
Joined November 2023
- Tweets 13,297
- Following 660
- Followers 661
- Likes 11,302
1,084 Photos and videos







Pinned Tweet

Live look at $NVO data scientists trying to find a way to frame semaglutide favorably against competition
1
5
2,663
I think Berobenatide probably is a better molecule than sema Independent of the longer t1/2, explained by Gas full bias. $Pfe did themselves a disservice with their stupid monthly dosing and large step titration schemes.

The t1/2 of berobenatide is 15 days, that means w/ monthly dosing they're stretching it out to 2x t1/2. That's worse than tirzepatide which is already bad enough at 1.4x t1/2. That's why many experiment with splitting doses, especially fast metabolizers. $PFE are retards
2
131
Going 2x t1/2 between doses is excessive. It means you have a huge acute spike after dosing, which is when you get the worst GI symptoms. And in the back half of the month the drug will only be around 1/4-1/3 of its peak concentration, so you may not be in a therapeutic range.
1
45
That's why if they just stick with a normal weekly dosing they should get much better ratio of therapeutic benefit to side effect burden.
33
Claude is so annoying it makes working through anything 5x harder because its stupid programming tells it to fight you on every single point and be endlessly pedantic. It's mentally exhausing.
52
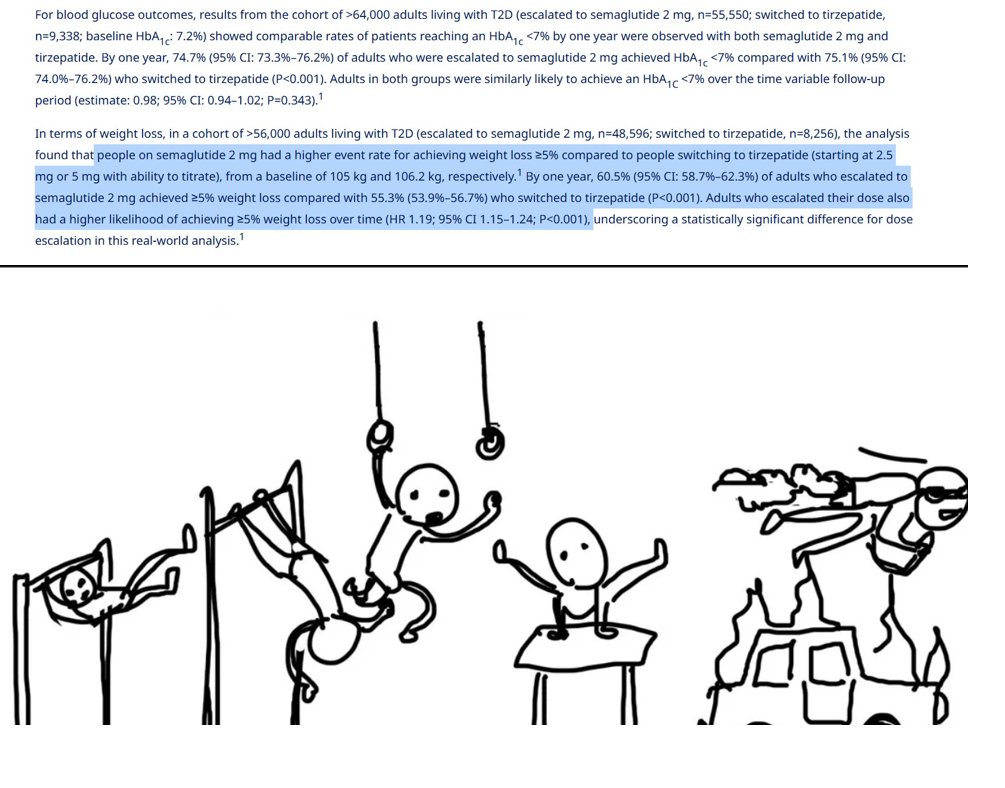
If you compare 4.8mg/mo bero vs 2.4mg/wk sema gives you the same avg exposure due to bero having 2x the t1/2 but it caused 12.4% pbo-adj wl in 28 weeks versus same wl in 68wk for sema. If they ditch the stupid dosing and titration gimmicks, think they'll show it's superior. $nvo
1
92
The theory behind Gas bias is you avoid B-arrestin recruitment, which causes endocytosis (receptor is physically pulled into the cell so sensitivity is reduced). So the mechanism behind bero > sema at = exposure is you are retaining full sensitivity.
33
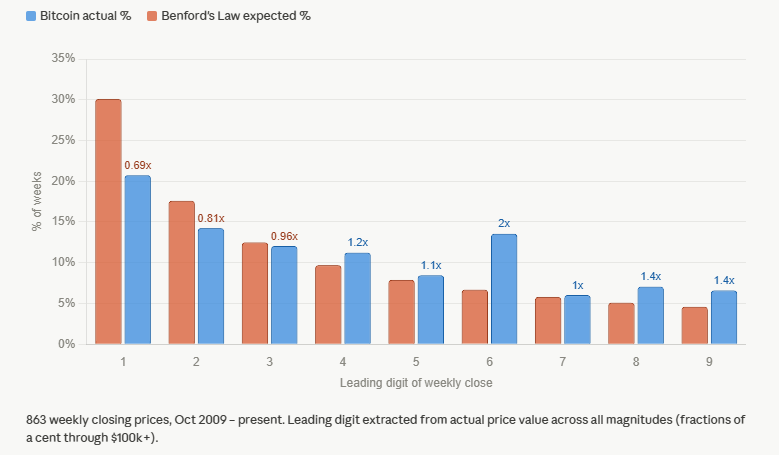
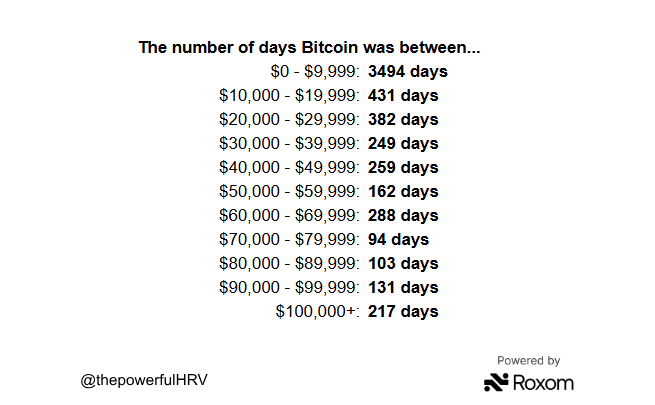
Benford's law agrees, BTC has spent 2x the expected time at a number beginning with "6". 1-3 are the most in need of backfilling $BTCUSD

