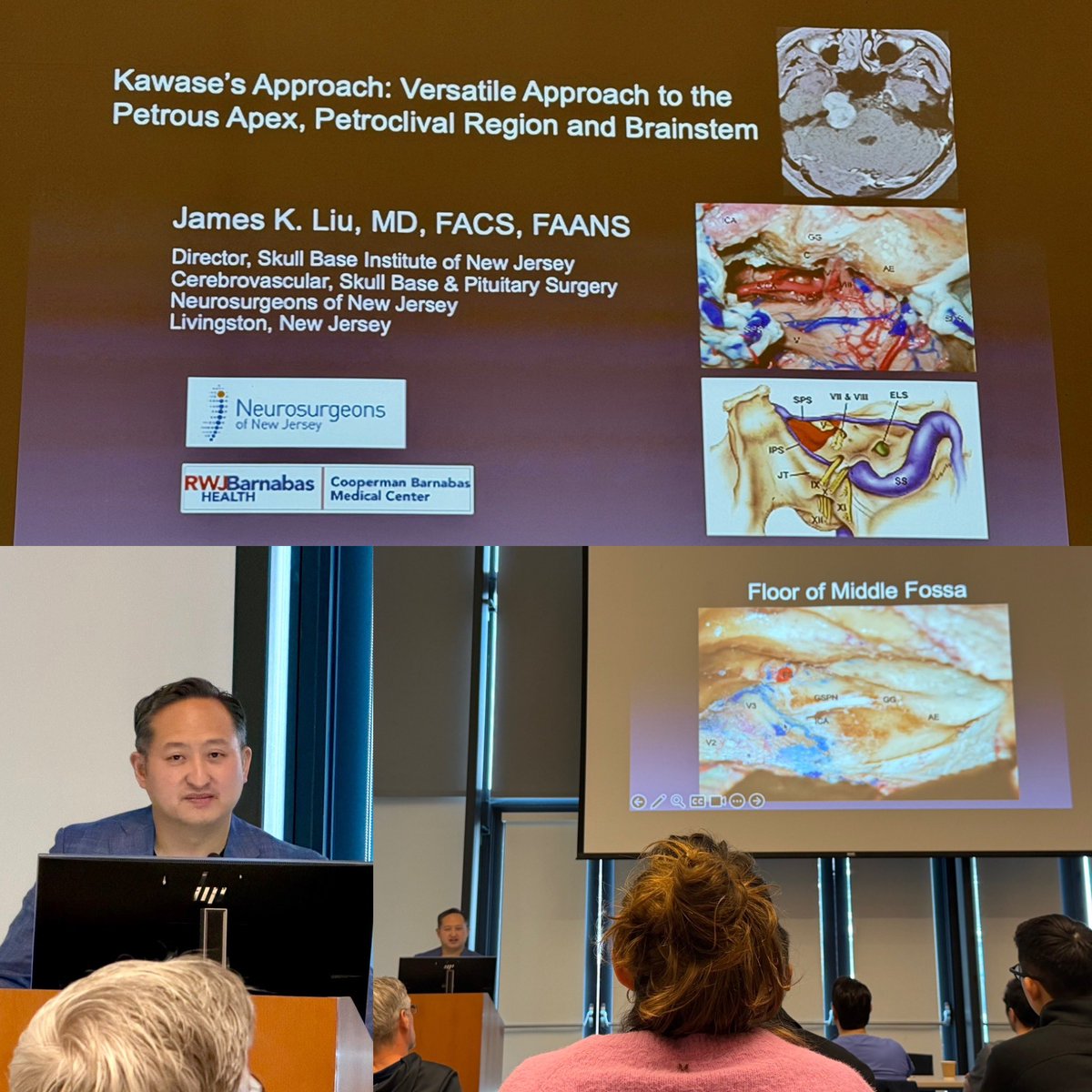
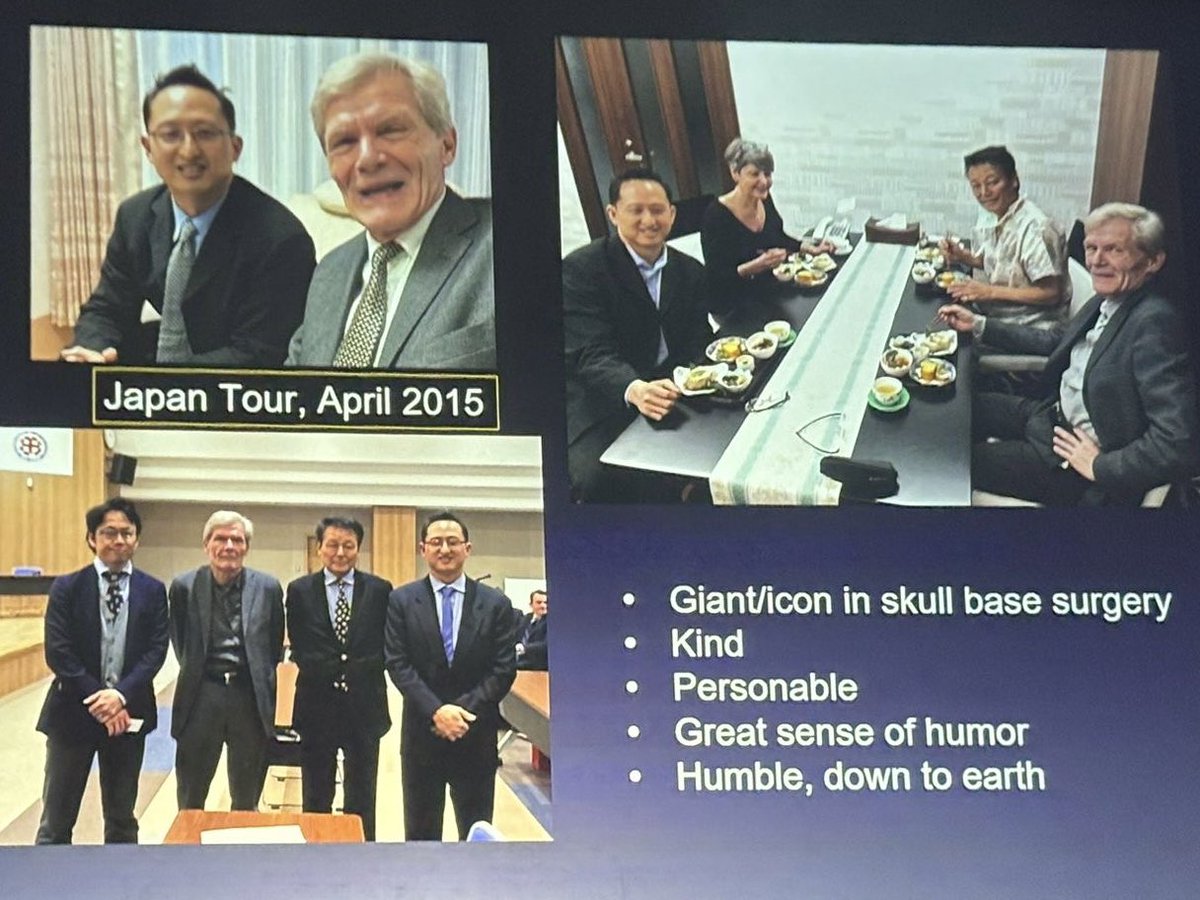
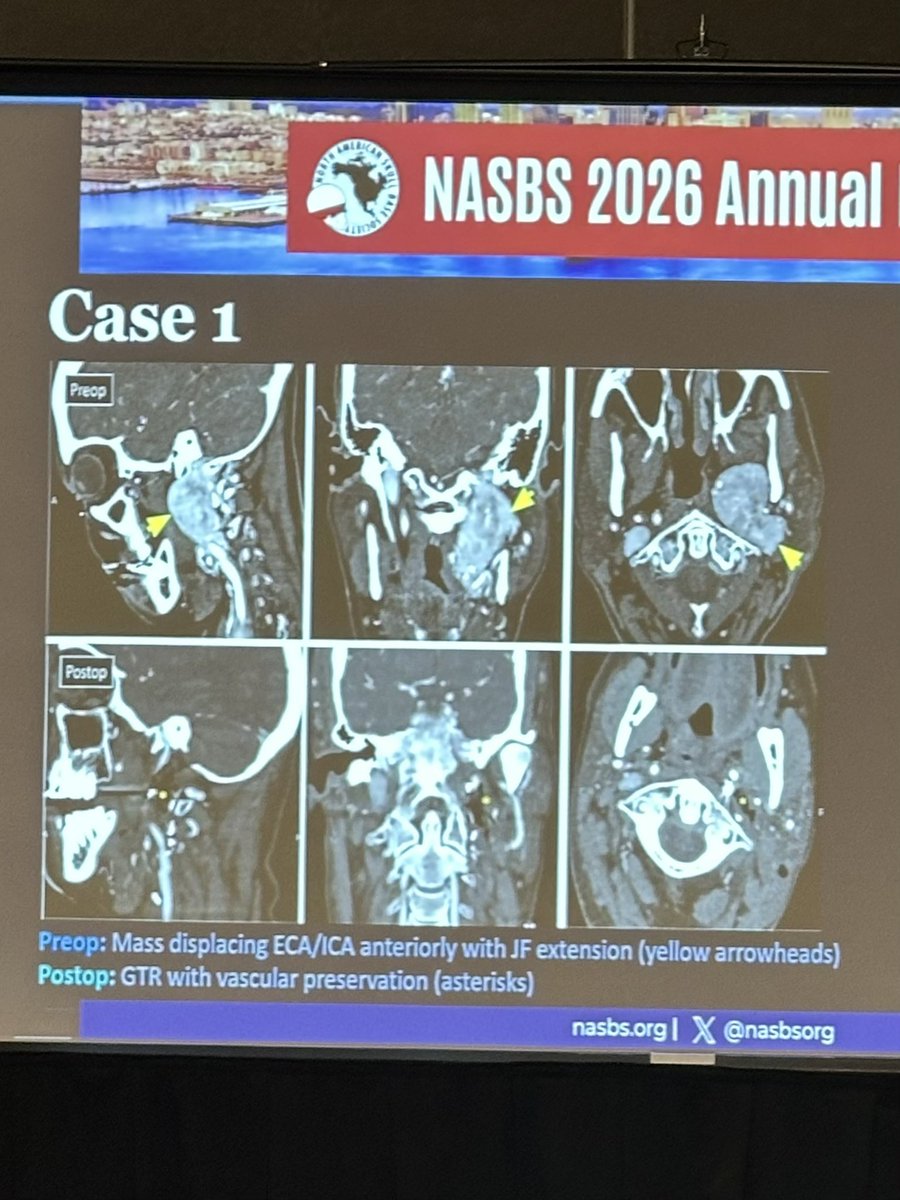
Bernard George Education Day #Nasbs2026 organized by @SC_Froelich. We honored the late Prof. B. George for his outstanding contributions to skull base surgery, technical mastery, commitment to education, and personal friendship. Spoke on modern microsurgical approaches to jugular foramen tumors, a topic that was heavily influenced by his teachings. Great to hear perspectives and personal anecdotes from his trainees, friends and colleagues whom he has greatly impacted. @jacquesmorcosmd @PrevedelloDanny @NASBSorg @NeuroSurgeryNJ @APHP

1
2
22
1,499
Mar 9
Congrats to @Rutgers_NJMS med student Jin Ha for presenting our functional and quality of life outcomes of my vagal #paraganglioma microsurgery series. Great seeing my old residents Kevin Zhao and Raja Jani. #JerseyStrong @NeuroSurgeryNJ @CBMCNJ @RWJUH @RUNeurosurgery @NASBSorg #NASBS2026


34
1,596
Mar 9
Great catching up with my mentor Bill Couldwell and fellow University of Utah Alumni, @MichaelKarsy and @DrWallyMD at #nasbs2026 @NASBSorg #UtahStrong @UofUNeurosurg @NeuroSurgeryNJ

3
1
27
1,060
Mar 8
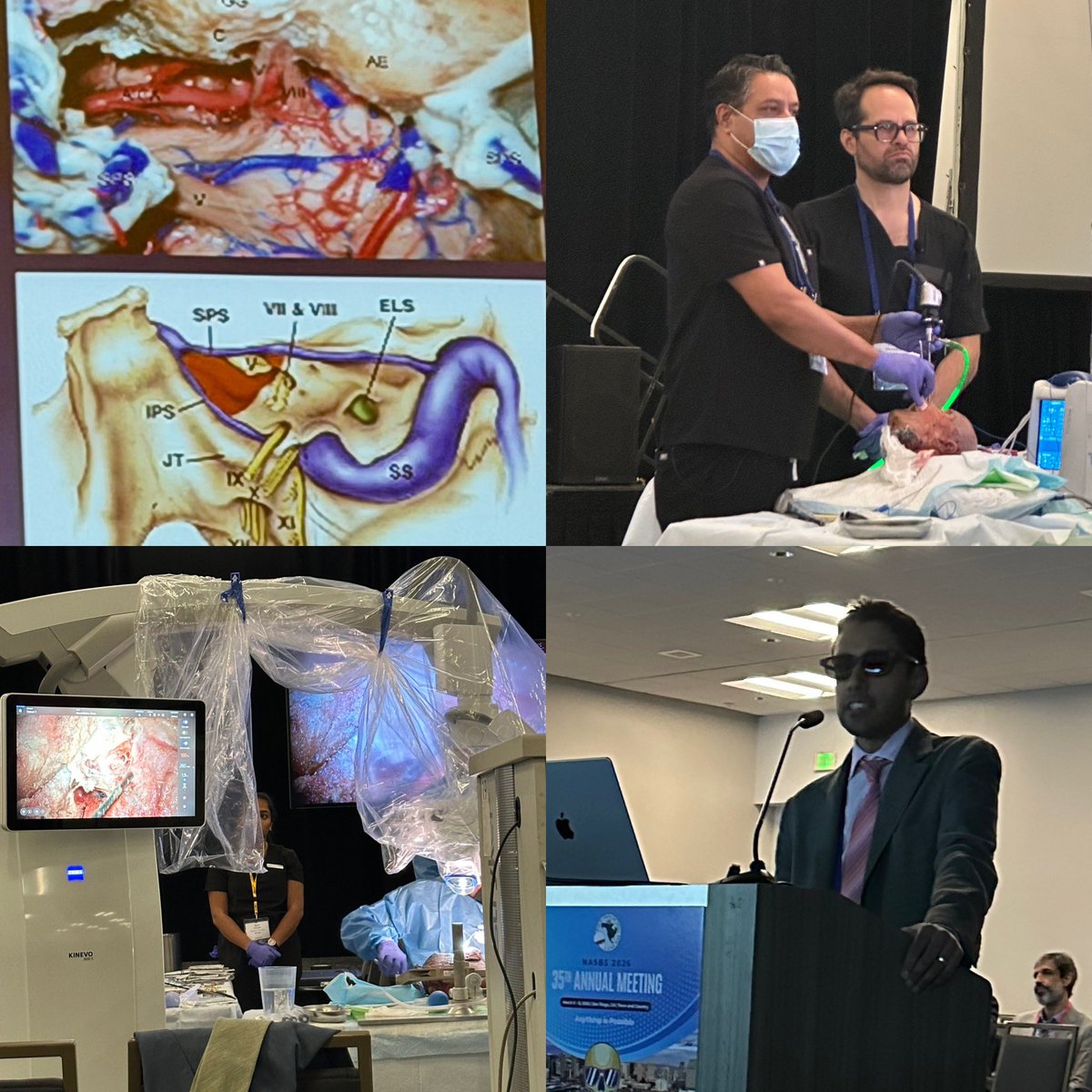
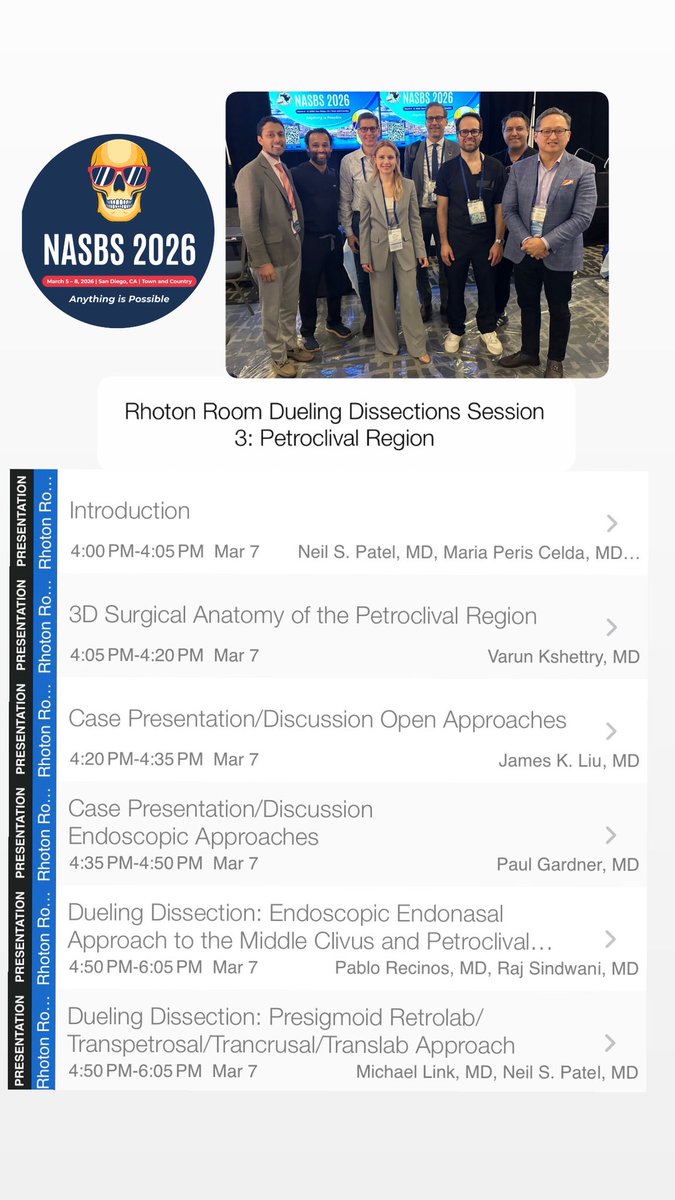
Everything you wanted to know about the petroclival skull base but was afraid ask. Amazing Rhoton room dueling dissection today! #nasbs2026 @PerisCelda @MayoClinicNeuro @PabloRecinosMD @MdSindwani @CleClinicNS @NYUneurosurgery @NeuroSurgeryNJ @CBMCNJ @RWJBarnabas @NASBSorg
2
1
45
1,636
Mar 6
Annual Meeting of the North American Skull Base Society #NASBS2026 pre-meeting cadaver dissection course. Great to see friends and colleagues. You stay classy, SanDiego! @NeuroSurgeryNJ @drRMP10 @MohamedALabibMD @DrBaskaya @GarniBDarian @ASamyYoussef @ProfesorMura @DrShaanRaza @NASBSorg @CBMCNJ @RWJBarnabas



1
1
39
1,806
Mar 2
Aloha! Honored to give an invited lecture on "The Art of the Clip: Microsurgical Clipping Strategies for Complex Cerebral Aneurysms" at the 11th Joint Neurosurgical Convention (The 11th Pan-Pacific Neurosurgical Congress and the 11th International Mt. BANDAI Symposium for Neuroscience) in Honolulu, Hawaii. A sincere mahalo to Dr. Masahiro Shimizu from Kanto Neurosurgical Hospital and Dr. Soichi Oya from Gunma University for organizing this great event. This meeting has a rich legacy, greatly shaped by the late Prof. Takanori Fukushima, who was instrumental in developing this meeting, bringing together top neurosurgeons from the Pan-Pacific region and Europe, blending academic progress with personal connection. The gala dinner was a particularly moving tribute to the late Prof. Takanori Fukushima. Taka, your presence at the congress was missed, but your legacy lives on in every surgeon you inspired and every patient helped. Every time we step into the OR, not a single complex brain operation goes by without channeling our inner Fukushima.