64
Gray market is not really an economically relevant "competitor". Particularly in the premium t2d market. Not much overlap between the retarded "biohackers" who happily shoot up Chinese rat poison vs patients who want safe and regulated drugs. Different populations.
23h

Retatrutide hit 30% weight loss at ADA. All the headlines ran the same number.
Retatrutide is already available via the grey-market, unapproved, 37 of 37 samples failed purity testing. The higher Lilly prices the real thing, the bigger the counterfeit market it subsidizes.
Lilly can move to kill that market. IMO most pricing models miss it.
New Kontra ↓
$LLY $NVO

3
2
510
I think that might be what he's trying to argue. I'm not sure kind of unclear due to clickbaity presentation
2
50
But they're not going to price it so low just because a gray market exists.
1
33
This guy just doesn't know when to shut the fuck up. He can't make a deal because he can't go 5 seconds without talking about how big he thinks his dick is. That's not how you show you're dealing in good faith.

TRUMP ON IRAN: HOPEFULLY, THIS PROCESS WILL ALL WORK OUT QUICKLY, EASILY, AND SMOOTHLY; IF IT DOESN'T, WE HAVE ULTIMATE ALTERNATIVE
85
case in point, The same online marketplaces where you can get reta also have tirzepatide. Yet branded tzp is selling like hotcakes.
87
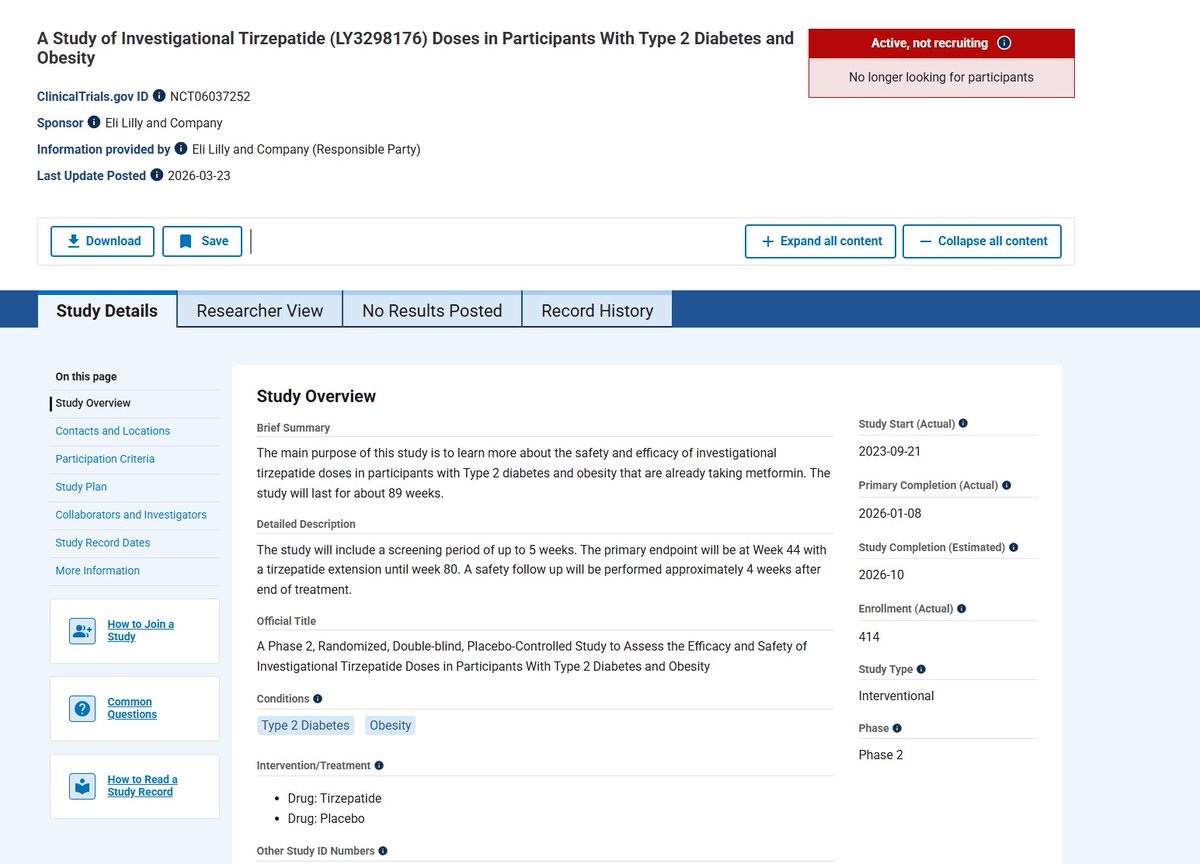
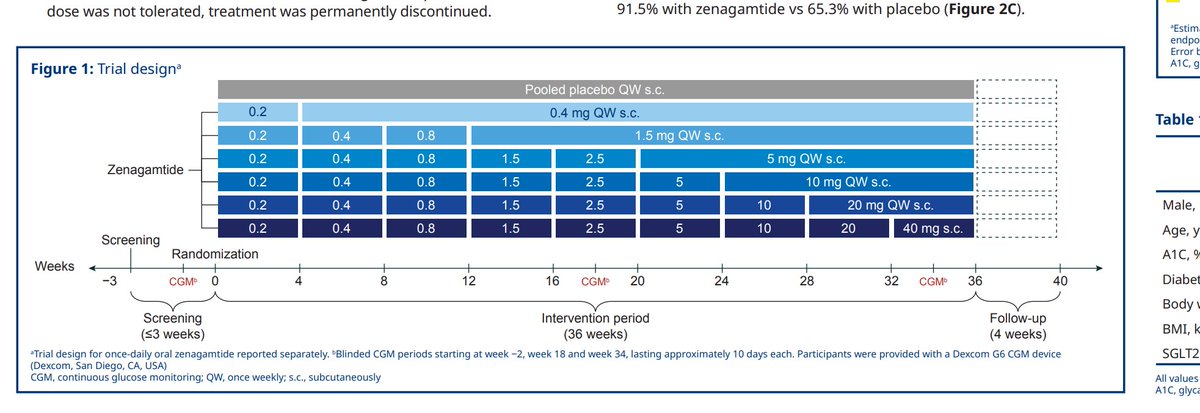
Thinking more about Zenagamtide. Induction dose is 0.2 mg, and they run it up to 40. I can't find any drug where the multiplier between the induction and max dose is 200x. Most requiring titr are btw 10-20. Ie tzp, 6x from 2.5 to 15. Semaglutide 10x (now 30x with HD). $nvo $lly
It seems 5mg may be max dose that works w/o unacceptable DC rates. T2D and males are both less sensitive to GI upset so obesity trial (usually 60-70% F) will be worse. 5mg arm may be able to stretch the titration sched more. >=10mg won't have time w/i P3 format $NVO $lly $vktx
3
7
4,803
In this earlier trial they started the induction dose at 0.3, so they lowered it by a third to try to improve the tolerability.