#Neurosurgery #SurgeonLife #JNC2026 #BrainSurgery #FukushimaMafia @neurosurgerynj @CBMCNJ @RWJBarnabas



5
627
Mar 1
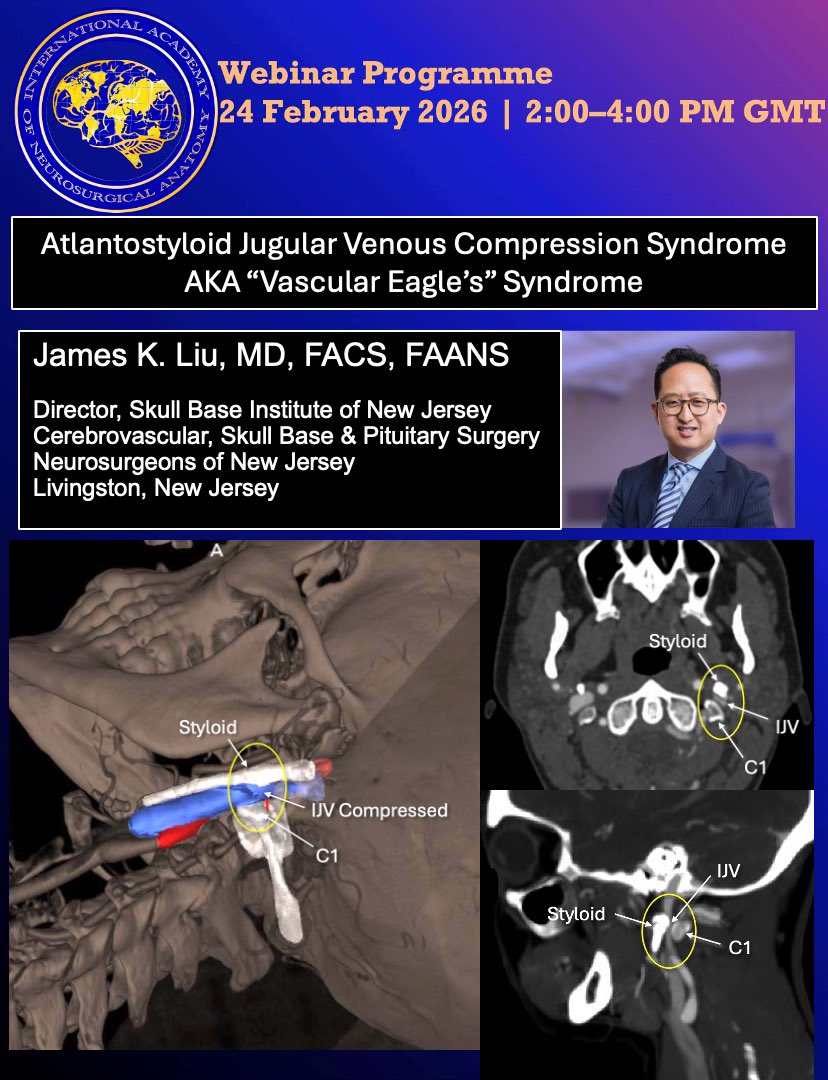
I recently had the privilege of speaking at a webinar hosted by the International Academy of Neurosurgical Anatomy (IANA) on a topic that is both deeply important and profoundly under-recognized: Atlantostyloid Jugular Venous Compression Syndrome.
This rare neurological condition results from severe compression of the internal jugular vein between the styloid process and the C1 transverse process. When this venous outflow obstruction occurs, it can significantly impair cerebral venous drainage, leading to symptoms consistent with elevated intracranial pressure.
A Devastating — and Often Dismissed — Condition
Patients with Atlantostyloid Jugular Venous Compression Syndrome frequently suffer from:
• Persistent headaches
• Debilitating head pressure
• Visual snow
• Brain fog
• Inability to function in daily activities
• Profound fatigue
• Dizziness
• Tinnitus
What makes this condition particularly tragic is not only the severity of the symptoms, but how often patients are dismissed. Many see multiple specialists across neurology, ENT, ophthalmology, psychiatry, and primary care. Imaging may be labeled “normal” if venous compression is not specifically evaluated. Too often, patients are told that nothing is wrong — or worse, that their symptoms are psychological.
These individuals are not imagining their illness. They are living with a structural venous outflow obstruction that, when properly identified, is treatable.
Why Proper Decompression Matters
A key focus of my lecture was the importance of complete, 360-degree venous decompression. Inadequate surgical intervention can leave patients just as symptomatic as before, resulting in persistent and debilitating impairment.
Effective treatment requires:
• Styloidectomy past the point of compression, extending to the skull base
• C1 transverse process removal (“C1 shave”)
• Jugular vein fasciotomy
• Selective digastric muscle division or resection, if needed
Partial decompression, limited styloid removal, absence of C1 shaving is often insufficient. The internal jugular vein must be fully released circumferentially to restore adequate venous outflow. Without comprehensive decompression, symptoms frequently persist without meaningful improvement.
Raising Awareness
This condition remains under-recognized in mainstream neurology and neurosurgery, yet it can dramatically impact quality of life. Increasing awareness among clinicians is critical — not only for diagnosis, but for appropriate surgical planning and execution.
I am grateful to IANA for the opportunity to speak on this topic and to help bring attention to a group of patients who are too often overlooked.
You can listen to my full lecture here (starts at 16:33):
youtube.com/live/nGFDx88RvnM…
If you care for patients with unexplained symptoms of intracranial hypertension, refractory headaches, or persistent neurological complaints despite “normal” workups, I encourage you to consider venous outflow obstruction in your differential diagnosis. Recognition is the first step — and when properly treated, these patients can regain their lives.
For inquiries:
James K. Liu, MD
Director, Skull Base Institute of New Jersey
973-577-2888
Email: jliu@neurosurgerynj.com
@SkullBaseMD
#VascularEagles #EaglesSyndrome
@NeuroSurgeryNJ @CBMCNJ @RWJBarnabas
2
26
1,500
Jan 28
I’m truly honored to be an invited guest lecturer for the Skull Base Surgery Society of India Webinar this morning. Grateful for the opportunity to share and exchange ideas with such an incredible community of neurosurgeons and educators.
I’ll be speaking on endoscopic endonasal approaches for complex craniopharyngiomas, a topic that continues to evolve and challenge us in meaningful ways.
It’s a privilege to be on the program alongside such esteemed colleagues as Dr. Laligam Sekhar, Dr. Basant Misra, Dr. Sarat Chandra, and Dr. Dwarakanath Srinivas. Looking forward to a stimulating academic exchange and great discussions.
Thank you to the India Skull Base Society for the invitation — excited for what’s ahead!
Starts 9:30am EST, wed, 1/28/26
Link to join:
Scan QR code in the photo.
#skullbasesurgery #craniopharyngioma
@NeuroSurgeryNJ @CBMCNJ @RWJBarnabas
2
8
363
Jan 23
Dear Friends and Colleagues,
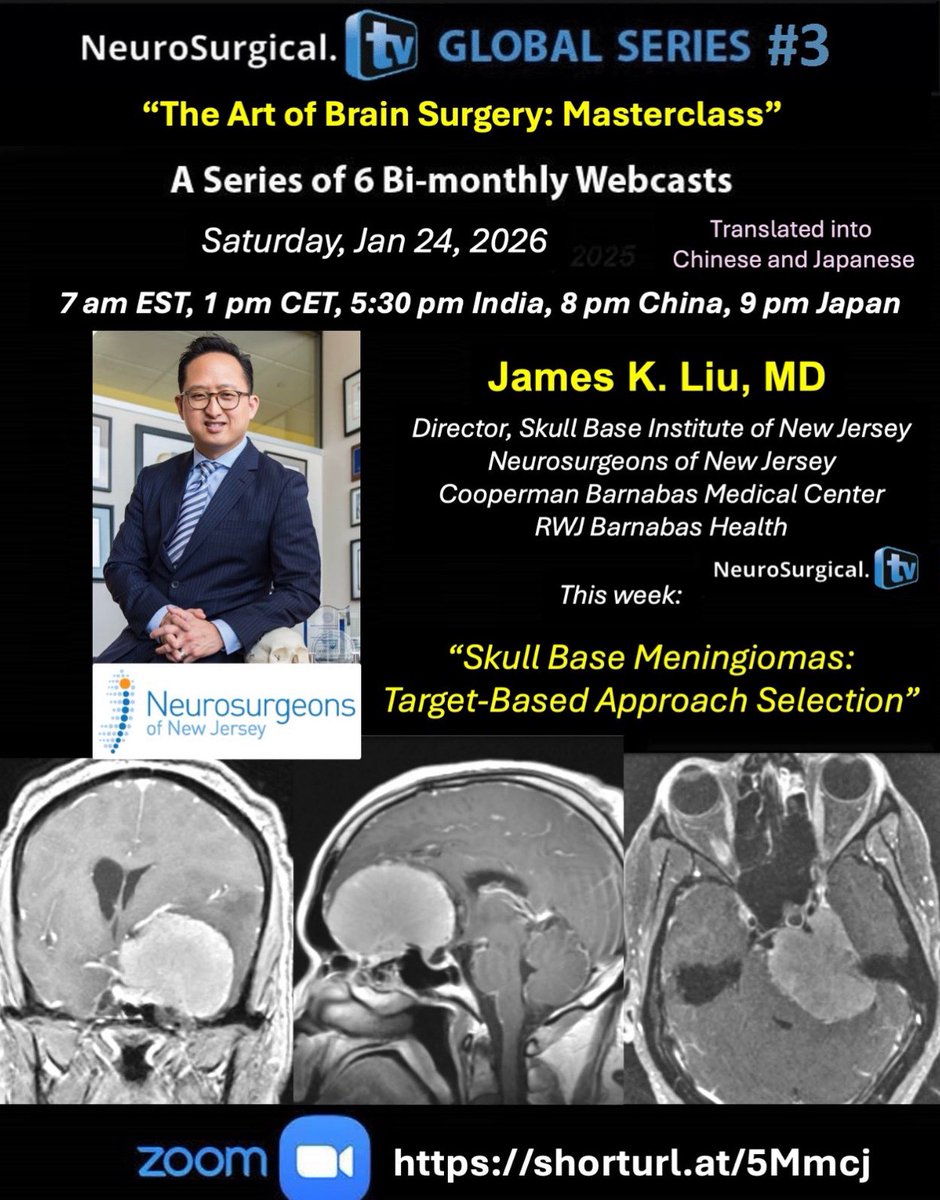
I am very excited to kick off 2026 with another installment of my bimonthly lecture series, "The Art of Brain Surgery: Masterclass" in collaboration with @NeuroSurgicalTV. It’s an immersive operative video series emphasizing intraoperative “game time” decision making, anatomical considerations, practical technical pearls, tricks of the trade, and complication avoidance.
Kicking off first episode with:
“Skull Base Meningiomas: Target-Based Approach Selection” this Saturday, January 24 at 7 am EST.