1
148
Amycretin is a GLP-1 analog covalently bonded to an amylin analog. It's kind of like if they just duct taped a sema molecule to a cagrilintide molecule. And they are both fully unbiased. So it's like a sledgehammer approach.
2
2
137
So the point is they didn't just arbitrarily choose 0.2mg to start, they knew it had massive tolerability issues already and this is their way to try to work around it. But the multiple from induction to therapeutic dose should be red flag.
138
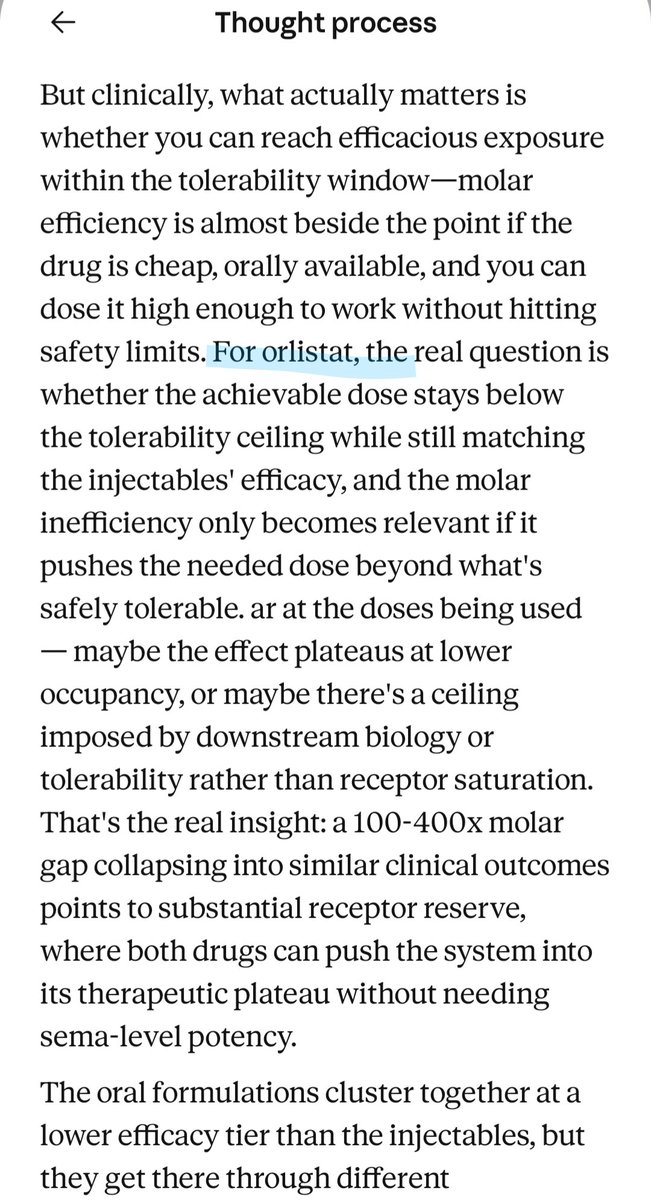
Asking Claude PK/PD q's about current oral glp-1s and it keeps calling orforglipron "orlistat" in its "thoughts". Realized orfo at = mass dose gives roughly 400x the molarity vs sema w/ similar clinical response, which is interesting science but may not be clinically relevant
2
1
230
I think closer to 30%. The rel potency at glp-1r is 16.6x higher for sema, and the molar mass is ~15% lower. so at = mass in blood you get 16.6/.85= 19.5x receptor activation from sem. but the mass is 2.4/15=.16. so 19.5 *0.16=3.12 or ->1/3.12= 32% the activation from 15mg tzp
1
77
This is for Gs activation. TZP recruitment of B-arrestin is almost zero vs full recruitment for sema
73