Objectives: Learn the nuances of the technique, tips and tricks and operative pearls to maximize tumor resection while preserving cranial nerves. Meningiomas serve as perfect tour guides to take you through the complex skull base real estate.
neurosurgical.tv/james-liu-m…
ZOOM REGISTRATION:
shorturl.at/5Mmcj
Webinar ID
881 1388 4560
#meningioma #skullbasesurgery #neurosurgery #education
@neurosurgerynj @coopermanbarnabas @rwjbarnabas_health @meningiomacompanion @meningiomasinfo whs.meningioma.awareness @meningiomamommas @rutgersneurosurgery @rutgerscancerinstitute @rutgers_rhinology_skullbase @rutgers_oto @nymcbrainspine @alifathali @montefioreneurosurgery @uofuneurosurgery @nyu_neurosurgery @nasbs_org
1
3
20
1,068
18 Dec 2025
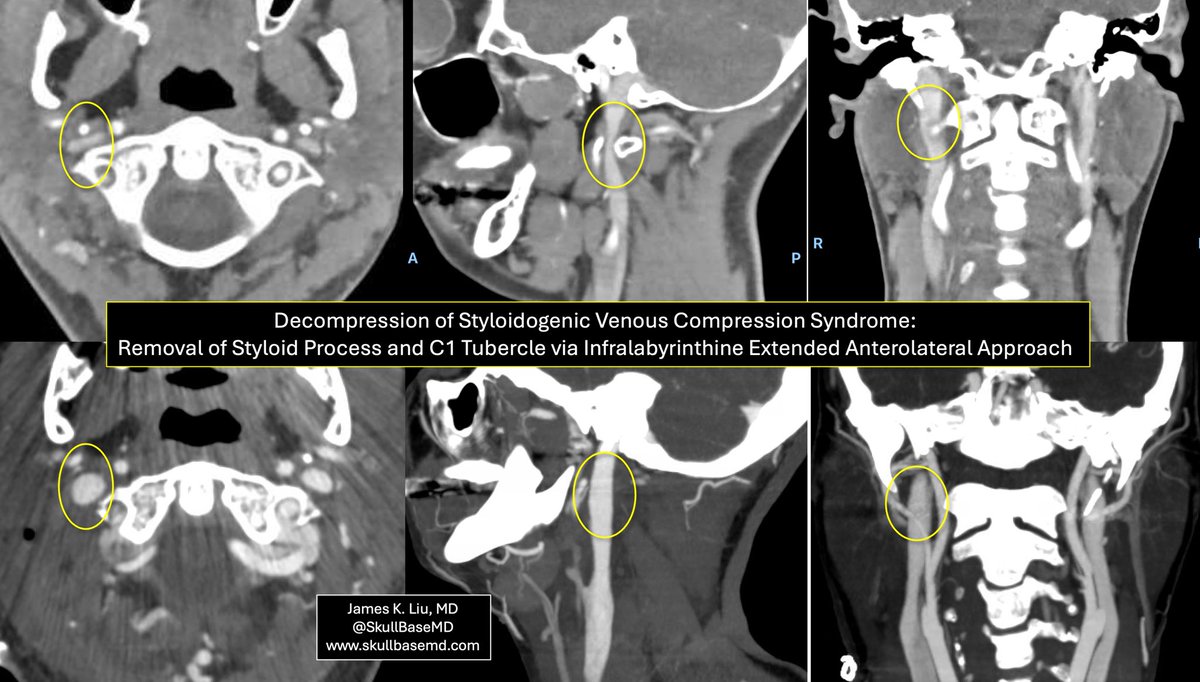
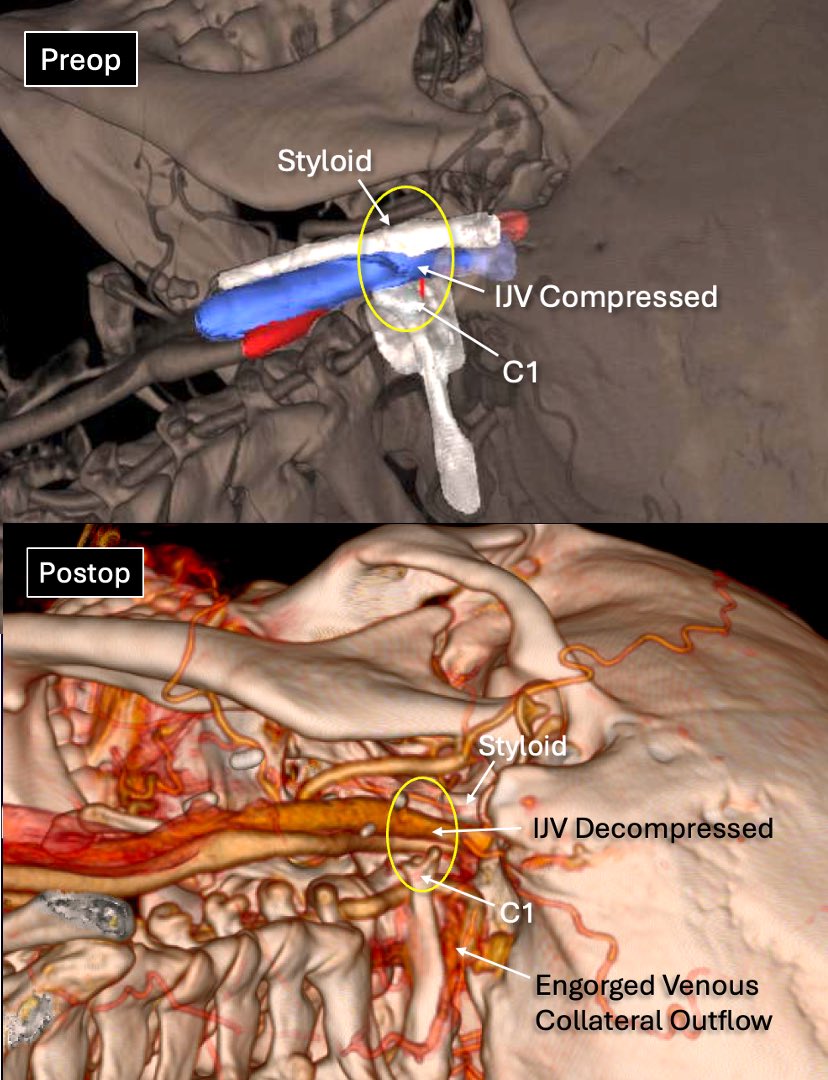
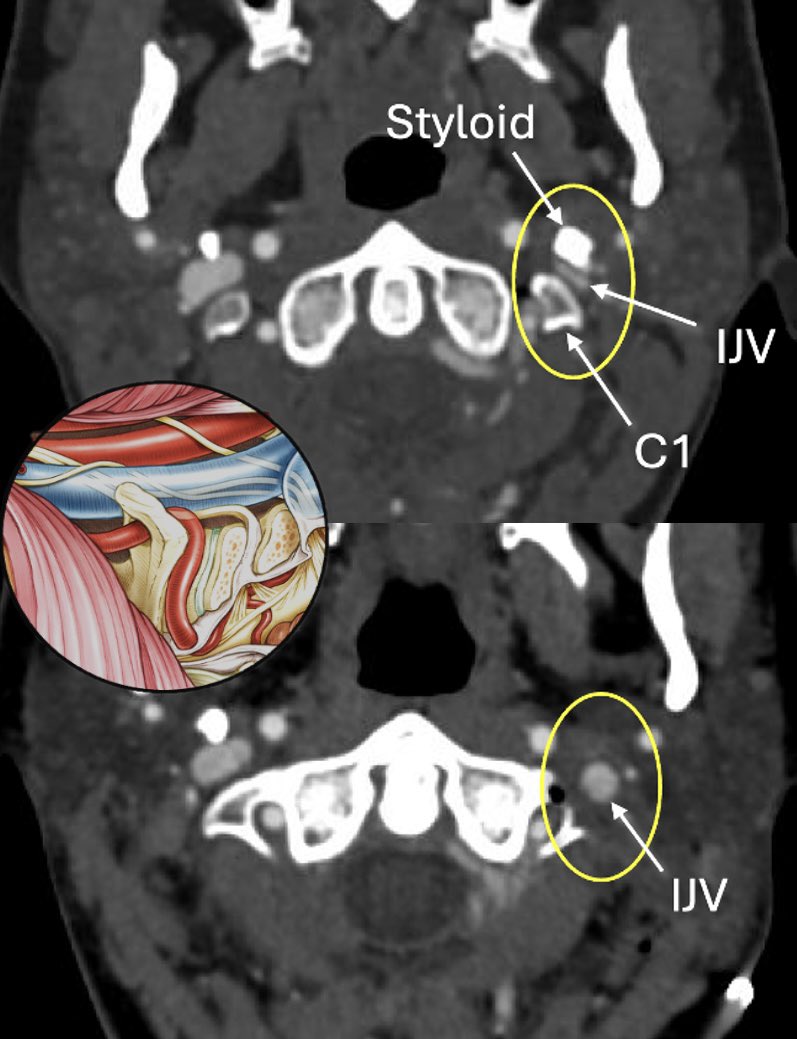
Styloidogenic Venous Compression Syndrome is an under-recognized cause of intracranial venous hypertension and debilitating symptoms. It is often inaccurately referred to as Eagle’s syndrome or venous Eagle’s variant because of the relationship to an elongated styloid process.
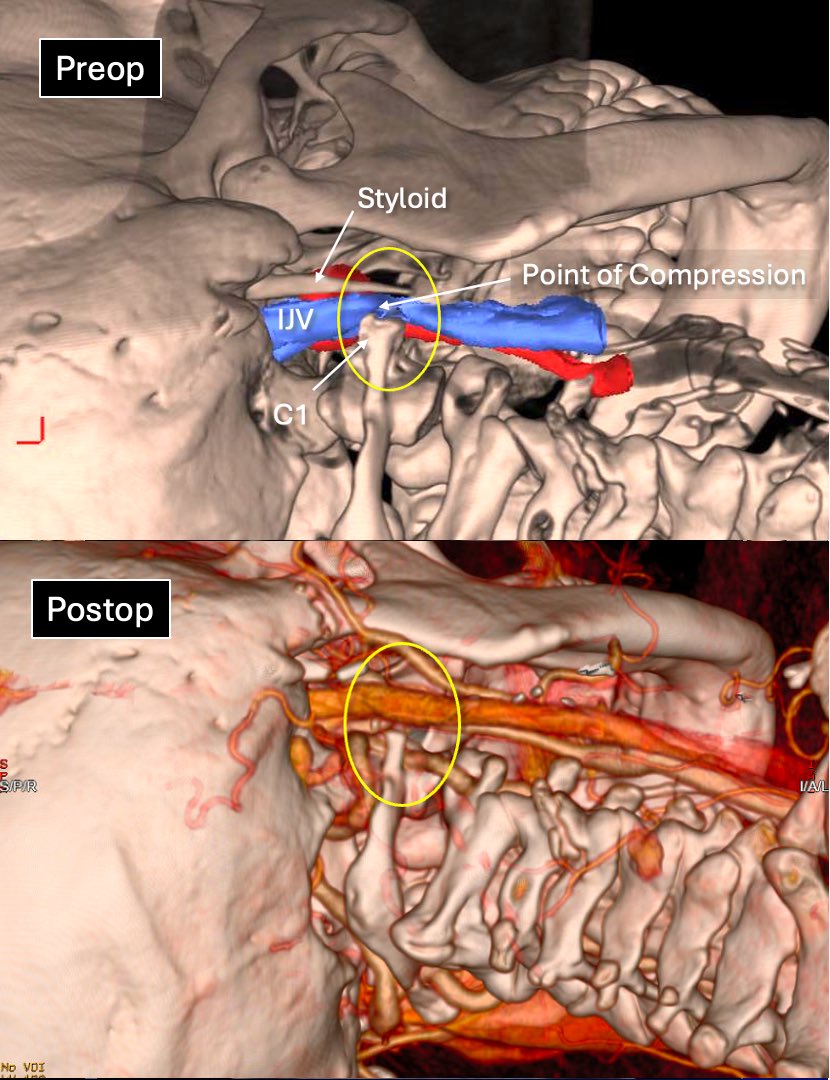
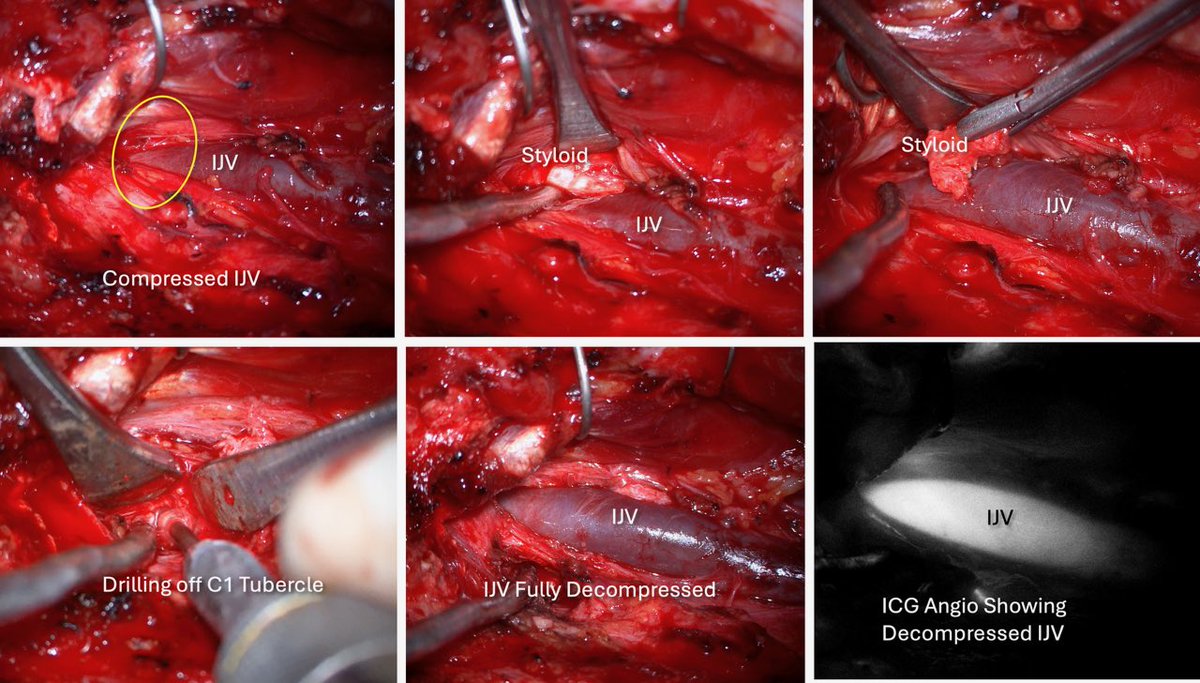
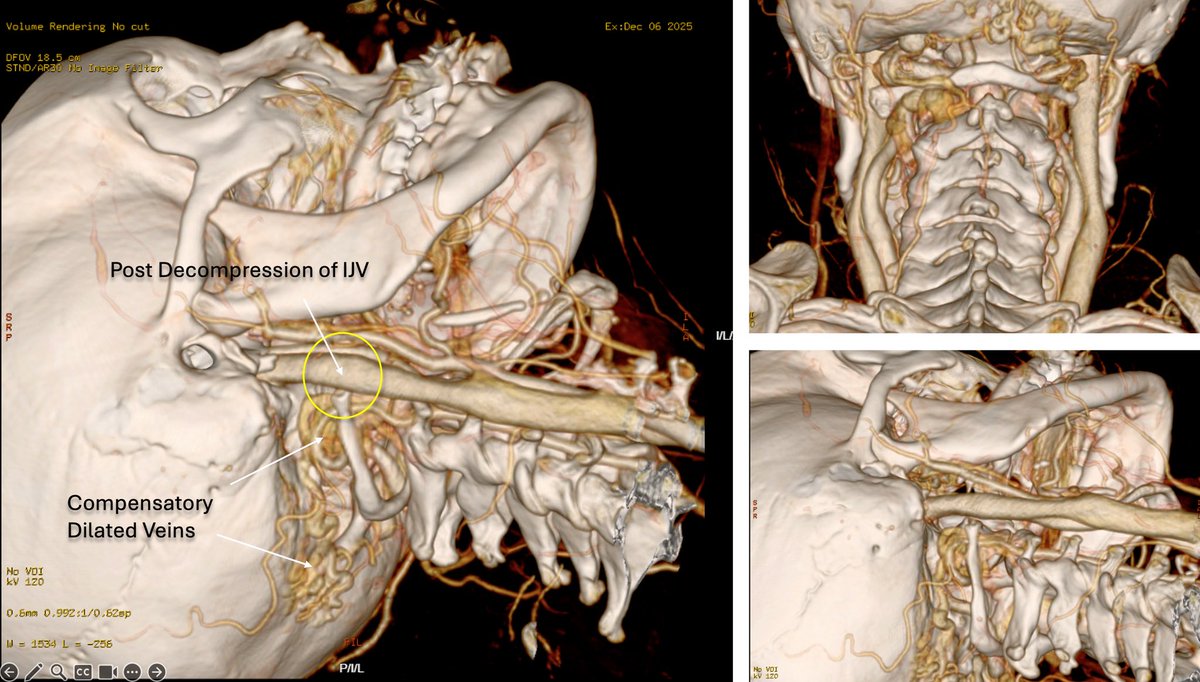
This patient had symptoms of intracranial venous hypertension where an elongated styloid process and C1 tubercle pinch off the internal jugular vein, impairing brain venous drainage (yellow circle). A dynamic angiogram by showed engorged collateral venous ouflow at the skull base with a pressure gradient at the level of the jugular vein compression at C1. We successfully treated the venous compression by performing microsurgical styloidectomy with drilling of the C1 tubercle, achieving complete 360-degree decompression of the internal jugular vein.
➡️ Pre- and post-operative images show dramatic restoration of venous flow, and intra-op photos demonstrate the key steps of the procedure. A reminder that anatomy matters — and that targeted skull base techniques can provide definitive relief when the diagnosis is correct. A technically demanding skull base and vascular problem — but one that can be definitively treated when recognized.
Rare diagnosis. Precise surgery. Meaningful outcome.
@SkullBaseMD
skullbasemd.com
@neurosurgerynj
#styloidogenicjugularvenouscompressionsyndrome #eaglessyndrome #skullbasesurgery #skullbasemd @coopermanbarnabas @rwjbarnabas_health
1
1
14
607